News
On Second Thought: Aspirin for Primary Prevention — What We Really Know
Recommendations vis-à-vis aspirin have evolved at a dizzying pace.
News
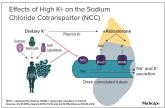
Sodium vs Potassium for Lowering Blood Pressure?
Nephrologist discusses benefits of reducing salt in diet and eating more potassium to reduce BP.
Opinion

Multivitamins and dementia: Untangling the COSMOS study web
When you get a positive result in your research, it’s always exciting. But when a slew of studies that came before you are negative, you aren’t...
Opinion
Conflicting blood pressure targets: Déjà vu all over again
Arguing about 140/90 mm Hg or 130/80 mm Hg is less important than acknowledging that we should be aggressive in screening for and treating...
Opinion
Is it time to stop treating high triglycerides?
There may be noncardiovascular reasons to treat hypertriglyceridemia.