News

Just gas? New study on colic suggests some longer-term implications
Colic may reflect a bit more than most of us have been taught and shouldn’t necessarily be “shrugged off.”
News
Integrating mental health and primary care: From dipping a toe to taking a plunge
New models of integrated or collaborative care between primary care and mental health clinicians have been attempted and tested.
Opinion

AAP vs. AED on obesity treatment: Is there a middle ground?
Productive dialogue would be likely enhanced if both sides avoided unfounded speculation about bias and motive and worked from a good faith...
Opinion
New guidelines say pediatricians should screen for anxiety: Now what?
While pediatricians fully appreciate how common clinically significant anxiety is and its impact on the lives of youth, the reception for the...
Article

Incorporating positive psychiatry with children and adolescents
SECOND OF 4 PARTS
The principles and practices of positive psychiatry can be readily adapted into routine practice.
Opinion
Surgeon General releases child mental health call to action
While recognizing that technology, smartphones, and social media are here to stay, a number of suggestions were given to parents, media...
News

Online mental health treatment: Is this the answer we’ve been waiting for?
For some families, it is likely to provide new access to services not easily obtainable locally, while for others it could end up being a costly...
News
Ending the ED ‘boarding’ of youth with mental health needs
Health care systems and governments need to evaluate the degree to which more hospital or residential beds may still be needed, despite our best...
Opinion
COVID-19 and youth suicide: Do the numbers match the headlines?
Whether or not the pandemic is making things significantly worse, youth suicide remains an enormous public health imperative, with every one being...
Opinion

Getting the most out of a psychiatric consultation
Know who to send it to, what to ask for, and what information to include in a consult request.
Opinion
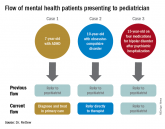
Pediatricians take on more mental health care
Many pediatricians already endorse the idea that mild to moderate mental health problems are “in their lane.”

Opinion

Anxiety disorders: Psychopharmacologic treatment update
Although medications can be useful in treating anxiety disorders, they are not recommended as a stand alone treatment.
Opinion

Nature versus nurture: 50 years of a popular debate
Dr. Rettew gives a brief history of a debate that’s endured and fascinated for centuries.