Article
A Comparison of Knowledge Acquisition and Perceived Efficacy of a Traditional vs Flipped Classroom–Based Dermatology Residency Curriculum
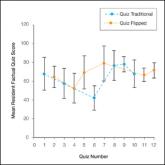
Flipped and traditional classroom models were compared in the Duke University Medical Center (Durham, North Carolina) dermatology residency...
Article

Pityriasis Rubra Pilaris and Severe Hypereosinophilia
A 63-year-old man presented with a prior diagnosis of severe psoriasis affecting the extremities, neck, face, and scalp of 1 year’s duration. He...