User login
While Residents Rest
In the three years since the Accreditation Council for Graduate Medical Education (ACGME) instituted duty hour standards, academic and community-based internal medicine (IM) residency programs have had to change the way they do business. Although several surveys have documented residents’ satisfaction with reduced duty hours, some program directors and medical directors are concerned that complying with the standards can contribute to faculty burnout, affect continuity of patient care, and diminish residents’ educational opportunities. In recent interviews, IM program directors and medical directors of hospital medicine services shared their challenges of complying with the standards.
Who Takes Care of Patients?
The major provisions of the ACGME Common Duty Hour Standards, which took effect July 1, 2003, call for a weekly work limit of 80 hours, averaged over four weeks; a 24-hour limit on continuous duty time, with an additional period of as many as six hours to allow for continuity of care and educational activities, referred to as the “30-hour rule”; one day in seven free from all patient care; in-house call no more than once every three nights; and a 10-hour rest period between duty periods and in-house call. For more information on the new standards, visit www.acgme.org.
By instituting decreased duty hours, the council aimed to ensure that residents would be well rested, medical errors would be reduced, and patient safety would be improved. Tom Baudendistel, MD, associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health, believes, however, that at the administrative level, the standards create “a potential for residency programs to be at odds with hospitals’ missions. Residency is making less money for the hospitals: For the same amount of dollars, they are receiving less coverage. So, hospitals hire additional attending physicians and physician extenders, which are a lot more expensive.”
With residents less available for extended duty hours, one of the largest challenges is to “figure out who’s going to take care of the patients,” notes Daniel Dressler, MD, MSc, director of the Hospital Medicine Service at Emory University Hospital, Atlanta. “At least in our institution, hospital medicine has stepped in to provide that care for many of the patients. We cannot get any additional house staff, and because their hours have been cut—reasonably so—we’re having to fill in the necessary gaps.”
The same phenomenon has occurred at Virginia Commonwealth University, Richmond, where Alan Dow, MD, MSHA, is assistant professor of Internal Medicine and director of the Academic Hospitalist Service. “My group has gone from two physicians four years ago, to now having 15 physicians,” he said recently. “We’ve grown, in large part, because we’re making up for the residency caps, but also because we’ve found other roles for ourselves in the health system to contribute and help.”
Another effect of decreased duty hours has been to contribute to the advent of non-teaching services, notes Dr. Baudendistel and Arpana R. Vidyarthi, MD, assistant professor of medicine and director of Quality-General Inpatient Medicine, University of California, San Francisco. At a recent panel she conducted at the SHM annual meeting, Dr. Vidyarthi said the main reason panelists cited for instituting non-teaching services was to reduce workloads for residents and comply with duty hours standards.

—Arpana R. Vidyarthi, MD
Maintain Continuity of Care
The resident work hour caps have created a kind of mismatch with daily hospital routines, says Dr. Dow. In the ideal world, residents could admit patients at 7 or 8 a.m., allowing ample time to perform a comprehensive history and physical, review patients’ tests results, synthesize all the information in an educational way, and then be able to leave at 5 or 6 p.m. that evening. “Unfortunately,” he says, “patients show up at 4 or 5 p.m., until about 8 or 10 p.m., depending on the day. Ideally, we would have the same person admit and discharge the patient, but that just isn’t feasible because of the work hour caps.”
At Virginia Commonwealth, Dr. Dow’s hospitalist group has found that assigning admitting duties and ongoing patient care to separate teams allows for better patient care. Designated admitting physicians handle the admitting work in the late afternoons and evenings when most patients come up to the floor. All of the patient care is then transferred to another group of physicians who work during the day, ordering tests, speaking with consultants, and talking with families and social workers.
“What we’ve done is try to focus on continuity from that second day of hospitalization until discharge,” says Dr. Dow, “because I think the most critical point for errors in care is at discharge. We want to make sure that by the time patients go home, the discharging physician and the rest of the group have a really good idea of what is going on with those patients: What kind of home situation are they going to? What kind of follow-up do they have? What kind of medications are they going to be on? What kind of home services will they need?”
Dr. Dow has also noticed that reduced resident hours have resulted in the necessity for faculty to be more “available and present, and to focus on making the team more efficient. For my group of hospitalists, this is not a problem because our clinical venue is the hospital. But for people who are active researchers or who need to go to other clinical venues, this can be very difficult because their obligations in the hospital are more than they were five years ago.”
Casualties of Caps
No one argues that decreased duty hours are a bad idea. As a consequence, however, more work has fallen to faculty. Because residents have to be out of the hospital at designated cut-off points, attendings must stay up-to-speed with nuances of paperwork and electronic medical records. Sources agreed that they have observed faculty members working harder and harder, and many worry about issues with potential burnout among the faculty.
“As duty-hour decreases have changed the nature of the academic hospitalist’s job, this leaves less and less time to do not just the things that you may enjoy and find intellectually satisfying, but also the things that are expected for getting promoted—a necessary part of life as an academic hospitalist,” says Dr. Vidyarthi.
Other program directors voiced concerns that certain provisions of the duty standards might foster less connection to both the treatment team and to patients. “I think the fear I have as an educator,” says Dr. Baudendistel, “is the erosion of the continuity and the professionalism that is a byproduct of the work hours decrease, with the implicit hand-offs that occur in care. This is a paradigm shift. When I was a resident, this was my patient because I didn’t have too many days off. I saw my patient through the long hospitalization.”
But with changes in the duty hours, he says, now “the residents with reduced work hours and mandated days off might only admit the patient. Then three other house staff will see the patients and discharge them, and it’s not their patient any more. Who’s there to provide the continuity? It’s the attendings. So then the residents can abdicate responsibility to the senior residents and the attendings because they are only at the hospital for, say, a 12-hour shift.
“I think that shift work mentality is a definite threat to professionalism,” he concludes. “And that mentality is not good for patient care.”
Studies of Standards’ Effects
Few studies have been published specific to the hospital medicine experience with the reduced duty hours. Lin, et al., conducted four focus groups of internal medicine residents at the Washington University School of Medicine (St. Louis, Mo.), and found concerns about the effects of the duty hour restrictions on patient care and medical education.1 A study published this January in Academic Medicine by Dr. Vidyarthi and colleagues at UCSF asked 164 internal medicine residents to rate the value of their educational activities, frequency of administrative tasks interfering with education, and their educational satisfaction after duty hours were reduced.2 Dr. Vidyarthi and her coauthors did not see an increase in educational satisfaction, which was one of the expected outcomes of the new duty hour restrictions. She believes that for educational satisfaction among residents to increase, additional structural changes also must be put in place.
“If this is really an educational endeavor, then we need to make it such,” she says. “Duty hour decreases are here, so let’s make this amount of time that [the residents] are spending in the hospital as educationally valuable as possible.”
Can Less Be More?
One effect of reduced resident availability is that hospital medicine programs must become more thoughtful about the content of the educational experience for residents. If residents will see fewer patients because of fewer hours on duty, how might the remaining patient contacts be maximized for their educational opportunities?
“I think that there is much room for making their time in the hospital as educationally valuable as possible,” asserts Dr. Vidyarthi, “from pedagogical ways of thinking about medicine, to decreasing the number of tasks that they do that are not educational in value.”
Dr. Dressler agrees. “By reducing the resident work hours, we definitely reduce the amount of patient contact by residents,” he says. “Now, whether or not that will dramatically affect the amount of education the residents receive would be difficult to measure. Potentially, down the road, the American Board of Internal Medicine or some other governing board may decide that residency programs need to be longer. Medical training programs have instituted a comprehensive programmatic change [with the new work hours], will attempt to evaluate all the potential downsides as well as the value of this change, and, ultimately, will have to address problems or unexpected results in the new system in order to optimize patient care as well as physician trainee education.”
At California Pacific Medical Center’s residency program, “there are certain components we have had to re-analyze, and consider. [For example,] what is our core educational mandate that we’re trying to achieve? ” asks Dr. Baudendistel. Examining residents’ rotations, he says, has led to decisions to take residents off certain rotations, such as transplant nephrology, in favor of less esoteric rotations.
Hospitalists to the Rescue?
The question remains whether the reduced duty hours are better from the patient’s point of view. “The number of sign-outs that we’re seeing due to the duty hour decreases is significant. Interns will sign out approximately 300 times in a month, which is more than the number of patients they’ll see in the course of a year and, in fact, more often than they will eat in a month,” says Dr. Vidyarthi. “So, the challenge for the safety of patients [one of the impetuses for the decreased duty hours] is being balanced against having better rested, potentially better educated, happier residents. It’s really a Faustian bargain. Are we making this bargain [for better-rested residents] such that patients will, in fact, not be safer, because of the sign outs?”
Concerns about continuity of care under the new standard are “reasonable and legitimate,” says Dr. Dressler. “From a hospital medicine standpoint, that is how we practice: We are frequently handing off care. We understand that there is an inherent potential risk of doing that, and we like to be able to teach and train residents and students to understand how to do that effectively as part of their practice. Because hospitalists do this daily, we have an understanding of how to train people to optimally handoff patients to other clinicians and/or transition patients to other care settings or the outpatient arena.”
Dr. Dow views his hospitalist group as a sort of a “free safety,” taking care of patients that residents may not be able to take care of. “I view hospitalists as problem-solvers. Whether it’s a specific patient with a medical or social need, or a system problem, our big role is in filling those needs,” he says. “When patients need to be admitted and no other group is available, my hospitalist group is ready to care for folks.” TH
Gretchen Henkel is based in California.
References:
- Lin GA, Beck DC, Garbutt JM. Residents’ perceptions of the effects of work hour limitations at a large teaching hospital. Acad Med. 2006 Jan;81(1):63-67.
- Vidyarthi AR, Katz PP, Wall SD, et al. Impact of reduced duty hours on residents’ educational satisfaction at the University of California, San Francisco. Acad Med. 2006 Jan;81(1):76-81.
In the three years since the Accreditation Council for Graduate Medical Education (ACGME) instituted duty hour standards, academic and community-based internal medicine (IM) residency programs have had to change the way they do business. Although several surveys have documented residents’ satisfaction with reduced duty hours, some program directors and medical directors are concerned that complying with the standards can contribute to faculty burnout, affect continuity of patient care, and diminish residents’ educational opportunities. In recent interviews, IM program directors and medical directors of hospital medicine services shared their challenges of complying with the standards.
Who Takes Care of Patients?
The major provisions of the ACGME Common Duty Hour Standards, which took effect July 1, 2003, call for a weekly work limit of 80 hours, averaged over four weeks; a 24-hour limit on continuous duty time, with an additional period of as many as six hours to allow for continuity of care and educational activities, referred to as the “30-hour rule”; one day in seven free from all patient care; in-house call no more than once every three nights; and a 10-hour rest period between duty periods and in-house call. For more information on the new standards, visit www.acgme.org.
By instituting decreased duty hours, the council aimed to ensure that residents would be well rested, medical errors would be reduced, and patient safety would be improved. Tom Baudendistel, MD, associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health, believes, however, that at the administrative level, the standards create “a potential for residency programs to be at odds with hospitals’ missions. Residency is making less money for the hospitals: For the same amount of dollars, they are receiving less coverage. So, hospitals hire additional attending physicians and physician extenders, which are a lot more expensive.”
With residents less available for extended duty hours, one of the largest challenges is to “figure out who’s going to take care of the patients,” notes Daniel Dressler, MD, MSc, director of the Hospital Medicine Service at Emory University Hospital, Atlanta. “At least in our institution, hospital medicine has stepped in to provide that care for many of the patients. We cannot get any additional house staff, and because their hours have been cut—reasonably so—we’re having to fill in the necessary gaps.”
The same phenomenon has occurred at Virginia Commonwealth University, Richmond, where Alan Dow, MD, MSHA, is assistant professor of Internal Medicine and director of the Academic Hospitalist Service. “My group has gone from two physicians four years ago, to now having 15 physicians,” he said recently. “We’ve grown, in large part, because we’re making up for the residency caps, but also because we’ve found other roles for ourselves in the health system to contribute and help.”
Another effect of decreased duty hours has been to contribute to the advent of non-teaching services, notes Dr. Baudendistel and Arpana R. Vidyarthi, MD, assistant professor of medicine and director of Quality-General Inpatient Medicine, University of California, San Francisco. At a recent panel she conducted at the SHM annual meeting, Dr. Vidyarthi said the main reason panelists cited for instituting non-teaching services was to reduce workloads for residents and comply with duty hours standards.
—Arpana R. Vidyarthi, MD
Maintain Continuity of Care
The resident work hour caps have created a kind of mismatch with daily hospital routines, says Dr. Dow. In the ideal world, residents could admit patients at 7 or 8 a.m., allowing ample time to perform a comprehensive history and physical, review patients’ tests results, synthesize all the information in an educational way, and then be able to leave at 5 or 6 p.m. that evening. “Unfortunately,” he says, “patients show up at 4 or 5 p.m., until about 8 or 10 p.m., depending on the day. Ideally, we would have the same person admit and discharge the patient, but that just isn’t feasible because of the work hour caps.”
At Virginia Commonwealth, Dr. Dow’s hospitalist group has found that assigning admitting duties and ongoing patient care to separate teams allows for better patient care. Designated admitting physicians handle the admitting work in the late afternoons and evenings when most patients come up to the floor. All of the patient care is then transferred to another group of physicians who work during the day, ordering tests, speaking with consultants, and talking with families and social workers.
“What we’ve done is try to focus on continuity from that second day of hospitalization until discharge,” says Dr. Dow, “because I think the most critical point for errors in care is at discharge. We want to make sure that by the time patients go home, the discharging physician and the rest of the group have a really good idea of what is going on with those patients: What kind of home situation are they going to? What kind of follow-up do they have? What kind of medications are they going to be on? What kind of home services will they need?”
Dr. Dow has also noticed that reduced resident hours have resulted in the necessity for faculty to be more “available and present, and to focus on making the team more efficient. For my group of hospitalists, this is not a problem because our clinical venue is the hospital. But for people who are active researchers or who need to go to other clinical venues, this can be very difficult because their obligations in the hospital are more than they were five years ago.”
Casualties of Caps
No one argues that decreased duty hours are a bad idea. As a consequence, however, more work has fallen to faculty. Because residents have to be out of the hospital at designated cut-off points, attendings must stay up-to-speed with nuances of paperwork and electronic medical records. Sources agreed that they have observed faculty members working harder and harder, and many worry about issues with potential burnout among the faculty.
“As duty-hour decreases have changed the nature of the academic hospitalist’s job, this leaves less and less time to do not just the things that you may enjoy and find intellectually satisfying, but also the things that are expected for getting promoted—a necessary part of life as an academic hospitalist,” says Dr. Vidyarthi.
Other program directors voiced concerns that certain provisions of the duty standards might foster less connection to both the treatment team and to patients. “I think the fear I have as an educator,” says Dr. Baudendistel, “is the erosion of the continuity and the professionalism that is a byproduct of the work hours decrease, with the implicit hand-offs that occur in care. This is a paradigm shift. When I was a resident, this was my patient because I didn’t have too many days off. I saw my patient through the long hospitalization.”
But with changes in the duty hours, he says, now “the residents with reduced work hours and mandated days off might only admit the patient. Then three other house staff will see the patients and discharge them, and it’s not their patient any more. Who’s there to provide the continuity? It’s the attendings. So then the residents can abdicate responsibility to the senior residents and the attendings because they are only at the hospital for, say, a 12-hour shift.
“I think that shift work mentality is a definite threat to professionalism,” he concludes. “And that mentality is not good for patient care.”
Studies of Standards’ Effects
Few studies have been published specific to the hospital medicine experience with the reduced duty hours. Lin, et al., conducted four focus groups of internal medicine residents at the Washington University School of Medicine (St. Louis, Mo.), and found concerns about the effects of the duty hour restrictions on patient care and medical education.1 A study published this January in Academic Medicine by Dr. Vidyarthi and colleagues at UCSF asked 164 internal medicine residents to rate the value of their educational activities, frequency of administrative tasks interfering with education, and their educational satisfaction after duty hours were reduced.2 Dr. Vidyarthi and her coauthors did not see an increase in educational satisfaction, which was one of the expected outcomes of the new duty hour restrictions. She believes that for educational satisfaction among residents to increase, additional structural changes also must be put in place.
“If this is really an educational endeavor, then we need to make it such,” she says. “Duty hour decreases are here, so let’s make this amount of time that [the residents] are spending in the hospital as educationally valuable as possible.”
Can Less Be More?
One effect of reduced resident availability is that hospital medicine programs must become more thoughtful about the content of the educational experience for residents. If residents will see fewer patients because of fewer hours on duty, how might the remaining patient contacts be maximized for their educational opportunities?
“I think that there is much room for making their time in the hospital as educationally valuable as possible,” asserts Dr. Vidyarthi, “from pedagogical ways of thinking about medicine, to decreasing the number of tasks that they do that are not educational in value.”
Dr. Dressler agrees. “By reducing the resident work hours, we definitely reduce the amount of patient contact by residents,” he says. “Now, whether or not that will dramatically affect the amount of education the residents receive would be difficult to measure. Potentially, down the road, the American Board of Internal Medicine or some other governing board may decide that residency programs need to be longer. Medical training programs have instituted a comprehensive programmatic change [with the new work hours], will attempt to evaluate all the potential downsides as well as the value of this change, and, ultimately, will have to address problems or unexpected results in the new system in order to optimize patient care as well as physician trainee education.”
At California Pacific Medical Center’s residency program, “there are certain components we have had to re-analyze, and consider. [For example,] what is our core educational mandate that we’re trying to achieve? ” asks Dr. Baudendistel. Examining residents’ rotations, he says, has led to decisions to take residents off certain rotations, such as transplant nephrology, in favor of less esoteric rotations.
Hospitalists to the Rescue?
The question remains whether the reduced duty hours are better from the patient’s point of view. “The number of sign-outs that we’re seeing due to the duty hour decreases is significant. Interns will sign out approximately 300 times in a month, which is more than the number of patients they’ll see in the course of a year and, in fact, more often than they will eat in a month,” says Dr. Vidyarthi. “So, the challenge for the safety of patients [one of the impetuses for the decreased duty hours] is being balanced against having better rested, potentially better educated, happier residents. It’s really a Faustian bargain. Are we making this bargain [for better-rested residents] such that patients will, in fact, not be safer, because of the sign outs?”
Concerns about continuity of care under the new standard are “reasonable and legitimate,” says Dr. Dressler. “From a hospital medicine standpoint, that is how we practice: We are frequently handing off care. We understand that there is an inherent potential risk of doing that, and we like to be able to teach and train residents and students to understand how to do that effectively as part of their practice. Because hospitalists do this daily, we have an understanding of how to train people to optimally handoff patients to other clinicians and/or transition patients to other care settings or the outpatient arena.”
Dr. Dow views his hospitalist group as a sort of a “free safety,” taking care of patients that residents may not be able to take care of. “I view hospitalists as problem-solvers. Whether it’s a specific patient with a medical or social need, or a system problem, our big role is in filling those needs,” he says. “When patients need to be admitted and no other group is available, my hospitalist group is ready to care for folks.” TH
Gretchen Henkel is based in California.
References:
- Lin GA, Beck DC, Garbutt JM. Residents’ perceptions of the effects of work hour limitations at a large teaching hospital. Acad Med. 2006 Jan;81(1):63-67.
- Vidyarthi AR, Katz PP, Wall SD, et al. Impact of reduced duty hours on residents’ educational satisfaction at the University of California, San Francisco. Acad Med. 2006 Jan;81(1):76-81.
In the three years since the Accreditation Council for Graduate Medical Education (ACGME) instituted duty hour standards, academic and community-based internal medicine (IM) residency programs have had to change the way they do business. Although several surveys have documented residents’ satisfaction with reduced duty hours, some program directors and medical directors are concerned that complying with the standards can contribute to faculty burnout, affect continuity of patient care, and diminish residents’ educational opportunities. In recent interviews, IM program directors and medical directors of hospital medicine services shared their challenges of complying with the standards.
Who Takes Care of Patients?
The major provisions of the ACGME Common Duty Hour Standards, which took effect July 1, 2003, call for a weekly work limit of 80 hours, averaged over four weeks; a 24-hour limit on continuous duty time, with an additional period of as many as six hours to allow for continuity of care and educational activities, referred to as the “30-hour rule”; one day in seven free from all patient care; in-house call no more than once every three nights; and a 10-hour rest period between duty periods and in-house call. For more information on the new standards, visit www.acgme.org.
By instituting decreased duty hours, the council aimed to ensure that residents would be well rested, medical errors would be reduced, and patient safety would be improved. Tom Baudendistel, MD, associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health, believes, however, that at the administrative level, the standards create “a potential for residency programs to be at odds with hospitals’ missions. Residency is making less money for the hospitals: For the same amount of dollars, they are receiving less coverage. So, hospitals hire additional attending physicians and physician extenders, which are a lot more expensive.”
With residents less available for extended duty hours, one of the largest challenges is to “figure out who’s going to take care of the patients,” notes Daniel Dressler, MD, MSc, director of the Hospital Medicine Service at Emory University Hospital, Atlanta. “At least in our institution, hospital medicine has stepped in to provide that care for many of the patients. We cannot get any additional house staff, and because their hours have been cut—reasonably so—we’re having to fill in the necessary gaps.”
The same phenomenon has occurred at Virginia Commonwealth University, Richmond, where Alan Dow, MD, MSHA, is assistant professor of Internal Medicine and director of the Academic Hospitalist Service. “My group has gone from two physicians four years ago, to now having 15 physicians,” he said recently. “We’ve grown, in large part, because we’re making up for the residency caps, but also because we’ve found other roles for ourselves in the health system to contribute and help.”
Another effect of decreased duty hours has been to contribute to the advent of non-teaching services, notes Dr. Baudendistel and Arpana R. Vidyarthi, MD, assistant professor of medicine and director of Quality-General Inpatient Medicine, University of California, San Francisco. At a recent panel she conducted at the SHM annual meeting, Dr. Vidyarthi said the main reason panelists cited for instituting non-teaching services was to reduce workloads for residents and comply with duty hours standards.
—Arpana R. Vidyarthi, MD
Maintain Continuity of Care
The resident work hour caps have created a kind of mismatch with daily hospital routines, says Dr. Dow. In the ideal world, residents could admit patients at 7 or 8 a.m., allowing ample time to perform a comprehensive history and physical, review patients’ tests results, synthesize all the information in an educational way, and then be able to leave at 5 or 6 p.m. that evening. “Unfortunately,” he says, “patients show up at 4 or 5 p.m., until about 8 or 10 p.m., depending on the day. Ideally, we would have the same person admit and discharge the patient, but that just isn’t feasible because of the work hour caps.”
At Virginia Commonwealth, Dr. Dow’s hospitalist group has found that assigning admitting duties and ongoing patient care to separate teams allows for better patient care. Designated admitting physicians handle the admitting work in the late afternoons and evenings when most patients come up to the floor. All of the patient care is then transferred to another group of physicians who work during the day, ordering tests, speaking with consultants, and talking with families and social workers.
“What we’ve done is try to focus on continuity from that second day of hospitalization until discharge,” says Dr. Dow, “because I think the most critical point for errors in care is at discharge. We want to make sure that by the time patients go home, the discharging physician and the rest of the group have a really good idea of what is going on with those patients: What kind of home situation are they going to? What kind of follow-up do they have? What kind of medications are they going to be on? What kind of home services will they need?”
Dr. Dow has also noticed that reduced resident hours have resulted in the necessity for faculty to be more “available and present, and to focus on making the team more efficient. For my group of hospitalists, this is not a problem because our clinical venue is the hospital. But for people who are active researchers or who need to go to other clinical venues, this can be very difficult because their obligations in the hospital are more than they were five years ago.”
Casualties of Caps
No one argues that decreased duty hours are a bad idea. As a consequence, however, more work has fallen to faculty. Because residents have to be out of the hospital at designated cut-off points, attendings must stay up-to-speed with nuances of paperwork and electronic medical records. Sources agreed that they have observed faculty members working harder and harder, and many worry about issues with potential burnout among the faculty.
“As duty-hour decreases have changed the nature of the academic hospitalist’s job, this leaves less and less time to do not just the things that you may enjoy and find intellectually satisfying, but also the things that are expected for getting promoted—a necessary part of life as an academic hospitalist,” says Dr. Vidyarthi.
Other program directors voiced concerns that certain provisions of the duty standards might foster less connection to both the treatment team and to patients. “I think the fear I have as an educator,” says Dr. Baudendistel, “is the erosion of the continuity and the professionalism that is a byproduct of the work hours decrease, with the implicit hand-offs that occur in care. This is a paradigm shift. When I was a resident, this was my patient because I didn’t have too many days off. I saw my patient through the long hospitalization.”
But with changes in the duty hours, he says, now “the residents with reduced work hours and mandated days off might only admit the patient. Then three other house staff will see the patients and discharge them, and it’s not their patient any more. Who’s there to provide the continuity? It’s the attendings. So then the residents can abdicate responsibility to the senior residents and the attendings because they are only at the hospital for, say, a 12-hour shift.
“I think that shift work mentality is a definite threat to professionalism,” he concludes. “And that mentality is not good for patient care.”
Studies of Standards’ Effects
Few studies have been published specific to the hospital medicine experience with the reduced duty hours. Lin, et al., conducted four focus groups of internal medicine residents at the Washington University School of Medicine (St. Louis, Mo.), and found concerns about the effects of the duty hour restrictions on patient care and medical education.1 A study published this January in Academic Medicine by Dr. Vidyarthi and colleagues at UCSF asked 164 internal medicine residents to rate the value of their educational activities, frequency of administrative tasks interfering with education, and their educational satisfaction after duty hours were reduced.2 Dr. Vidyarthi and her coauthors did not see an increase in educational satisfaction, which was one of the expected outcomes of the new duty hour restrictions. She believes that for educational satisfaction among residents to increase, additional structural changes also must be put in place.
“If this is really an educational endeavor, then we need to make it such,” she says. “Duty hour decreases are here, so let’s make this amount of time that [the residents] are spending in the hospital as educationally valuable as possible.”
Can Less Be More?
One effect of reduced resident availability is that hospital medicine programs must become more thoughtful about the content of the educational experience for residents. If residents will see fewer patients because of fewer hours on duty, how might the remaining patient contacts be maximized for their educational opportunities?
“I think that there is much room for making their time in the hospital as educationally valuable as possible,” asserts Dr. Vidyarthi, “from pedagogical ways of thinking about medicine, to decreasing the number of tasks that they do that are not educational in value.”
Dr. Dressler agrees. “By reducing the resident work hours, we definitely reduce the amount of patient contact by residents,” he says. “Now, whether or not that will dramatically affect the amount of education the residents receive would be difficult to measure. Potentially, down the road, the American Board of Internal Medicine or some other governing board may decide that residency programs need to be longer. Medical training programs have instituted a comprehensive programmatic change [with the new work hours], will attempt to evaluate all the potential downsides as well as the value of this change, and, ultimately, will have to address problems or unexpected results in the new system in order to optimize patient care as well as physician trainee education.”
At California Pacific Medical Center’s residency program, “there are certain components we have had to re-analyze, and consider. [For example,] what is our core educational mandate that we’re trying to achieve? ” asks Dr. Baudendistel. Examining residents’ rotations, he says, has led to decisions to take residents off certain rotations, such as transplant nephrology, in favor of less esoteric rotations.
Hospitalists to the Rescue?
The question remains whether the reduced duty hours are better from the patient’s point of view. “The number of sign-outs that we’re seeing due to the duty hour decreases is significant. Interns will sign out approximately 300 times in a month, which is more than the number of patients they’ll see in the course of a year and, in fact, more often than they will eat in a month,” says Dr. Vidyarthi. “So, the challenge for the safety of patients [one of the impetuses for the decreased duty hours] is being balanced against having better rested, potentially better educated, happier residents. It’s really a Faustian bargain. Are we making this bargain [for better-rested residents] such that patients will, in fact, not be safer, because of the sign outs?”
Concerns about continuity of care under the new standard are “reasonable and legitimate,” says Dr. Dressler. “From a hospital medicine standpoint, that is how we practice: We are frequently handing off care. We understand that there is an inherent potential risk of doing that, and we like to be able to teach and train residents and students to understand how to do that effectively as part of their practice. Because hospitalists do this daily, we have an understanding of how to train people to optimally handoff patients to other clinicians and/or transition patients to other care settings or the outpatient arena.”
Dr. Dow views his hospitalist group as a sort of a “free safety,” taking care of patients that residents may not be able to take care of. “I view hospitalists as problem-solvers. Whether it’s a specific patient with a medical or social need, or a system problem, our big role is in filling those needs,” he says. “When patients need to be admitted and no other group is available, my hospitalist group is ready to care for folks.” TH
Gretchen Henkel is based in California.
References:
- Lin GA, Beck DC, Garbutt JM. Residents’ perceptions of the effects of work hour limitations at a large teaching hospital. Acad Med. 2006 Jan;81(1):63-67.
- Vidyarthi AR, Katz PP, Wall SD, et al. Impact of reduced duty hours on residents’ educational satisfaction at the University of California, San Francisco. Acad Med. 2006 Jan;81(1):76-81.
Take Research Initiative
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.

Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.

Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.
Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.
Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.
Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.
Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
Tough Negotiations Avert B.C. Hospitalist Walkout
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
Show us the Money
At a hefty 291 pages, SHM’s 2005-2006 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” contains a wealth of detail about hospitalists and their working conditions. Most readers will probably first refer to the compensation and benefits package statistics. But take a closer look: The survey’s chapters and tables yield a depth of even more helpful information.
After reviewing the survey’s “Executive Summary” (available online at the SHM Web site, www.hospitalmedicine.org), Charlene Carroll Clark, MD, a hospitalist at Inpatient Care Service at Good Samaritan Regional Medical Center in Corvallis, Ore., says “I think knowledge is always a good thing. Just knowing what is going on in other locations helps us. We can see that we fit right in with the median compensation, and that we are competitive as we recruit.”
It is reassuring, other sources concurred, to see that their hospitalist groups compare favorably with national median salaries and benefits packages. However, some group leaders caution that hospitalists should not benchmark their groups’ professional viability using only compensation and benefits medians. The real worth of the survey’s statistics, they say, will be realized when hospitalists utilize the document as a tool for improving management and care processes at their own institutions.
Indeed, in conversations with SHM leaders and with hospitalists across the country, it becomes clear that the survey has multiple uses, depending on its readers’ specific characteristics. And that’s just what SHM intends, says Joe Miller, SHM senior vice president, who was in charge of the survey project. “Our role was to create more of an almanac and a reference, rather than furnish an interpretation,” says Miller. “I think the real value for people will be in finding the metrics that are descriptive of their particular program.”
Survey Participation Increases
Miller is gratified by the increase in participation since the 2003-2004 SHM survey. Two years ago approximately 300 hospital medicine group (HMG) leaders participated in the survey. This time 396 HMG leaders participated—a 32% increase. Individual hospitalists completing the survey increased by more than 500 over the previous survey to a total of 2,550 individual hospitalist respondents.
“Given the magnitude of this survey, I think we’ve got very impressive representation of the industry,” says Miller. For instance, the regional representation of respondents was almost equally divided: 24% from the East, 26% from the South, 27% from the Midwest, and 22% from the West.
Miller attributes the greater participation to a variety of factors: conducting a multifaceted communication campaign, targeting every SHM board member and committee member, and extending the survey deadline.
An Eclectic and Thriving Group
According to Miller, the survey reveals many characteristics about hospitalists and the profession in general. While some of the results may not be surprising, they serve to corroborate (with real numbers) what many have perceived anecdotally about the hospital medicine movement. For instance:
- The hospital medicine movement is diverse. The survey documents six different models for hospital medicine programs. Currently, 34% of hospitalists are employed by hospitals or hospital corporations, and 12% are employed by local hospitalist-only groups. Multistate hospitalist-only groups or management companies employ 19%, while multi-specialty groups employ 14% of hospitalists. Academic hospital medicine programs employ 20%, and another 2% are employed by emergency or critical care physician groups.
- Hospitalists provide documented value for their hospitals, including around-the-clock patient care (51% of HMGs have on-site providers at night, and 41% of programs provide hospitalists on call), and participation in quality improvement (86%), hospital committees (92%), and other value-added activities, such as implementing information technology (54%).
- Other trends emerge when comparing 2003-2004 survey results with the current survey, including an increase in HMGs that now use a hybrid coverage schedule (a combination of shift and call schedules; an increase to 35% from 27%); more groups being paid using a mixed compensation model (a combination of salary and productive/performance-based compensation; up to 67% from 47% in 2003-2004); and a slight increase in hospitalists employed by academic institutions—up to 20% from a prior 16%.
Value Added


The survey also underscores hospitalists’ roles as change leaders in their institutions. In the “non-clinical activities” section of Chapter 3, “The Work of Hospital Medicine Groups,” results reveal high participation in hospital committees (92%), in quality improvement initiatives (86%); and other activities, such as generating practice guidelines, teaching, planning, and research.
John A. Bolinger, DO, FACP, medical director of the hospitalist program at Terre Haute (Ind.) Regional Hospital, serves on multiple committees at his hospital: critical care, pharmacy therapeutics, patient safety, credentials (as chair), and the executive committee. He and his hospital’s clinical pharmacist have developed standardized order sets, a new IV insulin protocol, and a new DVT prophylaxis protocol.
“I think participation in non-clinical activities is a plus for the hospitalist profession,” he says. In addition, “every hospital with a hospitalist involved in practice sees a tremendous benefit from that very thing.”
The Devil’s in the Details
John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, and cofounder and past president of SHM, was one of three panelists at the recent annual meeting where survey results were presented. Dr. Nelson believes that the statistics “can be a kind of starting point for thinking about whether your workload and compensation are typical. However,” he cautions, “the mistake I see so often is that people tend to think the average compensation, the average workload, are right for a given practice. Well, there are very few practices that are average. The variation is dramatic, and there’s no reason you should be average.”
Dr. Nelson advises hospitalists and group leaders not to interpret the compensation medians in the survey as a “final authority” for what hospitalists should be earning. Rather, he says, “what you could do is look at the big picture of an average practice—in terms of compensation, productivity, and other factors, such as location, whether your practice is primary adult or pediatric—and then compare your practice to see how you differ.
“Do you work harder and make less? In that case, you might want to fix it. If you work less and make more, you might want to be quiet!” he quips.
Brian Bossard, MD, medical director of Inpatient Physician Associates, a group of 15 hospitalists and two nurse coordinators that contracts with Bryan LGH hospital in Lincoln, Neb., to provide hospitalist services, agrees with Dr. Nelson’s characterization of the survey results as “a starting point.” While Dr. Bossard declined to state specifics about his group’s compensation figures, he did say that the median total compensation for non-leader physician hospitalists ($168,000 per year) was “about what I would expect it to be if you combine all hospitalists.”
He says that the numbers listed for HMG leaders was more reliable because leader roles are not quite as variable as non-leader roles. The survey shows that HMG leaders typically make $12,000 more annually than non-leader hospitalists, and that they tend to do less clinical work.
“It is also important to caution everyone in this area, too: This survey has not established the correct salary for a group leader—it varies tremendously,” reiterates Dr. Nelson.
In his role as HMG director, Dr. Bossard finds the survey’s work hours and work productivity data more valuable than compensation medians. “The number of hours per shift [median, 10.8] is very useful as a guide, I think, for someone who is starting a program or for someone like me, who knows what my numbers are,” he explains. “That—the median of 187 shifts per year; 10.8 hours per shift—provides an excellent target for new or established groups.”
Dr. Clark says that, in terms of pertinent data, the average number of encounters per hour was high on her list. Although that information is not highlighted in the survey’s “Executive Summary,” it is contained in Chapter 8, “Hospitalist Productivity.” Dr. Clark says this issue engenders an ongoing discussion with hospital administration.
“There are only so many patients you can see and provide excellent care, but there is a pull [from the administrative side] that they would like that number to be more,” she explains. “It’s nice to know what the average number of encounters is and what the society considers reasonable. I think it’s one of those things that we’re going to have to emphasize since the trade-off for seeing increased numbers of patients is to sacrifice quality patient care.”
Walter Bohnenblust, MD, is medical director of a hospitalist group at The Reading Hospital and Medical Center in West Reading, Pa. “What I like most about the survey is that productivity is represented not just with total billing, but with encounters and RVUs [relative value units]. We are in a low reimbursement area here, so if the survey included only gross charges and gross collections and not encounters plus RVUs, it would be more difficult in our market to justify to administration how hard we’re working. It’s uncanny how our group fits right in with the median in terms of productivity,” he says. “This gives me a baseline and more leverage with the administration, when they say we should be doing twice as many encounters as I think is reasonable.
“Like it or not, when someone is paying a subsidy for your service, they will try to get more out of you,” continues Dr. Bohnenblust. “It’s their job to try and get more out of the nurses and more out of the doctors. It’s not just us they’re picking on—the ER docs at our hospital have the same pressure. It’s good to have these numbers to go back and say, ‘Look, we are right where we should be [in terms of work productivity]. If you try and work us harder, you may lose some people and also not get out of the program what you wish.’”
Work productivity data provides an additional tool for recruitment, adds Dr. Bohnenblust, although he has not had much problem attracting new staff: “People are smart enough now to not only look at what [the prospective hospitalist group] income is, but how many patients they will have to see and what the work hours are.”
Uses of the Survey
Chapter 3, “The Work of Hospital Medicine Groups,” devotes attention to the types of non-clinical activities in which hospitalists participate. The section, say several sources, can also be a valuable negotiating tool with hospital administrators because it quantifies the amount of time hospitalists spend in such endeavors.
“One of the things that hospitalists add to inpatient care is that they have a greater presence all throughout the day in that facility,” says Timothy Bode, MD, medical director of Hospital Physician Services of Central Alabama. “And they’re a lot more involved with the medical staff, serving on committees, and involved in new processes and changes.
“To be able to see what kind of numbers are represented nationally, with hospitalists’ involvement in non-clinical activities, helps me with the hospitalists in my group,” he continues. “I can use these numbers to say, ‘This is a national trend. We need to be involved and we need to be leaders here as well, because that’s really the core of what we do.’ ”
Dr. Clark sees another important aspect of the hospitalist role: “ … participating on committees and QI initiatives and developing order sets, [which] can be additional and/or non-paid time. I think this needs to be recognized by hospitals in general, and physicians have to advocate for their value in this regard.”
The section on participation in non-clinical activities also drew praise from Dr. Bossard. “I don’t think this [percentage of time in non-clinical activities] would be necessary in terms of negotiating with the hospital, but it would be a very useful gauge for assessing where an individual program is relative to the rest of the programs, to see whether you are overdoing or under-representing yourself on committees.
“These surveys are just fabulous,” he says. “I’ve used the prior surveys to present information to the hospitals and identify how hard we’re working relative to our own region, and I present results to my hospitalist group in terms of pay and benefits. The survey is a wonderful tool.”
Academic Hospitalists Weigh In
Robert Wachter, MD, FACP, professor and associate chairman of the department of medicine at the University of California, San Francisco, and past president of SHM, also participated in the survey panel discussion and addresses issues specific to academic hospitalists. The growth in academic hospitalists shown in the current survey—while not surprising—confirms his impression that the field has grown in the last couple of years. The evidence of growth furnishes useful information for him as a hospitalist group leader in an academic institution.
“Unlike seven or eight years ago when I would be competing against only a handful of other academic programs for good people, I am now going to be competing against dozens and dozens of different groups,” he explains. “That changes the dynamic of my recruiting strategy.”
In addition, Dr. Wachter says he will make use of specific tables addressing concerns of academic hospitalists. “There are certain issues that are very different in an academic program, as compared to a community-based program,” he notes. “For instance, in my environment, burnout issues—or ‘dissatisfiers’—may relate to income or schedules or the abilities of support staff, but they may also relate to the teaching role or the research infrastructure—things that may be irrelevant to other people [in community programs] answering the surveys.”
Healthy Signs, Troubling Signs
Dr. Nelson summarizes his main points from the panel discussion about the survey: “It seems to show that incomes are rising faster than could be explained by inflation. There is also a rise in productivity, so incomes are up in part due to that.”
Another healthy trend, he says, is that in the last several surveys there has been a significant decline in hospitalists paid a fixed salary and an increase in those paid a combination of a base salary with a variable component, such as productivity. “I think getting away from fixed salaries is a good idea,” he notes.
Mary Jo Gorman, MD, MBA, SHM president and chief medical officer of IPC—The Hospitalist Company, was also a presenter during the survey’s debut in panel discussion. “Sustainability,” she says, is “very important for the field of hospital medicine. What this [survey] shows is that physicians are making a living, doing better than the average internist, and apparently getting career longevity out of this. Each year, the percentage of people who are staying in hospital medicine is increasing. New people are coming to the field, but other people are also staying. It’s not all about money and hours worked, but it’s some magical mixture of that.”
Dr. Bolinger agrees: “I definitely think that hospital medicine will sustain itself because we’re constantly setting the standard, and we’re showing the way it should be, the way it can be. As a profession, and as physicians, we are constantly striving to improve our quality of care. I think we are setting the mark for evidence-based medicine, and trying to encourage more evidence-based research.”
Dr. Bossard, who is based in Lincoln, Neb., found the 9% program turnover rate to be a relatively healthy sign, as did Dr. Wachter. “The turnover rates do not strike me as being incredibly high, given the portability of the field,” says Dr. Wachter. “We know very well that it is easier for hospitalists to pick up and leave their institutions for another one. In a primary care practice, changing practices involves a fair amount of work and a moderate amount of angst: You’re saying goodbye to all your patients and changing practice structure and style.”
One statistic did strike Dr. Bossard as potentially troubling, however: the increase in the percentage of hospitalists employed by multi-state hospitalist-only group or management companies from 9% in the 2003-2004 survey to 19% in the current survey.
“I think we’re seeing larger entities infiltrating markets and I’m not sure it’s a healthy trend for the hospitalist movement,” he says. “If you bring in physicians who do things a certain way, who may not have a commitment to a certain community, then I think you potentially lose some of the benefit of hospitalist programs. I think the finances will change. There will be a profit issue: Neither the hospital systems nor the hospitalist will see [that profit], and that’s a concerning trend to me.”
A Service to Members
Dr. Bohnenblust believes SHM truly serves its members by conducting the survey. The particular work environments and conditions of hospitalists can only be appreciated by a survey this specific, he says: “I applaud them for this [survey]. This is exactly what SHM needs to do to keep us viable as a profession.”
Dr. Wachter also believes the surveys are an invaluable tool.
“ … [Because we work in a] still-new field, we [hospitalists] are operating in a complex marketplace,” he says. “We are trying to figure out the best practices across all dimensions: schedules, organization structure, reporting relationships, funding. These kinds of surveys do not necessarily tell you the best practices, but they tell you about the prevalent practices. And I think that often is helpful in examining your own system and seeing whether it’s organized in the way you want to organize it. Having the society be the source of such information is a useful thing to do. It also helps the society design programs.”
The survey highlights many of the strengths of the growing hospital medicine movement. “I think in medicine in general there has been a frustration with having so much to do in so little time that it brings on stress,” says Dr. Bode. “When you can have a practice that devotes itself to one area, like the hospital, when you’re not running back and forth from the office to the hospital, you feel that you can really do a good job.
“I think most of the general population has no idea how the [healthcare] system works,” he continues. “To have a few minutes to spend telling patients how it works and how their care is flowing along is neat. You don’t feel that you have got to rush in and rush out all the time. The system can be so complex and frustrating for patients. When you can dive into the middle of it and try to streamline and demystify it, it’s really exciting.”
Conclusion
All survey participants received a free CD of the survey results. Copies of the CD as well as a booklet are available for purchase.
For more information on ordering “The Authoritative Source on the State of the Hospital Medicine Movement,” contact SHM at (800) 843-3360. TH
Gretchen Henkel writes regularly for The Hospitalist.
At a hefty 291 pages, SHM’s 2005-2006 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” contains a wealth of detail about hospitalists and their working conditions. Most readers will probably first refer to the compensation and benefits package statistics. But take a closer look: The survey’s chapters and tables yield a depth of even more helpful information.
After reviewing the survey’s “Executive Summary” (available online at the SHM Web site, www.hospitalmedicine.org), Charlene Carroll Clark, MD, a hospitalist at Inpatient Care Service at Good Samaritan Regional Medical Center in Corvallis, Ore., says “I think knowledge is always a good thing. Just knowing what is going on in other locations helps us. We can see that we fit right in with the median compensation, and that we are competitive as we recruit.”
It is reassuring, other sources concurred, to see that their hospitalist groups compare favorably with national median salaries and benefits packages. However, some group leaders caution that hospitalists should not benchmark their groups’ professional viability using only compensation and benefits medians. The real worth of the survey’s statistics, they say, will be realized when hospitalists utilize the document as a tool for improving management and care processes at their own institutions.
Indeed, in conversations with SHM leaders and with hospitalists across the country, it becomes clear that the survey has multiple uses, depending on its readers’ specific characteristics. And that’s just what SHM intends, says Joe Miller, SHM senior vice president, who was in charge of the survey project. “Our role was to create more of an almanac and a reference, rather than furnish an interpretation,” says Miller. “I think the real value for people will be in finding the metrics that are descriptive of their particular program.”
Survey Participation Increases
Miller is gratified by the increase in participation since the 2003-2004 SHM survey. Two years ago approximately 300 hospital medicine group (HMG) leaders participated in the survey. This time 396 HMG leaders participated—a 32% increase. Individual hospitalists completing the survey increased by more than 500 over the previous survey to a total of 2,550 individual hospitalist respondents.
“Given the magnitude of this survey, I think we’ve got very impressive representation of the industry,” says Miller. For instance, the regional representation of respondents was almost equally divided: 24% from the East, 26% from the South, 27% from the Midwest, and 22% from the West.
Miller attributes the greater participation to a variety of factors: conducting a multifaceted communication campaign, targeting every SHM board member and committee member, and extending the survey deadline.
An Eclectic and Thriving Group
According to Miller, the survey reveals many characteristics about hospitalists and the profession in general. While some of the results may not be surprising, they serve to corroborate (with real numbers) what many have perceived anecdotally about the hospital medicine movement. For instance:
- The hospital medicine movement is diverse. The survey documents six different models for hospital medicine programs. Currently, 34% of hospitalists are employed by hospitals or hospital corporations, and 12% are employed by local hospitalist-only groups. Multistate hospitalist-only groups or management companies employ 19%, while multi-specialty groups employ 14% of hospitalists. Academic hospital medicine programs employ 20%, and another 2% are employed by emergency or critical care physician groups.
- Hospitalists provide documented value for their hospitals, including around-the-clock patient care (51% of HMGs have on-site providers at night, and 41% of programs provide hospitalists on call), and participation in quality improvement (86%), hospital committees (92%), and other value-added activities, such as implementing information technology (54%).
- Other trends emerge when comparing 2003-2004 survey results with the current survey, including an increase in HMGs that now use a hybrid coverage schedule (a combination of shift and call schedules; an increase to 35% from 27%); more groups being paid using a mixed compensation model (a combination of salary and productive/performance-based compensation; up to 67% from 47% in 2003-2004); and a slight increase in hospitalists employed by academic institutions—up to 20% from a prior 16%.
Value Added
The survey also underscores hospitalists’ roles as change leaders in their institutions. In the “non-clinical activities” section of Chapter 3, “The Work of Hospital Medicine Groups,” results reveal high participation in hospital committees (92%), in quality improvement initiatives (86%); and other activities, such as generating practice guidelines, teaching, planning, and research.
John A. Bolinger, DO, FACP, medical director of the hospitalist program at Terre Haute (Ind.) Regional Hospital, serves on multiple committees at his hospital: critical care, pharmacy therapeutics, patient safety, credentials (as chair), and the executive committee. He and his hospital’s clinical pharmacist have developed standardized order sets, a new IV insulin protocol, and a new DVT prophylaxis protocol.
“I think participation in non-clinical activities is a plus for the hospitalist profession,” he says. In addition, “every hospital with a hospitalist involved in practice sees a tremendous benefit from that very thing.”
The Devil’s in the Details
John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, and cofounder and past president of SHM, was one of three panelists at the recent annual meeting where survey results were presented. Dr. Nelson believes that the statistics “can be a kind of starting point for thinking about whether your workload and compensation are typical. However,” he cautions, “the mistake I see so often is that people tend to think the average compensation, the average workload, are right for a given practice. Well, there are very few practices that are average. The variation is dramatic, and there’s no reason you should be average.”
Dr. Nelson advises hospitalists and group leaders not to interpret the compensation medians in the survey as a “final authority” for what hospitalists should be earning. Rather, he says, “what you could do is look at the big picture of an average practice—in terms of compensation, productivity, and other factors, such as location, whether your practice is primary adult or pediatric—and then compare your practice to see how you differ.
“Do you work harder and make less? In that case, you might want to fix it. If you work less and make more, you might want to be quiet!” he quips.
Brian Bossard, MD, medical director of Inpatient Physician Associates, a group of 15 hospitalists and two nurse coordinators that contracts with Bryan LGH hospital in Lincoln, Neb., to provide hospitalist services, agrees with Dr. Nelson’s characterization of the survey results as “a starting point.” While Dr. Bossard declined to state specifics about his group’s compensation figures, he did say that the median total compensation for non-leader physician hospitalists ($168,000 per year) was “about what I would expect it to be if you combine all hospitalists.”
He says that the numbers listed for HMG leaders was more reliable because leader roles are not quite as variable as non-leader roles. The survey shows that HMG leaders typically make $12,000 more annually than non-leader hospitalists, and that they tend to do less clinical work.
“It is also important to caution everyone in this area, too: This survey has not established the correct salary for a group leader—it varies tremendously,” reiterates Dr. Nelson.
In his role as HMG director, Dr. Bossard finds the survey’s work hours and work productivity data more valuable than compensation medians. “The number of hours per shift [median, 10.8] is very useful as a guide, I think, for someone who is starting a program or for someone like me, who knows what my numbers are,” he explains. “That—the median of 187 shifts per year; 10.8 hours per shift—provides an excellent target for new or established groups.”
Dr. Clark says that, in terms of pertinent data, the average number of encounters per hour was high on her list. Although that information is not highlighted in the survey’s “Executive Summary,” it is contained in Chapter 8, “Hospitalist Productivity.” Dr. Clark says this issue engenders an ongoing discussion with hospital administration.
“There are only so many patients you can see and provide excellent care, but there is a pull [from the administrative side] that they would like that number to be more,” she explains. “It’s nice to know what the average number of encounters is and what the society considers reasonable. I think it’s one of those things that we’re going to have to emphasize since the trade-off for seeing increased numbers of patients is to sacrifice quality patient care.”
Walter Bohnenblust, MD, is medical director of a hospitalist group at The Reading Hospital and Medical Center in West Reading, Pa. “What I like most about the survey is that productivity is represented not just with total billing, but with encounters and RVUs [relative value units]. We are in a low reimbursement area here, so if the survey included only gross charges and gross collections and not encounters plus RVUs, it would be more difficult in our market to justify to administration how hard we’re working. It’s uncanny how our group fits right in with the median in terms of productivity,” he says. “This gives me a baseline and more leverage with the administration, when they say we should be doing twice as many encounters as I think is reasonable.
“Like it or not, when someone is paying a subsidy for your service, they will try to get more out of you,” continues Dr. Bohnenblust. “It’s their job to try and get more out of the nurses and more out of the doctors. It’s not just us they’re picking on—the ER docs at our hospital have the same pressure. It’s good to have these numbers to go back and say, ‘Look, we are right where we should be [in terms of work productivity]. If you try and work us harder, you may lose some people and also not get out of the program what you wish.’”
Work productivity data provides an additional tool for recruitment, adds Dr. Bohnenblust, although he has not had much problem attracting new staff: “People are smart enough now to not only look at what [the prospective hospitalist group] income is, but how many patients they will have to see and what the work hours are.”
Uses of the Survey
Chapter 3, “The Work of Hospital Medicine Groups,” devotes attention to the types of non-clinical activities in which hospitalists participate. The section, say several sources, can also be a valuable negotiating tool with hospital administrators because it quantifies the amount of time hospitalists spend in such endeavors.
“One of the things that hospitalists add to inpatient care is that they have a greater presence all throughout the day in that facility,” says Timothy Bode, MD, medical director of Hospital Physician Services of Central Alabama. “And they’re a lot more involved with the medical staff, serving on committees, and involved in new processes and changes.
“To be able to see what kind of numbers are represented nationally, with hospitalists’ involvement in non-clinical activities, helps me with the hospitalists in my group,” he continues. “I can use these numbers to say, ‘This is a national trend. We need to be involved and we need to be leaders here as well, because that’s really the core of what we do.’ ”
Dr. Clark sees another important aspect of the hospitalist role: “ … participating on committees and QI initiatives and developing order sets, [which] can be additional and/or non-paid time. I think this needs to be recognized by hospitals in general, and physicians have to advocate for their value in this regard.”
The section on participation in non-clinical activities also drew praise from Dr. Bossard. “I don’t think this [percentage of time in non-clinical activities] would be necessary in terms of negotiating with the hospital, but it would be a very useful gauge for assessing where an individual program is relative to the rest of the programs, to see whether you are overdoing or under-representing yourself on committees.
“These surveys are just fabulous,” he says. “I’ve used the prior surveys to present information to the hospitals and identify how hard we’re working relative to our own region, and I present results to my hospitalist group in terms of pay and benefits. The survey is a wonderful tool.”
Academic Hospitalists Weigh In
Robert Wachter, MD, FACP, professor and associate chairman of the department of medicine at the University of California, San Francisco, and past president of SHM, also participated in the survey panel discussion and addresses issues specific to academic hospitalists. The growth in academic hospitalists shown in the current survey—while not surprising—confirms his impression that the field has grown in the last couple of years. The evidence of growth furnishes useful information for him as a hospitalist group leader in an academic institution.
“Unlike seven or eight years ago when I would be competing against only a handful of other academic programs for good people, I am now going to be competing against dozens and dozens of different groups,” he explains. “That changes the dynamic of my recruiting strategy.”
In addition, Dr. Wachter says he will make use of specific tables addressing concerns of academic hospitalists. “There are certain issues that are very different in an academic program, as compared to a community-based program,” he notes. “For instance, in my environment, burnout issues—or ‘dissatisfiers’—may relate to income or schedules or the abilities of support staff, but they may also relate to the teaching role or the research infrastructure—things that may be irrelevant to other people [in community programs] answering the surveys.”
Healthy Signs, Troubling Signs
Dr. Nelson summarizes his main points from the panel discussion about the survey: “It seems to show that incomes are rising faster than could be explained by inflation. There is also a rise in productivity, so incomes are up in part due to that.”
Another healthy trend, he says, is that in the last several surveys there has been a significant decline in hospitalists paid a fixed salary and an increase in those paid a combination of a base salary with a variable component, such as productivity. “I think getting away from fixed salaries is a good idea,” he notes.
Mary Jo Gorman, MD, MBA, SHM president and chief medical officer of IPC—The Hospitalist Company, was also a presenter during the survey’s debut in panel discussion. “Sustainability,” she says, is “very important for the field of hospital medicine. What this [survey] shows is that physicians are making a living, doing better than the average internist, and apparently getting career longevity out of this. Each year, the percentage of people who are staying in hospital medicine is increasing. New people are coming to the field, but other people are also staying. It’s not all about money and hours worked, but it’s some magical mixture of that.”
Dr. Bolinger agrees: “I definitely think that hospital medicine will sustain itself because we’re constantly setting the standard, and we’re showing the way it should be, the way it can be. As a profession, and as physicians, we are constantly striving to improve our quality of care. I think we are setting the mark for evidence-based medicine, and trying to encourage more evidence-based research.”
Dr. Bossard, who is based in Lincoln, Neb., found the 9% program turnover rate to be a relatively healthy sign, as did Dr. Wachter. “The turnover rates do not strike me as being incredibly high, given the portability of the field,” says Dr. Wachter. “We know very well that it is easier for hospitalists to pick up and leave their institutions for another one. In a primary care practice, changing practices involves a fair amount of work and a moderate amount of angst: You’re saying goodbye to all your patients and changing practice structure and style.”
One statistic did strike Dr. Bossard as potentially troubling, however: the increase in the percentage of hospitalists employed by multi-state hospitalist-only group or management companies from 9% in the 2003-2004 survey to 19% in the current survey.
“I think we’re seeing larger entities infiltrating markets and I’m not sure it’s a healthy trend for the hospitalist movement,” he says. “If you bring in physicians who do things a certain way, who may not have a commitment to a certain community, then I think you potentially lose some of the benefit of hospitalist programs. I think the finances will change. There will be a profit issue: Neither the hospital systems nor the hospitalist will see [that profit], and that’s a concerning trend to me.”
A Service to Members
Dr. Bohnenblust believes SHM truly serves its members by conducting the survey. The particular work environments and conditions of hospitalists can only be appreciated by a survey this specific, he says: “I applaud them for this [survey]. This is exactly what SHM needs to do to keep us viable as a profession.”
Dr. Wachter also believes the surveys are an invaluable tool.
“ … [Because we work in a] still-new field, we [hospitalists] are operating in a complex marketplace,” he says. “We are trying to figure out the best practices across all dimensions: schedules, organization structure, reporting relationships, funding. These kinds of surveys do not necessarily tell you the best practices, but they tell you about the prevalent practices. And I think that often is helpful in examining your own system and seeing whether it’s organized in the way you want to organize it. Having the society be the source of such information is a useful thing to do. It also helps the society design programs.”
The survey highlights many of the strengths of the growing hospital medicine movement. “I think in medicine in general there has been a frustration with having so much to do in so little time that it brings on stress,” says Dr. Bode. “When you can have a practice that devotes itself to one area, like the hospital, when you’re not running back and forth from the office to the hospital, you feel that you can really do a good job.
“I think most of the general population has no idea how the [healthcare] system works,” he continues. “To have a few minutes to spend telling patients how it works and how their care is flowing along is neat. You don’t feel that you have got to rush in and rush out all the time. The system can be so complex and frustrating for patients. When you can dive into the middle of it and try to streamline and demystify it, it’s really exciting.”
Conclusion
All survey participants received a free CD of the survey results. Copies of the CD as well as a booklet are available for purchase.
For more information on ordering “The Authoritative Source on the State of the Hospital Medicine Movement,” contact SHM at (800) 843-3360. TH
Gretchen Henkel writes regularly for The Hospitalist.
At a hefty 291 pages, SHM’s 2005-2006 survey, “The Authoritative Source on the State of the Hospital Medicine Movement,” contains a wealth of detail about hospitalists and their working conditions. Most readers will probably first refer to the compensation and benefits package statistics. But take a closer look: The survey’s chapters and tables yield a depth of even more helpful information.
After reviewing the survey’s “Executive Summary” (available online at the SHM Web site, www.hospitalmedicine.org), Charlene Carroll Clark, MD, a hospitalist at Inpatient Care Service at Good Samaritan Regional Medical Center in Corvallis, Ore., says “I think knowledge is always a good thing. Just knowing what is going on in other locations helps us. We can see that we fit right in with the median compensation, and that we are competitive as we recruit.”
It is reassuring, other sources concurred, to see that their hospitalist groups compare favorably with national median salaries and benefits packages. However, some group leaders caution that hospitalists should not benchmark their groups’ professional viability using only compensation and benefits medians. The real worth of the survey’s statistics, they say, will be realized when hospitalists utilize the document as a tool for improving management and care processes at their own institutions.
Indeed, in conversations with SHM leaders and with hospitalists across the country, it becomes clear that the survey has multiple uses, depending on its readers’ specific characteristics. And that’s just what SHM intends, says Joe Miller, SHM senior vice president, who was in charge of the survey project. “Our role was to create more of an almanac and a reference, rather than furnish an interpretation,” says Miller. “I think the real value for people will be in finding the metrics that are descriptive of their particular program.”
Survey Participation Increases
Miller is gratified by the increase in participation since the 2003-2004 SHM survey. Two years ago approximately 300 hospital medicine group (HMG) leaders participated in the survey. This time 396 HMG leaders participated—a 32% increase. Individual hospitalists completing the survey increased by more than 500 over the previous survey to a total of 2,550 individual hospitalist respondents.
“Given the magnitude of this survey, I think we’ve got very impressive representation of the industry,” says Miller. For instance, the regional representation of respondents was almost equally divided: 24% from the East, 26% from the South, 27% from the Midwest, and 22% from the West.
Miller attributes the greater participation to a variety of factors: conducting a multifaceted communication campaign, targeting every SHM board member and committee member, and extending the survey deadline.
An Eclectic and Thriving Group
According to Miller, the survey reveals many characteristics about hospitalists and the profession in general. While some of the results may not be surprising, they serve to corroborate (with real numbers) what many have perceived anecdotally about the hospital medicine movement. For instance:
- The hospital medicine movement is diverse. The survey documents six different models for hospital medicine programs. Currently, 34% of hospitalists are employed by hospitals or hospital corporations, and 12% are employed by local hospitalist-only groups. Multistate hospitalist-only groups or management companies employ 19%, while multi-specialty groups employ 14% of hospitalists. Academic hospital medicine programs employ 20%, and another 2% are employed by emergency or critical care physician groups.
- Hospitalists provide documented value for their hospitals, including around-the-clock patient care (51% of HMGs have on-site providers at night, and 41% of programs provide hospitalists on call), and participation in quality improvement (86%), hospital committees (92%), and other value-added activities, such as implementing information technology (54%).
- Other trends emerge when comparing 2003-2004 survey results with the current survey, including an increase in HMGs that now use a hybrid coverage schedule (a combination of shift and call schedules; an increase to 35% from 27%); more groups being paid using a mixed compensation model (a combination of salary and productive/performance-based compensation; up to 67% from 47% in 2003-2004); and a slight increase in hospitalists employed by academic institutions—up to 20% from a prior 16%.
Value Added
The survey also underscores hospitalists’ roles as change leaders in their institutions. In the “non-clinical activities” section of Chapter 3, “The Work of Hospital Medicine Groups,” results reveal high participation in hospital committees (92%), in quality improvement initiatives (86%); and other activities, such as generating practice guidelines, teaching, planning, and research.
John A. Bolinger, DO, FACP, medical director of the hospitalist program at Terre Haute (Ind.) Regional Hospital, serves on multiple committees at his hospital: critical care, pharmacy therapeutics, patient safety, credentials (as chair), and the executive committee. He and his hospital’s clinical pharmacist have developed standardized order sets, a new IV insulin protocol, and a new DVT prophylaxis protocol.
“I think participation in non-clinical activities is a plus for the hospitalist profession,” he says. In addition, “every hospital with a hospitalist involved in practice sees a tremendous benefit from that very thing.”
The Devil’s in the Details
John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, and cofounder and past president of SHM, was one of three panelists at the recent annual meeting where survey results were presented. Dr. Nelson believes that the statistics “can be a kind of starting point for thinking about whether your workload and compensation are typical. However,” he cautions, “the mistake I see so often is that people tend to think the average compensation, the average workload, are right for a given practice. Well, there are very few practices that are average. The variation is dramatic, and there’s no reason you should be average.”
Dr. Nelson advises hospitalists and group leaders not to interpret the compensation medians in the survey as a “final authority” for what hospitalists should be earning. Rather, he says, “what you could do is look at the big picture of an average practice—in terms of compensation, productivity, and other factors, such as location, whether your practice is primary adult or pediatric—and then compare your practice to see how you differ.
“Do you work harder and make less? In that case, you might want to fix it. If you work less and make more, you might want to be quiet!” he quips.
Brian Bossard, MD, medical director of Inpatient Physician Associates, a group of 15 hospitalists and two nurse coordinators that contracts with Bryan LGH hospital in Lincoln, Neb., to provide hospitalist services, agrees with Dr. Nelson’s characterization of the survey results as “a starting point.” While Dr. Bossard declined to state specifics about his group’s compensation figures, he did say that the median total compensation for non-leader physician hospitalists ($168,000 per year) was “about what I would expect it to be if you combine all hospitalists.”
He says that the numbers listed for HMG leaders was more reliable because leader roles are not quite as variable as non-leader roles. The survey shows that HMG leaders typically make $12,000 more annually than non-leader hospitalists, and that they tend to do less clinical work.
“It is also important to caution everyone in this area, too: This survey has not established the correct salary for a group leader—it varies tremendously,” reiterates Dr. Nelson.
In his role as HMG director, Dr. Bossard finds the survey’s work hours and work productivity data more valuable than compensation medians. “The number of hours per shift [median, 10.8] is very useful as a guide, I think, for someone who is starting a program or for someone like me, who knows what my numbers are,” he explains. “That—the median of 187 shifts per year; 10.8 hours per shift—provides an excellent target for new or established groups.”
Dr. Clark says that, in terms of pertinent data, the average number of encounters per hour was high on her list. Although that information is not highlighted in the survey’s “Executive Summary,” it is contained in Chapter 8, “Hospitalist Productivity.” Dr. Clark says this issue engenders an ongoing discussion with hospital administration.
“There are only so many patients you can see and provide excellent care, but there is a pull [from the administrative side] that they would like that number to be more,” she explains. “It’s nice to know what the average number of encounters is and what the society considers reasonable. I think it’s one of those things that we’re going to have to emphasize since the trade-off for seeing increased numbers of patients is to sacrifice quality patient care.”
Walter Bohnenblust, MD, is medical director of a hospitalist group at The Reading Hospital and Medical Center in West Reading, Pa. “What I like most about the survey is that productivity is represented not just with total billing, but with encounters and RVUs [relative value units]. We are in a low reimbursement area here, so if the survey included only gross charges and gross collections and not encounters plus RVUs, it would be more difficult in our market to justify to administration how hard we’re working. It’s uncanny how our group fits right in with the median in terms of productivity,” he says. “This gives me a baseline and more leverage with the administration, when they say we should be doing twice as many encounters as I think is reasonable.
“Like it or not, when someone is paying a subsidy for your service, they will try to get more out of you,” continues Dr. Bohnenblust. “It’s their job to try and get more out of the nurses and more out of the doctors. It’s not just us they’re picking on—the ER docs at our hospital have the same pressure. It’s good to have these numbers to go back and say, ‘Look, we are right where we should be [in terms of work productivity]. If you try and work us harder, you may lose some people and also not get out of the program what you wish.’”
Work productivity data provides an additional tool for recruitment, adds Dr. Bohnenblust, although he has not had much problem attracting new staff: “People are smart enough now to not only look at what [the prospective hospitalist group] income is, but how many patients they will have to see and what the work hours are.”
Uses of the Survey
Chapter 3, “The Work of Hospital Medicine Groups,” devotes attention to the types of non-clinical activities in which hospitalists participate. The section, say several sources, can also be a valuable negotiating tool with hospital administrators because it quantifies the amount of time hospitalists spend in such endeavors.
“One of the things that hospitalists add to inpatient care is that they have a greater presence all throughout the day in that facility,” says Timothy Bode, MD, medical director of Hospital Physician Services of Central Alabama. “And they’re a lot more involved with the medical staff, serving on committees, and involved in new processes and changes.
“To be able to see what kind of numbers are represented nationally, with hospitalists’ involvement in non-clinical activities, helps me with the hospitalists in my group,” he continues. “I can use these numbers to say, ‘This is a national trend. We need to be involved and we need to be leaders here as well, because that’s really the core of what we do.’ ”
Dr. Clark sees another important aspect of the hospitalist role: “ … participating on committees and QI initiatives and developing order sets, [which] can be additional and/or non-paid time. I think this needs to be recognized by hospitals in general, and physicians have to advocate for their value in this regard.”
The section on participation in non-clinical activities also drew praise from Dr. Bossard. “I don’t think this [percentage of time in non-clinical activities] would be necessary in terms of negotiating with the hospital, but it would be a very useful gauge for assessing where an individual program is relative to the rest of the programs, to see whether you are overdoing or under-representing yourself on committees.
“These surveys are just fabulous,” he says. “I’ve used the prior surveys to present information to the hospitals and identify how hard we’re working relative to our own region, and I present results to my hospitalist group in terms of pay and benefits. The survey is a wonderful tool.”
Academic Hospitalists Weigh In
Robert Wachter, MD, FACP, professor and associate chairman of the department of medicine at the University of California, San Francisco, and past president of SHM, also participated in the survey panel discussion and addresses issues specific to academic hospitalists. The growth in academic hospitalists shown in the current survey—while not surprising—confirms his impression that the field has grown in the last couple of years. The evidence of growth furnishes useful information for him as a hospitalist group leader in an academic institution.
“Unlike seven or eight years ago when I would be competing against only a handful of other academic programs for good people, I am now going to be competing against dozens and dozens of different groups,” he explains. “That changes the dynamic of my recruiting strategy.”
In addition, Dr. Wachter says he will make use of specific tables addressing concerns of academic hospitalists. “There are certain issues that are very different in an academic program, as compared to a community-based program,” he notes. “For instance, in my environment, burnout issues—or ‘dissatisfiers’—may relate to income or schedules or the abilities of support staff, but they may also relate to the teaching role or the research infrastructure—things that may be irrelevant to other people [in community programs] answering the surveys.”
Healthy Signs, Troubling Signs
Dr. Nelson summarizes his main points from the panel discussion about the survey: “It seems to show that incomes are rising faster than could be explained by inflation. There is also a rise in productivity, so incomes are up in part due to that.”
Another healthy trend, he says, is that in the last several surveys there has been a significant decline in hospitalists paid a fixed salary and an increase in those paid a combination of a base salary with a variable component, such as productivity. “I think getting away from fixed salaries is a good idea,” he notes.
Mary Jo Gorman, MD, MBA, SHM president and chief medical officer of IPC—The Hospitalist Company, was also a presenter during the survey’s debut in panel discussion. “Sustainability,” she says, is “very important for the field of hospital medicine. What this [survey] shows is that physicians are making a living, doing better than the average internist, and apparently getting career longevity out of this. Each year, the percentage of people who are staying in hospital medicine is increasing. New people are coming to the field, but other people are also staying. It’s not all about money and hours worked, but it’s some magical mixture of that.”
Dr. Bolinger agrees: “I definitely think that hospital medicine will sustain itself because we’re constantly setting the standard, and we’re showing the way it should be, the way it can be. As a profession, and as physicians, we are constantly striving to improve our quality of care. I think we are setting the mark for evidence-based medicine, and trying to encourage more evidence-based research.”
Dr. Bossard, who is based in Lincoln, Neb., found the 9% program turnover rate to be a relatively healthy sign, as did Dr. Wachter. “The turnover rates do not strike me as being incredibly high, given the portability of the field,” says Dr. Wachter. “We know very well that it is easier for hospitalists to pick up and leave their institutions for another one. In a primary care practice, changing practices involves a fair amount of work and a moderate amount of angst: You’re saying goodbye to all your patients and changing practice structure and style.”
One statistic did strike Dr. Bossard as potentially troubling, however: the increase in the percentage of hospitalists employed by multi-state hospitalist-only group or management companies from 9% in the 2003-2004 survey to 19% in the current survey.
“I think we’re seeing larger entities infiltrating markets and I’m not sure it’s a healthy trend for the hospitalist movement,” he says. “If you bring in physicians who do things a certain way, who may not have a commitment to a certain community, then I think you potentially lose some of the benefit of hospitalist programs. I think the finances will change. There will be a profit issue: Neither the hospital systems nor the hospitalist will see [that profit], and that’s a concerning trend to me.”
A Service to Members
Dr. Bohnenblust believes SHM truly serves its members by conducting the survey. The particular work environments and conditions of hospitalists can only be appreciated by a survey this specific, he says: “I applaud them for this [survey]. This is exactly what SHM needs to do to keep us viable as a profession.”
Dr. Wachter also believes the surveys are an invaluable tool.
“ … [Because we work in a] still-new field, we [hospitalists] are operating in a complex marketplace,” he says. “We are trying to figure out the best practices across all dimensions: schedules, organization structure, reporting relationships, funding. These kinds of surveys do not necessarily tell you the best practices, but they tell you about the prevalent practices. And I think that often is helpful in examining your own system and seeing whether it’s organized in the way you want to organize it. Having the society be the source of such information is a useful thing to do. It also helps the society design programs.”
The survey highlights many of the strengths of the growing hospital medicine movement. “I think in medicine in general there has been a frustration with having so much to do in so little time that it brings on stress,” says Dr. Bode. “When you can have a practice that devotes itself to one area, like the hospital, when you’re not running back and forth from the office to the hospital, you feel that you can really do a good job.
“I think most of the general population has no idea how the [healthcare] system works,” he continues. “To have a few minutes to spend telling patients how it works and how their care is flowing along is neat. You don’t feel that you have got to rush in and rush out all the time. The system can be so complex and frustrating for patients. When you can dive into the middle of it and try to streamline and demystify it, it’s really exciting.”
Conclusion
All survey participants received a free CD of the survey results. Copies of the CD as well as a booklet are available for purchase.
For more information on ordering “The Authoritative Source on the State of the Hospital Medicine Movement,” contact SHM at (800) 843-3360. TH
Gretchen Henkel writes regularly for The Hospitalist.
Palliative Consult
Hospital-based palliative care programs are gaining traction in the United States as studies show their efficacy in decreasing length of stay and improved quality of patient care.1,2 According to the American Hospital Association, 22% of all U.S. hospitals now have such programs.3 These programs—with their emphasis on coordinated, team-delivered care and communication—seem tailor-made for the expertise of hospitalists who are increasingly taking the lead to establish them at their institutions.
Through the SHM Web site (www.hospitalmedicine.org) and the Center to Advance Palliative Care (www.capc.org) ample resources exist for developing program infrastructure and acquiring on-site training (see www.capc.org/palliative-care-leadershipinitiative/overview).
There are unwritten protocols, however, that can make or break a palliative care service. Hospitalists involved with palliative care often find themselves relating to oncologists because many patients who have palliative care needs are undergoing inpatient curative treatments (such as brachytherapy) or are actively dying. Palliative care experts interviewed for this article agreed that in order to encourage referrals from their oncology colleagues, hospitalists must be attentive to oncologists’ concerns and to consultation etiquette.
“Palliative care has been something that oncologists traditionally think they do pretty well,” says David H. Lawson, MD, section chief, Medical Oncology at Emory Clinic. “I think there will be a lot of variability between oncologists about what they see as their province and what they see as open for someone else.”
—Diane E. Meier, MD
Assessing Oncologists’ Needs
During the organizational phase of a hospital-based palliative care service, it is advisable to meet with oncologists one-on-one, believes Charles F. von Gunten, MD, PhD, medical director of the Palliative Care Consultation Service at the University of California, San Diego, and director of the Center for Palliative Studies at San Diego Hospice and Palliative Care. “All consult services are fundamentally about providing advice to the managing physician when requested, about what is requested, and nothing else.”
He recommends that hospitalists involved in development of a hospital-based palliative care service find out how key oncologists at their hospital perceive the needs in the area of palliative care. “This may not match what the hospitalist thinks the oncologist needs, but that’s immaterial,” he cautions.
This advice squares with that of Steve Pantilat, MD, immediate past-president of SHM, and his team at the University of California, San Francisco. The palliative care service at UCSF is one of six Palliative Care Leadership Centers nationwide, so designated during an initiative launched two years ago by the Center to Advance Palliative Care. (The Robert Wood Johnson Foundation underwrites training activities at the six centers.) The issue in establishing palliative care services, says Dr. Pantilat, is “figuring out what would attract oncologists about such a program. What issues are most salient to them? Instead of saying, ‘I have a new service; would you please use it?’ You have to come in and say, ‘We’re thinking of starting this new service; how can we be of help to you?’ ”
Dr. Lawson agrees with Dr. von Gunten and Dr. Pantilat that hospitalists must develop communication with oncologists early during the start-up phase of a palliative care service. Hospitalists who offer palliative care services should also take time to familiarize themselves with patients’ treatment plans.
“I think there is going to be a learning curve for palliative care specialists,” says Dr. Lawson. “Part of that learning is to get some sense of how oncologists make decisions about whether to give chemo[therapy] or not. Oftentimes, there are pressures that might not be obvious.”
For instance, it may appear to a palliative care consultant that a certain patient should not undergo chemotherapy, but in fact the patient or the family may demand it.
Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, says the majority of consults she does are with oncology patients. She has found that attending Monday morning sign-out meetings with Emory oncologists has not only increased referrals to the palliative care service, but has added to her understanding of oncologists’ decision-making processes.
“When I go to weekly meetings, I hear the full spectrum of what they are doing. I see how oncologists work and how they decide about treatments,” she says. “It’s been a really good experience because I never would have seen this from the hospitalist viewpoint.”
Emory’s palliative care program was launched in November 2005 and has grown so quickly that they already need additional staff.
The Primary Client
The “key message” for a hospitalist when asked to do a palliative care consult is to remember that the client of a consultation service is the referring physician, points out geriatrician Diane E. Meier, MD, director of the Center to Advance Palliative Care and the director of the Hertzberg Palliative Care Institute at Mount Sinai School of Medicine in New York City. “As a geriatrician, if I call in an infectious disease consultant, I’m calling that physician to help me make decisions about my patient—not for that person to take over the care of my patient or to undermine my relationship to that patient. This is basic consultation etiquette, but physicians are often not taught in medical school or residency the difference between a primary care responsibility and a consultation responsibility.”
“The biggest mistake that people make in putting together palliative care services,” concurs Dr. von Gunten, “is thinking that the patient is the client. That isn’t true. It is the person requesting the consultation—meaning, the referring physician or the managing service. The patient is the secondary beneficiary.
“The language we use—‘my patient’—is fundamental to the practice of American medicine,” explains Dr. von Gunten. You have to respect that. If you go to someone’s home, you don’t redecorate it because you don’t like their taste. You do not comment on their choice of draperies or their choice of food. The same applies to medical consultations.” (See “Consult Etiquette for Palliative Care Services,” p. 33.)
Oncologists generally feel “very possessive” about their patients, adds Dr. von Gunten. Even though oncologists are technically also consultants (to the patient’s primary care physician), the pattern in American medicine is that oncologists treating patients acquire the status of a primary care physician. “So,” he says, “you treat them with that kind of respect, which means that you ask permission before you do things, and you don’t disparage what they are doing—either to their faces or to their patients or to other bystanders like nurses.”
Dr. Lawson agrees that oncologists often have a strong personal bond with their patients. “These personal feelings are often reciprocated by the patients and families,” he says. “Accepting another person [the hospitalist as palliative care consultant] into the equation can be difficult at times, even more so while the patient is still in the hospital and the oncologist is still around.”
The palliative care program at Emory is consult-driven. “The doctor has to agree to us getting involved, so I don’t get into territorial issues,” says Dr. Grossman. “When I do get involved with patients, the oncologists welcome me taking care of them and realize the benefit of what I’m doing. They see that my approach is collaborative.”
Dr. Grossman has been able to offer services to oncologists whose patients are receiving chemotherapy and experiencing significant symptoms, such as pain. When hospitalists on the hospital medicine service consult her about cancer patients, she calls the primary oncologist to familiarize herself with the patient’s background and to check if other treatments are available.
Strengths of Hospitalists
Palliative care should be distinguished from hospice or end-of-life care, although it can be concurrent. Palliative care needs—ranging from symptom management to alleviating psychological suffering—can exist at any point along the cancer care trajectory, notes Dr. von Gunten, who was a co-developer with Dr. Pantilat and others of the California Hospital Initiative in Palliative Services program to assist hospitals to develop palliative services.4
Hospitalists, says Dr. von Gunten, already possess some of the baseline skills needed to deliver palliative care: They’re based in the hospital and so have the opportunity to interact with patients and their families; they are experienced in hospital-based management of patients; they are experienced in teamwork with other providers also based in the hospital. The ability to be available to patients and physicians 24/7 is a real advantage in symptom management, says Dr. Lawson.
Because hospitalists by definition care for people who are not their primary care patients, the sophistication and sensitivity about working with one’s colleagues “is already inculcated,” observes Dr. Meier. In addition, “hospitalists understand that their responsibility to and relationship with the patient is only one piece of being a good doctor. Ensuring good care for a patient means very high level and high intensity communications with everyone involved in that patient’s care: all the other specialists, the primary care physician, and the floor team—the social workers, nurses, certified nursing assistants, dietary staff, and rehab and physiatry staff. Unless everyone is reading from the same page, the patient’s care will not be good. Very often, it’s the hospitalist or palliative care consultant who is at the center of the wheel, making sure that all the spokes are getting the same message,” she says.
Busy oncologists may call upon Dr. Grossman’s service to conduct family meetings about care plans. “Patients are very loyal to their oncologists, and they want their oncologists to be supportive of their decisions,” she notes. “I always explain to patients that my consultation was requested or supported by their oncologist. I am not there to cause more barriers; I’m there to have everybody on board and to understand where the patient is. We call everybody in—the social worker, the nurse, chaplaincy staff—because our approach is interdisciplinary and these are the essential members of our team.”
Dr. Grossman believes that hospitalists’ training in teamwork and communications are key to providing a good experience for oncology patients and their families. She is board certified in palliative care, which allows her to bring additional expertise to symptom support, including situations where she can help the dying process be as peaceful as possible—for both patient and family.
The issues important in palliative care—availability to patients, families, and referring physicians, ability to work in teams, and quality of care—dovetail with the primary goals of hospital medicine. Hospitalists’ palliative care services can thrive when they forge strong foundational relationships with their referring colleagues. TH
Gretchen Henkel regularly contributes to The Hospitalist.
References
- Selwyn PA, Rivard M, Kappell D, et al. Palliative care for AIDS at a large urban teaching hospital: program description and preliminary outcomes. J Palliat Med. 2003 Jun;6(3):461-474.
- Ryan A, Carter J, Lucas J, Berger J. You need not make the journey alone: overcoming impediments to providing palliative care in a public urban teaching hospital. Am J Hosp Palliat Care. 2002 May-June;19(3):171-180.
- The Case for Hospital-Based Palliative Care, published by the Center to Advance Palliative Care. Available online at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Last accessed March 22, 2006.
- Pantilat SZ, Rabow MW, Citko J, et al. Evaluating the California Hospital Initiative in Palliative Services. Arch Intern Med. 2006 Jan 23;166(2):227-230.
Hospital-based palliative care programs are gaining traction in the United States as studies show their efficacy in decreasing length of stay and improved quality of patient care.1,2 According to the American Hospital Association, 22% of all U.S. hospitals now have such programs.3 These programs—with their emphasis on coordinated, team-delivered care and communication—seem tailor-made for the expertise of hospitalists who are increasingly taking the lead to establish them at their institutions.
Through the SHM Web site (www.hospitalmedicine.org) and the Center to Advance Palliative Care (www.capc.org) ample resources exist for developing program infrastructure and acquiring on-site training (see www.capc.org/palliative-care-leadershipinitiative/overview).
There are unwritten protocols, however, that can make or break a palliative care service. Hospitalists involved with palliative care often find themselves relating to oncologists because many patients who have palliative care needs are undergoing inpatient curative treatments (such as brachytherapy) or are actively dying. Palliative care experts interviewed for this article agreed that in order to encourage referrals from their oncology colleagues, hospitalists must be attentive to oncologists’ concerns and to consultation etiquette.
“Palliative care has been something that oncologists traditionally think they do pretty well,” says David H. Lawson, MD, section chief, Medical Oncology at Emory Clinic. “I think there will be a lot of variability between oncologists about what they see as their province and what they see as open for someone else.”
—Diane E. Meier, MD
Assessing Oncologists’ Needs
During the organizational phase of a hospital-based palliative care service, it is advisable to meet with oncologists one-on-one, believes Charles F. von Gunten, MD, PhD, medical director of the Palliative Care Consultation Service at the University of California, San Diego, and director of the Center for Palliative Studies at San Diego Hospice and Palliative Care. “All consult services are fundamentally about providing advice to the managing physician when requested, about what is requested, and nothing else.”
He recommends that hospitalists involved in development of a hospital-based palliative care service find out how key oncologists at their hospital perceive the needs in the area of palliative care. “This may not match what the hospitalist thinks the oncologist needs, but that’s immaterial,” he cautions.
This advice squares with that of Steve Pantilat, MD, immediate past-president of SHM, and his team at the University of California, San Francisco. The palliative care service at UCSF is one of six Palliative Care Leadership Centers nationwide, so designated during an initiative launched two years ago by the Center to Advance Palliative Care. (The Robert Wood Johnson Foundation underwrites training activities at the six centers.) The issue in establishing palliative care services, says Dr. Pantilat, is “figuring out what would attract oncologists about such a program. What issues are most salient to them? Instead of saying, ‘I have a new service; would you please use it?’ You have to come in and say, ‘We’re thinking of starting this new service; how can we be of help to you?’ ”
Dr. Lawson agrees with Dr. von Gunten and Dr. Pantilat that hospitalists must develop communication with oncologists early during the start-up phase of a palliative care service. Hospitalists who offer palliative care services should also take time to familiarize themselves with patients’ treatment plans.
“I think there is going to be a learning curve for palliative care specialists,” says Dr. Lawson. “Part of that learning is to get some sense of how oncologists make decisions about whether to give chemo[therapy] or not. Oftentimes, there are pressures that might not be obvious.”
For instance, it may appear to a palliative care consultant that a certain patient should not undergo chemotherapy, but in fact the patient or the family may demand it.
Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, says the majority of consults she does are with oncology patients. She has found that attending Monday morning sign-out meetings with Emory oncologists has not only increased referrals to the palliative care service, but has added to her understanding of oncologists’ decision-making processes.
“When I go to weekly meetings, I hear the full spectrum of what they are doing. I see how oncologists work and how they decide about treatments,” she says. “It’s been a really good experience because I never would have seen this from the hospitalist viewpoint.”
Emory’s palliative care program was launched in November 2005 and has grown so quickly that they already need additional staff.
The Primary Client
The “key message” for a hospitalist when asked to do a palliative care consult is to remember that the client of a consultation service is the referring physician, points out geriatrician Diane E. Meier, MD, director of the Center to Advance Palliative Care and the director of the Hertzberg Palliative Care Institute at Mount Sinai School of Medicine in New York City. “As a geriatrician, if I call in an infectious disease consultant, I’m calling that physician to help me make decisions about my patient—not for that person to take over the care of my patient or to undermine my relationship to that patient. This is basic consultation etiquette, but physicians are often not taught in medical school or residency the difference between a primary care responsibility and a consultation responsibility.”
“The biggest mistake that people make in putting together palliative care services,” concurs Dr. von Gunten, “is thinking that the patient is the client. That isn’t true. It is the person requesting the consultation—meaning, the referring physician or the managing service. The patient is the secondary beneficiary.
“The language we use—‘my patient’—is fundamental to the practice of American medicine,” explains Dr. von Gunten. You have to respect that. If you go to someone’s home, you don’t redecorate it because you don’t like their taste. You do not comment on their choice of draperies or their choice of food. The same applies to medical consultations.” (See “Consult Etiquette for Palliative Care Services,” p. 33.)
Oncologists generally feel “very possessive” about their patients, adds Dr. von Gunten. Even though oncologists are technically also consultants (to the patient’s primary care physician), the pattern in American medicine is that oncologists treating patients acquire the status of a primary care physician. “So,” he says, “you treat them with that kind of respect, which means that you ask permission before you do things, and you don’t disparage what they are doing—either to their faces or to their patients or to other bystanders like nurses.”
Dr. Lawson agrees that oncologists often have a strong personal bond with their patients. “These personal feelings are often reciprocated by the patients and families,” he says. “Accepting another person [the hospitalist as palliative care consultant] into the equation can be difficult at times, even more so while the patient is still in the hospital and the oncologist is still around.”
The palliative care program at Emory is consult-driven. “The doctor has to agree to us getting involved, so I don’t get into territorial issues,” says Dr. Grossman. “When I do get involved with patients, the oncologists welcome me taking care of them and realize the benefit of what I’m doing. They see that my approach is collaborative.”
Dr. Grossman has been able to offer services to oncologists whose patients are receiving chemotherapy and experiencing significant symptoms, such as pain. When hospitalists on the hospital medicine service consult her about cancer patients, she calls the primary oncologist to familiarize herself with the patient’s background and to check if other treatments are available.
Strengths of Hospitalists
Palliative care should be distinguished from hospice or end-of-life care, although it can be concurrent. Palliative care needs—ranging from symptom management to alleviating psychological suffering—can exist at any point along the cancer care trajectory, notes Dr. von Gunten, who was a co-developer with Dr. Pantilat and others of the California Hospital Initiative in Palliative Services program to assist hospitals to develop palliative services.4
Hospitalists, says Dr. von Gunten, already possess some of the baseline skills needed to deliver palliative care: They’re based in the hospital and so have the opportunity to interact with patients and their families; they are experienced in hospital-based management of patients; they are experienced in teamwork with other providers also based in the hospital. The ability to be available to patients and physicians 24/7 is a real advantage in symptom management, says Dr. Lawson.
Because hospitalists by definition care for people who are not their primary care patients, the sophistication and sensitivity about working with one’s colleagues “is already inculcated,” observes Dr. Meier. In addition, “hospitalists understand that their responsibility to and relationship with the patient is only one piece of being a good doctor. Ensuring good care for a patient means very high level and high intensity communications with everyone involved in that patient’s care: all the other specialists, the primary care physician, and the floor team—the social workers, nurses, certified nursing assistants, dietary staff, and rehab and physiatry staff. Unless everyone is reading from the same page, the patient’s care will not be good. Very often, it’s the hospitalist or palliative care consultant who is at the center of the wheel, making sure that all the spokes are getting the same message,” she says.
Busy oncologists may call upon Dr. Grossman’s service to conduct family meetings about care plans. “Patients are very loyal to their oncologists, and they want their oncologists to be supportive of their decisions,” she notes. “I always explain to patients that my consultation was requested or supported by their oncologist. I am not there to cause more barriers; I’m there to have everybody on board and to understand where the patient is. We call everybody in—the social worker, the nurse, chaplaincy staff—because our approach is interdisciplinary and these are the essential members of our team.”
Dr. Grossman believes that hospitalists’ training in teamwork and communications are key to providing a good experience for oncology patients and their families. She is board certified in palliative care, which allows her to bring additional expertise to symptom support, including situations where she can help the dying process be as peaceful as possible—for both patient and family.
The issues important in palliative care—availability to patients, families, and referring physicians, ability to work in teams, and quality of care—dovetail with the primary goals of hospital medicine. Hospitalists’ palliative care services can thrive when they forge strong foundational relationships with their referring colleagues. TH
Gretchen Henkel regularly contributes to The Hospitalist.
References
- Selwyn PA, Rivard M, Kappell D, et al. Palliative care for AIDS at a large urban teaching hospital: program description and preliminary outcomes. J Palliat Med. 2003 Jun;6(3):461-474.
- Ryan A, Carter J, Lucas J, Berger J. You need not make the journey alone: overcoming impediments to providing palliative care in a public urban teaching hospital. Am J Hosp Palliat Care. 2002 May-June;19(3):171-180.
- The Case for Hospital-Based Palliative Care, published by the Center to Advance Palliative Care. Available online at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Last accessed March 22, 2006.
- Pantilat SZ, Rabow MW, Citko J, et al. Evaluating the California Hospital Initiative in Palliative Services. Arch Intern Med. 2006 Jan 23;166(2):227-230.
Hospital-based palliative care programs are gaining traction in the United States as studies show their efficacy in decreasing length of stay and improved quality of patient care.1,2 According to the American Hospital Association, 22% of all U.S. hospitals now have such programs.3 These programs—with their emphasis on coordinated, team-delivered care and communication—seem tailor-made for the expertise of hospitalists who are increasingly taking the lead to establish them at their institutions.
Through the SHM Web site (www.hospitalmedicine.org) and the Center to Advance Palliative Care (www.capc.org) ample resources exist for developing program infrastructure and acquiring on-site training (see www.capc.org/palliative-care-leadershipinitiative/overview).
There are unwritten protocols, however, that can make or break a palliative care service. Hospitalists involved with palliative care often find themselves relating to oncologists because many patients who have palliative care needs are undergoing inpatient curative treatments (such as brachytherapy) or are actively dying. Palliative care experts interviewed for this article agreed that in order to encourage referrals from their oncology colleagues, hospitalists must be attentive to oncologists’ concerns and to consultation etiquette.
“Palliative care has been something that oncologists traditionally think they do pretty well,” says David H. Lawson, MD, section chief, Medical Oncology at Emory Clinic. “I think there will be a lot of variability between oncologists about what they see as their province and what they see as open for someone else.”
—Diane E. Meier, MD
Assessing Oncologists’ Needs
During the organizational phase of a hospital-based palliative care service, it is advisable to meet with oncologists one-on-one, believes Charles F. von Gunten, MD, PhD, medical director of the Palliative Care Consultation Service at the University of California, San Diego, and director of the Center for Palliative Studies at San Diego Hospice and Palliative Care. “All consult services are fundamentally about providing advice to the managing physician when requested, about what is requested, and nothing else.”
He recommends that hospitalists involved in development of a hospital-based palliative care service find out how key oncologists at their hospital perceive the needs in the area of palliative care. “This may not match what the hospitalist thinks the oncologist needs, but that’s immaterial,” he cautions.
This advice squares with that of Steve Pantilat, MD, immediate past-president of SHM, and his team at the University of California, San Francisco. The palliative care service at UCSF is one of six Palliative Care Leadership Centers nationwide, so designated during an initiative launched two years ago by the Center to Advance Palliative Care. (The Robert Wood Johnson Foundation underwrites training activities at the six centers.) The issue in establishing palliative care services, says Dr. Pantilat, is “figuring out what would attract oncologists about such a program. What issues are most salient to them? Instead of saying, ‘I have a new service; would you please use it?’ You have to come in and say, ‘We’re thinking of starting this new service; how can we be of help to you?’ ”
Dr. Lawson agrees with Dr. von Gunten and Dr. Pantilat that hospitalists must develop communication with oncologists early during the start-up phase of a palliative care service. Hospitalists who offer palliative care services should also take time to familiarize themselves with patients’ treatment plans.
“I think there is going to be a learning curve for palliative care specialists,” says Dr. Lawson. “Part of that learning is to get some sense of how oncologists make decisions about whether to give chemo[therapy] or not. Oftentimes, there are pressures that might not be obvious.”
For instance, it may appear to a palliative care consultant that a certain patient should not undergo chemotherapy, but in fact the patient or the family may demand it.
Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, says the majority of consults she does are with oncology patients. She has found that attending Monday morning sign-out meetings with Emory oncologists has not only increased referrals to the palliative care service, but has added to her understanding of oncologists’ decision-making processes.
“When I go to weekly meetings, I hear the full spectrum of what they are doing. I see how oncologists work and how they decide about treatments,” she says. “It’s been a really good experience because I never would have seen this from the hospitalist viewpoint.”
Emory’s palliative care program was launched in November 2005 and has grown so quickly that they already need additional staff.
The Primary Client
The “key message” for a hospitalist when asked to do a palliative care consult is to remember that the client of a consultation service is the referring physician, points out geriatrician Diane E. Meier, MD, director of the Center to Advance Palliative Care and the director of the Hertzberg Palliative Care Institute at Mount Sinai School of Medicine in New York City. “As a geriatrician, if I call in an infectious disease consultant, I’m calling that physician to help me make decisions about my patient—not for that person to take over the care of my patient or to undermine my relationship to that patient. This is basic consultation etiquette, but physicians are often not taught in medical school or residency the difference between a primary care responsibility and a consultation responsibility.”
“The biggest mistake that people make in putting together palliative care services,” concurs Dr. von Gunten, “is thinking that the patient is the client. That isn’t true. It is the person requesting the consultation—meaning, the referring physician or the managing service. The patient is the secondary beneficiary.
“The language we use—‘my patient’—is fundamental to the practice of American medicine,” explains Dr. von Gunten. You have to respect that. If you go to someone’s home, you don’t redecorate it because you don’t like their taste. You do not comment on their choice of draperies or their choice of food. The same applies to medical consultations.” (See “Consult Etiquette for Palliative Care Services,” p. 33.)
Oncologists generally feel “very possessive” about their patients, adds Dr. von Gunten. Even though oncologists are technically also consultants (to the patient’s primary care physician), the pattern in American medicine is that oncologists treating patients acquire the status of a primary care physician. “So,” he says, “you treat them with that kind of respect, which means that you ask permission before you do things, and you don’t disparage what they are doing—either to their faces or to their patients or to other bystanders like nurses.”
Dr. Lawson agrees that oncologists often have a strong personal bond with their patients. “These personal feelings are often reciprocated by the patients and families,” he says. “Accepting another person [the hospitalist as palliative care consultant] into the equation can be difficult at times, even more so while the patient is still in the hospital and the oncologist is still around.”
The palliative care program at Emory is consult-driven. “The doctor has to agree to us getting involved, so I don’t get into territorial issues,” says Dr. Grossman. “When I do get involved with patients, the oncologists welcome me taking care of them and realize the benefit of what I’m doing. They see that my approach is collaborative.”
Dr. Grossman has been able to offer services to oncologists whose patients are receiving chemotherapy and experiencing significant symptoms, such as pain. When hospitalists on the hospital medicine service consult her about cancer patients, she calls the primary oncologist to familiarize herself with the patient’s background and to check if other treatments are available.
Strengths of Hospitalists
Palliative care should be distinguished from hospice or end-of-life care, although it can be concurrent. Palliative care needs—ranging from symptom management to alleviating psychological suffering—can exist at any point along the cancer care trajectory, notes Dr. von Gunten, who was a co-developer with Dr. Pantilat and others of the California Hospital Initiative in Palliative Services program to assist hospitals to develop palliative services.4
Hospitalists, says Dr. von Gunten, already possess some of the baseline skills needed to deliver palliative care: They’re based in the hospital and so have the opportunity to interact with patients and their families; they are experienced in hospital-based management of patients; they are experienced in teamwork with other providers also based in the hospital. The ability to be available to patients and physicians 24/7 is a real advantage in symptom management, says Dr. Lawson.
Because hospitalists by definition care for people who are not their primary care patients, the sophistication and sensitivity about working with one’s colleagues “is already inculcated,” observes Dr. Meier. In addition, “hospitalists understand that their responsibility to and relationship with the patient is only one piece of being a good doctor. Ensuring good care for a patient means very high level and high intensity communications with everyone involved in that patient’s care: all the other specialists, the primary care physician, and the floor team—the social workers, nurses, certified nursing assistants, dietary staff, and rehab and physiatry staff. Unless everyone is reading from the same page, the patient’s care will not be good. Very often, it’s the hospitalist or palliative care consultant who is at the center of the wheel, making sure that all the spokes are getting the same message,” she says.
Busy oncologists may call upon Dr. Grossman’s service to conduct family meetings about care plans. “Patients are very loyal to their oncologists, and they want their oncologists to be supportive of their decisions,” she notes. “I always explain to patients that my consultation was requested or supported by their oncologist. I am not there to cause more barriers; I’m there to have everybody on board and to understand where the patient is. We call everybody in—the social worker, the nurse, chaplaincy staff—because our approach is interdisciplinary and these are the essential members of our team.”
Dr. Grossman believes that hospitalists’ training in teamwork and communications are key to providing a good experience for oncology patients and their families. She is board certified in palliative care, which allows her to bring additional expertise to symptom support, including situations where she can help the dying process be as peaceful as possible—for both patient and family.
The issues important in palliative care—availability to patients, families, and referring physicians, ability to work in teams, and quality of care—dovetail with the primary goals of hospital medicine. Hospitalists’ palliative care services can thrive when they forge strong foundational relationships with their referring colleagues. TH
Gretchen Henkel regularly contributes to The Hospitalist.
References
- Selwyn PA, Rivard M, Kappell D, et al. Palliative care for AIDS at a large urban teaching hospital: program description and preliminary outcomes. J Palliat Med. 2003 Jun;6(3):461-474.
- Ryan A, Carter J, Lucas J, Berger J. You need not make the journey alone: overcoming impediments to providing palliative care in a public urban teaching hospital. Am J Hosp Palliat Care. 2002 May-June;19(3):171-180.
- The Case for Hospital-Based Palliative Care, published by the Center to Advance Palliative Care. Available online at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Last accessed March 22, 2006.
- Pantilat SZ, Rabow MW, Citko J, et al. Evaluating the California Hospital Initiative in Palliative Services. Arch Intern Med. 2006 Jan 23;166(2):227-230.
Invaluable Assistants
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team—from the team members’ points of view. Each installment of “Alliances” provides valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Several months ago, a patient with decompensated end-stage liver disease was admitted to the Internal Medicine Hospitalist Service at the University of Texas Medical Branch in Galveston and required a paracentesis. One of the new hospitalist faculty members was taken aback when the physician assistant (PA) on the service volunteered to do the procedure. “He was surprised,” says Karen Kislingbury, PA-C, a member of SHM’s Non-Physician Provider Task Force and a PA with the Internal Medicine Hospitalist Service, “that the scope of practice for the physician assistant included [performing] procedures.”
PAs are not new to the hospital setting, and their inclusion as physician extenders to increase patient access to care will likely increase in the current regulatory environment—especially state-mandated staff/patient ratios and resident work hour limitations. The efficacy of utilizing physician extenders to improve patient care and outcomes has been validated in studies over the past two decades. A recent Journal of Trauma study found statistically significant reductions in floor, ICU, and overall hospital lengths of stay after incorporating physician extenders into their trauma service.1
However, hospitalists unfamiliar with PAs may not understand their colleagues’ roles and scope of practice. As her anecdote illustrated, Kislingbury notes that “although PAs aren’t new to the healthcare delivery system, and physicians have been utilizing us for a long time, our partnership in the unique setting of hospital medicine is kind of new.”
Kislingbury’s colleague Ryan Genzink, PA-C, who works with Hospitalists of West Michigan, a private hospitalists-only group that subcontracts hospitalist services to Spectrum Health of Grand Rapids, Mich., agrees with her assessment.
“There are more and more PAs and [nurse practitioners] working in hospital medicine, and I think there is a lot of curiosity and some apprehension on the part of people who have not worked with these non-physician providers,” says Genzink.
Genzink, also a member of SHM’s Non-Physician Provider Task Force, speculates that the apprehension of physicians who have not worked with PAs may be due to a misunderstanding of the PA’s role. “They’re either underestimating or overestimating exactly what a PA can do or what they are getting when they hire a PA,” he says.
A Short History of the Profession
PA programs officially began in the mid-1960s at Duke University Medical School (Durham, N.C.). Eugene Stead, MD, is credited with developing the concept of the physician assistant as a health professional who would work with physician supervision to extend patient access to care, according to the American Academy of Physician Assistants.
For the first class of PAs in 1965, Dr. Stead selected Navy corpsmen who had received medical training and experience during their service in Vietnam. The curriculum was based on Dr. Stead’s knowledge of fast-track training of physicians during World War II. From this early program, the profession has evolved to more than 130 programs that now adhere to rigorous national accreditation standards set forth by the independent Accreditation Review Commission on Education for the Physician Assistant (ARC-PA). The ARC-PA is sponsored by the American Medical Association and the American College of Surgeons, among many other professional medical organizations (www.aapa.org/geninfo1.html).
Scope of Practice
Prerequisites to PA programs include two years of college courses in basic and behavioral science, as well as prior experience in healthcare. According to a report generated by the Association of Physician Assistant Programs, most PA students have earned a bachelor’s degree and have an average of 38 months of healthcare experience before being admitted to a PA program.2
The first year of PA education comprises a didactic curriculum with coursework in anatomy, physiology, biochemistry, pharmacology, physical diagnosis, pathophysiology, microbiology, clinical laboratory sciences, behavioral sciences, and medical ethics. In the second year, students receive hands-on clinical training through a series of rotations—typically in family and internal medicine, obstetrics and gynecology, pediatrics, general surgery, emergency medicine, and psychiatry. By the time they graduate (typical PA programs last an average of 26 months), PAs will have completed more than 2,000 hours of supervised clinical practice.
PAs work in all areas of medicine. Although hospital bylaws and state regulations often stipulate the PA’s scope of practice, the major determinant of duties is the supervising physician. The relationship between supervising physician and PA, says Kislingbury, is a collaborative one. Duties are “defined on an individual basis, and they are determined based on our [PAs’] experience, the physicians’ experience with us, and then the nuances of the system and the hospital itself.
“The PA who is hired should know what his or her scope of practice is,” she continues. “By the time they have graduated and obtained their license, they should know what their state allows them to do.”
For instance, according to the American Academy of Physician Assistants, 48 of the 50 states, plus the District of Columbia and [the U.S. Territory of] Guam, authorize PAs to prescribe medications. In California, PA prescriptions are referred to as “written prescription transmittal orders.”
“For the most part,” says Genzink, “the supervising physician determines what the PA is capable of doing, within the guidelines of state law.”
Within Genzink’s hospital medicine group (with which he has been affiliated for five years) the physician and PA roles are very similar.
“We see the same type of patients in a team approach. For instance, it’s not uncommon for one of us to order a test early in the day, and then, when results come back, the other person may be discharging that patient or prescribing other treatments, if necessary,” he explains. “In general, the physicians take care of the more complicated patients, while PAs take care of more routine patients.”
Genzink’s group experience aligns with findings of a 1998 University of Pittsburgh School of Nursing Study, which evaluated provider roles and patient outcomes in an acute care setting.3 Compared with acute care nurse practitioners and PAs, residents in that study tended to care for patients who were older and sicker.
Genzink reports that in his group initial histories and physicals, as well as the consultations, are performed exclusively by the PAs and then the physician takes over for treatment. “Based on the acuity of the patient,” says Genzink, “the physician may be right down there to see the patient immediately.”
Areas for Improvement?
Although the two PAs interviewed for this article report positive experiences working with hospitalists, they admit that some physicians continue to hold misperceptions about the PA’s role in caring for patients.
Kislingbury says that hospitalists could improve their delegation of duties to the PAs and recognize their scope of practice. She admits that delegation duties can be improved through gaining experience. “Although the PA profession has been around for a while, there are a surprising number of institutions that do not utilize physician assistants on the wards in routine rounds and bedside-type care,” says Kislingbury.
“I think some of the problems develop when they [physicians] hire a PA and expect to get a physician—and they [don’t],” says Genzink. “The easiest way for me to explain the role is to compare it to a teaching model. All physicians have been through residency programs. They understand the hierarchy that involves training and teaching residents. PAs come out of school ‘green,’ with the assumption that training will go on at the workplace. So, if a physician takes the same stance toward a new PA as they would toward an intern, that is a pretty close comparison.
“You begin by letting PAs or interns do a few simple things, and as they master those, you teach them more,” he continues. “And then, hopefully, over time they’ve been able to master everything that the physician is able to master. [Employing a PA] is a significant investment. And, it takes time. Sometimes, that process can be very easy, depending on the person. Sometimes it can be very slow, and I think that’s sometimes where some of the frustration may come in.”
Genzink adds that in his hospital medicine group, the physicians are familiar with the idea that part of their job as supervising physicians is to train new PAs.
Kislingbury points that out that PAs can also play a role in informing the physician team members about the range of cases they are allowed to treat, thus furthering the collaboration between PAs and hospitalists: “It is merely a matter of educating the team members about what we can and cannot do.”
Accordingly, the SHM Non-Physician Provider Task Force was formed to provide a resource to hospitalists who work with PAs and have questions about scope of practice, reimbursement, and other issues as they pertain to PAs and nurse practitioners. (Visit www.hospitalmedicine.org for more information.) The Task Force is a resource for non-physicians providers, too, offering educational opportunities at SHM meetings, more visibility with the specialty, and a voice for advocacy.
The Positives of the Collaboration
While the PAs report that hospitalists could improve in communicating about their practice roles with PAs, “There are so many things that hospitalists do right!” says Kislingbury. Calling the experience of working with hospitalists a privilege, she says that “where it is a true partnership, we are treated as equals, we are given the responsibility that our experience will allow, and we are truly team members.
“Hospitalists are geared into the efficiencies of the system and the nuances of the hospital. These are subtleties that come with practicing in an area for a long period of time, not just coming in for a month and then leaving and returning,” she says. “Hospitalists know the daily ins and outs, and it is really a pleasure to learn from them.”
Prior to his affiliation with Hospitalists of West Michigan, Genzink was employed directly by a hospital in Grand Rapids. The physicians with whom he now works have been hospitalists almost exclusively throughout their medical careers. “One of the main benefits they offer is availability, simply because we [the group’s practice members] are in the hospital 24/7,” he says. “They also have more experience in dealing with more complex issues, just as do the PAs that are working in our system.”
What about the notion that PAs and nurse practitioners are more skilled or practiced with patient and family communications? One study by Rudy, et al. found that nurse practitioners and PAs were more likely than residents to discuss patients with bedside nurses and to interact with patients’ families.3 Genzink does not find this to be the case in his group’s practice.
“That presumption [that PAs are more communicative with families and patients] may have come about simply because as the demands on hospitalists continue to grow and the workload increases, adding the PA to the team means there are more people to do things like that [handle family communications],” he says. “Certainly, in our group, the PAs do lots of patient education, and we talk to patients about end-of-life issues and other difficult matters as well. But that is not delegated to them; in our group, both the PAs and the physicians participate equally in patient and family communication.”
Daily Learning
Hospitalists and PAs also complement each other in the interdisciplinary care team because, “as a general rule, hospitalists love to teach,” says Kislingbury. “They don’t forget that just because you have your PA degree your learning does not stop there. The PA profession is almost like on-the-job training. You are allowed to choose the specialty that you want, and you gain your experience when you enter that [arena], as opposed to an internship or residency, where you first gain experience and then enter the specialty. We so appreciate the ability of the hospitalist to teach because we are learning while doing, on a day-to-day basis. It’s invaluable to have their teaching.” TH
Gretchen Henkel also writes about dealing with difficult families in this issue.
Resources
- Christmas AB, Reynolds J, Hodges S, et al. Physician extenders impact trauma systems. J Trauma. 2005 May;58(5):917-920.
- Nineteenth Annual Report on Physician Assistant Educational Programs in the United States, 2002-2203. Alexandria, Va. Association of Physician Assistant Programs.
- Rudy EB, Davidson LJ, Daly B, et al. Care activities and outcomes of patients cared for by acute care nurse practitioners, physician assistants, and resident physicians: a comparison. Am J Crit Care. 1998 Jul;7(4):267-281.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team—from the team members’ points of view. Each installment of “Alliances” provides valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Several months ago, a patient with decompensated end-stage liver disease was admitted to the Internal Medicine Hospitalist Service at the University of Texas Medical Branch in Galveston and required a paracentesis. One of the new hospitalist faculty members was taken aback when the physician assistant (PA) on the service volunteered to do the procedure. “He was surprised,” says Karen Kislingbury, PA-C, a member of SHM’s Non-Physician Provider Task Force and a PA with the Internal Medicine Hospitalist Service, “that the scope of practice for the physician assistant included [performing] procedures.”
PAs are not new to the hospital setting, and their inclusion as physician extenders to increase patient access to care will likely increase in the current regulatory environment—especially state-mandated staff/patient ratios and resident work hour limitations. The efficacy of utilizing physician extenders to improve patient care and outcomes has been validated in studies over the past two decades. A recent Journal of Trauma study found statistically significant reductions in floor, ICU, and overall hospital lengths of stay after incorporating physician extenders into their trauma service.1
However, hospitalists unfamiliar with PAs may not understand their colleagues’ roles and scope of practice. As her anecdote illustrated, Kislingbury notes that “although PAs aren’t new to the healthcare delivery system, and physicians have been utilizing us for a long time, our partnership in the unique setting of hospital medicine is kind of new.”
Kislingbury’s colleague Ryan Genzink, PA-C, who works with Hospitalists of West Michigan, a private hospitalists-only group that subcontracts hospitalist services to Spectrum Health of Grand Rapids, Mich., agrees with her assessment.
“There are more and more PAs and [nurse practitioners] working in hospital medicine, and I think there is a lot of curiosity and some apprehension on the part of people who have not worked with these non-physician providers,” says Genzink.
Genzink, also a member of SHM’s Non-Physician Provider Task Force, speculates that the apprehension of physicians who have not worked with PAs may be due to a misunderstanding of the PA’s role. “They’re either underestimating or overestimating exactly what a PA can do or what they are getting when they hire a PA,” he says.
A Short History of the Profession
PA programs officially began in the mid-1960s at Duke University Medical School (Durham, N.C.). Eugene Stead, MD, is credited with developing the concept of the physician assistant as a health professional who would work with physician supervision to extend patient access to care, according to the American Academy of Physician Assistants.
For the first class of PAs in 1965, Dr. Stead selected Navy corpsmen who had received medical training and experience during their service in Vietnam. The curriculum was based on Dr. Stead’s knowledge of fast-track training of physicians during World War II. From this early program, the profession has evolved to more than 130 programs that now adhere to rigorous national accreditation standards set forth by the independent Accreditation Review Commission on Education for the Physician Assistant (ARC-PA). The ARC-PA is sponsored by the American Medical Association and the American College of Surgeons, among many other professional medical organizations (www.aapa.org/geninfo1.html).
Scope of Practice
Prerequisites to PA programs include two years of college courses in basic and behavioral science, as well as prior experience in healthcare. According to a report generated by the Association of Physician Assistant Programs, most PA students have earned a bachelor’s degree and have an average of 38 months of healthcare experience before being admitted to a PA program.2
The first year of PA education comprises a didactic curriculum with coursework in anatomy, physiology, biochemistry, pharmacology, physical diagnosis, pathophysiology, microbiology, clinical laboratory sciences, behavioral sciences, and medical ethics. In the second year, students receive hands-on clinical training through a series of rotations—typically in family and internal medicine, obstetrics and gynecology, pediatrics, general surgery, emergency medicine, and psychiatry. By the time they graduate (typical PA programs last an average of 26 months), PAs will have completed more than 2,000 hours of supervised clinical practice.
PAs work in all areas of medicine. Although hospital bylaws and state regulations often stipulate the PA’s scope of practice, the major determinant of duties is the supervising physician. The relationship between supervising physician and PA, says Kislingbury, is a collaborative one. Duties are “defined on an individual basis, and they are determined based on our [PAs’] experience, the physicians’ experience with us, and then the nuances of the system and the hospital itself.
“The PA who is hired should know what his or her scope of practice is,” she continues. “By the time they have graduated and obtained their license, they should know what their state allows them to do.”
For instance, according to the American Academy of Physician Assistants, 48 of the 50 states, plus the District of Columbia and [the U.S. Territory of] Guam, authorize PAs to prescribe medications. In California, PA prescriptions are referred to as “written prescription transmittal orders.”
“For the most part,” says Genzink, “the supervising physician determines what the PA is capable of doing, within the guidelines of state law.”
Within Genzink’s hospital medicine group (with which he has been affiliated for five years) the physician and PA roles are very similar.
“We see the same type of patients in a team approach. For instance, it’s not uncommon for one of us to order a test early in the day, and then, when results come back, the other person may be discharging that patient or prescribing other treatments, if necessary,” he explains. “In general, the physicians take care of the more complicated patients, while PAs take care of more routine patients.”
Genzink’s group experience aligns with findings of a 1998 University of Pittsburgh School of Nursing Study, which evaluated provider roles and patient outcomes in an acute care setting.3 Compared with acute care nurse practitioners and PAs, residents in that study tended to care for patients who were older and sicker.
Genzink reports that in his group initial histories and physicals, as well as the consultations, are performed exclusively by the PAs and then the physician takes over for treatment. “Based on the acuity of the patient,” says Genzink, “the physician may be right down there to see the patient immediately.”
Areas for Improvement?
Although the two PAs interviewed for this article report positive experiences working with hospitalists, they admit that some physicians continue to hold misperceptions about the PA’s role in caring for patients.
Kislingbury says that hospitalists could improve their delegation of duties to the PAs and recognize their scope of practice. She admits that delegation duties can be improved through gaining experience. “Although the PA profession has been around for a while, there are a surprising number of institutions that do not utilize physician assistants on the wards in routine rounds and bedside-type care,” says Kislingbury.
“I think some of the problems develop when they [physicians] hire a PA and expect to get a physician—and they [don’t],” says Genzink. “The easiest way for me to explain the role is to compare it to a teaching model. All physicians have been through residency programs. They understand the hierarchy that involves training and teaching residents. PAs come out of school ‘green,’ with the assumption that training will go on at the workplace. So, if a physician takes the same stance toward a new PA as they would toward an intern, that is a pretty close comparison.
“You begin by letting PAs or interns do a few simple things, and as they master those, you teach them more,” he continues. “And then, hopefully, over time they’ve been able to master everything that the physician is able to master. [Employing a PA] is a significant investment. And, it takes time. Sometimes, that process can be very easy, depending on the person. Sometimes it can be very slow, and I think that’s sometimes where some of the frustration may come in.”
Genzink adds that in his hospital medicine group, the physicians are familiar with the idea that part of their job as supervising physicians is to train new PAs.
Kislingbury points that out that PAs can also play a role in informing the physician team members about the range of cases they are allowed to treat, thus furthering the collaboration between PAs and hospitalists: “It is merely a matter of educating the team members about what we can and cannot do.”
Accordingly, the SHM Non-Physician Provider Task Force was formed to provide a resource to hospitalists who work with PAs and have questions about scope of practice, reimbursement, and other issues as they pertain to PAs and nurse practitioners. (Visit www.hospitalmedicine.org for more information.) The Task Force is a resource for non-physicians providers, too, offering educational opportunities at SHM meetings, more visibility with the specialty, and a voice for advocacy.
The Positives of the Collaboration
While the PAs report that hospitalists could improve in communicating about their practice roles with PAs, “There are so many things that hospitalists do right!” says Kislingbury. Calling the experience of working with hospitalists a privilege, she says that “where it is a true partnership, we are treated as equals, we are given the responsibility that our experience will allow, and we are truly team members.
“Hospitalists are geared into the efficiencies of the system and the nuances of the hospital. These are subtleties that come with practicing in an area for a long period of time, not just coming in for a month and then leaving and returning,” she says. “Hospitalists know the daily ins and outs, and it is really a pleasure to learn from them.”
Prior to his affiliation with Hospitalists of West Michigan, Genzink was employed directly by a hospital in Grand Rapids. The physicians with whom he now works have been hospitalists almost exclusively throughout their medical careers. “One of the main benefits they offer is availability, simply because we [the group’s practice members] are in the hospital 24/7,” he says. “They also have more experience in dealing with more complex issues, just as do the PAs that are working in our system.”
What about the notion that PAs and nurse practitioners are more skilled or practiced with patient and family communications? One study by Rudy, et al. found that nurse practitioners and PAs were more likely than residents to discuss patients with bedside nurses and to interact with patients’ families.3 Genzink does not find this to be the case in his group’s practice.
“That presumption [that PAs are more communicative with families and patients] may have come about simply because as the demands on hospitalists continue to grow and the workload increases, adding the PA to the team means there are more people to do things like that [handle family communications],” he says. “Certainly, in our group, the PAs do lots of patient education, and we talk to patients about end-of-life issues and other difficult matters as well. But that is not delegated to them; in our group, both the PAs and the physicians participate equally in patient and family communication.”
Daily Learning
Hospitalists and PAs also complement each other in the interdisciplinary care team because, “as a general rule, hospitalists love to teach,” says Kislingbury. “They don’t forget that just because you have your PA degree your learning does not stop there. The PA profession is almost like on-the-job training. You are allowed to choose the specialty that you want, and you gain your experience when you enter that [arena], as opposed to an internship or residency, where you first gain experience and then enter the specialty. We so appreciate the ability of the hospitalist to teach because we are learning while doing, on a day-to-day basis. It’s invaluable to have their teaching.” TH
Gretchen Henkel also writes about dealing with difficult families in this issue.
Resources
- Christmas AB, Reynolds J, Hodges S, et al. Physician extenders impact trauma systems. J Trauma. 2005 May;58(5):917-920.
- Nineteenth Annual Report on Physician Assistant Educational Programs in the United States, 2002-2203. Alexandria, Va. Association of Physician Assistant Programs.
- Rudy EB, Davidson LJ, Daly B, et al. Care activities and outcomes of patients cared for by acute care nurse practitioners, physician assistants, and resident physicians: a comparison. Am J Crit Care. 1998 Jul;7(4):267-281.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team—from the team members’ points of view. Each installment of “Alliances” provides valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Several months ago, a patient with decompensated end-stage liver disease was admitted to the Internal Medicine Hospitalist Service at the University of Texas Medical Branch in Galveston and required a paracentesis. One of the new hospitalist faculty members was taken aback when the physician assistant (PA) on the service volunteered to do the procedure. “He was surprised,” says Karen Kislingbury, PA-C, a member of SHM’s Non-Physician Provider Task Force and a PA with the Internal Medicine Hospitalist Service, “that the scope of practice for the physician assistant included [performing] procedures.”
PAs are not new to the hospital setting, and their inclusion as physician extenders to increase patient access to care will likely increase in the current regulatory environment—especially state-mandated staff/patient ratios and resident work hour limitations. The efficacy of utilizing physician extenders to improve patient care and outcomes has been validated in studies over the past two decades. A recent Journal of Trauma study found statistically significant reductions in floor, ICU, and overall hospital lengths of stay after incorporating physician extenders into their trauma service.1
However, hospitalists unfamiliar with PAs may not understand their colleagues’ roles and scope of practice. As her anecdote illustrated, Kislingbury notes that “although PAs aren’t new to the healthcare delivery system, and physicians have been utilizing us for a long time, our partnership in the unique setting of hospital medicine is kind of new.”
Kislingbury’s colleague Ryan Genzink, PA-C, who works with Hospitalists of West Michigan, a private hospitalists-only group that subcontracts hospitalist services to Spectrum Health of Grand Rapids, Mich., agrees with her assessment.
“There are more and more PAs and [nurse practitioners] working in hospital medicine, and I think there is a lot of curiosity and some apprehension on the part of people who have not worked with these non-physician providers,” says Genzink.
Genzink, also a member of SHM’s Non-Physician Provider Task Force, speculates that the apprehension of physicians who have not worked with PAs may be due to a misunderstanding of the PA’s role. “They’re either underestimating or overestimating exactly what a PA can do or what they are getting when they hire a PA,” he says.
A Short History of the Profession
PA programs officially began in the mid-1960s at Duke University Medical School (Durham, N.C.). Eugene Stead, MD, is credited with developing the concept of the physician assistant as a health professional who would work with physician supervision to extend patient access to care, according to the American Academy of Physician Assistants.
For the first class of PAs in 1965, Dr. Stead selected Navy corpsmen who had received medical training and experience during their service in Vietnam. The curriculum was based on Dr. Stead’s knowledge of fast-track training of physicians during World War II. From this early program, the profession has evolved to more than 130 programs that now adhere to rigorous national accreditation standards set forth by the independent Accreditation Review Commission on Education for the Physician Assistant (ARC-PA). The ARC-PA is sponsored by the American Medical Association and the American College of Surgeons, among many other professional medical organizations (www.aapa.org/geninfo1.html).
Scope of Practice
Prerequisites to PA programs include two years of college courses in basic and behavioral science, as well as prior experience in healthcare. According to a report generated by the Association of Physician Assistant Programs, most PA students have earned a bachelor’s degree and have an average of 38 months of healthcare experience before being admitted to a PA program.2
The first year of PA education comprises a didactic curriculum with coursework in anatomy, physiology, biochemistry, pharmacology, physical diagnosis, pathophysiology, microbiology, clinical laboratory sciences, behavioral sciences, and medical ethics. In the second year, students receive hands-on clinical training through a series of rotations—typically in family and internal medicine, obstetrics and gynecology, pediatrics, general surgery, emergency medicine, and psychiatry. By the time they graduate (typical PA programs last an average of 26 months), PAs will have completed more than 2,000 hours of supervised clinical practice.
PAs work in all areas of medicine. Although hospital bylaws and state regulations often stipulate the PA’s scope of practice, the major determinant of duties is the supervising physician. The relationship between supervising physician and PA, says Kislingbury, is a collaborative one. Duties are “defined on an individual basis, and they are determined based on our [PAs’] experience, the physicians’ experience with us, and then the nuances of the system and the hospital itself.
“The PA who is hired should know what his or her scope of practice is,” she continues. “By the time they have graduated and obtained their license, they should know what their state allows them to do.”
For instance, according to the American Academy of Physician Assistants, 48 of the 50 states, plus the District of Columbia and [the U.S. Territory of] Guam, authorize PAs to prescribe medications. In California, PA prescriptions are referred to as “written prescription transmittal orders.”
“For the most part,” says Genzink, “the supervising physician determines what the PA is capable of doing, within the guidelines of state law.”
Within Genzink’s hospital medicine group (with which he has been affiliated for five years) the physician and PA roles are very similar.
“We see the same type of patients in a team approach. For instance, it’s not uncommon for one of us to order a test early in the day, and then, when results come back, the other person may be discharging that patient or prescribing other treatments, if necessary,” he explains. “In general, the physicians take care of the more complicated patients, while PAs take care of more routine patients.”
Genzink’s group experience aligns with findings of a 1998 University of Pittsburgh School of Nursing Study, which evaluated provider roles and patient outcomes in an acute care setting.3 Compared with acute care nurse practitioners and PAs, residents in that study tended to care for patients who were older and sicker.
Genzink reports that in his group initial histories and physicals, as well as the consultations, are performed exclusively by the PAs and then the physician takes over for treatment. “Based on the acuity of the patient,” says Genzink, “the physician may be right down there to see the patient immediately.”
Areas for Improvement?
Although the two PAs interviewed for this article report positive experiences working with hospitalists, they admit that some physicians continue to hold misperceptions about the PA’s role in caring for patients.
Kislingbury says that hospitalists could improve their delegation of duties to the PAs and recognize their scope of practice. She admits that delegation duties can be improved through gaining experience. “Although the PA profession has been around for a while, there are a surprising number of institutions that do not utilize physician assistants on the wards in routine rounds and bedside-type care,” says Kislingbury.
“I think some of the problems develop when they [physicians] hire a PA and expect to get a physician—and they [don’t],” says Genzink. “The easiest way for me to explain the role is to compare it to a teaching model. All physicians have been through residency programs. They understand the hierarchy that involves training and teaching residents. PAs come out of school ‘green,’ with the assumption that training will go on at the workplace. So, if a physician takes the same stance toward a new PA as they would toward an intern, that is a pretty close comparison.
“You begin by letting PAs or interns do a few simple things, and as they master those, you teach them more,” he continues. “And then, hopefully, over time they’ve been able to master everything that the physician is able to master. [Employing a PA] is a significant investment. And, it takes time. Sometimes, that process can be very easy, depending on the person. Sometimes it can be very slow, and I think that’s sometimes where some of the frustration may come in.”
Genzink adds that in his hospital medicine group, the physicians are familiar with the idea that part of their job as supervising physicians is to train new PAs.
Kislingbury points that out that PAs can also play a role in informing the physician team members about the range of cases they are allowed to treat, thus furthering the collaboration between PAs and hospitalists: “It is merely a matter of educating the team members about what we can and cannot do.”
Accordingly, the SHM Non-Physician Provider Task Force was formed to provide a resource to hospitalists who work with PAs and have questions about scope of practice, reimbursement, and other issues as they pertain to PAs and nurse practitioners. (Visit www.hospitalmedicine.org for more information.) The Task Force is a resource for non-physicians providers, too, offering educational opportunities at SHM meetings, more visibility with the specialty, and a voice for advocacy.
The Positives of the Collaboration
While the PAs report that hospitalists could improve in communicating about their practice roles with PAs, “There are so many things that hospitalists do right!” says Kislingbury. Calling the experience of working with hospitalists a privilege, she says that “where it is a true partnership, we are treated as equals, we are given the responsibility that our experience will allow, and we are truly team members.
“Hospitalists are geared into the efficiencies of the system and the nuances of the hospital. These are subtleties that come with practicing in an area for a long period of time, not just coming in for a month and then leaving and returning,” she says. “Hospitalists know the daily ins and outs, and it is really a pleasure to learn from them.”
Prior to his affiliation with Hospitalists of West Michigan, Genzink was employed directly by a hospital in Grand Rapids. The physicians with whom he now works have been hospitalists almost exclusively throughout their medical careers. “One of the main benefits they offer is availability, simply because we [the group’s practice members] are in the hospital 24/7,” he says. “They also have more experience in dealing with more complex issues, just as do the PAs that are working in our system.”
What about the notion that PAs and nurse practitioners are more skilled or practiced with patient and family communications? One study by Rudy, et al. found that nurse practitioners and PAs were more likely than residents to discuss patients with bedside nurses and to interact with patients’ families.3 Genzink does not find this to be the case in his group’s practice.
“That presumption [that PAs are more communicative with families and patients] may have come about simply because as the demands on hospitalists continue to grow and the workload increases, adding the PA to the team means there are more people to do things like that [handle family communications],” he says. “Certainly, in our group, the PAs do lots of patient education, and we talk to patients about end-of-life issues and other difficult matters as well. But that is not delegated to them; in our group, both the PAs and the physicians participate equally in patient and family communication.”
Daily Learning
Hospitalists and PAs also complement each other in the interdisciplinary care team because, “as a general rule, hospitalists love to teach,” says Kislingbury. “They don’t forget that just because you have your PA degree your learning does not stop there. The PA profession is almost like on-the-job training. You are allowed to choose the specialty that you want, and you gain your experience when you enter that [arena], as opposed to an internship or residency, where you first gain experience and then enter the specialty. We so appreciate the ability of the hospitalist to teach because we are learning while doing, on a day-to-day basis. It’s invaluable to have their teaching.” TH
Gretchen Henkel also writes about dealing with difficult families in this issue.
Resources
- Christmas AB, Reynolds J, Hodges S, et al. Physician extenders impact trauma systems. J Trauma. 2005 May;58(5):917-920.
- Nineteenth Annual Report on Physician Assistant Educational Programs in the United States, 2002-2203. Alexandria, Va. Association of Physician Assistant Programs.
- Rudy EB, Davidson LJ, Daly B, et al. Care activities and outcomes of patients cared for by acute care nurse practitioners, physician assistants, and resident physicians: a comparison. Am J Crit Care. 1998 Jul;7(4):267-281.
The Challenge of Family
It’s extremely hard being in a room with a family that is angry, confrontational, and hostile,” says clinical social worker Jane B. Hawgood, MSW, who often works with the hospitalist group on the General Medicine Service at the University of California at San Francisco Medical Center. “When you read about these cases in a textbook, it seems so clean and neat.”
Hospitalists have all encountered them: family members who, because of their behavior toward providers, come to be labeled as “difficult.” What are the best ways to deal with patients’ family members who are unresponsive, overbearing, or outright hostile to physicians and the care team? And how do you proceed to a treatment plan that is best for the patient?
The first step, believes Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, and chair of SHM’s Ethics Committee, is to avoid using the term “difficult.”
“I think ‘difficult’ is a loaded term and kind of pejorative,” says Dr. Baudendistel. “When their loved ones are in the hospital, families are vulnerable. They don’t really know what to expect. I don’t know that I wouldn’t want my grandmother, or mother described as a ‘difficult patient,’ or a family member described as ‘difficult.’ Rather than saying, ‘this is a difficult family member,’ I would rather phrase it, ‘This is someone who has a lot of worries.’ ”
Hawgood employs a similar approach. “I like to define the situation as ‘a family member who is having difficulty dealing with the patient’s illness,’” she says. “If I hear, during rounds, that this family is difficult, I immediately begin asking myself, ‘Why are they having difficulty? Is this an interpersonal issue? Does this family member have a psychiatric history? Is there a history of a past problem with the medical system? Is it a financial issue?’ I really try not to presume things. I always try and keep an open mind about what a patient’s and family’s goals are, and what I can do to help. You need to clearly understand your goals and have good support from your team to redirect the energy.”
“Unrealistic expectations” might describe some of the encounters for Adrienne Bennett, MD, director for the Division of Hospital Medicine and associate clinical professor of medicine at Ohio State University. In her former post as founder and director of hospitalist services at Newton Wellesley, a community teaching hospital in the western suburbs of Boston, she and colleagues dealt with a relatively affluent patient population. Some of the patients and families, she says, “can sometimes be somewhat demanding and difficult if they feel they aren’t getting what they’re entitled to. In that sense, they can become ‘the angry daughter,’ as my colleague used to say.”
—Jane Hawgood, MSW
Building Trust
Because they do not have an ongoing history with patients, hospitalists may often be starting at a disadvantage in forming a new relationship. Dr. Baudendistel believes hospitalists can quickly learn the skill of reassuring patients and their families. One way to do that, he says, is to “link with the primary care physician.” He often calls the primary care physician and tells the family of his conversations with the family doctor, thus establishing a level of comfort for them. He makes it clear to the family that he is available to them, giving them phone and pager numbers so they can easily reach him.
Dr. Baudendistel also tries to accommodate family members’ schedules, setting up visits when working family members are able to come to the hospital or making sure to have daily telephone contact if it is not possible to synchronize in-person visits with them.
Most families, he has found, are then willing to listen and work with him. As familiarity with hospitalists increases, family concerns about a “stranger” caring for their loved one slowly diminish. “Patients and families generally accept the idea of seeing a new doctor in the hospital a little bit more easily each year that goes by,” he notes.
Another technique used at California Pacific Medical Center, Dr. Baudendistel adds, is to pair a hospitalist with the same patient if he or she is readmitted. “We really believe in the continuity of the relationship, so we try to preserve that as much as possible,” he says, “because the big obstacle for hospitalists is always handoffs.”
On the Same Page
Intrinsic to forming a relationship with the patient and family is to discuss their goals of care, says Hawgood. Shana Weber, DO, FAAP, a pediatric hospitalist at Alaska Native Medical Center in Anchorage, agrees.
“You need to be on the same page,” she says. “Without knowing what the parents are hoping to get from their child’s stay before discharge, you really cannot help them.”
For instance, says Dr. Weber, some parents may be surprised to learn that their child is going to be sent home with a feeding tube or other nursing care needs.
“It is important to find out what their agenda is and what yours is. Parents’ expectations can be very different from ours,” she explains. “Letting parents know you’re listening—whether or not you agree with what they’re saying—is half the battle. You need to verify their feelings, let them know you’re listening to them, and that you understand their concerns.”
Use Team Resources
Accessing the expertise of other providers may be necessary to complete discharge plans for complicated cases. Dr. Baudendistel recalls a 30-year-old woman with a progressive neurological condition who had previously been living in the community. Her condition had deteriorated to the extent that she would no longer be able to eat safely, and, thus, she would not be able to return home. The team brought in a speech therapist, physical therapist, social worker, and discharge planner to meet with the family and present options.
Hospitalists interviewed for this article agreed that clinical social workers bring a much-needed perspective to dealing with families. One recent case at UCSF Medical Center involved a woman in her late 50s whose cancer, after multiple treatments and treatment complications, had come back very aggressively. One of her daughters, a young woman in her 20s, “had developed a very deep religious faith that she could cure her mother through prayers and faith,” recalls Hawgood. “As her mother deteriorated, the daughter became more angry and hostile to the hospitalists.”
Hawgood approached the daughter and asked if she would sit down and talk with her, and tell her what had gone wrong in the past, and “how we could improve things in the future.” As she listened to the daughter, she realized how much the daughter loved her mother and how desperately frightened she was.
“If I could help you in one way, what would that be?” Hawgood asked the daughter.
After a silence, the daughter replied, “We need a refrigerator.”
It turned out that the family was financially unable to replace a broken refrigerator. To take her mother home, the daughter needed a way to refrigerate enteral feeding supplies. And Hawgood was able to secure a refrigerator for the family, and says that the incident underscored for her the importance of keeping an open mind.
Later, when the mother was dying, Hawgood was again asked by the team to provide support for the daughter so that hospitalists could care for their patient. “She was so angry, and it was directed at the hospitalists,” recalls Hawgood. “It was just her absolute inability to accept that her mother, who was the center in her life, was going to die. You have to give people credit and respect. You have to understand where they’re coming from and what’s going to work for them.”
Training Adequate?
According to a 2003-2004 survey conducted by the American Association of Medical Colleges, 124 out of 125 medical schools included communication skills as required courses for their medical students.1 However, Dr. Baudendistel points out that there are currently no national standards for proficiency in communications skills and that the field is in relative infancy at this time. Inclusion of interpersonal and communication skills as one of the Accreditation Council for Graduate Medical Education’s (ACGME) core competencies will help focus more attention on how to teach communication skills, he believes.2
“Communication is now one of the six core competencies,” he says. “It’s no longer secondary to being a smart doctor: It’s equally important in the view of the ACGME. So I think that will help.”
Beyond standardization of communication skills curricula, it is also necessary, he emphasizes, to verify providers’ proficiency in those skills. In the California Pacific Medical Center’s residency program residents receive 360-degree evaluations. These go beyond the typical evaluations in the past, wherein residents would be evaluated by supervising attending physicians and interns working under them. Now, evaluations of residents are sought from nurses—and from the patients themselves. Obtaining 360-degree feedback from all those who have interacted with the resident functions as a valuable teaching tool.
Experience: the Best Teacher
While most agree that training and required communications courses should be increased, Dr. Bennett points out that some of the hospitalist’s expertise with family communications will simply evolve with time and experience.
“I’ve learned a lot from situations in group meetings with a social worker or a patient ombudsperson, just watching how they manage the situation,” she says. At Newton Wellesley Hospital, social workers and chaplains were sometimes better able to find the right way to phrase something so it came across in a way the family could accept, recalls Dr. Bennett. She raises the a case of a 50-year-old man who came in with cardiac arrest and whom they needed to withdraw from life support. He had been born and raised Catholic, but had converted to Judaism, which was his ex-wife’s religion as well as that of his children. He had an extensive family (he was one of 10 children), who were concerned about his ability to receive Catholic last rites. The chaplain understood the implications for both religions and was able to negotiate a compromise that satisfied both sides and allowed life support to be withdrawn.
Dr. Weber, who completed her residency at DeVos Children’s Hospital in Grand Rapids, Mich., praised the training she received in doctor-patient communications while in medical school. However, once she arrived in Anchorage, she discovered that the cultural norms of Alaska native people required some on-the-job learning.
She once asked an adolescent girl with Crohn’s disease whether she had any belly pain. “She wasn’t answering me, and I thought, ‘Oh great—just another typical teenage girl’” remembers Dr. Weber. “Well, I thought she wasn’t answering me, but she was lifting her eyebrows, which means ‘yes.’ But I didn’t know that.”
Dr. Weber has found nurses and other long-time hospital staff to be very helpful in learning how to communicate with her patient population.
Context and History
Hawgood reminds hospitalists that families often come into hospitals with past histories of things gone wrong.
“The whole healthcare system is so volatile now,” she observes. “People feel rushed, they feel [they are being] rushed out of hospital. They don’t have adequate healthcare insurance; they don’t have adequate care in the community. We send people out with trachs, tube feeds, open wounds, and pain issues. People are dealing with limited money, trying to juggle work, children, and elderly parents. So they have reasons to be angry.”
Families feel frustrated when their loved one is sick, agrees Dr. Baudendistel. “It may be that your role is to just let them vent their frustration.”
Says Hawgood, “I tell the people I train that I have nothing to lose. The patients and their families have everything to lose. So, even if I get off on the wrong foot, I’ll go back and ask, ‘could I start again?’ And usually, people will say, ‘yes.’ It’s up to me to make it work.”
Dr. Weber recalls one family at ANMC with a special needs child who had been in a Seattle hospital, and was readmitted to their facility with kidney stones. He was not getting better and the physicians recommended that the family travel back to Seattle, where a pediatric urologist could remove the stones. The parents were uncomfortable with the recommendation that their son return to Seattle.
“We did need to bring in a mediator, and have several family care conferences with the parents, with social workers and discharge planners, and all involved providers,” says Dr. Weber.
In the course of the conferences, the family revealed that their child’s disabilities were due to a missed diagnosis of meningitis when he was a baby. “They harbored a lot of resentment toward the medical profession in general,” says Dr. Weber. “It was hard to work through that. They couldn’t let it go—and I don’t blame them—and it caused them to always question our motives and our intentions.”
During the care conferences, the team let the family tell their story of the meningitis case again. Just by listening to the family’s history with that event, the team was able to validate the family’s concerns. The parents agreed to take their son to Seattle for the procedure, and later sent a thank you card to the pediatric team at ANMC that had treated him.
Don’t Make Assumptions
Hawgood always cautions physicians to enter the patient’s room with an open mind and to be open to cues and clues about the family’s situation. She praises the UCSF hospitalists’ training of young residents.
“They let them take the lead in patient interviews, then we all discuss how that interview went, and how things could have been done better,” says Hawgood. For instance, she recommends that hospitalists “allow for some silence in the room. You don’t have to fill up every minute with conversation. Look for the non-verbal cues, the things that weren’t said.”
In Dr. Weber’s hospital, pediatric patients come from all over state. It is not unusual for a baby to be in the neonatal intensive care unit for a while before the parents come back to visit. It would be easy to question, she says, whether these people are going to be good parents. “But until you know their social situation, you really have no place saying that,” says Dr. Weber. “You may find that they have six other children at home and cannot be here because they have no other caregivers for their children, and their village is 200 miles away.”
The Best You Can Do
Despite the care team’s best efforts, there will be a few cases, admits Dr. Bennett, where “you just can’t make much headway.” She recalls the case of an elderly man who had had a massive stroke, lived in a nursing home, and had not communicated for years. The man’s daughter was convinced, however, that he communicated with her and was “adamant that everything had to be done. We tried and tried,” explains Dr. Bennett, calling several group meetings and using hospital chaplains as allies, “but she just couldn’t hear it, and couldn’t see it [that her father would not get better]. She was too vested in believing that he did, in fact, communicate with her and that he would get better.”
In such cases the team may have to do the best they can to honor the patient’s and the family member’s value system and help them abide by that.
“There’s one other thing about difficult families and difficult patients: You have such an intense relationship with them that you don’t have with other people,” notes Hawgood. “If you can hang in there, they’re the best relationships you can have. You are so emotionally engaged in trying to make it work. I have chosen to work with hospitalists because of the approach they take. I think it’s the most efficient model you can use in a hospital. We really talk about the goals of care, and what we understand about the patient’s and family’s goals of care. We approach this from the point of view that they deserve care. What can we do to make a difference, so that it works for the patient and the families?” TH
Writer Gretchen Henkel lives in California.
References
- “Number of U.S. Medical Schools Teaching Selected Topics 2003-2004.” Compiled by the American Association of Medical Colleges Institutional Profile System. Available online at: http://services.aamc.org/currdir/section2/03-04hottopics.pdf. Last accessed January 26, 2006.
- General Competencies; ACGME Outcome Project. September, 1999. Available online at: www.acgme.org/outcome/comp/compMin.asp. Last accessed January 27, 2006.
It’s extremely hard being in a room with a family that is angry, confrontational, and hostile,” says clinical social worker Jane B. Hawgood, MSW, who often works with the hospitalist group on the General Medicine Service at the University of California at San Francisco Medical Center. “When you read about these cases in a textbook, it seems so clean and neat.”
Hospitalists have all encountered them: family members who, because of their behavior toward providers, come to be labeled as “difficult.” What are the best ways to deal with patients’ family members who are unresponsive, overbearing, or outright hostile to physicians and the care team? And how do you proceed to a treatment plan that is best for the patient?
The first step, believes Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, and chair of SHM’s Ethics Committee, is to avoid using the term “difficult.”
“I think ‘difficult’ is a loaded term and kind of pejorative,” says Dr. Baudendistel. “When their loved ones are in the hospital, families are vulnerable. They don’t really know what to expect. I don’t know that I wouldn’t want my grandmother, or mother described as a ‘difficult patient,’ or a family member described as ‘difficult.’ Rather than saying, ‘this is a difficult family member,’ I would rather phrase it, ‘This is someone who has a lot of worries.’ ”
Hawgood employs a similar approach. “I like to define the situation as ‘a family member who is having difficulty dealing with the patient’s illness,’” she says. “If I hear, during rounds, that this family is difficult, I immediately begin asking myself, ‘Why are they having difficulty? Is this an interpersonal issue? Does this family member have a psychiatric history? Is there a history of a past problem with the medical system? Is it a financial issue?’ I really try not to presume things. I always try and keep an open mind about what a patient’s and family’s goals are, and what I can do to help. You need to clearly understand your goals and have good support from your team to redirect the energy.”
“Unrealistic expectations” might describe some of the encounters for Adrienne Bennett, MD, director for the Division of Hospital Medicine and associate clinical professor of medicine at Ohio State University. In her former post as founder and director of hospitalist services at Newton Wellesley, a community teaching hospital in the western suburbs of Boston, she and colleagues dealt with a relatively affluent patient population. Some of the patients and families, she says, “can sometimes be somewhat demanding and difficult if they feel they aren’t getting what they’re entitled to. In that sense, they can become ‘the angry daughter,’ as my colleague used to say.”
—Jane Hawgood, MSW
Building Trust
Because they do not have an ongoing history with patients, hospitalists may often be starting at a disadvantage in forming a new relationship. Dr. Baudendistel believes hospitalists can quickly learn the skill of reassuring patients and their families. One way to do that, he says, is to “link with the primary care physician.” He often calls the primary care physician and tells the family of his conversations with the family doctor, thus establishing a level of comfort for them. He makes it clear to the family that he is available to them, giving them phone and pager numbers so they can easily reach him.
Dr. Baudendistel also tries to accommodate family members’ schedules, setting up visits when working family members are able to come to the hospital or making sure to have daily telephone contact if it is not possible to synchronize in-person visits with them.
Most families, he has found, are then willing to listen and work with him. As familiarity with hospitalists increases, family concerns about a “stranger” caring for their loved one slowly diminish. “Patients and families generally accept the idea of seeing a new doctor in the hospital a little bit more easily each year that goes by,” he notes.
Another technique used at California Pacific Medical Center, Dr. Baudendistel adds, is to pair a hospitalist with the same patient if he or she is readmitted. “We really believe in the continuity of the relationship, so we try to preserve that as much as possible,” he says, “because the big obstacle for hospitalists is always handoffs.”
On the Same Page
Intrinsic to forming a relationship with the patient and family is to discuss their goals of care, says Hawgood. Shana Weber, DO, FAAP, a pediatric hospitalist at Alaska Native Medical Center in Anchorage, agrees.
“You need to be on the same page,” she says. “Without knowing what the parents are hoping to get from their child’s stay before discharge, you really cannot help them.”
For instance, says Dr. Weber, some parents may be surprised to learn that their child is going to be sent home with a feeding tube or other nursing care needs.
“It is important to find out what their agenda is and what yours is. Parents’ expectations can be very different from ours,” she explains. “Letting parents know you’re listening—whether or not you agree with what they’re saying—is half the battle. You need to verify their feelings, let them know you’re listening to them, and that you understand their concerns.”
Use Team Resources
Accessing the expertise of other providers may be necessary to complete discharge plans for complicated cases. Dr. Baudendistel recalls a 30-year-old woman with a progressive neurological condition who had previously been living in the community. Her condition had deteriorated to the extent that she would no longer be able to eat safely, and, thus, she would not be able to return home. The team brought in a speech therapist, physical therapist, social worker, and discharge planner to meet with the family and present options.
Hospitalists interviewed for this article agreed that clinical social workers bring a much-needed perspective to dealing with families. One recent case at UCSF Medical Center involved a woman in her late 50s whose cancer, after multiple treatments and treatment complications, had come back very aggressively. One of her daughters, a young woman in her 20s, “had developed a very deep religious faith that she could cure her mother through prayers and faith,” recalls Hawgood. “As her mother deteriorated, the daughter became more angry and hostile to the hospitalists.”
Hawgood approached the daughter and asked if she would sit down and talk with her, and tell her what had gone wrong in the past, and “how we could improve things in the future.” As she listened to the daughter, she realized how much the daughter loved her mother and how desperately frightened she was.
“If I could help you in one way, what would that be?” Hawgood asked the daughter.
After a silence, the daughter replied, “We need a refrigerator.”
It turned out that the family was financially unable to replace a broken refrigerator. To take her mother home, the daughter needed a way to refrigerate enteral feeding supplies. And Hawgood was able to secure a refrigerator for the family, and says that the incident underscored for her the importance of keeping an open mind.
Later, when the mother was dying, Hawgood was again asked by the team to provide support for the daughter so that hospitalists could care for their patient. “She was so angry, and it was directed at the hospitalists,” recalls Hawgood. “It was just her absolute inability to accept that her mother, who was the center in her life, was going to die. You have to give people credit and respect. You have to understand where they’re coming from and what’s going to work for them.”
Training Adequate?
According to a 2003-2004 survey conducted by the American Association of Medical Colleges, 124 out of 125 medical schools included communication skills as required courses for their medical students.1 However, Dr. Baudendistel points out that there are currently no national standards for proficiency in communications skills and that the field is in relative infancy at this time. Inclusion of interpersonal and communication skills as one of the Accreditation Council for Graduate Medical Education’s (ACGME) core competencies will help focus more attention on how to teach communication skills, he believes.2
“Communication is now one of the six core competencies,” he says. “It’s no longer secondary to being a smart doctor: It’s equally important in the view of the ACGME. So I think that will help.”
Beyond standardization of communication skills curricula, it is also necessary, he emphasizes, to verify providers’ proficiency in those skills. In the California Pacific Medical Center’s residency program residents receive 360-degree evaluations. These go beyond the typical evaluations in the past, wherein residents would be evaluated by supervising attending physicians and interns working under them. Now, evaluations of residents are sought from nurses—and from the patients themselves. Obtaining 360-degree feedback from all those who have interacted with the resident functions as a valuable teaching tool.
Experience: the Best Teacher
While most agree that training and required communications courses should be increased, Dr. Bennett points out that some of the hospitalist’s expertise with family communications will simply evolve with time and experience.
“I’ve learned a lot from situations in group meetings with a social worker or a patient ombudsperson, just watching how they manage the situation,” she says. At Newton Wellesley Hospital, social workers and chaplains were sometimes better able to find the right way to phrase something so it came across in a way the family could accept, recalls Dr. Bennett. She raises the a case of a 50-year-old man who came in with cardiac arrest and whom they needed to withdraw from life support. He had been born and raised Catholic, but had converted to Judaism, which was his ex-wife’s religion as well as that of his children. He had an extensive family (he was one of 10 children), who were concerned about his ability to receive Catholic last rites. The chaplain understood the implications for both religions and was able to negotiate a compromise that satisfied both sides and allowed life support to be withdrawn.
Dr. Weber, who completed her residency at DeVos Children’s Hospital in Grand Rapids, Mich., praised the training she received in doctor-patient communications while in medical school. However, once she arrived in Anchorage, she discovered that the cultural norms of Alaska native people required some on-the-job learning.
She once asked an adolescent girl with Crohn’s disease whether she had any belly pain. “She wasn’t answering me, and I thought, ‘Oh great—just another typical teenage girl’” remembers Dr. Weber. “Well, I thought she wasn’t answering me, but she was lifting her eyebrows, which means ‘yes.’ But I didn’t know that.”
Dr. Weber has found nurses and other long-time hospital staff to be very helpful in learning how to communicate with her patient population.
Context and History
Hawgood reminds hospitalists that families often come into hospitals with past histories of things gone wrong.
“The whole healthcare system is so volatile now,” she observes. “People feel rushed, they feel [they are being] rushed out of hospital. They don’t have adequate healthcare insurance; they don’t have adequate care in the community. We send people out with trachs, tube feeds, open wounds, and pain issues. People are dealing with limited money, trying to juggle work, children, and elderly parents. So they have reasons to be angry.”
Families feel frustrated when their loved one is sick, agrees Dr. Baudendistel. “It may be that your role is to just let them vent their frustration.”
Says Hawgood, “I tell the people I train that I have nothing to lose. The patients and their families have everything to lose. So, even if I get off on the wrong foot, I’ll go back and ask, ‘could I start again?’ And usually, people will say, ‘yes.’ It’s up to me to make it work.”
Dr. Weber recalls one family at ANMC with a special needs child who had been in a Seattle hospital, and was readmitted to their facility with kidney stones. He was not getting better and the physicians recommended that the family travel back to Seattle, where a pediatric urologist could remove the stones. The parents were uncomfortable with the recommendation that their son return to Seattle.
“We did need to bring in a mediator, and have several family care conferences with the parents, with social workers and discharge planners, and all involved providers,” says Dr. Weber.
In the course of the conferences, the family revealed that their child’s disabilities were due to a missed diagnosis of meningitis when he was a baby. “They harbored a lot of resentment toward the medical profession in general,” says Dr. Weber. “It was hard to work through that. They couldn’t let it go—and I don’t blame them—and it caused them to always question our motives and our intentions.”
During the care conferences, the team let the family tell their story of the meningitis case again. Just by listening to the family’s history with that event, the team was able to validate the family’s concerns. The parents agreed to take their son to Seattle for the procedure, and later sent a thank you card to the pediatric team at ANMC that had treated him.
Don’t Make Assumptions
Hawgood always cautions physicians to enter the patient’s room with an open mind and to be open to cues and clues about the family’s situation. She praises the UCSF hospitalists’ training of young residents.
“They let them take the lead in patient interviews, then we all discuss how that interview went, and how things could have been done better,” says Hawgood. For instance, she recommends that hospitalists “allow for some silence in the room. You don’t have to fill up every minute with conversation. Look for the non-verbal cues, the things that weren’t said.”
In Dr. Weber’s hospital, pediatric patients come from all over state. It is not unusual for a baby to be in the neonatal intensive care unit for a while before the parents come back to visit. It would be easy to question, she says, whether these people are going to be good parents. “But until you know their social situation, you really have no place saying that,” says Dr. Weber. “You may find that they have six other children at home and cannot be here because they have no other caregivers for their children, and their village is 200 miles away.”
The Best You Can Do
Despite the care team’s best efforts, there will be a few cases, admits Dr. Bennett, where “you just can’t make much headway.” She recalls the case of an elderly man who had had a massive stroke, lived in a nursing home, and had not communicated for years. The man’s daughter was convinced, however, that he communicated with her and was “adamant that everything had to be done. We tried and tried,” explains Dr. Bennett, calling several group meetings and using hospital chaplains as allies, “but she just couldn’t hear it, and couldn’t see it [that her father would not get better]. She was too vested in believing that he did, in fact, communicate with her and that he would get better.”
In such cases the team may have to do the best they can to honor the patient’s and the family member’s value system and help them abide by that.
“There’s one other thing about difficult families and difficult patients: You have such an intense relationship with them that you don’t have with other people,” notes Hawgood. “If you can hang in there, they’re the best relationships you can have. You are so emotionally engaged in trying to make it work. I have chosen to work with hospitalists because of the approach they take. I think it’s the most efficient model you can use in a hospital. We really talk about the goals of care, and what we understand about the patient’s and family’s goals of care. We approach this from the point of view that they deserve care. What can we do to make a difference, so that it works for the patient and the families?” TH
Writer Gretchen Henkel lives in California.
References
- “Number of U.S. Medical Schools Teaching Selected Topics 2003-2004.” Compiled by the American Association of Medical Colleges Institutional Profile System. Available online at: http://services.aamc.org/currdir/section2/03-04hottopics.pdf. Last accessed January 26, 2006.
- General Competencies; ACGME Outcome Project. September, 1999. Available online at: www.acgme.org/outcome/comp/compMin.asp. Last accessed January 27, 2006.
It’s extremely hard being in a room with a family that is angry, confrontational, and hostile,” says clinical social worker Jane B. Hawgood, MSW, who often works with the hospitalist group on the General Medicine Service at the University of California at San Francisco Medical Center. “When you read about these cases in a textbook, it seems so clean and neat.”
Hospitalists have all encountered them: family members who, because of their behavior toward providers, come to be labeled as “difficult.” What are the best ways to deal with patients’ family members who are unresponsive, overbearing, or outright hostile to physicians and the care team? And how do you proceed to a treatment plan that is best for the patient?
The first step, believes Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, and chair of SHM’s Ethics Committee, is to avoid using the term “difficult.”
“I think ‘difficult’ is a loaded term and kind of pejorative,” says Dr. Baudendistel. “When their loved ones are in the hospital, families are vulnerable. They don’t really know what to expect. I don’t know that I wouldn’t want my grandmother, or mother described as a ‘difficult patient,’ or a family member described as ‘difficult.’ Rather than saying, ‘this is a difficult family member,’ I would rather phrase it, ‘This is someone who has a lot of worries.’ ”
Hawgood employs a similar approach. “I like to define the situation as ‘a family member who is having difficulty dealing with the patient’s illness,’” she says. “If I hear, during rounds, that this family is difficult, I immediately begin asking myself, ‘Why are they having difficulty? Is this an interpersonal issue? Does this family member have a psychiatric history? Is there a history of a past problem with the medical system? Is it a financial issue?’ I really try not to presume things. I always try and keep an open mind about what a patient’s and family’s goals are, and what I can do to help. You need to clearly understand your goals and have good support from your team to redirect the energy.”
“Unrealistic expectations” might describe some of the encounters for Adrienne Bennett, MD, director for the Division of Hospital Medicine and associate clinical professor of medicine at Ohio State University. In her former post as founder and director of hospitalist services at Newton Wellesley, a community teaching hospital in the western suburbs of Boston, she and colleagues dealt with a relatively affluent patient population. Some of the patients and families, she says, “can sometimes be somewhat demanding and difficult if they feel they aren’t getting what they’re entitled to. In that sense, they can become ‘the angry daughter,’ as my colleague used to say.”
—Jane Hawgood, MSW
Building Trust
Because they do not have an ongoing history with patients, hospitalists may often be starting at a disadvantage in forming a new relationship. Dr. Baudendistel believes hospitalists can quickly learn the skill of reassuring patients and their families. One way to do that, he says, is to “link with the primary care physician.” He often calls the primary care physician and tells the family of his conversations with the family doctor, thus establishing a level of comfort for them. He makes it clear to the family that he is available to them, giving them phone and pager numbers so they can easily reach him.
Dr. Baudendistel also tries to accommodate family members’ schedules, setting up visits when working family members are able to come to the hospital or making sure to have daily telephone contact if it is not possible to synchronize in-person visits with them.
Most families, he has found, are then willing to listen and work with him. As familiarity with hospitalists increases, family concerns about a “stranger” caring for their loved one slowly diminish. “Patients and families generally accept the idea of seeing a new doctor in the hospital a little bit more easily each year that goes by,” he notes.
Another technique used at California Pacific Medical Center, Dr. Baudendistel adds, is to pair a hospitalist with the same patient if he or she is readmitted. “We really believe in the continuity of the relationship, so we try to preserve that as much as possible,” he says, “because the big obstacle for hospitalists is always handoffs.”
On the Same Page
Intrinsic to forming a relationship with the patient and family is to discuss their goals of care, says Hawgood. Shana Weber, DO, FAAP, a pediatric hospitalist at Alaska Native Medical Center in Anchorage, agrees.
“You need to be on the same page,” she says. “Without knowing what the parents are hoping to get from their child’s stay before discharge, you really cannot help them.”
For instance, says Dr. Weber, some parents may be surprised to learn that their child is going to be sent home with a feeding tube or other nursing care needs.
“It is important to find out what their agenda is and what yours is. Parents’ expectations can be very different from ours,” she explains. “Letting parents know you’re listening—whether or not you agree with what they’re saying—is half the battle. You need to verify their feelings, let them know you’re listening to them, and that you understand their concerns.”
Use Team Resources
Accessing the expertise of other providers may be necessary to complete discharge plans for complicated cases. Dr. Baudendistel recalls a 30-year-old woman with a progressive neurological condition who had previously been living in the community. Her condition had deteriorated to the extent that she would no longer be able to eat safely, and, thus, she would not be able to return home. The team brought in a speech therapist, physical therapist, social worker, and discharge planner to meet with the family and present options.
Hospitalists interviewed for this article agreed that clinical social workers bring a much-needed perspective to dealing with families. One recent case at UCSF Medical Center involved a woman in her late 50s whose cancer, after multiple treatments and treatment complications, had come back very aggressively. One of her daughters, a young woman in her 20s, “had developed a very deep religious faith that she could cure her mother through prayers and faith,” recalls Hawgood. “As her mother deteriorated, the daughter became more angry and hostile to the hospitalists.”
Hawgood approached the daughter and asked if she would sit down and talk with her, and tell her what had gone wrong in the past, and “how we could improve things in the future.” As she listened to the daughter, she realized how much the daughter loved her mother and how desperately frightened she was.
“If I could help you in one way, what would that be?” Hawgood asked the daughter.
After a silence, the daughter replied, “We need a refrigerator.”
It turned out that the family was financially unable to replace a broken refrigerator. To take her mother home, the daughter needed a way to refrigerate enteral feeding supplies. And Hawgood was able to secure a refrigerator for the family, and says that the incident underscored for her the importance of keeping an open mind.
Later, when the mother was dying, Hawgood was again asked by the team to provide support for the daughter so that hospitalists could care for their patient. “She was so angry, and it was directed at the hospitalists,” recalls Hawgood. “It was just her absolute inability to accept that her mother, who was the center in her life, was going to die. You have to give people credit and respect. You have to understand where they’re coming from and what’s going to work for them.”
Training Adequate?
According to a 2003-2004 survey conducted by the American Association of Medical Colleges, 124 out of 125 medical schools included communication skills as required courses for their medical students.1 However, Dr. Baudendistel points out that there are currently no national standards for proficiency in communications skills and that the field is in relative infancy at this time. Inclusion of interpersonal and communication skills as one of the Accreditation Council for Graduate Medical Education’s (ACGME) core competencies will help focus more attention on how to teach communication skills, he believes.2
“Communication is now one of the six core competencies,” he says. “It’s no longer secondary to being a smart doctor: It’s equally important in the view of the ACGME. So I think that will help.”
Beyond standardization of communication skills curricula, it is also necessary, he emphasizes, to verify providers’ proficiency in those skills. In the California Pacific Medical Center’s residency program residents receive 360-degree evaluations. These go beyond the typical evaluations in the past, wherein residents would be evaluated by supervising attending physicians and interns working under them. Now, evaluations of residents are sought from nurses—and from the patients themselves. Obtaining 360-degree feedback from all those who have interacted with the resident functions as a valuable teaching tool.
Experience: the Best Teacher
While most agree that training and required communications courses should be increased, Dr. Bennett points out that some of the hospitalist’s expertise with family communications will simply evolve with time and experience.
“I’ve learned a lot from situations in group meetings with a social worker or a patient ombudsperson, just watching how they manage the situation,” she says. At Newton Wellesley Hospital, social workers and chaplains were sometimes better able to find the right way to phrase something so it came across in a way the family could accept, recalls Dr. Bennett. She raises the a case of a 50-year-old man who came in with cardiac arrest and whom they needed to withdraw from life support. He had been born and raised Catholic, but had converted to Judaism, which was his ex-wife’s religion as well as that of his children. He had an extensive family (he was one of 10 children), who were concerned about his ability to receive Catholic last rites. The chaplain understood the implications for both religions and was able to negotiate a compromise that satisfied both sides and allowed life support to be withdrawn.
Dr. Weber, who completed her residency at DeVos Children’s Hospital in Grand Rapids, Mich., praised the training she received in doctor-patient communications while in medical school. However, once she arrived in Anchorage, she discovered that the cultural norms of Alaska native people required some on-the-job learning.
She once asked an adolescent girl with Crohn’s disease whether she had any belly pain. “She wasn’t answering me, and I thought, ‘Oh great—just another typical teenage girl’” remembers Dr. Weber. “Well, I thought she wasn’t answering me, but she was lifting her eyebrows, which means ‘yes.’ But I didn’t know that.”
Dr. Weber has found nurses and other long-time hospital staff to be very helpful in learning how to communicate with her patient population.
Context and History
Hawgood reminds hospitalists that families often come into hospitals with past histories of things gone wrong.
“The whole healthcare system is so volatile now,” she observes. “People feel rushed, they feel [they are being] rushed out of hospital. They don’t have adequate healthcare insurance; they don’t have adequate care in the community. We send people out with trachs, tube feeds, open wounds, and pain issues. People are dealing with limited money, trying to juggle work, children, and elderly parents. So they have reasons to be angry.”
Families feel frustrated when their loved one is sick, agrees Dr. Baudendistel. “It may be that your role is to just let them vent their frustration.”
Says Hawgood, “I tell the people I train that I have nothing to lose. The patients and their families have everything to lose. So, even if I get off on the wrong foot, I’ll go back and ask, ‘could I start again?’ And usually, people will say, ‘yes.’ It’s up to me to make it work.”
Dr. Weber recalls one family at ANMC with a special needs child who had been in a Seattle hospital, and was readmitted to their facility with kidney stones. He was not getting better and the physicians recommended that the family travel back to Seattle, where a pediatric urologist could remove the stones. The parents were uncomfortable with the recommendation that their son return to Seattle.
“We did need to bring in a mediator, and have several family care conferences with the parents, with social workers and discharge planners, and all involved providers,” says Dr. Weber.
In the course of the conferences, the family revealed that their child’s disabilities were due to a missed diagnosis of meningitis when he was a baby. “They harbored a lot of resentment toward the medical profession in general,” says Dr. Weber. “It was hard to work through that. They couldn’t let it go—and I don’t blame them—and it caused them to always question our motives and our intentions.”
During the care conferences, the team let the family tell their story of the meningitis case again. Just by listening to the family’s history with that event, the team was able to validate the family’s concerns. The parents agreed to take their son to Seattle for the procedure, and later sent a thank you card to the pediatric team at ANMC that had treated him.
Don’t Make Assumptions
Hawgood always cautions physicians to enter the patient’s room with an open mind and to be open to cues and clues about the family’s situation. She praises the UCSF hospitalists’ training of young residents.
“They let them take the lead in patient interviews, then we all discuss how that interview went, and how things could have been done better,” says Hawgood. For instance, she recommends that hospitalists “allow for some silence in the room. You don’t have to fill up every minute with conversation. Look for the non-verbal cues, the things that weren’t said.”
In Dr. Weber’s hospital, pediatric patients come from all over state. It is not unusual for a baby to be in the neonatal intensive care unit for a while before the parents come back to visit. It would be easy to question, she says, whether these people are going to be good parents. “But until you know their social situation, you really have no place saying that,” says Dr. Weber. “You may find that they have six other children at home and cannot be here because they have no other caregivers for their children, and their village is 200 miles away.”
The Best You Can Do
Despite the care team’s best efforts, there will be a few cases, admits Dr. Bennett, where “you just can’t make much headway.” She recalls the case of an elderly man who had had a massive stroke, lived in a nursing home, and had not communicated for years. The man’s daughter was convinced, however, that he communicated with her and was “adamant that everything had to be done. We tried and tried,” explains Dr. Bennett, calling several group meetings and using hospital chaplains as allies, “but she just couldn’t hear it, and couldn’t see it [that her father would not get better]. She was too vested in believing that he did, in fact, communicate with her and that he would get better.”
In such cases the team may have to do the best they can to honor the patient’s and the family member’s value system and help them abide by that.
“There’s one other thing about difficult families and difficult patients: You have such an intense relationship with them that you don’t have with other people,” notes Hawgood. “If you can hang in there, they’re the best relationships you can have. You are so emotionally engaged in trying to make it work. I have chosen to work with hospitalists because of the approach they take. I think it’s the most efficient model you can use in a hospital. We really talk about the goals of care, and what we understand about the patient’s and family’s goals of care. We approach this from the point of view that they deserve care. What can we do to make a difference, so that it works for the patient and the families?” TH
Writer Gretchen Henkel lives in California.
References
- “Number of U.S. Medical Schools Teaching Selected Topics 2003-2004.” Compiled by the American Association of Medical Colleges Institutional Profile System. Available online at: http://services.aamc.org/currdir/section2/03-04hottopics.pdf. Last accessed January 26, 2006.
- General Competencies; ACGME Outcome Project. September, 1999. Available online at: www.acgme.org/outcome/comp/compMin.asp. Last accessed January 27, 2006.
The Gender Factor
In 1980 women physicians represented 11.6% of all U.S. physicians. In 2003 they represented 26% of the total physician population.1 Drawing from the ranks of internal medicine and pediatrics, in which women physicians represent 41.8% and 65.6% of all residents, hospital medicine will likely reap the benefits of these increasing numbers.2 Indeed, hospital medicine appears to offer many advantages for women: an intrinsically collaborative working environment, flexible work hours, and the opportunity to participate in forming the structure for a new specialty. But do enough opportunities for advancement exist in this relatively young specialty?
The Hospitalist recently talked with women hospitalists, SHM leadership, and a researcher on gender discrimination in academic medicine. All shared their perceptions about how hospital medicine fares regarding inclusion of women—both in the ranks and in leadership positions.
A Career that Works
“As a woman hospitalist, I’ve had many opportunities to advocate for patient safety and quality being the primary guiding principle in reorganizing care,” says Lakshmi Halasyamani, MD, associate chair, Department of Internal Medicine and an academic hospitalist at St. Joseph Mercy Hospital, Ann Arbor, Mich. “I think as women we do juggle a lot of responsibilities, but I think those skills probably uniquely position us to be very effective in managing groups and being members and leaders of teams.”
As a mother of two young children, Dr. Halasyamani enjoys the flexibility of her current position. “I have a very busy life, but I make sure I have time to do the other parts of my life because those will never come back to me. Today, I went to my daughter’s school and helped her class with some of their math problems, and I chair a multicultural committee at her school as well.”
She finds that she brings the same type of organizational skills to both her working and family life. “Whether it’s preparing for a school assembly or preparing for a patient safety committee meeting,” explains Dr. Halasyamani, “there just isn’t time to focus on what is not important or to come unprepared. Every minute is incredibly precious.”
Like Dr. Halasyamani, Sheri Chernetsky Tejedor, MD, a clinical instructor of medicine at Emory University School of Medicine in Atlanta, has also been able to carve out a clinical and academic track that suits her present needs for family time. Under a supportive supervisor, Mark Williams, MD, FACP, professor of medicine and director, Emory Hospital Medicine Unit, and editor of the Journal of Hospital Medicine, Dr. Tejedor has worked part time as a hospitalist in a nearby community hospital; has worked in academia, including writing and research in quality improvement; and essentially has been a full-time mother when she is home. “I haven’t felt that any doors have closed, and the only ones that have closed are ones that I’ve closed myself—just accepting that I can’t do everything,” says Dr. Tejedor.
According to the AMA, 62.6% of all women physicians fall within the specialties of internal medicine, pediatrics, family medicine, obstetrics/gynecology, psychiatry, and anesthesiology.1 That is one reason the numbers of women in hospital medicine are also increasing, says Larry Wellikson, MD, FACP, CEO of SHM.
“Because hospitalists come from the ranks of pediatricians and internists, as those specialties attract more women, I think they will also find hospital medicine very attractive as they are looking for their career choice,” says Dr. Wellikson.

—Lakshmi Halasyamani, MD
Approaching Parity?
Although SHM does not currently keep statistics on percentages of women in the organization, many hospitalist services point to increasing numbers of women in their departments. For instance, SHM Past President Robert Wachter, MD, FACP, director of the hospitalist group at the University of California, San Francisco, reports that 57% (12 out of 21) of the hospitalists in his group are women. This majority does not stem from deliberate recruiting on his part.
“My goal here has been to recruit and retain the best people. I couldn’t care less whether they are women or men,” says Dr. Wachter. “I would begin to care if we were so skewed in one direction or the other that it might indicate that we weren’t providing a positive environment for either women or men. But our group has grown organically and it has just turned out that we’ve ended up with more women than men.”
Leadership Opportunities in Medicine
While overall increases in the numbers of women physicians can be seen as a hopeful sign, these percentages may mask the reality for women trying to achieve parity in leadership roles. In fact, the percentages of women in leadership positions in academic medicine remain low: For example, only 11% of department chairs in medical schools are women, and 10% of medical school deans are women.1
A higher percentage of women in a particular specialty does not necessarily translate into better advancement opportunities, according to statistician Arlene S. Ash, PhD, a research professor in the Department of General Internal Medicine at the Boston University School of Medicine. “Sadly,” she says, “the main thing you can predict about a specialty with more women is that it will be less well-paid overall.”
Many committee assignments and semi-leadership positions in the academic medicine arena are informally awarded, and they often go to men. “Often these are innocent decisions,” explains Dr. Ash. “The positions carry perks, and perhaps some regular funding, and can be stepping stones to later promotion, but they usually go to the person who pops into the mind of the administrator making the decision.”
It takes “incredible vigilance,” says Dr. Ash, “to see your way past the prejudiced lens with which we all, having grown up in this society, view the relative value of men’s and women’s contributions.”
To achieve more parity for women, Dr. Ash believes it’s necessary to more closely scrutinize and to set standards for leadership selection processes. Currently, she explains, “There is no comprehensive attempt to cast a wide net, to consider all who might be appropriate, and to ensure a non-sexist, non-biased process for choosing people to get such positions. Even in departments with more than 50% women, and even where the problem is recognized, most of these ‘gateway’ opportunities still go to guys.”
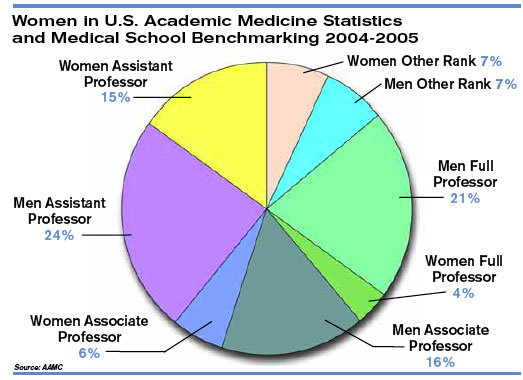
Hospitalists Breaking the Mold?
Those interviewed believe hospital medicine, as a new specialty, may have a chance to break the traditional molds established by more entrenched medical school specialties.
“We’re inventing this entire thing [the hospital medicine specialty] as we go along, so we have not had time to develop an ‘old boys’ network,’” quips Dr. Wachter. “The hope is that if you start a field now, it will not develop along those lines. As we look at those holding leadership roles at individual hospitals and in the society, you find that talented people rise to the top. If you start with a neutral playing field without the tradition and history of the smoke-filled room, it turns out that people sort out on their skills and their interests.”
“I think hospital medicine is a very accessible profession for women on a number of levels,” says Dr. Wellikson. “This is a young, growing, evolving field—as opposed to some of the more static fields in medicine, like orthopedics or thoracic surgery. One of the hallmarks of hospital medicine is creating true teams of health professionals. Women come in as equals, with good ideas, and I think this is mirrored on the SHM Board.”
Currently, four of the 12 SHM board members are women; Jean Huddleston, MD, of the Mayo Clinic is a past president; and the incoming president, Mary Jo Gorman, MD, of IPC, is also a woman. “We [the Society of Hospital Medicine] are very much an open tent,” remarks Dr. Wellikson.
According to Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston, there are pros and cons to hospital medicine being a new specialty.
“In some ways, because [hospital medicine] is a new specialty, women may have been given the opportunity to lead hospitalist programs because early hospitalist services—at least initially—were viewed as experimental,” she says. “Many hospital leaders hired hospitalists to function as ‘super residents’ rather than as leaders. So, therefore, academic institutions didn’t really feel that they had much to lose by hiring women versus men, and many hospitalist leaders—male and female—found themselves functioning as middle managers without necessarily having much input into their job descriptions.
“Even in 2006 some physician administrators hire hospitalists with the expectation that turnover is inevitable as physicians advance to other specialties,” continues Dr. McKean. “Hospital administrators and residency directors may not understand the evolving role of hospitalists as change agents in the hospital setting and may not recognize that hospitalists offer special expertise in addition to on-site availability. So it’s a two-edged sword. A lot of hospital medicine programs, because they have not only young physician leaders, but also proportionately more female physician leaders, may find that they really cannot have the same amount of clout as other established specialties within the department of medicine hierarchy.”
Dr. Halasyamani believes that the male hierarchy may be changing. In hospital medicine, she notes, “because the emphasis in inpatient care delivery is so team focused, the leaders in hospital medicine who are able to best meet those goals and have those skills are really the ones who are being given the most opportunity. If the structures within organizations are very hierarchical, then care delivery ends up looking that way. But if the leadership and decision-making structures are more collaborative, then I think care reflects that.”
At her institution, Dr. Halasyamani has had numerous opportunities to help build some of those new structures. For example, in the past year, she helped form an institutional quality and patient safety collaborative practice team, which she chaired jointly with the head of nursing. The team “brings together people who touch the patient; they identify the barriers in delivering the type of care that we want to be proud of every time, and to help solve those problems.”
Possible Pitfalls
Can hospital medicine, in fact, succeed in developing new leadership paradigms? Much will depend on consciously constructing new systems for nurturing talent and leaders. “You really have to think through your mechanisms for recognizing and rewarding achievement and ask if those mechanisms encourage the behaviors you want to encourage, or do they disadvantage people who do the work that you most want done?” says Dr. Ash.
For example, she says, the collaborative nature of hospital medicine can create problems with career advancement. “To do something meaningful, you may need to involve 20 people on a five-year project,” she explains. “How do you ensure that those people don’t get punished for choosing that work?”
Dr. Ash, together with Boston University colleague Phyllis L. Carr, MD, and Linda Pololi, MD, from Brandeis University (the principal investigator) has started a Josiah Macy Jr. Foundation-funded project to “try to change the culture of academic medicine so that it will better encourage and reward collaborative research,” she says. “This change should benefit the entire academic enterprise—although its immediate goal is to make a common career track for women more viable.
“I want to fix a generic problem about the failure to reward certain kinds of highly desirable activities,” says Dr. Ash. “The current reward system hurts women more than men, but I’m not the slightest bit unhappy—it would be a wonderful thing, actually—for men who do collaborative research to also get the career benefits they deserve.”
Advice for Leaders and Women
Are opportunities for women hospitalists improving? Dr. McKean thinks that “hierarchies exist in hospitals, where surgeons are more powerful than physicians in the department of medicine, which has its own internal hierarchy. I see many more women interviewing for internal medicine slots. And, you could say, that’s great, it’s equalizing out. But I wonder if all it’s going to mean is that the pay scale will go down. I think that’s a real consideration. What we’re seeing now is that the starting salary for physician assistants in the hospital may be more than the starting salary for some physicians in primary care. Adding more women [to a specialty] may not change inequalities. The key is adding more women in the highest leadership positions.”
“The whole process of growing talent needs to be done in a take-control sort of way,” says Dr. Ash. There is a predictable, ongoing need to fill leadership positions, she notes, and “not enough good thought about how to systematically reach out to the entire potential talent pool.”
“Mentorship is very important,” emphasizes Dr. McKean. Her own career as a physician was characterized early on, she says, by a lack of support and mentorship. Twenty-five years later, she hopes things are beginning to change and hospital medicine may in fact set the standard for other specialties for both male and female physicians.
“Medicine is always going to be unpredictable,” she continues. “It will always be stressful. There will be acutely ill patients, and people will return [to the hospital] with unanticipated problems. You cannot change this reality. But you can change how things are structured. The more the Society of Hospital Medicine can give people the tools to identify modifiable risk factors in their own practices, help leaders of the hospitalist services analyze what works and what doesn’t work, and allow for as much diversity as possible within each service, I think that a career in hospital medicine will be sustainable and extremely satisfying, and that people will get promoted. They will find different niches in which they are expert.”
To that end, with Win Whitcomb, MD (SHM co-founder), Dr. McKean approached the SHM to charge a task force to identify what makes for a long and satisfying career in hospital medicine and to develop practice standards. The job-person fit is important, and she advises young women hospitalists to take a look at themselves, define what is important, and then “tailor a schedule around that. If it is important to you to be teaching residents, for example, then you need to be in an academic program. If it is more important to have time off, and to work shifts, then you might want to work at a community hospital. There are a lot of different models,” she says “so you have to look at yourself and your husband and the other issues you have to grapple with in addition to your career.”
Above all Dr. McKean urges women (as well as men) to be receptive to advocates or mentors within their organizations.
Going Forward
Overall, Dr. Wachter sees “the nature of the field [of hospital medicine] as one that involves a lot of collaboration and multidisciplinary work seems to draw a certain kind of person. The kind of person who is most happy and successful in our field is one who likes working closely with nurses, physical therapists, social workers, and hospital administrators, and recognizes that the quality of care and patients’ outcomes are going to be, in large part, dependent on how well that team functions.”
Many younger women and men hospitalists are finding that the job-person fit contributes to a fulfilling work/life balance.
“I chose this field because I was interested in inpatient care,” says Dr. Tejedor, and the flexibility offered by her institution has reinforced that choice. “This [hospital medicine] is a great way to have the best of everything.” TH
Writer Gretchen Henkel is based in California.
References
- Women in Medicine Statistics. Prepared by the Women Physicians Congress from Physician Characteristics and Distribution in the US, 2005 ed., Chicago. AMA Press. Available at www.ama-assn.org/ama1/pub/upload/mm/19/wimstats2005.pdf. Last accessed January 9, 2005.
- Table 2. Distribution of Residents by Specialty, 1994 Compared to 2004. Women in U.S. Academic Medicine: Statistics and Medical School Benchmarking, 2004-2005. Association of American Medical Colleges; page 12. Available at www.aamc.org/members/wim/statistics/stats05/wimstats2005.pdf. Last accessed January 9, 2005.
In 1980 women physicians represented 11.6% of all U.S. physicians. In 2003 they represented 26% of the total physician population.1 Drawing from the ranks of internal medicine and pediatrics, in which women physicians represent 41.8% and 65.6% of all residents, hospital medicine will likely reap the benefits of these increasing numbers.2 Indeed, hospital medicine appears to offer many advantages for women: an intrinsically collaborative working environment, flexible work hours, and the opportunity to participate in forming the structure for a new specialty. But do enough opportunities for advancement exist in this relatively young specialty?
The Hospitalist recently talked with women hospitalists, SHM leadership, and a researcher on gender discrimination in academic medicine. All shared their perceptions about how hospital medicine fares regarding inclusion of women—both in the ranks and in leadership positions.
A Career that Works
“As a woman hospitalist, I’ve had many opportunities to advocate for patient safety and quality being the primary guiding principle in reorganizing care,” says Lakshmi Halasyamani, MD, associate chair, Department of Internal Medicine and an academic hospitalist at St. Joseph Mercy Hospital, Ann Arbor, Mich. “I think as women we do juggle a lot of responsibilities, but I think those skills probably uniquely position us to be very effective in managing groups and being members and leaders of teams.”
As a mother of two young children, Dr. Halasyamani enjoys the flexibility of her current position. “I have a very busy life, but I make sure I have time to do the other parts of my life because those will never come back to me. Today, I went to my daughter’s school and helped her class with some of their math problems, and I chair a multicultural committee at her school as well.”
She finds that she brings the same type of organizational skills to both her working and family life. “Whether it’s preparing for a school assembly or preparing for a patient safety committee meeting,” explains Dr. Halasyamani, “there just isn’t time to focus on what is not important or to come unprepared. Every minute is incredibly precious.”
Like Dr. Halasyamani, Sheri Chernetsky Tejedor, MD, a clinical instructor of medicine at Emory University School of Medicine in Atlanta, has also been able to carve out a clinical and academic track that suits her present needs for family time. Under a supportive supervisor, Mark Williams, MD, FACP, professor of medicine and director, Emory Hospital Medicine Unit, and editor of the Journal of Hospital Medicine, Dr. Tejedor has worked part time as a hospitalist in a nearby community hospital; has worked in academia, including writing and research in quality improvement; and essentially has been a full-time mother when she is home. “I haven’t felt that any doors have closed, and the only ones that have closed are ones that I’ve closed myself—just accepting that I can’t do everything,” says Dr. Tejedor.
According to the AMA, 62.6% of all women physicians fall within the specialties of internal medicine, pediatrics, family medicine, obstetrics/gynecology, psychiatry, and anesthesiology.1 That is one reason the numbers of women in hospital medicine are also increasing, says Larry Wellikson, MD, FACP, CEO of SHM.
“Because hospitalists come from the ranks of pediatricians and internists, as those specialties attract more women, I think they will also find hospital medicine very attractive as they are looking for their career choice,” says Dr. Wellikson.
—Lakshmi Halasyamani, MD
Approaching Parity?
Although SHM does not currently keep statistics on percentages of women in the organization, many hospitalist services point to increasing numbers of women in their departments. For instance, SHM Past President Robert Wachter, MD, FACP, director of the hospitalist group at the University of California, San Francisco, reports that 57% (12 out of 21) of the hospitalists in his group are women. This majority does not stem from deliberate recruiting on his part.
“My goal here has been to recruit and retain the best people. I couldn’t care less whether they are women or men,” says Dr. Wachter. “I would begin to care if we were so skewed in one direction or the other that it might indicate that we weren’t providing a positive environment for either women or men. But our group has grown organically and it has just turned out that we’ve ended up with more women than men.”
Leadership Opportunities in Medicine
While overall increases in the numbers of women physicians can be seen as a hopeful sign, these percentages may mask the reality for women trying to achieve parity in leadership roles. In fact, the percentages of women in leadership positions in academic medicine remain low: For example, only 11% of department chairs in medical schools are women, and 10% of medical school deans are women.1
A higher percentage of women in a particular specialty does not necessarily translate into better advancement opportunities, according to statistician Arlene S. Ash, PhD, a research professor in the Department of General Internal Medicine at the Boston University School of Medicine. “Sadly,” she says, “the main thing you can predict about a specialty with more women is that it will be less well-paid overall.”
Many committee assignments and semi-leadership positions in the academic medicine arena are informally awarded, and they often go to men. “Often these are innocent decisions,” explains Dr. Ash. “The positions carry perks, and perhaps some regular funding, and can be stepping stones to later promotion, but they usually go to the person who pops into the mind of the administrator making the decision.”
It takes “incredible vigilance,” says Dr. Ash, “to see your way past the prejudiced lens with which we all, having grown up in this society, view the relative value of men’s and women’s contributions.”
To achieve more parity for women, Dr. Ash believes it’s necessary to more closely scrutinize and to set standards for leadership selection processes. Currently, she explains, “There is no comprehensive attempt to cast a wide net, to consider all who might be appropriate, and to ensure a non-sexist, non-biased process for choosing people to get such positions. Even in departments with more than 50% women, and even where the problem is recognized, most of these ‘gateway’ opportunities still go to guys.”
Hospitalists Breaking the Mold?
Those interviewed believe hospital medicine, as a new specialty, may have a chance to break the traditional molds established by more entrenched medical school specialties.
“We’re inventing this entire thing [the hospital medicine specialty] as we go along, so we have not had time to develop an ‘old boys’ network,’” quips Dr. Wachter. “The hope is that if you start a field now, it will not develop along those lines. As we look at those holding leadership roles at individual hospitals and in the society, you find that talented people rise to the top. If you start with a neutral playing field without the tradition and history of the smoke-filled room, it turns out that people sort out on their skills and their interests.”
“I think hospital medicine is a very accessible profession for women on a number of levels,” says Dr. Wellikson. “This is a young, growing, evolving field—as opposed to some of the more static fields in medicine, like orthopedics or thoracic surgery. One of the hallmarks of hospital medicine is creating true teams of health professionals. Women come in as equals, with good ideas, and I think this is mirrored on the SHM Board.”
Currently, four of the 12 SHM board members are women; Jean Huddleston, MD, of the Mayo Clinic is a past president; and the incoming president, Mary Jo Gorman, MD, of IPC, is also a woman. “We [the Society of Hospital Medicine] are very much an open tent,” remarks Dr. Wellikson.
According to Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston, there are pros and cons to hospital medicine being a new specialty.
“In some ways, because [hospital medicine] is a new specialty, women may have been given the opportunity to lead hospitalist programs because early hospitalist services—at least initially—were viewed as experimental,” she says. “Many hospital leaders hired hospitalists to function as ‘super residents’ rather than as leaders. So, therefore, academic institutions didn’t really feel that they had much to lose by hiring women versus men, and many hospitalist leaders—male and female—found themselves functioning as middle managers without necessarily having much input into their job descriptions.
“Even in 2006 some physician administrators hire hospitalists with the expectation that turnover is inevitable as physicians advance to other specialties,” continues Dr. McKean. “Hospital administrators and residency directors may not understand the evolving role of hospitalists as change agents in the hospital setting and may not recognize that hospitalists offer special expertise in addition to on-site availability. So it’s a two-edged sword. A lot of hospital medicine programs, because they have not only young physician leaders, but also proportionately more female physician leaders, may find that they really cannot have the same amount of clout as other established specialties within the department of medicine hierarchy.”
Dr. Halasyamani believes that the male hierarchy may be changing. In hospital medicine, she notes, “because the emphasis in inpatient care delivery is so team focused, the leaders in hospital medicine who are able to best meet those goals and have those skills are really the ones who are being given the most opportunity. If the structures within organizations are very hierarchical, then care delivery ends up looking that way. But if the leadership and decision-making structures are more collaborative, then I think care reflects that.”
At her institution, Dr. Halasyamani has had numerous opportunities to help build some of those new structures. For example, in the past year, she helped form an institutional quality and patient safety collaborative practice team, which she chaired jointly with the head of nursing. The team “brings together people who touch the patient; they identify the barriers in delivering the type of care that we want to be proud of every time, and to help solve those problems.”
Possible Pitfalls
Can hospital medicine, in fact, succeed in developing new leadership paradigms? Much will depend on consciously constructing new systems for nurturing talent and leaders. “You really have to think through your mechanisms for recognizing and rewarding achievement and ask if those mechanisms encourage the behaviors you want to encourage, or do they disadvantage people who do the work that you most want done?” says Dr. Ash.
For example, she says, the collaborative nature of hospital medicine can create problems with career advancement. “To do something meaningful, you may need to involve 20 people on a five-year project,” she explains. “How do you ensure that those people don’t get punished for choosing that work?”
Dr. Ash, together with Boston University colleague Phyllis L. Carr, MD, and Linda Pololi, MD, from Brandeis University (the principal investigator) has started a Josiah Macy Jr. Foundation-funded project to “try to change the culture of academic medicine so that it will better encourage and reward collaborative research,” she says. “This change should benefit the entire academic enterprise—although its immediate goal is to make a common career track for women more viable.
“I want to fix a generic problem about the failure to reward certain kinds of highly desirable activities,” says Dr. Ash. “The current reward system hurts women more than men, but I’m not the slightest bit unhappy—it would be a wonderful thing, actually—for men who do collaborative research to also get the career benefits they deserve.”
Advice for Leaders and Women
Are opportunities for women hospitalists improving? Dr. McKean thinks that “hierarchies exist in hospitals, where surgeons are more powerful than physicians in the department of medicine, which has its own internal hierarchy. I see many more women interviewing for internal medicine slots. And, you could say, that’s great, it’s equalizing out. But I wonder if all it’s going to mean is that the pay scale will go down. I think that’s a real consideration. What we’re seeing now is that the starting salary for physician assistants in the hospital may be more than the starting salary for some physicians in primary care. Adding more women [to a specialty] may not change inequalities. The key is adding more women in the highest leadership positions.”
“The whole process of growing talent needs to be done in a take-control sort of way,” says Dr. Ash. There is a predictable, ongoing need to fill leadership positions, she notes, and “not enough good thought about how to systematically reach out to the entire potential talent pool.”
“Mentorship is very important,” emphasizes Dr. McKean. Her own career as a physician was characterized early on, she says, by a lack of support and mentorship. Twenty-five years later, she hopes things are beginning to change and hospital medicine may in fact set the standard for other specialties for both male and female physicians.
“Medicine is always going to be unpredictable,” she continues. “It will always be stressful. There will be acutely ill patients, and people will return [to the hospital] with unanticipated problems. You cannot change this reality. But you can change how things are structured. The more the Society of Hospital Medicine can give people the tools to identify modifiable risk factors in their own practices, help leaders of the hospitalist services analyze what works and what doesn’t work, and allow for as much diversity as possible within each service, I think that a career in hospital medicine will be sustainable and extremely satisfying, and that people will get promoted. They will find different niches in which they are expert.”
To that end, with Win Whitcomb, MD (SHM co-founder), Dr. McKean approached the SHM to charge a task force to identify what makes for a long and satisfying career in hospital medicine and to develop practice standards. The job-person fit is important, and she advises young women hospitalists to take a look at themselves, define what is important, and then “tailor a schedule around that. If it is important to you to be teaching residents, for example, then you need to be in an academic program. If it is more important to have time off, and to work shifts, then you might want to work at a community hospital. There are a lot of different models,” she says “so you have to look at yourself and your husband and the other issues you have to grapple with in addition to your career.”
Above all Dr. McKean urges women (as well as men) to be receptive to advocates or mentors within their organizations.
Going Forward
Overall, Dr. Wachter sees “the nature of the field [of hospital medicine] as one that involves a lot of collaboration and multidisciplinary work seems to draw a certain kind of person. The kind of person who is most happy and successful in our field is one who likes working closely with nurses, physical therapists, social workers, and hospital administrators, and recognizes that the quality of care and patients’ outcomes are going to be, in large part, dependent on how well that team functions.”
Many younger women and men hospitalists are finding that the job-person fit contributes to a fulfilling work/life balance.
“I chose this field because I was interested in inpatient care,” says Dr. Tejedor, and the flexibility offered by her institution has reinforced that choice. “This [hospital medicine] is a great way to have the best of everything.” TH
Writer Gretchen Henkel is based in California.
References
- Women in Medicine Statistics. Prepared by the Women Physicians Congress from Physician Characteristics and Distribution in the US, 2005 ed., Chicago. AMA Press. Available at www.ama-assn.org/ama1/pub/upload/mm/19/wimstats2005.pdf. Last accessed January 9, 2005.
- Table 2. Distribution of Residents by Specialty, 1994 Compared to 2004. Women in U.S. Academic Medicine: Statistics and Medical School Benchmarking, 2004-2005. Association of American Medical Colleges; page 12. Available at www.aamc.org/members/wim/statistics/stats05/wimstats2005.pdf. Last accessed January 9, 2005.
In 1980 women physicians represented 11.6% of all U.S. physicians. In 2003 they represented 26% of the total physician population.1 Drawing from the ranks of internal medicine and pediatrics, in which women physicians represent 41.8% and 65.6% of all residents, hospital medicine will likely reap the benefits of these increasing numbers.2 Indeed, hospital medicine appears to offer many advantages for women: an intrinsically collaborative working environment, flexible work hours, and the opportunity to participate in forming the structure for a new specialty. But do enough opportunities for advancement exist in this relatively young specialty?
The Hospitalist recently talked with women hospitalists, SHM leadership, and a researcher on gender discrimination in academic medicine. All shared their perceptions about how hospital medicine fares regarding inclusion of women—both in the ranks and in leadership positions.
A Career that Works
“As a woman hospitalist, I’ve had many opportunities to advocate for patient safety and quality being the primary guiding principle in reorganizing care,” says Lakshmi Halasyamani, MD, associate chair, Department of Internal Medicine and an academic hospitalist at St. Joseph Mercy Hospital, Ann Arbor, Mich. “I think as women we do juggle a lot of responsibilities, but I think those skills probably uniquely position us to be very effective in managing groups and being members and leaders of teams.”
As a mother of two young children, Dr. Halasyamani enjoys the flexibility of her current position. “I have a very busy life, but I make sure I have time to do the other parts of my life because those will never come back to me. Today, I went to my daughter’s school and helped her class with some of their math problems, and I chair a multicultural committee at her school as well.”
She finds that she brings the same type of organizational skills to both her working and family life. “Whether it’s preparing for a school assembly or preparing for a patient safety committee meeting,” explains Dr. Halasyamani, “there just isn’t time to focus on what is not important or to come unprepared. Every minute is incredibly precious.”
Like Dr. Halasyamani, Sheri Chernetsky Tejedor, MD, a clinical instructor of medicine at Emory University School of Medicine in Atlanta, has also been able to carve out a clinical and academic track that suits her present needs for family time. Under a supportive supervisor, Mark Williams, MD, FACP, professor of medicine and director, Emory Hospital Medicine Unit, and editor of the Journal of Hospital Medicine, Dr. Tejedor has worked part time as a hospitalist in a nearby community hospital; has worked in academia, including writing and research in quality improvement; and essentially has been a full-time mother when she is home. “I haven’t felt that any doors have closed, and the only ones that have closed are ones that I’ve closed myself—just accepting that I can’t do everything,” says Dr. Tejedor.
According to the AMA, 62.6% of all women physicians fall within the specialties of internal medicine, pediatrics, family medicine, obstetrics/gynecology, psychiatry, and anesthesiology.1 That is one reason the numbers of women in hospital medicine are also increasing, says Larry Wellikson, MD, FACP, CEO of SHM.
“Because hospitalists come from the ranks of pediatricians and internists, as those specialties attract more women, I think they will also find hospital medicine very attractive as they are looking for their career choice,” says Dr. Wellikson.
—Lakshmi Halasyamani, MD
Approaching Parity?
Although SHM does not currently keep statistics on percentages of women in the organization, many hospitalist services point to increasing numbers of women in their departments. For instance, SHM Past President Robert Wachter, MD, FACP, director of the hospitalist group at the University of California, San Francisco, reports that 57% (12 out of 21) of the hospitalists in his group are women. This majority does not stem from deliberate recruiting on his part.
“My goal here has been to recruit and retain the best people. I couldn’t care less whether they are women or men,” says Dr. Wachter. “I would begin to care if we were so skewed in one direction or the other that it might indicate that we weren’t providing a positive environment for either women or men. But our group has grown organically and it has just turned out that we’ve ended up with more women than men.”
Leadership Opportunities in Medicine
While overall increases in the numbers of women physicians can be seen as a hopeful sign, these percentages may mask the reality for women trying to achieve parity in leadership roles. In fact, the percentages of women in leadership positions in academic medicine remain low: For example, only 11% of department chairs in medical schools are women, and 10% of medical school deans are women.1
A higher percentage of women in a particular specialty does not necessarily translate into better advancement opportunities, according to statistician Arlene S. Ash, PhD, a research professor in the Department of General Internal Medicine at the Boston University School of Medicine. “Sadly,” she says, “the main thing you can predict about a specialty with more women is that it will be less well-paid overall.”
Many committee assignments and semi-leadership positions in the academic medicine arena are informally awarded, and they often go to men. “Often these are innocent decisions,” explains Dr. Ash. “The positions carry perks, and perhaps some regular funding, and can be stepping stones to later promotion, but they usually go to the person who pops into the mind of the administrator making the decision.”
It takes “incredible vigilance,” says Dr. Ash, “to see your way past the prejudiced lens with which we all, having grown up in this society, view the relative value of men’s and women’s contributions.”
To achieve more parity for women, Dr. Ash believes it’s necessary to more closely scrutinize and to set standards for leadership selection processes. Currently, she explains, “There is no comprehensive attempt to cast a wide net, to consider all who might be appropriate, and to ensure a non-sexist, non-biased process for choosing people to get such positions. Even in departments with more than 50% women, and even where the problem is recognized, most of these ‘gateway’ opportunities still go to guys.”
Hospitalists Breaking the Mold?
Those interviewed believe hospital medicine, as a new specialty, may have a chance to break the traditional molds established by more entrenched medical school specialties.
“We’re inventing this entire thing [the hospital medicine specialty] as we go along, so we have not had time to develop an ‘old boys’ network,’” quips Dr. Wachter. “The hope is that if you start a field now, it will not develop along those lines. As we look at those holding leadership roles at individual hospitals and in the society, you find that talented people rise to the top. If you start with a neutral playing field without the tradition and history of the smoke-filled room, it turns out that people sort out on their skills and their interests.”
“I think hospital medicine is a very accessible profession for women on a number of levels,” says Dr. Wellikson. “This is a young, growing, evolving field—as opposed to some of the more static fields in medicine, like orthopedics or thoracic surgery. One of the hallmarks of hospital medicine is creating true teams of health professionals. Women come in as equals, with good ideas, and I think this is mirrored on the SHM Board.”
Currently, four of the 12 SHM board members are women; Jean Huddleston, MD, of the Mayo Clinic is a past president; and the incoming president, Mary Jo Gorman, MD, of IPC, is also a woman. “We [the Society of Hospital Medicine] are very much an open tent,” remarks Dr. Wellikson.
According to Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston, there are pros and cons to hospital medicine being a new specialty.
“In some ways, because [hospital medicine] is a new specialty, women may have been given the opportunity to lead hospitalist programs because early hospitalist services—at least initially—were viewed as experimental,” she says. “Many hospital leaders hired hospitalists to function as ‘super residents’ rather than as leaders. So, therefore, academic institutions didn’t really feel that they had much to lose by hiring women versus men, and many hospitalist leaders—male and female—found themselves functioning as middle managers without necessarily having much input into their job descriptions.
“Even in 2006 some physician administrators hire hospitalists with the expectation that turnover is inevitable as physicians advance to other specialties,” continues Dr. McKean. “Hospital administrators and residency directors may not understand the evolving role of hospitalists as change agents in the hospital setting and may not recognize that hospitalists offer special expertise in addition to on-site availability. So it’s a two-edged sword. A lot of hospital medicine programs, because they have not only young physician leaders, but also proportionately more female physician leaders, may find that they really cannot have the same amount of clout as other established specialties within the department of medicine hierarchy.”
Dr. Halasyamani believes that the male hierarchy may be changing. In hospital medicine, she notes, “because the emphasis in inpatient care delivery is so team focused, the leaders in hospital medicine who are able to best meet those goals and have those skills are really the ones who are being given the most opportunity. If the structures within organizations are very hierarchical, then care delivery ends up looking that way. But if the leadership and decision-making structures are more collaborative, then I think care reflects that.”
At her institution, Dr. Halasyamani has had numerous opportunities to help build some of those new structures. For example, in the past year, she helped form an institutional quality and patient safety collaborative practice team, which she chaired jointly with the head of nursing. The team “brings together people who touch the patient; they identify the barriers in delivering the type of care that we want to be proud of every time, and to help solve those problems.”
Possible Pitfalls
Can hospital medicine, in fact, succeed in developing new leadership paradigms? Much will depend on consciously constructing new systems for nurturing talent and leaders. “You really have to think through your mechanisms for recognizing and rewarding achievement and ask if those mechanisms encourage the behaviors you want to encourage, or do they disadvantage people who do the work that you most want done?” says Dr. Ash.
For example, she says, the collaborative nature of hospital medicine can create problems with career advancement. “To do something meaningful, you may need to involve 20 people on a five-year project,” she explains. “How do you ensure that those people don’t get punished for choosing that work?”
Dr. Ash, together with Boston University colleague Phyllis L. Carr, MD, and Linda Pololi, MD, from Brandeis University (the principal investigator) has started a Josiah Macy Jr. Foundation-funded project to “try to change the culture of academic medicine so that it will better encourage and reward collaborative research,” she says. “This change should benefit the entire academic enterprise—although its immediate goal is to make a common career track for women more viable.
“I want to fix a generic problem about the failure to reward certain kinds of highly desirable activities,” says Dr. Ash. “The current reward system hurts women more than men, but I’m not the slightest bit unhappy—it would be a wonderful thing, actually—for men who do collaborative research to also get the career benefits they deserve.”
Advice for Leaders and Women
Are opportunities for women hospitalists improving? Dr. McKean thinks that “hierarchies exist in hospitals, where surgeons are more powerful than physicians in the department of medicine, which has its own internal hierarchy. I see many more women interviewing for internal medicine slots. And, you could say, that’s great, it’s equalizing out. But I wonder if all it’s going to mean is that the pay scale will go down. I think that’s a real consideration. What we’re seeing now is that the starting salary for physician assistants in the hospital may be more than the starting salary for some physicians in primary care. Adding more women [to a specialty] may not change inequalities. The key is adding more women in the highest leadership positions.”
“The whole process of growing talent needs to be done in a take-control sort of way,” says Dr. Ash. There is a predictable, ongoing need to fill leadership positions, she notes, and “not enough good thought about how to systematically reach out to the entire potential talent pool.”
“Mentorship is very important,” emphasizes Dr. McKean. Her own career as a physician was characterized early on, she says, by a lack of support and mentorship. Twenty-five years later, she hopes things are beginning to change and hospital medicine may in fact set the standard for other specialties for both male and female physicians.
“Medicine is always going to be unpredictable,” she continues. “It will always be stressful. There will be acutely ill patients, and people will return [to the hospital] with unanticipated problems. You cannot change this reality. But you can change how things are structured. The more the Society of Hospital Medicine can give people the tools to identify modifiable risk factors in their own practices, help leaders of the hospitalist services analyze what works and what doesn’t work, and allow for as much diversity as possible within each service, I think that a career in hospital medicine will be sustainable and extremely satisfying, and that people will get promoted. They will find different niches in which they are expert.”
To that end, with Win Whitcomb, MD (SHM co-founder), Dr. McKean approached the SHM to charge a task force to identify what makes for a long and satisfying career in hospital medicine and to develop practice standards. The job-person fit is important, and she advises young women hospitalists to take a look at themselves, define what is important, and then “tailor a schedule around that. If it is important to you to be teaching residents, for example, then you need to be in an academic program. If it is more important to have time off, and to work shifts, then you might want to work at a community hospital. There are a lot of different models,” she says “so you have to look at yourself and your husband and the other issues you have to grapple with in addition to your career.”
Above all Dr. McKean urges women (as well as men) to be receptive to advocates or mentors within their organizations.
Going Forward
Overall, Dr. Wachter sees “the nature of the field [of hospital medicine] as one that involves a lot of collaboration and multidisciplinary work seems to draw a certain kind of person. The kind of person who is most happy and successful in our field is one who likes working closely with nurses, physical therapists, social workers, and hospital administrators, and recognizes that the quality of care and patients’ outcomes are going to be, in large part, dependent on how well that team functions.”
Many younger women and men hospitalists are finding that the job-person fit contributes to a fulfilling work/life balance.
“I chose this field because I was interested in inpatient care,” says Dr. Tejedor, and the flexibility offered by her institution has reinforced that choice. “This [hospital medicine] is a great way to have the best of everything.” TH
Writer Gretchen Henkel is based in California.
References
- Women in Medicine Statistics. Prepared by the Women Physicians Congress from Physician Characteristics and Distribution in the US, 2005 ed., Chicago. AMA Press. Available at www.ama-assn.org/ama1/pub/upload/mm/19/wimstats2005.pdf. Last accessed January 9, 2005.
- Table 2. Distribution of Residents by Specialty, 1994 Compared to 2004. Women in U.S. Academic Medicine: Statistics and Medical School Benchmarking, 2004-2005. Association of American Medical Colleges; page 12. Available at www.aamc.org/members/wim/statistics/stats05/wimstats2005.pdf. Last accessed January 9, 2005.
Core Visionaries
If you want something done, the saying goes, ask a busy person to do it. That was precisely the situation when SHM’s Core Competencies Task Force editorial board was formed in May 2003. Charged with producing the society’s first-ever curriculum guidance document, the editorial team faced a daunting task: solicit, organize, and edit chapters for the competencies framework on topics from specific clinical conditions to ethical issues. Over the next two and a half years, each of the physician members contributed hundreds of hours of uncompensated time to the project, juggling work, family, and other professional obligations.
Because they are so involved with their own institutions and the future of hospital medicine, the physicians tapped to guide the core competencies to reality were the right pick.
“Working with the four of them was phenomenal,” says SHM staff member Tina Budnitz, MPH, who serves on both the Education Committee and the Core Competencies Task Force. “They are all incredibly hard working, driven, and intelligent. I think the hardest thing was just the logistics of coordinating schedules, since this was a volunteer activity for them.” Budnitz points out that the original target date for completion of the core competencies was early 2005. Instead, the sheer bulk of editing work pushed the deadline back to early 2006, when release of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development by the Society of Hospital Medicine coincides with the premiere of the Journal of Hospital Medicine.
Recently, The Hospitalist caught up with each of the editorial board members, who divulged some of their personal motivations for participating in the ambitious core competencies project. They also discussed the workings of the editorial board and assessed the success of their efforts.
—Daniel D. Dressler, MD, MSc
Genesis and Vision
During a July 2002 Educational Summit the SHM Education Committee and Board of Directors determined that one element necessary to evolve SHM’s educational offerings would be a framework to guide and prioritize their efforts. A parallel conversation within the Education Committee, according to Budnitz, revolved around the need to better define hospital medicine. “We’re frequently asked, ‘what differentiates a hospitalist from other general internists? What exactly should the expectations be for a practicing hospitalist?’ ” she explains.
The Editorial Board
Michael J. Pistoria, DO, FACP, associate program director, Internal Medicine Residency, and medical director of both the Hospitalist Services and the Express Admission Unit at Lehigh Valley Hospital in Allentown, Pa., began his journey as chair of the Core Competencies Task Force shortly after SHM’s September 2002 Education Summit retreat.
Dr. Pistoria also serves on SHM’s Education Committee and admits that his allegiance to the field was a strong motivation for agreeing to participate in generating the Core Competencies.
“In my mind, hospital medicine is one of the neatest things in medicine to come along in a long time,” says Dr. Pistoria. “Hospital medicine has the potential to make a significant, positive difference in the way healthcare is delivered in the United States. And to have the opportunity to be a part of a process that helps define hospital medicine, to me, was just something almost too good to be true.”
A very active SHM member, Alpesh Amin, MD, MBA, FACP, is the associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California Irvine (UCI), where he also founded the UCI hospitalist program in 1998. His role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his key role in the Core Competencies Task Force editorial board.
“It was one of my goals—while chairing the Education Committee—for our society to put together the core competencies for hospital medicine,” says Dr. Amin. “I felt that if we had core competencies, this would be the next step to move us toward defining the field of hospital medicine.”
Accordingly, Dr. Amin was instrumental during the first and second SHM Education Summits in securing both committee and SHM Board of Directors’ buy-in of such a project.
For Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine, involvement with SHM’s (and formerly NAIP’s) Education Committee was a natural extension of his own interests in medical education. At Emory University Hospital, Dr. Dressler conducts a hospital medicine elective for house staff, “to give them a better understanding of what hospital medicine is and what we do, both in the community setting and in the academic setting.”
“I thought that [development of core competencies] was something that hospitalists as a group needed to do in order to a) become recognized and b) to clarify our own understanding and expectations of hospitalist physicians around the country,” he says.

—Tina Budnitz, MPH
Like her colleagues on the editorial board, Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist (BWF) Service (Boston), attended the 2002 SHM Education Summit and subsequently joined the Core Competencies Task Force. She is also co-chair of the society’s Career Satisfaction Task Force and views this role as linked to the missions of core competencies and education because education is a key component of professional advancement and engagement in the field. The Career Satisfaction Task Force, she notes, examines what components contribute to a long and satisfying career in hospital medicine.
Dr. McKean’s personal motivation for participation on the Core Competencies Task Force relates directly to her love of teaching. Having developed two hospitalist programs (one with physicians Andy Halpert, former chief of medicine for Harvard Vanguard Associations and subsequently the BWF program in 1998) she has seen firsthand that “people right out of residency do not have all the skills that they need in order to be effective hospitalists.”
As medical director of the BWF Hospitalist Service, Dr. McKean developed a weekly Harvard Medical School CME conference Update in Hospital Medicine for members of the hospitalist service, as well a medical consultation syllabus for the newest members of the hospitalist service to distribute to residents.
“I identified what the newest members of our service right out of residency didn’t learn during their residency training and tried to make sure that we would have people come in and teach them about hospital medicine,” she explains.
As the hospitalist service matured, hospitalists developed significant expertise in these topics and frequently participate in this didactic series of lectures.
“Initially,” recounts Dr. McKean, “I was the only senior physician with experience in hospital medicine, but now my job is much easier, as I continue to learn from other hospitalists in our program.”

—Sylvia C.W. McKean, MD, FACP
A Framework, Not a Text
“We have a great team,” says Dr. Amin of the Task Force editorial board. “I think our goals were clear. We wanted to develop a set of competencies that would be unique and offer 1) an opportunity to define the space that we, as hospitalists, lead in system-based practice; and 2) a framework that would cross over the span of time, so that others could use that framework to develop future curricula.
“Once you write a book, the context is fixed. We thought this [framework for curriculum development] was a creative way of facilitating future projects and ideas,” he continues. “It becomes more of a bible for competencies in hospital medicine.”
Budnitz says the idea was to develop an enduring, flexible blueprint. “We set out to develop a guide that would serve as a blueprint for curricular development in hospital medicine,” she explains. “We wanted to standardize the expectations for learning outcomes but still allow curriculum developers to add their expertise of content and context. Each chapter of the guide is written as a set of learning objectives. We crafted these objectives to clearly indicate a proficiency level.
“For example,” says Budnitz, “it is a different expectation that someone can list the drugs that they might order for a particular condition, versus analyzing the benefits and limitations of different therapeutic approaches. And in both scenarios we have left it up to the content and curriculum developers to determine the precise list of therapeutic agents that are included in curricula and the educational approach that will most likely yield the intended learning outcome.”
Dr. Dressler elaborates on his colleagues’ characterizations of the document: “We weren’t planning on this being an overarching, comprehensive text on hospital medicine. We were not trying to develop or even provide content.”
Instead, he says, the aim was to provide medical educators with a relatively generic framework that would retain flexibility for change. “For instance,” he explains, “if a new drug comes out that is useful for [treating] heart failure, the expectation is that hospitalists should be able to explain and utilize the new and useful medications, but that we were not going to list every drug in the Core Competencies compendium.”
“The one idea that we kept coming back to is that we wanted to design a set of competencies,” said Dr. Pistoria. “We didn’t want to publish a textbook; we didn’t want to come up with a curriculum per se. We wanted to come up with a framework that someone could use to develop their own hospitalist program in their own institution.”
Soliciting Input
The Core Competencies Task Force developed an initial organizational structure for the guide and a list of chapter topics. The resulting chapter list was turned into a survey and sent to the SHM Board of Directors, Core Competencies Task Force, and Education Committee. The survey was also sent to a sample of members within each SHM region or chapter via its chapter or region director. A review of core competencies generated by other medical specialties and allied health professional societies followed.
Then, the task force put out a call for nominations of chapter contributors. Budnitz judges that there were between 150-200 responses for potential contributors. Reviewing all the nominations was no small task. In some cases the editorial board deemed it necessary to recruit non-hospitalist content experts to generate some chapters, such as those dealing with medical-legal issues. In those instances, the “outside expert” was often paired with a hospitalist to ensure that the hospitalist perspective was included.
Strategies for Content Inclusion
Dr. Amin points out that the task force “went as broad and as wide as we could to get feedback on the content for the Core Competencies.” However, it was simply not possible—nor was it the editorial board’s intent—to compile an exhaustive list of all the hundreds of diagnoses that hospitalists may see on a regular basis. The editorial board identified common diagnoses from the top 15-20 DRGs from the Medicare database. The task was then to communicate the most important aspects of what hospitalists do, in the domains of knowledge, skills, and attitudes.
To manage the sheer bulk of solicited CVs and potential chapter authors, the editorial board used a divide-and-conquer strategy. Even so, says Dr. Pistoria, this process took a fair amount of time. When chapters began arriving and the task force was reduced to the core editorial board, “the homework started kicking up, with a lot of home editing time, telephone and e-mail editing, and some face-to-face meetings to ensure that chapters were standardized and had the same format.”
Once the editorial board began its work, it was relatively easy to decide that majority rule would be the best process for resolving differences of opinion, “but honestly,” says Dr. McKean, “only a handful of issues were generated. If we didn’t develop a consensus or if we were not all in agreement, then we sometimes looked for feedback from experts outside of the task force and the editorial board.”
Keeping with the ethos of inclusion, most board members consulted with other experts at their institution about key elements to include in the document.
Regarding the “majority rules” process, “Everyone had the chance during the editorial process to voice their opinions,” says Dr. Pistoria. “If they had concerns and were able to persuade enough people, the appropriate change would be made. I think, in the end, that everyone in the core editorial group felt that their opinions were heard, and I think that lends itself to the pride that we all feel in the final product.”

—Alpesh Amin, MD, MBA, FACP
A Work in Progress
Budnitz contributed critical guidance when the board generated writing guidelines for chapter authors. Each received a template for their chapter: a document instructing them how to write a competency, and a letter indicating the intent for their particular chapter. The template went through several iterations, she says, as early chapters were returned and the board began their editing.
For example, each clinical condition is discussed through the domains of knowledge, skills, and attitudes. It was the board’s job to ensure that concepts consistently appeared in the same domain across chapters with a similar degree of specificity and in the same order. “Partway through the process, we refined our template and made it more specific,” reports Budnitz. “We were able to give the second round of contributors a little more guidance as a result.
“We originally thought the document would be ready in early 2005,” she explains. “I think we were under the misimpression that the chapters would come back, that we’d read through them in a month or two, and it would be done. It turns out that just the sheer logistics of editing four or five versions of 70 chapters was quite a process.”
“I think [the Core Competencies] is something that SHM can be proud of,” said Dr. Pistoria of the group’s efforts. “But this is by no means the end of the project – it’s only the beginning. It is a work in progress.”
Dr. Dressler agreed with Dr. Pistoria’s characterization of the Core Competencies as a work in progress.
“I am pretty satisfied with what we’ve accomplished,” says Dr. Dressler. “By no means do I feel that this is the end-all, be-all for hospital medicine, or even for education in hospital medicine. It’s a start. We expect comment. We expect criticism. Being hospitalists, we are all open and aware and willing to make changes. And so we make a start, our initial best effort to get something out there that hospitalists can look at, utilize, and then offer feedback. Our primary goal is to provide a structure for consistency in practice and consistency in expectations. We would like to make [the Core Competencies] something that hospitalists and hospitalist educators feel is useful and that can change with the needs of our specialty.”

—Michael Pistoria, DO, FACP
Concluding Thoughts
“[Working on the Core Competencies] was an exciting project,” says Dr. Amin. “It took a lot of time. We had to spend a fair amount of time learning before we could actually define what we wanted from our chapter authors. But it was a good process. It was a four-year process to develop a document that would be worthwhile and hopefully stand the test of time in defining the core aspects of the field of hospital medicine. It was great to be chairing [the] education [committee] and seeing the value of helping to facilitate this project, and now looking more broadly across how to apply this project to future educational efforts.”
The project certainly had its challenges, most of which were related to time constraints.
“All of us were working very hard in our respective programs,” notes Dr. McKean, “and we were doing this on a volunteer basis. I think we had 10 face-to-face meetings, and sat at our computers on Saturday afternoons for conference calls using a Web-based editing program.”
For her part, Dr. McKean found working on the core competencies “very satisfying. I think I learned a lot from other people on this task force, editorial board, and the organization of the Society of Hospital Medicine. This project helped me reflect upon skills that I should try to obtain, and to think about more global issues than the day-to-day hospital politics in which I was involved. I did more strategic planning and thinking about retreats. So, it was a learning experience for me, and I also felt that I was contributing to something worthwhile. It was a chance to make a difference.
“From my own professional experience, the development process has helped me here, at Brigham and Women’s Hospital, so I hope that anyone who wants to apply the core competencies would feel free to e-mail us or contact us if they have any questions at all,” she says.
Dr. Pistoria agrees with Dr. McKean’s observations. “Working on the Core Competencies had a really big impact on me, both personally and professionally,” he says. “The process helped me mature in how I deal with running a project like this because I have been given the opportunity to do some similar things at my institution. Some of the ideas that we hit upon as we were editing and developing these competencies make one think, ‘We need to do this at our institution.’ Let’s take a strong look at, say, discharge processes, get a group together, and generate some recommendations that we can then institute.”
Other editorial board members also acknowledged that their participation gave them new insights into their own practice of hospital medicine.
“It’s easy to have in your head what you think is the right thing to do,” notes Dr. Dressler, “But until you actually have to try to develop consistency in wording and expectations, to put a process together that can result in a protocol, you realize that sometimes some elements get left out—for instance, the importance of family communication in the setting of DVT.”
Regarding the board members’ hard work, Budnitz remarks, “I can’t say enough about the dedication of the editorial board. They volunteered a tremendous amount of time and stuck with the project for three years. Since the board lived in multiple time zones, we often had calls where people would be participating at 6 a.m. or 9 p.m. We convened on weekends in multiple cities across the U.S. I sincerely enjoyed the opportunity to be a part of this project and hopefully impact the future of medical education.
“I think the document makes a bold statement. It defines the hospitalist as the captain of the ship—and calls on hospitalists to lead multidisciplinary teams to improve the quality of care. I hope it sparks interest and debate about how we recruit, train, prepare, and certify physicians in hospital medicine.”
Dr. Pistoria believes that the Core Competencies will advance hospitalist programs. In fact, he says, hospitalists around the country have already affected improvements in care coordination. The hospitalist movement in general furnishes hospitals with physicians who say, “ ‘I’m going to take ownership of what happens within the four walls of this hospital,’ ” says Dr. Pistoria. “Previous to that, people obviously cared about what happened in the hospital, but they also worried about their office practices. This is our office practice. We want it to work as well as it can for our patients, for us, for our nursing colleagues, for our janitors—everybody needs to, and should, benefit from this.” TH
Writer Gretchen Henkel wrote about cultural competency in the September issue of The Hospitalist.
If you want something done, the saying goes, ask a busy person to do it. That was precisely the situation when SHM’s Core Competencies Task Force editorial board was formed in May 2003. Charged with producing the society’s first-ever curriculum guidance document, the editorial team faced a daunting task: solicit, organize, and edit chapters for the competencies framework on topics from specific clinical conditions to ethical issues. Over the next two and a half years, each of the physician members contributed hundreds of hours of uncompensated time to the project, juggling work, family, and other professional obligations.
Because they are so involved with their own institutions and the future of hospital medicine, the physicians tapped to guide the core competencies to reality were the right pick.
“Working with the four of them was phenomenal,” says SHM staff member Tina Budnitz, MPH, who serves on both the Education Committee and the Core Competencies Task Force. “They are all incredibly hard working, driven, and intelligent. I think the hardest thing was just the logistics of coordinating schedules, since this was a volunteer activity for them.” Budnitz points out that the original target date for completion of the core competencies was early 2005. Instead, the sheer bulk of editing work pushed the deadline back to early 2006, when release of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development by the Society of Hospital Medicine coincides with the premiere of the Journal of Hospital Medicine.
Recently, The Hospitalist caught up with each of the editorial board members, who divulged some of their personal motivations for participating in the ambitious core competencies project. They also discussed the workings of the editorial board and assessed the success of their efforts.
—Daniel D. Dressler, MD, MSc
Genesis and Vision
During a July 2002 Educational Summit the SHM Education Committee and Board of Directors determined that one element necessary to evolve SHM’s educational offerings would be a framework to guide and prioritize their efforts. A parallel conversation within the Education Committee, according to Budnitz, revolved around the need to better define hospital medicine. “We’re frequently asked, ‘what differentiates a hospitalist from other general internists? What exactly should the expectations be for a practicing hospitalist?’ ” she explains.
The Editorial Board
Michael J. Pistoria, DO, FACP, associate program director, Internal Medicine Residency, and medical director of both the Hospitalist Services and the Express Admission Unit at Lehigh Valley Hospital in Allentown, Pa., began his journey as chair of the Core Competencies Task Force shortly after SHM’s September 2002 Education Summit retreat.
Dr. Pistoria also serves on SHM’s Education Committee and admits that his allegiance to the field was a strong motivation for agreeing to participate in generating the Core Competencies.
“In my mind, hospital medicine is one of the neatest things in medicine to come along in a long time,” says Dr. Pistoria. “Hospital medicine has the potential to make a significant, positive difference in the way healthcare is delivered in the United States. And to have the opportunity to be a part of a process that helps define hospital medicine, to me, was just something almost too good to be true.”
A very active SHM member, Alpesh Amin, MD, MBA, FACP, is the associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California Irvine (UCI), where he also founded the UCI hospitalist program in 1998. His role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his key role in the Core Competencies Task Force editorial board.
“It was one of my goals—while chairing the Education Committee—for our society to put together the core competencies for hospital medicine,” says Dr. Amin. “I felt that if we had core competencies, this would be the next step to move us toward defining the field of hospital medicine.”
Accordingly, Dr. Amin was instrumental during the first and second SHM Education Summits in securing both committee and SHM Board of Directors’ buy-in of such a project.
For Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine, involvement with SHM’s (and formerly NAIP’s) Education Committee was a natural extension of his own interests in medical education. At Emory University Hospital, Dr. Dressler conducts a hospital medicine elective for house staff, “to give them a better understanding of what hospital medicine is and what we do, both in the community setting and in the academic setting.”
“I thought that [development of core competencies] was something that hospitalists as a group needed to do in order to a) become recognized and b) to clarify our own understanding and expectations of hospitalist physicians around the country,” he says.
—Tina Budnitz, MPH
Like her colleagues on the editorial board, Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist (BWF) Service (Boston), attended the 2002 SHM Education Summit and subsequently joined the Core Competencies Task Force. She is also co-chair of the society’s Career Satisfaction Task Force and views this role as linked to the missions of core competencies and education because education is a key component of professional advancement and engagement in the field. The Career Satisfaction Task Force, she notes, examines what components contribute to a long and satisfying career in hospital medicine.
Dr. McKean’s personal motivation for participation on the Core Competencies Task Force relates directly to her love of teaching. Having developed two hospitalist programs (one with physicians Andy Halpert, former chief of medicine for Harvard Vanguard Associations and subsequently the BWF program in 1998) she has seen firsthand that “people right out of residency do not have all the skills that they need in order to be effective hospitalists.”
As medical director of the BWF Hospitalist Service, Dr. McKean developed a weekly Harvard Medical School CME conference Update in Hospital Medicine for members of the hospitalist service, as well a medical consultation syllabus for the newest members of the hospitalist service to distribute to residents.
“I identified what the newest members of our service right out of residency didn’t learn during their residency training and tried to make sure that we would have people come in and teach them about hospital medicine,” she explains.
As the hospitalist service matured, hospitalists developed significant expertise in these topics and frequently participate in this didactic series of lectures.
“Initially,” recounts Dr. McKean, “I was the only senior physician with experience in hospital medicine, but now my job is much easier, as I continue to learn from other hospitalists in our program.”
—Sylvia C.W. McKean, MD, FACP
A Framework, Not a Text
“We have a great team,” says Dr. Amin of the Task Force editorial board. “I think our goals were clear. We wanted to develop a set of competencies that would be unique and offer 1) an opportunity to define the space that we, as hospitalists, lead in system-based practice; and 2) a framework that would cross over the span of time, so that others could use that framework to develop future curricula.
“Once you write a book, the context is fixed. We thought this [framework for curriculum development] was a creative way of facilitating future projects and ideas,” he continues. “It becomes more of a bible for competencies in hospital medicine.”
Budnitz says the idea was to develop an enduring, flexible blueprint. “We set out to develop a guide that would serve as a blueprint for curricular development in hospital medicine,” she explains. “We wanted to standardize the expectations for learning outcomes but still allow curriculum developers to add their expertise of content and context. Each chapter of the guide is written as a set of learning objectives. We crafted these objectives to clearly indicate a proficiency level.
“For example,” says Budnitz, “it is a different expectation that someone can list the drugs that they might order for a particular condition, versus analyzing the benefits and limitations of different therapeutic approaches. And in both scenarios we have left it up to the content and curriculum developers to determine the precise list of therapeutic agents that are included in curricula and the educational approach that will most likely yield the intended learning outcome.”
Dr. Dressler elaborates on his colleagues’ characterizations of the document: “We weren’t planning on this being an overarching, comprehensive text on hospital medicine. We were not trying to develop or even provide content.”
Instead, he says, the aim was to provide medical educators with a relatively generic framework that would retain flexibility for change. “For instance,” he explains, “if a new drug comes out that is useful for [treating] heart failure, the expectation is that hospitalists should be able to explain and utilize the new and useful medications, but that we were not going to list every drug in the Core Competencies compendium.”
“The one idea that we kept coming back to is that we wanted to design a set of competencies,” said Dr. Pistoria. “We didn’t want to publish a textbook; we didn’t want to come up with a curriculum per se. We wanted to come up with a framework that someone could use to develop their own hospitalist program in their own institution.”
Soliciting Input
The Core Competencies Task Force developed an initial organizational structure for the guide and a list of chapter topics. The resulting chapter list was turned into a survey and sent to the SHM Board of Directors, Core Competencies Task Force, and Education Committee. The survey was also sent to a sample of members within each SHM region or chapter via its chapter or region director. A review of core competencies generated by other medical specialties and allied health professional societies followed.
Then, the task force put out a call for nominations of chapter contributors. Budnitz judges that there were between 150-200 responses for potential contributors. Reviewing all the nominations was no small task. In some cases the editorial board deemed it necessary to recruit non-hospitalist content experts to generate some chapters, such as those dealing with medical-legal issues. In those instances, the “outside expert” was often paired with a hospitalist to ensure that the hospitalist perspective was included.
Strategies for Content Inclusion
Dr. Amin points out that the task force “went as broad and as wide as we could to get feedback on the content for the Core Competencies.” However, it was simply not possible—nor was it the editorial board’s intent—to compile an exhaustive list of all the hundreds of diagnoses that hospitalists may see on a regular basis. The editorial board identified common diagnoses from the top 15-20 DRGs from the Medicare database. The task was then to communicate the most important aspects of what hospitalists do, in the domains of knowledge, skills, and attitudes.
To manage the sheer bulk of solicited CVs and potential chapter authors, the editorial board used a divide-and-conquer strategy. Even so, says Dr. Pistoria, this process took a fair amount of time. When chapters began arriving and the task force was reduced to the core editorial board, “the homework started kicking up, with a lot of home editing time, telephone and e-mail editing, and some face-to-face meetings to ensure that chapters were standardized and had the same format.”
Once the editorial board began its work, it was relatively easy to decide that majority rule would be the best process for resolving differences of opinion, “but honestly,” says Dr. McKean, “only a handful of issues were generated. If we didn’t develop a consensus or if we were not all in agreement, then we sometimes looked for feedback from experts outside of the task force and the editorial board.”
Keeping with the ethos of inclusion, most board members consulted with other experts at their institution about key elements to include in the document.
Regarding the “majority rules” process, “Everyone had the chance during the editorial process to voice their opinions,” says Dr. Pistoria. “If they had concerns and were able to persuade enough people, the appropriate change would be made. I think, in the end, that everyone in the core editorial group felt that their opinions were heard, and I think that lends itself to the pride that we all feel in the final product.”
—Alpesh Amin, MD, MBA, FACP
A Work in Progress
Budnitz contributed critical guidance when the board generated writing guidelines for chapter authors. Each received a template for their chapter: a document instructing them how to write a competency, and a letter indicating the intent for their particular chapter. The template went through several iterations, she says, as early chapters were returned and the board began their editing.
For example, each clinical condition is discussed through the domains of knowledge, skills, and attitudes. It was the board’s job to ensure that concepts consistently appeared in the same domain across chapters with a similar degree of specificity and in the same order. “Partway through the process, we refined our template and made it more specific,” reports Budnitz. “We were able to give the second round of contributors a little more guidance as a result.
“We originally thought the document would be ready in early 2005,” she explains. “I think we were under the misimpression that the chapters would come back, that we’d read through them in a month or two, and it would be done. It turns out that just the sheer logistics of editing four or five versions of 70 chapters was quite a process.”
“I think [the Core Competencies] is something that SHM can be proud of,” said Dr. Pistoria of the group’s efforts. “But this is by no means the end of the project – it’s only the beginning. It is a work in progress.”
Dr. Dressler agreed with Dr. Pistoria’s characterization of the Core Competencies as a work in progress.
“I am pretty satisfied with what we’ve accomplished,” says Dr. Dressler. “By no means do I feel that this is the end-all, be-all for hospital medicine, or even for education in hospital medicine. It’s a start. We expect comment. We expect criticism. Being hospitalists, we are all open and aware and willing to make changes. And so we make a start, our initial best effort to get something out there that hospitalists can look at, utilize, and then offer feedback. Our primary goal is to provide a structure for consistency in practice and consistency in expectations. We would like to make [the Core Competencies] something that hospitalists and hospitalist educators feel is useful and that can change with the needs of our specialty.”
—Michael Pistoria, DO, FACP
Concluding Thoughts
“[Working on the Core Competencies] was an exciting project,” says Dr. Amin. “It took a lot of time. We had to spend a fair amount of time learning before we could actually define what we wanted from our chapter authors. But it was a good process. It was a four-year process to develop a document that would be worthwhile and hopefully stand the test of time in defining the core aspects of the field of hospital medicine. It was great to be chairing [the] education [committee] and seeing the value of helping to facilitate this project, and now looking more broadly across how to apply this project to future educational efforts.”
The project certainly had its challenges, most of which were related to time constraints.
“All of us were working very hard in our respective programs,” notes Dr. McKean, “and we were doing this on a volunteer basis. I think we had 10 face-to-face meetings, and sat at our computers on Saturday afternoons for conference calls using a Web-based editing program.”
For her part, Dr. McKean found working on the core competencies “very satisfying. I think I learned a lot from other people on this task force, editorial board, and the organization of the Society of Hospital Medicine. This project helped me reflect upon skills that I should try to obtain, and to think about more global issues than the day-to-day hospital politics in which I was involved. I did more strategic planning and thinking about retreats. So, it was a learning experience for me, and I also felt that I was contributing to something worthwhile. It was a chance to make a difference.
“From my own professional experience, the development process has helped me here, at Brigham and Women’s Hospital, so I hope that anyone who wants to apply the core competencies would feel free to e-mail us or contact us if they have any questions at all,” she says.
Dr. Pistoria agrees with Dr. McKean’s observations. “Working on the Core Competencies had a really big impact on me, both personally and professionally,” he says. “The process helped me mature in how I deal with running a project like this because I have been given the opportunity to do some similar things at my institution. Some of the ideas that we hit upon as we were editing and developing these competencies make one think, ‘We need to do this at our institution.’ Let’s take a strong look at, say, discharge processes, get a group together, and generate some recommendations that we can then institute.”
Other editorial board members also acknowledged that their participation gave them new insights into their own practice of hospital medicine.
“It’s easy to have in your head what you think is the right thing to do,” notes Dr. Dressler, “But until you actually have to try to develop consistency in wording and expectations, to put a process together that can result in a protocol, you realize that sometimes some elements get left out—for instance, the importance of family communication in the setting of DVT.”
Regarding the board members’ hard work, Budnitz remarks, “I can’t say enough about the dedication of the editorial board. They volunteered a tremendous amount of time and stuck with the project for three years. Since the board lived in multiple time zones, we often had calls where people would be participating at 6 a.m. or 9 p.m. We convened on weekends in multiple cities across the U.S. I sincerely enjoyed the opportunity to be a part of this project and hopefully impact the future of medical education.
“I think the document makes a bold statement. It defines the hospitalist as the captain of the ship—and calls on hospitalists to lead multidisciplinary teams to improve the quality of care. I hope it sparks interest and debate about how we recruit, train, prepare, and certify physicians in hospital medicine.”
Dr. Pistoria believes that the Core Competencies will advance hospitalist programs. In fact, he says, hospitalists around the country have already affected improvements in care coordination. The hospitalist movement in general furnishes hospitals with physicians who say, “ ‘I’m going to take ownership of what happens within the four walls of this hospital,’ ” says Dr. Pistoria. “Previous to that, people obviously cared about what happened in the hospital, but they also worried about their office practices. This is our office practice. We want it to work as well as it can for our patients, for us, for our nursing colleagues, for our janitors—everybody needs to, and should, benefit from this.” TH
Writer Gretchen Henkel wrote about cultural competency in the September issue of The Hospitalist.
If you want something done, the saying goes, ask a busy person to do it. That was precisely the situation when SHM’s Core Competencies Task Force editorial board was formed in May 2003. Charged with producing the society’s first-ever curriculum guidance document, the editorial team faced a daunting task: solicit, organize, and edit chapters for the competencies framework on topics from specific clinical conditions to ethical issues. Over the next two and a half years, each of the physician members contributed hundreds of hours of uncompensated time to the project, juggling work, family, and other professional obligations.
Because they are so involved with their own institutions and the future of hospital medicine, the physicians tapped to guide the core competencies to reality were the right pick.
“Working with the four of them was phenomenal,” says SHM staff member Tina Budnitz, MPH, who serves on both the Education Committee and the Core Competencies Task Force. “They are all incredibly hard working, driven, and intelligent. I think the hardest thing was just the logistics of coordinating schedules, since this was a volunteer activity for them.” Budnitz points out that the original target date for completion of the core competencies was early 2005. Instead, the sheer bulk of editing work pushed the deadline back to early 2006, when release of The Core Competencies in Hospital Medicine: A Framework for Curriculum Development by the Society of Hospital Medicine coincides with the premiere of the Journal of Hospital Medicine.
Recently, The Hospitalist caught up with each of the editorial board members, who divulged some of their personal motivations for participating in the ambitious core competencies project. They also discussed the workings of the editorial board and assessed the success of their efforts.
—Daniel D. Dressler, MD, MSc
Genesis and Vision
During a July 2002 Educational Summit the SHM Education Committee and Board of Directors determined that one element necessary to evolve SHM’s educational offerings would be a framework to guide and prioritize their efforts. A parallel conversation within the Education Committee, according to Budnitz, revolved around the need to better define hospital medicine. “We’re frequently asked, ‘what differentiates a hospitalist from other general internists? What exactly should the expectations be for a practicing hospitalist?’ ” she explains.
The Editorial Board
Michael J. Pistoria, DO, FACP, associate program director, Internal Medicine Residency, and medical director of both the Hospitalist Services and the Express Admission Unit at Lehigh Valley Hospital in Allentown, Pa., began his journey as chair of the Core Competencies Task Force shortly after SHM’s September 2002 Education Summit retreat.
Dr. Pistoria also serves on SHM’s Education Committee and admits that his allegiance to the field was a strong motivation for agreeing to participate in generating the Core Competencies.
“In my mind, hospital medicine is one of the neatest things in medicine to come along in a long time,” says Dr. Pistoria. “Hospital medicine has the potential to make a significant, positive difference in the way healthcare is delivered in the United States. And to have the opportunity to be a part of a process that helps define hospital medicine, to me, was just something almost too good to be true.”
A very active SHM member, Alpesh Amin, MD, MBA, FACP, is the associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California Irvine (UCI), where he also founded the UCI hospitalist program in 1998. His role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his key role in the Core Competencies Task Force editorial board.
“It was one of my goals—while chairing the Education Committee—for our society to put together the core competencies for hospital medicine,” says Dr. Amin. “I felt that if we had core competencies, this would be the next step to move us toward defining the field of hospital medicine.”
Accordingly, Dr. Amin was instrumental during the first and second SHM Education Summits in securing both committee and SHM Board of Directors’ buy-in of such a project.
For Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine, involvement with SHM’s (and formerly NAIP’s) Education Committee was a natural extension of his own interests in medical education. At Emory University Hospital, Dr. Dressler conducts a hospital medicine elective for house staff, “to give them a better understanding of what hospital medicine is and what we do, both in the community setting and in the academic setting.”
“I thought that [development of core competencies] was something that hospitalists as a group needed to do in order to a) become recognized and b) to clarify our own understanding and expectations of hospitalist physicians around the country,” he says.
—Tina Budnitz, MPH
Like her colleagues on the editorial board, Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist (BWF) Service (Boston), attended the 2002 SHM Education Summit and subsequently joined the Core Competencies Task Force. She is also co-chair of the society’s Career Satisfaction Task Force and views this role as linked to the missions of core competencies and education because education is a key component of professional advancement and engagement in the field. The Career Satisfaction Task Force, she notes, examines what components contribute to a long and satisfying career in hospital medicine.
Dr. McKean’s personal motivation for participation on the Core Competencies Task Force relates directly to her love of teaching. Having developed two hospitalist programs (one with physicians Andy Halpert, former chief of medicine for Harvard Vanguard Associations and subsequently the BWF program in 1998) she has seen firsthand that “people right out of residency do not have all the skills that they need in order to be effective hospitalists.”
As medical director of the BWF Hospitalist Service, Dr. McKean developed a weekly Harvard Medical School CME conference Update in Hospital Medicine for members of the hospitalist service, as well a medical consultation syllabus for the newest members of the hospitalist service to distribute to residents.
“I identified what the newest members of our service right out of residency didn’t learn during their residency training and tried to make sure that we would have people come in and teach them about hospital medicine,” she explains.
As the hospitalist service matured, hospitalists developed significant expertise in these topics and frequently participate in this didactic series of lectures.
“Initially,” recounts Dr. McKean, “I was the only senior physician with experience in hospital medicine, but now my job is much easier, as I continue to learn from other hospitalists in our program.”
—Sylvia C.W. McKean, MD, FACP
A Framework, Not a Text
“We have a great team,” says Dr. Amin of the Task Force editorial board. “I think our goals were clear. We wanted to develop a set of competencies that would be unique and offer 1) an opportunity to define the space that we, as hospitalists, lead in system-based practice; and 2) a framework that would cross over the span of time, so that others could use that framework to develop future curricula.
“Once you write a book, the context is fixed. We thought this [framework for curriculum development] was a creative way of facilitating future projects and ideas,” he continues. “It becomes more of a bible for competencies in hospital medicine.”
Budnitz says the idea was to develop an enduring, flexible blueprint. “We set out to develop a guide that would serve as a blueprint for curricular development in hospital medicine,” she explains. “We wanted to standardize the expectations for learning outcomes but still allow curriculum developers to add their expertise of content and context. Each chapter of the guide is written as a set of learning objectives. We crafted these objectives to clearly indicate a proficiency level.
“For example,” says Budnitz, “it is a different expectation that someone can list the drugs that they might order for a particular condition, versus analyzing the benefits and limitations of different therapeutic approaches. And in both scenarios we have left it up to the content and curriculum developers to determine the precise list of therapeutic agents that are included in curricula and the educational approach that will most likely yield the intended learning outcome.”
Dr. Dressler elaborates on his colleagues’ characterizations of the document: “We weren’t planning on this being an overarching, comprehensive text on hospital medicine. We were not trying to develop or even provide content.”
Instead, he says, the aim was to provide medical educators with a relatively generic framework that would retain flexibility for change. “For instance,” he explains, “if a new drug comes out that is useful for [treating] heart failure, the expectation is that hospitalists should be able to explain and utilize the new and useful medications, but that we were not going to list every drug in the Core Competencies compendium.”
“The one idea that we kept coming back to is that we wanted to design a set of competencies,” said Dr. Pistoria. “We didn’t want to publish a textbook; we didn’t want to come up with a curriculum per se. We wanted to come up with a framework that someone could use to develop their own hospitalist program in their own institution.”
Soliciting Input
The Core Competencies Task Force developed an initial organizational structure for the guide and a list of chapter topics. The resulting chapter list was turned into a survey and sent to the SHM Board of Directors, Core Competencies Task Force, and Education Committee. The survey was also sent to a sample of members within each SHM region or chapter via its chapter or region director. A review of core competencies generated by other medical specialties and allied health professional societies followed.
Then, the task force put out a call for nominations of chapter contributors. Budnitz judges that there were between 150-200 responses for potential contributors. Reviewing all the nominations was no small task. In some cases the editorial board deemed it necessary to recruit non-hospitalist content experts to generate some chapters, such as those dealing with medical-legal issues. In those instances, the “outside expert” was often paired with a hospitalist to ensure that the hospitalist perspective was included.
Strategies for Content Inclusion
Dr. Amin points out that the task force “went as broad and as wide as we could to get feedback on the content for the Core Competencies.” However, it was simply not possible—nor was it the editorial board’s intent—to compile an exhaustive list of all the hundreds of diagnoses that hospitalists may see on a regular basis. The editorial board identified common diagnoses from the top 15-20 DRGs from the Medicare database. The task was then to communicate the most important aspects of what hospitalists do, in the domains of knowledge, skills, and attitudes.
To manage the sheer bulk of solicited CVs and potential chapter authors, the editorial board used a divide-and-conquer strategy. Even so, says Dr. Pistoria, this process took a fair amount of time. When chapters began arriving and the task force was reduced to the core editorial board, “the homework started kicking up, with a lot of home editing time, telephone and e-mail editing, and some face-to-face meetings to ensure that chapters were standardized and had the same format.”
Once the editorial board began its work, it was relatively easy to decide that majority rule would be the best process for resolving differences of opinion, “but honestly,” says Dr. McKean, “only a handful of issues were generated. If we didn’t develop a consensus or if we were not all in agreement, then we sometimes looked for feedback from experts outside of the task force and the editorial board.”
Keeping with the ethos of inclusion, most board members consulted with other experts at their institution about key elements to include in the document.
Regarding the “majority rules” process, “Everyone had the chance during the editorial process to voice their opinions,” says Dr. Pistoria. “If they had concerns and were able to persuade enough people, the appropriate change would be made. I think, in the end, that everyone in the core editorial group felt that their opinions were heard, and I think that lends itself to the pride that we all feel in the final product.”
—Alpesh Amin, MD, MBA, FACP
A Work in Progress
Budnitz contributed critical guidance when the board generated writing guidelines for chapter authors. Each received a template for their chapter: a document instructing them how to write a competency, and a letter indicating the intent for their particular chapter. The template went through several iterations, she says, as early chapters were returned and the board began their editing.
For example, each clinical condition is discussed through the domains of knowledge, skills, and attitudes. It was the board’s job to ensure that concepts consistently appeared in the same domain across chapters with a similar degree of specificity and in the same order. “Partway through the process, we refined our template and made it more specific,” reports Budnitz. “We were able to give the second round of contributors a little more guidance as a result.
“We originally thought the document would be ready in early 2005,” she explains. “I think we were under the misimpression that the chapters would come back, that we’d read through them in a month or two, and it would be done. It turns out that just the sheer logistics of editing four or five versions of 70 chapters was quite a process.”
“I think [the Core Competencies] is something that SHM can be proud of,” said Dr. Pistoria of the group’s efforts. “But this is by no means the end of the project – it’s only the beginning. It is a work in progress.”
Dr. Dressler agreed with Dr. Pistoria’s characterization of the Core Competencies as a work in progress.
“I am pretty satisfied with what we’ve accomplished,” says Dr. Dressler. “By no means do I feel that this is the end-all, be-all for hospital medicine, or even for education in hospital medicine. It’s a start. We expect comment. We expect criticism. Being hospitalists, we are all open and aware and willing to make changes. And so we make a start, our initial best effort to get something out there that hospitalists can look at, utilize, and then offer feedback. Our primary goal is to provide a structure for consistency in practice and consistency in expectations. We would like to make [the Core Competencies] something that hospitalists and hospitalist educators feel is useful and that can change with the needs of our specialty.”
—Michael Pistoria, DO, FACP
Concluding Thoughts
“[Working on the Core Competencies] was an exciting project,” says Dr. Amin. “It took a lot of time. We had to spend a fair amount of time learning before we could actually define what we wanted from our chapter authors. But it was a good process. It was a four-year process to develop a document that would be worthwhile and hopefully stand the test of time in defining the core aspects of the field of hospital medicine. It was great to be chairing [the] education [committee] and seeing the value of helping to facilitate this project, and now looking more broadly across how to apply this project to future educational efforts.”
The project certainly had its challenges, most of which were related to time constraints.
“All of us were working very hard in our respective programs,” notes Dr. McKean, “and we were doing this on a volunteer basis. I think we had 10 face-to-face meetings, and sat at our computers on Saturday afternoons for conference calls using a Web-based editing program.”
For her part, Dr. McKean found working on the core competencies “very satisfying. I think I learned a lot from other people on this task force, editorial board, and the organization of the Society of Hospital Medicine. This project helped me reflect upon skills that I should try to obtain, and to think about more global issues than the day-to-day hospital politics in which I was involved. I did more strategic planning and thinking about retreats. So, it was a learning experience for me, and I also felt that I was contributing to something worthwhile. It was a chance to make a difference.
“From my own professional experience, the development process has helped me here, at Brigham and Women’s Hospital, so I hope that anyone who wants to apply the core competencies would feel free to e-mail us or contact us if they have any questions at all,” she says.
Dr. Pistoria agrees with Dr. McKean’s observations. “Working on the Core Competencies had a really big impact on me, both personally and professionally,” he says. “The process helped me mature in how I deal with running a project like this because I have been given the opportunity to do some similar things at my institution. Some of the ideas that we hit upon as we were editing and developing these competencies make one think, ‘We need to do this at our institution.’ Let’s take a strong look at, say, discharge processes, get a group together, and generate some recommendations that we can then institute.”
Other editorial board members also acknowledged that their participation gave them new insights into their own practice of hospital medicine.
“It’s easy to have in your head what you think is the right thing to do,” notes Dr. Dressler, “But until you actually have to try to develop consistency in wording and expectations, to put a process together that can result in a protocol, you realize that sometimes some elements get left out—for instance, the importance of family communication in the setting of DVT.”
Regarding the board members’ hard work, Budnitz remarks, “I can’t say enough about the dedication of the editorial board. They volunteered a tremendous amount of time and stuck with the project for three years. Since the board lived in multiple time zones, we often had calls where people would be participating at 6 a.m. or 9 p.m. We convened on weekends in multiple cities across the U.S. I sincerely enjoyed the opportunity to be a part of this project and hopefully impact the future of medical education.
“I think the document makes a bold statement. It defines the hospitalist as the captain of the ship—and calls on hospitalists to lead multidisciplinary teams to improve the quality of care. I hope it sparks interest and debate about how we recruit, train, prepare, and certify physicians in hospital medicine.”
Dr. Pistoria believes that the Core Competencies will advance hospitalist programs. In fact, he says, hospitalists around the country have already affected improvements in care coordination. The hospitalist movement in general furnishes hospitals with physicians who say, “ ‘I’m going to take ownership of what happens within the four walls of this hospital,’ ” says Dr. Pistoria. “Previous to that, people obviously cared about what happened in the hospital, but they also worried about their office practices. This is our office practice. We want it to work as well as it can for our patients, for us, for our nursing colleagues, for our janitors—everybody needs to, and should, benefit from this.” TH
Writer Gretchen Henkel wrote about cultural competency in the September issue of The Hospitalist.
Are You Culturally Competent?
As the diversity of the U.S. population increases, so do the challenges for hospitalists, as they seek to deliver truly patient-centered care in the 21st century. The March 2002 Institute of Medicine report, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care,” concluded that, while some care inequities can be attributed to access and linguistic barriers, healthcare providers themselves may contribute to disparities in care for their minority patients.1
How can hospitalists ensure that they bridge the cultural divide between themselves and their patients from different racial, ethnic, and cultural backgrounds and avoid potential missteps in care delivery?
An Open Mind
Experts in cultural competency interviewed for this article explained that hospitalists can readily acquire the knowledge and skills necessary to effectively provide patient-centered care for all their patients. (See “Resource List,” p. 27.) But the most critical element in culturally competent healthcare delivery is the attitude with which the provider approaches his or her patients.
“I don’t think we can teach attitude,” says Alicia Fernandez, MD, assistant clinical professor of medicine, Division of General Internal Medicine, University of California, San Francisco, a nationally known researcher on language barriers and former full-time hospitalist. “But I think that any doctor who’s trying to do the best he or she can by their individual patients has the right attitude, which is to remain open to practicing patient-centered care.”

—Jack Percelay, MD
Physicians must be able to approach each patient on his or her own terms, and to acknowledge that members of different racial and ethnic groups hold beliefs about health and illness that diverge from those of Western medicine.
“You really need to have the capacity to empathize, and turn off all of your own belief systems, in some cases, to listen,” says Stacy Goldsholl, MD, a hospitalist based in Wilmington, N.C., and an SHM Board member.
Dr. Goldsholl recalls one situation involving a patient who was a Jehovah’s Witness who entered the hospital with a gastrointestinal bleed. Because of religious proscriptions, the patient refused a blood transfusion.
“It was extremely difficult as a scientist-trained physician, to watch someone bleed to a hemoglobin of 5, knowing that a simple transfusion would save this patient,” recalls Dr. Goldsholl.
The patient later underwent surgery without a transfusion and survived, but Dr. Goldsholl believes this case illustrates that delivering patient-centered care requires the practice not just of the science—but the art—of medicine.
“I think the real message is, you have to think outside of your own box,” she offers. “In addition, the cultural issues become much more pronounced when you start to approach end-of-life issues that take on more of a cultural, ethnic. and spiritual dimension.”
Awareness and Knowledge
Mitchell D. Wilson, MD, believes “the average American tends to be very ethnocentric. We are not taught cultural awareness in recognizing our own inherent biases, so we are unable to take the next step and recognize that there is a gap between our culture and another person’s culture that would require us to take a different approach.”
Dr. Wilson is associate professor of medicine, medical director and physician advisor, Department of Clinical Care Management, University of North Carolina (UNC) Hospitals, and section chief of hospital medicine and medical director, FirstHealth of the Carolinas Hospitalist Services, UNC School of Medicine, Chapel Hill. He is also an SHM Board member.
Dr. Wilson says that his own cultural awareness emanated from participation in a spirituality and medicine program for student doctors and nurses at the medical school where he trained and was later on faculty.
“I was able to function both as a small group facilitator and a large group panelist, and we used a case-based format for creating awareness of spirituality in medicine,” he explains.
Dr. Wilson notes that he later drew on these experiences when, as a hospitalist at a regional medical center, he was called to admit a woman to the hospital from the emergency department. She was dressed in traditional Muslim clothing and spoke no English. Knowing that it is offensive for traditional Islamic women to be examined by a man, Dr. Wilson asked through the woman’s friends who had accompanied the woman whether she would prefer a woman doctor and whether she would be comfortable at least with his taking her history. She answered “yes” to both questions.
Dr. Wilson prevailed upon a female doctor in a competing practice to perform the examination and also made a special effort to admit the patient to the female physician in his own group who would be working the next day.
“It’s not that I’ve been trained in cultural awareness,” he says, “but this case points out the importance of recognizing other traditions, so that you can deliver care that is effective and culturally sensitive.”
Earning Trust
Maren Grainger-Monsen, MD, senior research scholar and director of the Biomedical Ethics in Film Program at the Stanford University Center for Biomedical Ethics (Calif.), has produced several award-winning films about patients from different racial and ethnic groups and their interface with the healthcare delivery system. In the process of filming patients with their families, she has realized that as a physician she often mistook respect for trust.
Patients, she says, “would be respectful and polite and seeming to agree with me, but as I have worked on these films and spent time with families, I realize that they approach the physician and the hospital system with more caution and they wait to see if the people are trustworthy.”
Jack Percelay, MD, chair, American Academy of Pediatrics Section on Hospital Medicine and SHM Board member, notes that “hospitalists face more difficulty with some cultural issues than primary care providers because we’re thrust into a situation of an acute illness, whereas the primary care provider at least gets an opportunity to establish a relationship. In pediatric hospital medicine, we need to be very careful and cognizant of this, make sure we employ translation resources and social workers, and be hesitant to judge someone else’s value system, while still advocating for the patient.”
While it can be important to acquire a baseline of knowledge about dominant cultural and religious groups (especially if a group comprises a sizable percentage of patients seen at one’s institution), Dr. Fernandez cautions against using a laundry list approach to cultural competency.
“It’s helpful to know, for instance, that many Vietnamese here came as a result of the Vietnam War,” she says. “On the other hand, it is not that helpful to say [something like], ‘Don’t shake hands with Vietnamese.’ Our patients are forgiving of whether we shake hands or don’t shake hands. They are less forgiving when we appear not to listen to them.”
Lost in Translation
Nearly 14% of people who live in the United States speak a language other than English in their homes, according to the U.S. Census Bureau’s Census 2000 estimates.2 When a person with limited English proficiency (LEP) enters the healthcare system, the potential for medical error increases if language barriers are not addressed. Indeed, healthcare institutions that receive federal healthcare dollars (Medicare, Medicaid) are obligated under Title VI of the Civil Rights Act of 1964 to provide access to interpreter services—free of charge—to LEP patients.
Those interviewed for this article advised that physicians should avail themselves of trained medical interpreters whenever possible. These professionals are trained to translate providers’ and patients’ communications verbatim—without editing—and are conversant with medical terminology.
However, such resources may not be available in rural hospitals. Such is the case for William D. Atchley, Jr., MD, medical director of the Hospitalist Service at Sentara Careplex Hospital in Hampton, Va., who recently used a cafeteria staff person to translate while he examined and admitted a Mexico-born patient with rhabdomyolysis that resulted from heat exhaustion. Dr. Atchley, an SHM Board member, has also used family members as translators. He notes, though, that “trying to get an understanding of what is going on can be difficult at times because the one family member who may act as a translator may not have as good a command of English [as a trained medical interpreter]. You are always fearful that something could get lost in translation.”
Even large institutions that have medical interpreters on staff may not have 24-hour coverage. In that case, telephone interpreters through AT&T’s Language Line service can be another option (www.languageline.com). Physicians can also work with ad-hoc interpreters, defined as family members or friends who act as interpreters, but are not professionally trained, says Dr. Fernandez.
“It can pay off to first take a few minutes to explain to these interpreters that you want them to repeat everything they hear as much word for word as they can,” she explains. “Tell them that you will give them time to participate in the conversation—as a family member—later on. First, you want them to play this narrow role as interpreter, and later you will let them add information as the family member because their contribution is also valuable.”
Young people, including teenage children, should not be used to interpret unless the situation is immediately life-threatening. “There has been a lot of research,” says Dr. Fernandez, “showing that [using children as interpreters] distorts family roles and makes the children uncomfortable.”
For example, says Dr. Grainger-Monsen, it would be completely inappropriate for a child to translate while a physician asks his mother about her past sexual history or vaginal bleeding.

The Time It Takes
At San Francisco General Hospital, where Dr. Fernandez is an attending physician, there are 140 languages spoken each month. She says the variety of patient backgrounds presents a challenge even for someone like herself, who has conducted extensive research on barriers to minority healthcare. She admits that she sometimes experiences an “internal groan” when she notices that the next patient in her busy clinic day is someone who speaks a language that she doesn’t. Like many of the hospitalists interviewed for this article, Dr. Fernandez notes that because using medical interpreters is time-consuming, she experiences initial resistance to the process.
A 2004 Canadian study examined the relationship between length of stay and LEP in the ambulatory care setting. It found that LEP patients stayed in the hospital longer for conditions, such as unstable coronary syndromes and chest pain, stroke, diabetes, and elective hip replacement.3
Issues about cultural competency are “fairly complex,” notes Alpesh Amin, MD, MBA, FACP, executive director Hospitalist Program and vice chair for clinical affairs, Department of Medicine at the University of California, Irvine, and SHM Board member. Sorting through issues surrounding patients’ beliefs toward healthcare, as well as their family values and dynamics, “takes time to resolve, and if I really want to understand your personal beliefs, I’ve got to be willing to sit down and talk about it. But, I’m not going to get paid for that time. This is not a reimbursable expense for the physician.”
Still, taking time to explore a patient’s preferences could also shorten length of stay if, for instance, the patient indicated that prescribed management indicated after an expensive test would not be his choice of care, says Dr. Amin.
Understanding what beliefs and experiences patients bring to the table, as well as their past health behaviors, does involve a time investment, agrees Minn.-based Russell Holman, MD, national medical director for Cogent Healthcare, Inc. and SHM Board member. But that investment “can only help efficiency,” he maintains. “We’ve invested ourselves tremendously in terms of identifying what are best practices for a patient with heart failure, or pneumonia, or heart attack, but the cultural competency dimension of healthcare has been largely overlooked.”
Training in cultural competency is piecemeal at best, notes Dr. Holman, and often acquired on the job. He recalls a situation in which he learned first-hand the profound effect that culture has on health. While working with a Hmong man who was in a coma and on a ventilator, Dr. Holman initially attempted to seek decision-making from the patient’s wife.
“I found out that was not the appropriate decision-making process for their culture,” says Dr. Holman. The discussion was initiated in the patient’s room, and was moved to a lecture-style classroom to accommodate the 37 members of the man’s clan who came to discuss his condition.
“The fascinating thing to me was that the patient’s wife and the other women sat in the back of the classroom and did not speak the entire time,” explains Dr. Holman. “The decisions were largely conducted by the clan elders. I also found out that my patient was the clan leader, and the elders had very clear goals in mind. The goal was to keep this individual alive, because he was so important as a figure in the clan. I learned that their culture had a profound impact on their expectations of me as a physician and a provider—how I conducted myself in terms of family and clan communications, what resources I brought to bear to try and stabilize and improve his health, and how I worked with specialists. I also learned that although some clan and family members were fluent in English, even modest miscommunications, if I were to use them as translators, could result in significant setbacks.”
Prior to his current position with Cogent Healthcare, Dr. Holman managed a group of 30 hospitalists at HealthPartners Medical Group in Minnesota and in partnership with the Center for International Health developed a cultural competency curriculum for their group and for the University of Minnesota residents in training at Regions Hospital in St. Paul.
“When you are busy working in the hospital, you need to be able to quickly access some resources to be able to give you a ‘just in time’ amount of information and awareness” with which to approach your patient, he says.
Agents for Change?
In addition to Title VI compliance, hospitals are now surveyed by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and are evaluated on their ability to provide language services.
“This is a changing area,” notes Dr. Fernandez, “and I think it is important for hospitalists to be on the forefront of that change, part of the process that says, ‘Yes, we need to be able to provide more efficient, more patient-centered, and safer care.’ Language barriers, as one example, are inefficient, are dangerous, and are clearly associated with increased medical error.”
Dr. Percelay believes that dealing with patients from different backgrounds involves using “common sense, being respectful and legitimately curious, and avoiding shortcuts in terms of translation issues. I think if people have an inherent respect for diversity, and are open to it, it can enrich your practice.”
Dr. Fernandez agrees. “Practicing medicine in a patient-centered way is ultimately a more rewarding way to work and live,” she says. “There also needs to be reform at a national level that allows physicians and hospitalists to be appropriately compensated for much of the conversation and bedside work that we do.” TH
Writer Gretchen Henkel lives in California and writes regularly about healthcare.
References
- Unequal Treatment: Understanding Racial and Ethnic Disparities in Health Care. Institute of Medicine, National Academy of Sciences. 2002. Available from the National Academy Press Available at http://books.nap.edu/catalog/11036.html. Last accessed July 27, 2005; and Unequal Treatment: What Healthcare Providers Need to Know about Racial and Ethnic Disparities in Healthcare. Institute of Medicine, National Academy of Sciences. Available at www.nap.edu/catalog/10260.html. Last accessed July 27, 2005.
- Shin HB, Bruno R. Language use and English-speaking ability: a Census 2000 brief. U.S. Census Bureau, 2003. Available online at www.census.gov/population/www/cen2000/briefs.html. Last accessed July 27, 2005.
- John-Baptiste A, Naglie G, Tomlinson G, et al. The effect of English language proficiency on length of stay and in-hospital mortality. J Gen Intern Med. March 2004;19(3):221-228.
As the diversity of the U.S. population increases, so do the challenges for hospitalists, as they seek to deliver truly patient-centered care in the 21st century. The March 2002 Institute of Medicine report, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care,” concluded that, while some care inequities can be attributed to access and linguistic barriers, healthcare providers themselves may contribute to disparities in care for their minority patients.1
How can hospitalists ensure that they bridge the cultural divide between themselves and their patients from different racial, ethnic, and cultural backgrounds and avoid potential missteps in care delivery?
An Open Mind
Experts in cultural competency interviewed for this article explained that hospitalists can readily acquire the knowledge and skills necessary to effectively provide patient-centered care for all their patients. (See “Resource List,” p. 27.) But the most critical element in culturally competent healthcare delivery is the attitude with which the provider approaches his or her patients.
“I don’t think we can teach attitude,” says Alicia Fernandez, MD, assistant clinical professor of medicine, Division of General Internal Medicine, University of California, San Francisco, a nationally known researcher on language barriers and former full-time hospitalist. “But I think that any doctor who’s trying to do the best he or she can by their individual patients has the right attitude, which is to remain open to practicing patient-centered care.”
—Jack Percelay, MD
Physicians must be able to approach each patient on his or her own terms, and to acknowledge that members of different racial and ethnic groups hold beliefs about health and illness that diverge from those of Western medicine.
“You really need to have the capacity to empathize, and turn off all of your own belief systems, in some cases, to listen,” says Stacy Goldsholl, MD, a hospitalist based in Wilmington, N.C., and an SHM Board member.
Dr. Goldsholl recalls one situation involving a patient who was a Jehovah’s Witness who entered the hospital with a gastrointestinal bleed. Because of religious proscriptions, the patient refused a blood transfusion.
“It was extremely difficult as a scientist-trained physician, to watch someone bleed to a hemoglobin of 5, knowing that a simple transfusion would save this patient,” recalls Dr. Goldsholl.
The patient later underwent surgery without a transfusion and survived, but Dr. Goldsholl believes this case illustrates that delivering patient-centered care requires the practice not just of the science—but the art—of medicine.
“I think the real message is, you have to think outside of your own box,” she offers. “In addition, the cultural issues become much more pronounced when you start to approach end-of-life issues that take on more of a cultural, ethnic. and spiritual dimension.”
Awareness and Knowledge
Mitchell D. Wilson, MD, believes “the average American tends to be very ethnocentric. We are not taught cultural awareness in recognizing our own inherent biases, so we are unable to take the next step and recognize that there is a gap between our culture and another person’s culture that would require us to take a different approach.”
Dr. Wilson is associate professor of medicine, medical director and physician advisor, Department of Clinical Care Management, University of North Carolina (UNC) Hospitals, and section chief of hospital medicine and medical director, FirstHealth of the Carolinas Hospitalist Services, UNC School of Medicine, Chapel Hill. He is also an SHM Board member.
Dr. Wilson says that his own cultural awareness emanated from participation in a spirituality and medicine program for student doctors and nurses at the medical school where he trained and was later on faculty.
“I was able to function both as a small group facilitator and a large group panelist, and we used a case-based format for creating awareness of spirituality in medicine,” he explains.
Dr. Wilson notes that he later drew on these experiences when, as a hospitalist at a regional medical center, he was called to admit a woman to the hospital from the emergency department. She was dressed in traditional Muslim clothing and spoke no English. Knowing that it is offensive for traditional Islamic women to be examined by a man, Dr. Wilson asked through the woman’s friends who had accompanied the woman whether she would prefer a woman doctor and whether she would be comfortable at least with his taking her history. She answered “yes” to both questions.
Dr. Wilson prevailed upon a female doctor in a competing practice to perform the examination and also made a special effort to admit the patient to the female physician in his own group who would be working the next day.
“It’s not that I’ve been trained in cultural awareness,” he says, “but this case points out the importance of recognizing other traditions, so that you can deliver care that is effective and culturally sensitive.”
Earning Trust
Maren Grainger-Monsen, MD, senior research scholar and director of the Biomedical Ethics in Film Program at the Stanford University Center for Biomedical Ethics (Calif.), has produced several award-winning films about patients from different racial and ethnic groups and their interface with the healthcare delivery system. In the process of filming patients with their families, she has realized that as a physician she often mistook respect for trust.
Patients, she says, “would be respectful and polite and seeming to agree with me, but as I have worked on these films and spent time with families, I realize that they approach the physician and the hospital system with more caution and they wait to see if the people are trustworthy.”
Jack Percelay, MD, chair, American Academy of Pediatrics Section on Hospital Medicine and SHM Board member, notes that “hospitalists face more difficulty with some cultural issues than primary care providers because we’re thrust into a situation of an acute illness, whereas the primary care provider at least gets an opportunity to establish a relationship. In pediatric hospital medicine, we need to be very careful and cognizant of this, make sure we employ translation resources and social workers, and be hesitant to judge someone else’s value system, while still advocating for the patient.”
While it can be important to acquire a baseline of knowledge about dominant cultural and religious groups (especially if a group comprises a sizable percentage of patients seen at one’s institution), Dr. Fernandez cautions against using a laundry list approach to cultural competency.
“It’s helpful to know, for instance, that many Vietnamese here came as a result of the Vietnam War,” she says. “On the other hand, it is not that helpful to say [something like], ‘Don’t shake hands with Vietnamese.’ Our patients are forgiving of whether we shake hands or don’t shake hands. They are less forgiving when we appear not to listen to them.”
Lost in Translation
Nearly 14% of people who live in the United States speak a language other than English in their homes, according to the U.S. Census Bureau’s Census 2000 estimates.2 When a person with limited English proficiency (LEP) enters the healthcare system, the potential for medical error increases if language barriers are not addressed. Indeed, healthcare institutions that receive federal healthcare dollars (Medicare, Medicaid) are obligated under Title VI of the Civil Rights Act of 1964 to provide access to interpreter services—free of charge—to LEP patients.
Those interviewed for this article advised that physicians should avail themselves of trained medical interpreters whenever possible. These professionals are trained to translate providers’ and patients’ communications verbatim—without editing—and are conversant with medical terminology.
However, such resources may not be available in rural hospitals. Such is the case for William D. Atchley, Jr., MD, medical director of the Hospitalist Service at Sentara Careplex Hospital in Hampton, Va., who recently used a cafeteria staff person to translate while he examined and admitted a Mexico-born patient with rhabdomyolysis that resulted from heat exhaustion. Dr. Atchley, an SHM Board member, has also used family members as translators. He notes, though, that “trying to get an understanding of what is going on can be difficult at times because the one family member who may act as a translator may not have as good a command of English [as a trained medical interpreter]. You are always fearful that something could get lost in translation.”
Even large institutions that have medical interpreters on staff may not have 24-hour coverage. In that case, telephone interpreters through AT&T’s Language Line service can be another option (www.languageline.com). Physicians can also work with ad-hoc interpreters, defined as family members or friends who act as interpreters, but are not professionally trained, says Dr. Fernandez.
“It can pay off to first take a few minutes to explain to these interpreters that you want them to repeat everything they hear as much word for word as they can,” she explains. “Tell them that you will give them time to participate in the conversation—as a family member—later on. First, you want them to play this narrow role as interpreter, and later you will let them add information as the family member because their contribution is also valuable.”
Young people, including teenage children, should not be used to interpret unless the situation is immediately life-threatening. “There has been a lot of research,” says Dr. Fernandez, “showing that [using children as interpreters] distorts family roles and makes the children uncomfortable.”
For example, says Dr. Grainger-Monsen, it would be completely inappropriate for a child to translate while a physician asks his mother about her past sexual history or vaginal bleeding.
The Time It Takes
At San Francisco General Hospital, where Dr. Fernandez is an attending physician, there are 140 languages spoken each month. She says the variety of patient backgrounds presents a challenge even for someone like herself, who has conducted extensive research on barriers to minority healthcare. She admits that she sometimes experiences an “internal groan” when she notices that the next patient in her busy clinic day is someone who speaks a language that she doesn’t. Like many of the hospitalists interviewed for this article, Dr. Fernandez notes that because using medical interpreters is time-consuming, she experiences initial resistance to the process.
A 2004 Canadian study examined the relationship between length of stay and LEP in the ambulatory care setting. It found that LEP patients stayed in the hospital longer for conditions, such as unstable coronary syndromes and chest pain, stroke, diabetes, and elective hip replacement.3
Issues about cultural competency are “fairly complex,” notes Alpesh Amin, MD, MBA, FACP, executive director Hospitalist Program and vice chair for clinical affairs, Department of Medicine at the University of California, Irvine, and SHM Board member. Sorting through issues surrounding patients’ beliefs toward healthcare, as well as their family values and dynamics, “takes time to resolve, and if I really want to understand your personal beliefs, I’ve got to be willing to sit down and talk about it. But, I’m not going to get paid for that time. This is not a reimbursable expense for the physician.”
Still, taking time to explore a patient’s preferences could also shorten length of stay if, for instance, the patient indicated that prescribed management indicated after an expensive test would not be his choice of care, says Dr. Amin.
Understanding what beliefs and experiences patients bring to the table, as well as their past health behaviors, does involve a time investment, agrees Minn.-based Russell Holman, MD, national medical director for Cogent Healthcare, Inc. and SHM Board member. But that investment “can only help efficiency,” he maintains. “We’ve invested ourselves tremendously in terms of identifying what are best practices for a patient with heart failure, or pneumonia, or heart attack, but the cultural competency dimension of healthcare has been largely overlooked.”
Training in cultural competency is piecemeal at best, notes Dr. Holman, and often acquired on the job. He recalls a situation in which he learned first-hand the profound effect that culture has on health. While working with a Hmong man who was in a coma and on a ventilator, Dr. Holman initially attempted to seek decision-making from the patient’s wife.
“I found out that was not the appropriate decision-making process for their culture,” says Dr. Holman. The discussion was initiated in the patient’s room, and was moved to a lecture-style classroom to accommodate the 37 members of the man’s clan who came to discuss his condition.
“The fascinating thing to me was that the patient’s wife and the other women sat in the back of the classroom and did not speak the entire time,” explains Dr. Holman. “The decisions were largely conducted by the clan elders. I also found out that my patient was the clan leader, and the elders had very clear goals in mind. The goal was to keep this individual alive, because he was so important as a figure in the clan. I learned that their culture had a profound impact on their expectations of me as a physician and a provider—how I conducted myself in terms of family and clan communications, what resources I brought to bear to try and stabilize and improve his health, and how I worked with specialists. I also learned that although some clan and family members were fluent in English, even modest miscommunications, if I were to use them as translators, could result in significant setbacks.”
Prior to his current position with Cogent Healthcare, Dr. Holman managed a group of 30 hospitalists at HealthPartners Medical Group in Minnesota and in partnership with the Center for International Health developed a cultural competency curriculum for their group and for the University of Minnesota residents in training at Regions Hospital in St. Paul.
“When you are busy working in the hospital, you need to be able to quickly access some resources to be able to give you a ‘just in time’ amount of information and awareness” with which to approach your patient, he says.
Agents for Change?
In addition to Title VI compliance, hospitals are now surveyed by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and are evaluated on their ability to provide language services.
“This is a changing area,” notes Dr. Fernandez, “and I think it is important for hospitalists to be on the forefront of that change, part of the process that says, ‘Yes, we need to be able to provide more efficient, more patient-centered, and safer care.’ Language barriers, as one example, are inefficient, are dangerous, and are clearly associated with increased medical error.”
Dr. Percelay believes that dealing with patients from different backgrounds involves using “common sense, being respectful and legitimately curious, and avoiding shortcuts in terms of translation issues. I think if people have an inherent respect for diversity, and are open to it, it can enrich your practice.”
Dr. Fernandez agrees. “Practicing medicine in a patient-centered way is ultimately a more rewarding way to work and live,” she says. “There also needs to be reform at a national level that allows physicians and hospitalists to be appropriately compensated for much of the conversation and bedside work that we do.” TH
Writer Gretchen Henkel lives in California and writes regularly about healthcare.
References
- Unequal Treatment: Understanding Racial and Ethnic Disparities in Health Care. Institute of Medicine, National Academy of Sciences. 2002. Available from the National Academy Press Available at http://books.nap.edu/catalog/11036.html. Last accessed July 27, 2005; and Unequal Treatment: What Healthcare Providers Need to Know about Racial and Ethnic Disparities in Healthcare. Institute of Medicine, National Academy of Sciences. Available at www.nap.edu/catalog/10260.html. Last accessed July 27, 2005.
- Shin HB, Bruno R. Language use and English-speaking ability: a Census 2000 brief. U.S. Census Bureau, 2003. Available online at www.census.gov/population/www/cen2000/briefs.html. Last accessed July 27, 2005.
- John-Baptiste A, Naglie G, Tomlinson G, et al. The effect of English language proficiency on length of stay and in-hospital mortality. J Gen Intern Med. March 2004;19(3):221-228.
As the diversity of the U.S. population increases, so do the challenges for hospitalists, as they seek to deliver truly patient-centered care in the 21st century. The March 2002 Institute of Medicine report, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care,” concluded that, while some care inequities can be attributed to access and linguistic barriers, healthcare providers themselves may contribute to disparities in care for their minority patients.1
How can hospitalists ensure that they bridge the cultural divide between themselves and their patients from different racial, ethnic, and cultural backgrounds and avoid potential missteps in care delivery?
An Open Mind
Experts in cultural competency interviewed for this article explained that hospitalists can readily acquire the knowledge and skills necessary to effectively provide patient-centered care for all their patients. (See “Resource List,” p. 27.) But the most critical element in culturally competent healthcare delivery is the attitude with which the provider approaches his or her patients.
“I don’t think we can teach attitude,” says Alicia Fernandez, MD, assistant clinical professor of medicine, Division of General Internal Medicine, University of California, San Francisco, a nationally known researcher on language barriers and former full-time hospitalist. “But I think that any doctor who’s trying to do the best he or she can by their individual patients has the right attitude, which is to remain open to practicing patient-centered care.”
—Jack Percelay, MD
Physicians must be able to approach each patient on his or her own terms, and to acknowledge that members of different racial and ethnic groups hold beliefs about health and illness that diverge from those of Western medicine.
“You really need to have the capacity to empathize, and turn off all of your own belief systems, in some cases, to listen,” says Stacy Goldsholl, MD, a hospitalist based in Wilmington, N.C., and an SHM Board member.
Dr. Goldsholl recalls one situation involving a patient who was a Jehovah’s Witness who entered the hospital with a gastrointestinal bleed. Because of religious proscriptions, the patient refused a blood transfusion.
“It was extremely difficult as a scientist-trained physician, to watch someone bleed to a hemoglobin of 5, knowing that a simple transfusion would save this patient,” recalls Dr. Goldsholl.
The patient later underwent surgery without a transfusion and survived, but Dr. Goldsholl believes this case illustrates that delivering patient-centered care requires the practice not just of the science—but the art—of medicine.
“I think the real message is, you have to think outside of your own box,” she offers. “In addition, the cultural issues become much more pronounced when you start to approach end-of-life issues that take on more of a cultural, ethnic. and spiritual dimension.”
Awareness and Knowledge
Mitchell D. Wilson, MD, believes “the average American tends to be very ethnocentric. We are not taught cultural awareness in recognizing our own inherent biases, so we are unable to take the next step and recognize that there is a gap between our culture and another person’s culture that would require us to take a different approach.”
Dr. Wilson is associate professor of medicine, medical director and physician advisor, Department of Clinical Care Management, University of North Carolina (UNC) Hospitals, and section chief of hospital medicine and medical director, FirstHealth of the Carolinas Hospitalist Services, UNC School of Medicine, Chapel Hill. He is also an SHM Board member.
Dr. Wilson says that his own cultural awareness emanated from participation in a spirituality and medicine program for student doctors and nurses at the medical school where he trained and was later on faculty.
“I was able to function both as a small group facilitator and a large group panelist, and we used a case-based format for creating awareness of spirituality in medicine,” he explains.
Dr. Wilson notes that he later drew on these experiences when, as a hospitalist at a regional medical center, he was called to admit a woman to the hospital from the emergency department. She was dressed in traditional Muslim clothing and spoke no English. Knowing that it is offensive for traditional Islamic women to be examined by a man, Dr. Wilson asked through the woman’s friends who had accompanied the woman whether she would prefer a woman doctor and whether she would be comfortable at least with his taking her history. She answered “yes” to both questions.
Dr. Wilson prevailed upon a female doctor in a competing practice to perform the examination and also made a special effort to admit the patient to the female physician in his own group who would be working the next day.
“It’s not that I’ve been trained in cultural awareness,” he says, “but this case points out the importance of recognizing other traditions, so that you can deliver care that is effective and culturally sensitive.”
Earning Trust
Maren Grainger-Monsen, MD, senior research scholar and director of the Biomedical Ethics in Film Program at the Stanford University Center for Biomedical Ethics (Calif.), has produced several award-winning films about patients from different racial and ethnic groups and their interface with the healthcare delivery system. In the process of filming patients with their families, she has realized that as a physician she often mistook respect for trust.
Patients, she says, “would be respectful and polite and seeming to agree with me, but as I have worked on these films and spent time with families, I realize that they approach the physician and the hospital system with more caution and they wait to see if the people are trustworthy.”
Jack Percelay, MD, chair, American Academy of Pediatrics Section on Hospital Medicine and SHM Board member, notes that “hospitalists face more difficulty with some cultural issues than primary care providers because we’re thrust into a situation of an acute illness, whereas the primary care provider at least gets an opportunity to establish a relationship. In pediatric hospital medicine, we need to be very careful and cognizant of this, make sure we employ translation resources and social workers, and be hesitant to judge someone else’s value system, while still advocating for the patient.”
While it can be important to acquire a baseline of knowledge about dominant cultural and religious groups (especially if a group comprises a sizable percentage of patients seen at one’s institution), Dr. Fernandez cautions against using a laundry list approach to cultural competency.
“It’s helpful to know, for instance, that many Vietnamese here came as a result of the Vietnam War,” she says. “On the other hand, it is not that helpful to say [something like], ‘Don’t shake hands with Vietnamese.’ Our patients are forgiving of whether we shake hands or don’t shake hands. They are less forgiving when we appear not to listen to them.”
Lost in Translation
Nearly 14% of people who live in the United States speak a language other than English in their homes, according to the U.S. Census Bureau’s Census 2000 estimates.2 When a person with limited English proficiency (LEP) enters the healthcare system, the potential for medical error increases if language barriers are not addressed. Indeed, healthcare institutions that receive federal healthcare dollars (Medicare, Medicaid) are obligated under Title VI of the Civil Rights Act of 1964 to provide access to interpreter services—free of charge—to LEP patients.
Those interviewed for this article advised that physicians should avail themselves of trained medical interpreters whenever possible. These professionals are trained to translate providers’ and patients’ communications verbatim—without editing—and are conversant with medical terminology.
However, such resources may not be available in rural hospitals. Such is the case for William D. Atchley, Jr., MD, medical director of the Hospitalist Service at Sentara Careplex Hospital in Hampton, Va., who recently used a cafeteria staff person to translate while he examined and admitted a Mexico-born patient with rhabdomyolysis that resulted from heat exhaustion. Dr. Atchley, an SHM Board member, has also used family members as translators. He notes, though, that “trying to get an understanding of what is going on can be difficult at times because the one family member who may act as a translator may not have as good a command of English [as a trained medical interpreter]. You are always fearful that something could get lost in translation.”
Even large institutions that have medical interpreters on staff may not have 24-hour coverage. In that case, telephone interpreters through AT&T’s Language Line service can be another option (www.languageline.com). Physicians can also work with ad-hoc interpreters, defined as family members or friends who act as interpreters, but are not professionally trained, says Dr. Fernandez.
“It can pay off to first take a few minutes to explain to these interpreters that you want them to repeat everything they hear as much word for word as they can,” she explains. “Tell them that you will give them time to participate in the conversation—as a family member—later on. First, you want them to play this narrow role as interpreter, and later you will let them add information as the family member because their contribution is also valuable.”
Young people, including teenage children, should not be used to interpret unless the situation is immediately life-threatening. “There has been a lot of research,” says Dr. Fernandez, “showing that [using children as interpreters] distorts family roles and makes the children uncomfortable.”
For example, says Dr. Grainger-Monsen, it would be completely inappropriate for a child to translate while a physician asks his mother about her past sexual history or vaginal bleeding.
The Time It Takes
At San Francisco General Hospital, where Dr. Fernandez is an attending physician, there are 140 languages spoken each month. She says the variety of patient backgrounds presents a challenge even for someone like herself, who has conducted extensive research on barriers to minority healthcare. She admits that she sometimes experiences an “internal groan” when she notices that the next patient in her busy clinic day is someone who speaks a language that she doesn’t. Like many of the hospitalists interviewed for this article, Dr. Fernandez notes that because using medical interpreters is time-consuming, she experiences initial resistance to the process.
A 2004 Canadian study examined the relationship between length of stay and LEP in the ambulatory care setting. It found that LEP patients stayed in the hospital longer for conditions, such as unstable coronary syndromes and chest pain, stroke, diabetes, and elective hip replacement.3
Issues about cultural competency are “fairly complex,” notes Alpesh Amin, MD, MBA, FACP, executive director Hospitalist Program and vice chair for clinical affairs, Department of Medicine at the University of California, Irvine, and SHM Board member. Sorting through issues surrounding patients’ beliefs toward healthcare, as well as their family values and dynamics, “takes time to resolve, and if I really want to understand your personal beliefs, I’ve got to be willing to sit down and talk about it. But, I’m not going to get paid for that time. This is not a reimbursable expense for the physician.”
Still, taking time to explore a patient’s preferences could also shorten length of stay if, for instance, the patient indicated that prescribed management indicated after an expensive test would not be his choice of care, says Dr. Amin.
Understanding what beliefs and experiences patients bring to the table, as well as their past health behaviors, does involve a time investment, agrees Minn.-based Russell Holman, MD, national medical director for Cogent Healthcare, Inc. and SHM Board member. But that investment “can only help efficiency,” he maintains. “We’ve invested ourselves tremendously in terms of identifying what are best practices for a patient with heart failure, or pneumonia, or heart attack, but the cultural competency dimension of healthcare has been largely overlooked.”
Training in cultural competency is piecemeal at best, notes Dr. Holman, and often acquired on the job. He recalls a situation in which he learned first-hand the profound effect that culture has on health. While working with a Hmong man who was in a coma and on a ventilator, Dr. Holman initially attempted to seek decision-making from the patient’s wife.
“I found out that was not the appropriate decision-making process for their culture,” says Dr. Holman. The discussion was initiated in the patient’s room, and was moved to a lecture-style classroom to accommodate the 37 members of the man’s clan who came to discuss his condition.
“The fascinating thing to me was that the patient’s wife and the other women sat in the back of the classroom and did not speak the entire time,” explains Dr. Holman. “The decisions were largely conducted by the clan elders. I also found out that my patient was the clan leader, and the elders had very clear goals in mind. The goal was to keep this individual alive, because he was so important as a figure in the clan. I learned that their culture had a profound impact on their expectations of me as a physician and a provider—how I conducted myself in terms of family and clan communications, what resources I brought to bear to try and stabilize and improve his health, and how I worked with specialists. I also learned that although some clan and family members were fluent in English, even modest miscommunications, if I were to use them as translators, could result in significant setbacks.”
Prior to his current position with Cogent Healthcare, Dr. Holman managed a group of 30 hospitalists at HealthPartners Medical Group in Minnesota and in partnership with the Center for International Health developed a cultural competency curriculum for their group and for the University of Minnesota residents in training at Regions Hospital in St. Paul.
“When you are busy working in the hospital, you need to be able to quickly access some resources to be able to give you a ‘just in time’ amount of information and awareness” with which to approach your patient, he says.
Agents for Change?
In addition to Title VI compliance, hospitals are now surveyed by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and are evaluated on their ability to provide language services.
“This is a changing area,” notes Dr. Fernandez, “and I think it is important for hospitalists to be on the forefront of that change, part of the process that says, ‘Yes, we need to be able to provide more efficient, more patient-centered, and safer care.’ Language barriers, as one example, are inefficient, are dangerous, and are clearly associated with increased medical error.”
Dr. Percelay believes that dealing with patients from different backgrounds involves using “common sense, being respectful and legitimately curious, and avoiding shortcuts in terms of translation issues. I think if people have an inherent respect for diversity, and are open to it, it can enrich your practice.”
Dr. Fernandez agrees. “Practicing medicine in a patient-centered way is ultimately a more rewarding way to work and live,” she says. “There also needs to be reform at a national level that allows physicians and hospitalists to be appropriately compensated for much of the conversation and bedside work that we do.” TH
Writer Gretchen Henkel lives in California and writes regularly about healthcare.
References
- Unequal Treatment: Understanding Racial and Ethnic Disparities in Health Care. Institute of Medicine, National Academy of Sciences. 2002. Available from the National Academy Press Available at http://books.nap.edu/catalog/11036.html. Last accessed July 27, 2005; and Unequal Treatment: What Healthcare Providers Need to Know about Racial and Ethnic Disparities in Healthcare. Institute of Medicine, National Academy of Sciences. Available at www.nap.edu/catalog/10260.html. Last accessed July 27, 2005.
- Shin HB, Bruno R. Language use and English-speaking ability: a Census 2000 brief. U.S. Census Bureau, 2003. Available online at www.census.gov/population/www/cen2000/briefs.html. Last accessed July 27, 2005.
- John-Baptiste A, Naglie G, Tomlinson G, et al. The effect of English language proficiency on length of stay and in-hospital mortality. J Gen Intern Med. March 2004;19(3):221-228.