Quiz

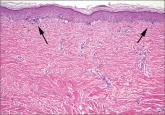
Lobular-Appearing Nodule on the Scalp
A 79-year-old woman presented with a lesion on the left side of the scalp of several years’ duration that had slowly increased in size. Despite...
Article
9 tips to help prevent derm biopsy mistakes
The authors—with expertise in dermatology and pathology—provide pointers that can help you improve your approach to skin biopsy.