Article
Recurrent Cutaneous Exophiala Phaeohyphomycosis in an Immunosuppressed Patient
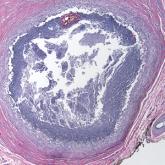
Phaeohyphomycosis is an infection with dematiaceous fungi that most commonly affects immunosuppressed patients.
Phaeohyphomycosis is an infection with dematiaceous fungi that most commonly affects immunosuppressed patients.