Article

The Top 100 Cited Articles in Clinical Orthopedic Sports Medicine
Orthopedic sports medicine continues to evolve, owing much of its clinical management and practice to rigorous academic research.
Article
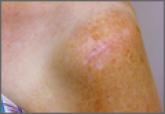
Cutaneous Burn Caused by Radiofrequency Ablation Probe During Shoulder Arthroscopy
It is common in shoulder surgery to perform an arthroscopic acromioplasty for patients with varying degrees of rotator cuff disease.