Article
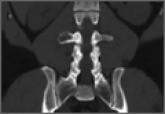
Ureter and Nerve Root Compression Secondary to Expansile Fibrous Dysplasia of the Transverse Process
Considering their proximity to abdominal viscera, transverse process lesions may pose a diagnostic challenge. We present a case of fibrous...