User login
Hospitalist Burnout
Long hours, extreme dedication to their work, and an overload of responsibility can make physicians more prone to burnout than other professionals. And hospitalists are no exception because they may experience more causes of burnout than other types of physicians.
Here are some basic facts about burnout among physicians, how to determine if you are burning out, and what to do about it.
Facts about Physician Burnout
In her presentation “Burnout and Hospitalists” at the 2005 SHM Annual Meeting in Chicago, Tosha Wetterneck, MD, hospitalist and assistant professor of medicine at University of Wisconsin (Madison), defined physician burnout as “erosion of engagement with the job.” The components of this erosion can include emotional exhaustion, depersonalization (distancing yourself from your job), and reduced personal accomplishment.
“Burnout,” said Dr. Wetterneck in her presentation, “is caused by work overload and time pressure, as well as role ambiguity, lack of job resources or support, severity of patient problems, and lack of reciprocity from patients.” Other factors include a perceived loss of control and rapid changes on the job.
Hospitalists in particular may be prone to burnout because they work under high expectations—their own as well as others’—to provide better outcomes. A 1999 study by the National Association of Inpatient Physicians (SHM’s former name) revealed a 13% burnout rate among hospitalists, with an additional 25% at risk for burnout. That may sound high, but emergency and critical care physicians experience burnout rates of up to 60%.
What to Do about Burnout
Lidia Schapira, MD, an oncologist at Massachusetts General Hospital, Boston, has written and spoken on the subject of physician burnout.
“It’s a real phenomenon,” she explains, “and in part it reflects an exaggerated commitment to work. But a professional who loves what they do—if they have support—can [experience] enthusiasm rather than burnout.”
Without support from their organization or colleagues, a physician can become overwhelmed by the long hours and responsibilities of work, among other stressors. Here are Dr. Schapira’s steps for dealing with burnout:
1. Recognize it: “The symptoms [of burnout] are very similar to depression,” she points out. “One way to distinguish between burnout and depression is to take a little holiday from work. If your symptoms are connected to work, you’ll feel better. If you feel equally bad on vacation, you probably suffer from depression.”
2. Address your stressors: If you realize you are burned out, your next step should be to make a list of on-the-job stressors and prioritize them. Then tackle them one at a time. “You have to identify the things that are most stressful to you and make changes,” says Dr. Schapira. “For example, if your schedule is overloaded, find a way to build in breaks for food or fresh air.”
If there are specific parts of the job that are “horrible” for you, she says, try to delegate them to someone else on your team. By delegating or swapping tasks with others, you may be able to eliminate your burnout—and possibly theirs as well. Another important factor is having an ally. “Find someone on your team who you can talk to,” advises Dr. Schapira. “Chat with your colleagues about your problems.”
3. Work for organizational change: Hospitalists can talk to their administrators and colleagues about easy changes that can eliminate stressors, such as a change to the schedule, improved communications or additional secretarial help to ease the burden.
“Point out that a change may lead to more productivity,” suggests Dr. Schapira. “There’s a far better likelihood of having your changes accepted.” To help ensure that your employer is willing to make some changes, point out that burnout in general is associated with turnover and absenteeism, lower productivity, and stress-related health outcomes including alcohol and drug abuse.
Find a Good Fit
One key to avoiding burnout is to make sure you find an employer you can be happy with.
“There are as many different styles of management as there are hospitalist groups,” says Michael-Anthony Williams, MD, president of Inpatient Services, PC, in Denver. “It’s important that the doctors in a group share values and have the same goal. There’s no right answer.”
Dr. Schapira agrees. “There needs to be a good fit between the physician and the workplace,” she says. “If you’re the only person constantly upset by the system, maybe you’re not working in the right place.”
Dr. Williams, a co-presenter with Dr. Wetterneck in Chicago, outlined how his hospital medicine group has combated burnout by hiring physicians who seem likely to be a good fit. Dr. Williams realized that the hospitalists at Inpatient Services value time off over monetary gain.
“Our group is not motivated by finances,” he explains. “The salaries aren’t as high here, and Denver attracts physicians who aren’t seeking a lot of money.” Therefore Inpatient Services provides more time off. “Everyone gets one vacation request each month,” [per person] says Dr. Williams. “Day-to-day, the job is very unpredictable. So we try to give people control over their schedule.”
Burnout is a serious emotional condition that can lead some hospitalists and other physicians to seek a change in career—or lead them to substance abuse or other problems. The good news is that identifying it in the first place and then advocating to change workplace conditions can overcome it. TH
Long hours, extreme dedication to their work, and an overload of responsibility can make physicians more prone to burnout than other professionals. And hospitalists are no exception because they may experience more causes of burnout than other types of physicians.
Here are some basic facts about burnout among physicians, how to determine if you are burning out, and what to do about it.
Facts about Physician Burnout
In her presentation “Burnout and Hospitalists” at the 2005 SHM Annual Meeting in Chicago, Tosha Wetterneck, MD, hospitalist and assistant professor of medicine at University of Wisconsin (Madison), defined physician burnout as “erosion of engagement with the job.” The components of this erosion can include emotional exhaustion, depersonalization (distancing yourself from your job), and reduced personal accomplishment.
“Burnout,” said Dr. Wetterneck in her presentation, “is caused by work overload and time pressure, as well as role ambiguity, lack of job resources or support, severity of patient problems, and lack of reciprocity from patients.” Other factors include a perceived loss of control and rapid changes on the job.
Hospitalists in particular may be prone to burnout because they work under high expectations—their own as well as others’—to provide better outcomes. A 1999 study by the National Association of Inpatient Physicians (SHM’s former name) revealed a 13% burnout rate among hospitalists, with an additional 25% at risk for burnout. That may sound high, but emergency and critical care physicians experience burnout rates of up to 60%.
What to Do about Burnout
Lidia Schapira, MD, an oncologist at Massachusetts General Hospital, Boston, has written and spoken on the subject of physician burnout.
“It’s a real phenomenon,” she explains, “and in part it reflects an exaggerated commitment to work. But a professional who loves what they do—if they have support—can [experience] enthusiasm rather than burnout.”
Without support from their organization or colleagues, a physician can become overwhelmed by the long hours and responsibilities of work, among other stressors. Here are Dr. Schapira’s steps for dealing with burnout:
1. Recognize it: “The symptoms [of burnout] are very similar to depression,” she points out. “One way to distinguish between burnout and depression is to take a little holiday from work. If your symptoms are connected to work, you’ll feel better. If you feel equally bad on vacation, you probably suffer from depression.”
2. Address your stressors: If you realize you are burned out, your next step should be to make a list of on-the-job stressors and prioritize them. Then tackle them one at a time. “You have to identify the things that are most stressful to you and make changes,” says Dr. Schapira. “For example, if your schedule is overloaded, find a way to build in breaks for food or fresh air.”
If there are specific parts of the job that are “horrible” for you, she says, try to delegate them to someone else on your team. By delegating or swapping tasks with others, you may be able to eliminate your burnout—and possibly theirs as well. Another important factor is having an ally. “Find someone on your team who you can talk to,” advises Dr. Schapira. “Chat with your colleagues about your problems.”
3. Work for organizational change: Hospitalists can talk to their administrators and colleagues about easy changes that can eliminate stressors, such as a change to the schedule, improved communications or additional secretarial help to ease the burden.
“Point out that a change may lead to more productivity,” suggests Dr. Schapira. “There’s a far better likelihood of having your changes accepted.” To help ensure that your employer is willing to make some changes, point out that burnout in general is associated with turnover and absenteeism, lower productivity, and stress-related health outcomes including alcohol and drug abuse.
Find a Good Fit
One key to avoiding burnout is to make sure you find an employer you can be happy with.
“There are as many different styles of management as there are hospitalist groups,” says Michael-Anthony Williams, MD, president of Inpatient Services, PC, in Denver. “It’s important that the doctors in a group share values and have the same goal. There’s no right answer.”
Dr. Schapira agrees. “There needs to be a good fit between the physician and the workplace,” she says. “If you’re the only person constantly upset by the system, maybe you’re not working in the right place.”
Dr. Williams, a co-presenter with Dr. Wetterneck in Chicago, outlined how his hospital medicine group has combated burnout by hiring physicians who seem likely to be a good fit. Dr. Williams realized that the hospitalists at Inpatient Services value time off over monetary gain.
“Our group is not motivated by finances,” he explains. “The salaries aren’t as high here, and Denver attracts physicians who aren’t seeking a lot of money.” Therefore Inpatient Services provides more time off. “Everyone gets one vacation request each month,” [per person] says Dr. Williams. “Day-to-day, the job is very unpredictable. So we try to give people control over their schedule.”
Burnout is a serious emotional condition that can lead some hospitalists and other physicians to seek a change in career—or lead them to substance abuse or other problems. The good news is that identifying it in the first place and then advocating to change workplace conditions can overcome it. TH
Long hours, extreme dedication to their work, and an overload of responsibility can make physicians more prone to burnout than other professionals. And hospitalists are no exception because they may experience more causes of burnout than other types of physicians.
Here are some basic facts about burnout among physicians, how to determine if you are burning out, and what to do about it.
Facts about Physician Burnout
In her presentation “Burnout and Hospitalists” at the 2005 SHM Annual Meeting in Chicago, Tosha Wetterneck, MD, hospitalist and assistant professor of medicine at University of Wisconsin (Madison), defined physician burnout as “erosion of engagement with the job.” The components of this erosion can include emotional exhaustion, depersonalization (distancing yourself from your job), and reduced personal accomplishment.
“Burnout,” said Dr. Wetterneck in her presentation, “is caused by work overload and time pressure, as well as role ambiguity, lack of job resources or support, severity of patient problems, and lack of reciprocity from patients.” Other factors include a perceived loss of control and rapid changes on the job.
Hospitalists in particular may be prone to burnout because they work under high expectations—their own as well as others’—to provide better outcomes. A 1999 study by the National Association of Inpatient Physicians (SHM’s former name) revealed a 13% burnout rate among hospitalists, with an additional 25% at risk for burnout. That may sound high, but emergency and critical care physicians experience burnout rates of up to 60%.
What to Do about Burnout
Lidia Schapira, MD, an oncologist at Massachusetts General Hospital, Boston, has written and spoken on the subject of physician burnout.
“It’s a real phenomenon,” she explains, “and in part it reflects an exaggerated commitment to work. But a professional who loves what they do—if they have support—can [experience] enthusiasm rather than burnout.”
Without support from their organization or colleagues, a physician can become overwhelmed by the long hours and responsibilities of work, among other stressors. Here are Dr. Schapira’s steps for dealing with burnout:
1. Recognize it: “The symptoms [of burnout] are very similar to depression,” she points out. “One way to distinguish between burnout and depression is to take a little holiday from work. If your symptoms are connected to work, you’ll feel better. If you feel equally bad on vacation, you probably suffer from depression.”
2. Address your stressors: If you realize you are burned out, your next step should be to make a list of on-the-job stressors and prioritize them. Then tackle them one at a time. “You have to identify the things that are most stressful to you and make changes,” says Dr. Schapira. “For example, if your schedule is overloaded, find a way to build in breaks for food or fresh air.”
If there are specific parts of the job that are “horrible” for you, she says, try to delegate them to someone else on your team. By delegating or swapping tasks with others, you may be able to eliminate your burnout—and possibly theirs as well. Another important factor is having an ally. “Find someone on your team who you can talk to,” advises Dr. Schapira. “Chat with your colleagues about your problems.”
3. Work for organizational change: Hospitalists can talk to their administrators and colleagues about easy changes that can eliminate stressors, such as a change to the schedule, improved communications or additional secretarial help to ease the burden.
“Point out that a change may lead to more productivity,” suggests Dr. Schapira. “There’s a far better likelihood of having your changes accepted.” To help ensure that your employer is willing to make some changes, point out that burnout in general is associated with turnover and absenteeism, lower productivity, and stress-related health outcomes including alcohol and drug abuse.
Find a Good Fit
One key to avoiding burnout is to make sure you find an employer you can be happy with.
“There are as many different styles of management as there are hospitalist groups,” says Michael-Anthony Williams, MD, president of Inpatient Services, PC, in Denver. “It’s important that the doctors in a group share values and have the same goal. There’s no right answer.”
Dr. Schapira agrees. “There needs to be a good fit between the physician and the workplace,” she says. “If you’re the only person constantly upset by the system, maybe you’re not working in the right place.”
Dr. Williams, a co-presenter with Dr. Wetterneck in Chicago, outlined how his hospital medicine group has combated burnout by hiring physicians who seem likely to be a good fit. Dr. Williams realized that the hospitalists at Inpatient Services value time off over monetary gain.
“Our group is not motivated by finances,” he explains. “The salaries aren’t as high here, and Denver attracts physicians who aren’t seeking a lot of money.” Therefore Inpatient Services provides more time off. “Everyone gets one vacation request each month,” [per person] says Dr. Williams. “Day-to-day, the job is very unpredictable. So we try to give people control over their schedule.”
Burnout is a serious emotional condition that can lead some hospitalists and other physicians to seek a change in career—or lead them to substance abuse or other problems. The good news is that identifying it in the first place and then advocating to change workplace conditions can overcome it. TH
Medicare Pays for Performance
The future of a Medicare-sponsored pay-for-performance model for hospitals rests on a three-year trial involving 268 hospitals and millions of dollars in bonuses.
The Centers for Medicare and Medicaid Services (CMS) has partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, to undertake The Premier Hospital Quality Incentive Demonstration Project. Premier was selected for this demonstration project because each of its hospital members has a database system in place that allows tracking and reporting of data for 34 quality measures.
“This is the only [pay-for-performance project] for hospitals at this time,” says Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS.
The project began in October 2003. At the end of each of the three years of the trial, top-performing hospitals are rewarded with cash bonuses from CMS. Performance is based on multiple evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. The individual measures are compiled into an overall quality score for each clinical condition.
“The administration is extremely interested in pay for performance in general, and very pleased with the project,” says Wynn. “The administrator is interested in expanding pay for performance to other hospitals, but exact details on this are not available.”
Money Matters
The pay structure of the project rewards those Premier hospitals that rank highest for each quality measure: Hospitals that rank in the top 20% of quality for the five general clinical areas receive a bonus. Those in the top 10% for each of the quality measures will receive a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% will receive a 1% bonus.
In the first year of the project, Medicare spent approximately $8.9 million in incentive bonuses, and bonuses per hospital ranged from $847,000 to $900,000. This money comes, in part, from savings earned by improved outcomes, including shorter hospital stays and fewer readmissions.
Overall, though, participants seem to believe that the real payoff is not in dollars, but in improved quality of care as well as public recognition of their outcomes. (CMS has agreed not to reveal the names of the 130 lowest-performing hospitals, but the top performers are enjoying positive publicity.)
“Quality is the key motivator,” says Bill M. Hazelwood, MD, FCCP, McLeod Regional Medical Center, Florence, S.C. “Money doesn’t do anything for me—I’m sure my administrators think differently. But our efforts have paid off in lives saved and in people getting home quicker.”
Winning Ways
Hackensack University Medical Center (N.J.) and McLeod Regional Medical Center each scored in the top 20% for all five clinical conditions. Hackensack earned the largest total bonus for the first year, receiving $848,000. A hospitalist from each of these institutions shares insights into their success.
Gerard A. Burns, MD, MBA, director of medical informatics at Hackensack University Medical Center, explains that meeting the quality measures set by Medicare for the project was not new. “Some are process measures like giving aspirin, and some are outcome measures, like our mortality rates,” he says. “Many are tried and true, and not totally foreign to all hospitals. We’ve seen these things before.”
A few of the measures require no additional work from staff. “Some are automatically calculated by the Premier databases,” says Dr. Burns. “There’s no data collection involved in some of these.”
Every week or month, each hospital downloads all of the coded data. The facility also receives results on how they are doing. “We get quarterly reports to see where we’re doing well and where we’re not doing well,” says Dr. Burns. “We may see too many re-admits, and ask, ‘What’s going on?’ We’ll take a closer look. Each time is a great opportunity to improve our scores.”
Many, if not most, of the participating hospitals saw immediate improvements for multiple quality measures. The problem is that now that the project is in its last year, it’s more difficult to find ways to improve.
“The big push from here on out is fine-tuning and finding new areas for improvement,” says Dr. Hazelwood. “We hope to plug in new information and improve outcomes. And, by its nature, we’ll have to increase the number of protocols. They help us in the hustle and bustle of daily practice.”
How Hospitalists Help
In a handful of top-ranked hospitals, hospitalists play an active role in helping to meet the quality measures.
“Our hospitalists contribute in three ways,” says Dr. Burns. “We have five full-time hospitalists in the emergency department to assist our ED physicians and admitting physicians. They use specific disease order sets with built-in processes for medications, etc. Using a hospitalist to assist or write these orders is one more layer on the team to ensure we do the right thing.”
In addition, hospitalists at Hackensack are often included in new multidisciplinary team rounds. “We have multidisciplinary teams of a physician—sometimes a hospitalist—along with a nurse manager, a case manager, a social worker, a nutritionist, and sometimes a pharmacist,” explains Dr. Burns. “The team discusses each patient and tries to facilitate the physician’s plan of care. They may have to bring in a coding person to help figure out the coding rules.”
And having hospitalists involved with patients admitted without primary care physicians is “a tremendous help,” according to Dr. Burns, “because they really focus on our care measures. And each month, we have new residents come in, and the hospitalists train them on the project.”
As for McLeod Regional Medical Center, Dr. Hazelwood says, “Hospitalists are big admitters to the hospital—especially for those unassigned patients. And like other physicians, we are involved in various physician-led committees that develop our protocol for change.”
Are top-ranking hospitals sharing their bonus earnings with participating hospitalists and other physicians? “As far as I know, that has not happened, and it will not happen,” says Charles Riccobono, MD, chairman of the Performance Improvement Department at Hackensack. “I would hope that [bonus] money will filter down to support other quality projects, but I don’t know if the funds have been earmarked for anything specific.”
The Future Impact
The outcome of The Premier Hospital Quality Incentive Demonstration Project will shape any pay-for-performance guidelines that Medicare sets for hospitals around the country, including new or revised protocols and data collection hospital-wide. Final information will be available soon after the project ends this fall. Meanwhile, all data collected on the quality measures is available on the CMS Web site at www.cms.hhs.gov/HospitalQualityInits/35_HospitalPremier.asp. TH
The future of a Medicare-sponsored pay-for-performance model for hospitals rests on a three-year trial involving 268 hospitals and millions of dollars in bonuses.
The Centers for Medicare and Medicaid Services (CMS) has partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, to undertake The Premier Hospital Quality Incentive Demonstration Project. Premier was selected for this demonstration project because each of its hospital members has a database system in place that allows tracking and reporting of data for 34 quality measures.
“This is the only [pay-for-performance project] for hospitals at this time,” says Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS.
The project began in October 2003. At the end of each of the three years of the trial, top-performing hospitals are rewarded with cash bonuses from CMS. Performance is based on multiple evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. The individual measures are compiled into an overall quality score for each clinical condition.
“The administration is extremely interested in pay for performance in general, and very pleased with the project,” says Wynn. “The administrator is interested in expanding pay for performance to other hospitals, but exact details on this are not available.”
Money Matters
The pay structure of the project rewards those Premier hospitals that rank highest for each quality measure: Hospitals that rank in the top 20% of quality for the five general clinical areas receive a bonus. Those in the top 10% for each of the quality measures will receive a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% will receive a 1% bonus.
In the first year of the project, Medicare spent approximately $8.9 million in incentive bonuses, and bonuses per hospital ranged from $847,000 to $900,000. This money comes, in part, from savings earned by improved outcomes, including shorter hospital stays and fewer readmissions.
Overall, though, participants seem to believe that the real payoff is not in dollars, but in improved quality of care as well as public recognition of their outcomes. (CMS has agreed not to reveal the names of the 130 lowest-performing hospitals, but the top performers are enjoying positive publicity.)
“Quality is the key motivator,” says Bill M. Hazelwood, MD, FCCP, McLeod Regional Medical Center, Florence, S.C. “Money doesn’t do anything for me—I’m sure my administrators think differently. But our efforts have paid off in lives saved and in people getting home quicker.”
Winning Ways
Hackensack University Medical Center (N.J.) and McLeod Regional Medical Center each scored in the top 20% for all five clinical conditions. Hackensack earned the largest total bonus for the first year, receiving $848,000. A hospitalist from each of these institutions shares insights into their success.
Gerard A. Burns, MD, MBA, director of medical informatics at Hackensack University Medical Center, explains that meeting the quality measures set by Medicare for the project was not new. “Some are process measures like giving aspirin, and some are outcome measures, like our mortality rates,” he says. “Many are tried and true, and not totally foreign to all hospitals. We’ve seen these things before.”
A few of the measures require no additional work from staff. “Some are automatically calculated by the Premier databases,” says Dr. Burns. “There’s no data collection involved in some of these.”
Every week or month, each hospital downloads all of the coded data. The facility also receives results on how they are doing. “We get quarterly reports to see where we’re doing well and where we’re not doing well,” says Dr. Burns. “We may see too many re-admits, and ask, ‘What’s going on?’ We’ll take a closer look. Each time is a great opportunity to improve our scores.”
Many, if not most, of the participating hospitals saw immediate improvements for multiple quality measures. The problem is that now that the project is in its last year, it’s more difficult to find ways to improve.
“The big push from here on out is fine-tuning and finding new areas for improvement,” says Dr. Hazelwood. “We hope to plug in new information and improve outcomes. And, by its nature, we’ll have to increase the number of protocols. They help us in the hustle and bustle of daily practice.”
How Hospitalists Help
In a handful of top-ranked hospitals, hospitalists play an active role in helping to meet the quality measures.
“Our hospitalists contribute in three ways,” says Dr. Burns. “We have five full-time hospitalists in the emergency department to assist our ED physicians and admitting physicians. They use specific disease order sets with built-in processes for medications, etc. Using a hospitalist to assist or write these orders is one more layer on the team to ensure we do the right thing.”
In addition, hospitalists at Hackensack are often included in new multidisciplinary team rounds. “We have multidisciplinary teams of a physician—sometimes a hospitalist—along with a nurse manager, a case manager, a social worker, a nutritionist, and sometimes a pharmacist,” explains Dr. Burns. “The team discusses each patient and tries to facilitate the physician’s plan of care. They may have to bring in a coding person to help figure out the coding rules.”
And having hospitalists involved with patients admitted without primary care physicians is “a tremendous help,” according to Dr. Burns, “because they really focus on our care measures. And each month, we have new residents come in, and the hospitalists train them on the project.”
As for McLeod Regional Medical Center, Dr. Hazelwood says, “Hospitalists are big admitters to the hospital—especially for those unassigned patients. And like other physicians, we are involved in various physician-led committees that develop our protocol for change.”
Are top-ranking hospitals sharing their bonus earnings with participating hospitalists and other physicians? “As far as I know, that has not happened, and it will not happen,” says Charles Riccobono, MD, chairman of the Performance Improvement Department at Hackensack. “I would hope that [bonus] money will filter down to support other quality projects, but I don’t know if the funds have been earmarked for anything specific.”
The Future Impact
The outcome of The Premier Hospital Quality Incentive Demonstration Project will shape any pay-for-performance guidelines that Medicare sets for hospitals around the country, including new or revised protocols and data collection hospital-wide. Final information will be available soon after the project ends this fall. Meanwhile, all data collected on the quality measures is available on the CMS Web site at www.cms.hhs.gov/HospitalQualityInits/35_HospitalPremier.asp. TH
The future of a Medicare-sponsored pay-for-performance model for hospitals rests on a three-year trial involving 268 hospitals and millions of dollars in bonuses.
The Centers for Medicare and Medicaid Services (CMS) has partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, to undertake The Premier Hospital Quality Incentive Demonstration Project. Premier was selected for this demonstration project because each of its hospital members has a database system in place that allows tracking and reporting of data for 34 quality measures.
“This is the only [pay-for-performance project] for hospitals at this time,” says Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS.
The project began in October 2003. At the end of each of the three years of the trial, top-performing hospitals are rewarded with cash bonuses from CMS. Performance is based on multiple evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. The individual measures are compiled into an overall quality score for each clinical condition.
“The administration is extremely interested in pay for performance in general, and very pleased with the project,” says Wynn. “The administrator is interested in expanding pay for performance to other hospitals, but exact details on this are not available.”
Money Matters
The pay structure of the project rewards those Premier hospitals that rank highest for each quality measure: Hospitals that rank in the top 20% of quality for the five general clinical areas receive a bonus. Those in the top 10% for each of the quality measures will receive a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% will receive a 1% bonus.
In the first year of the project, Medicare spent approximately $8.9 million in incentive bonuses, and bonuses per hospital ranged from $847,000 to $900,000. This money comes, in part, from savings earned by improved outcomes, including shorter hospital stays and fewer readmissions.
Overall, though, participants seem to believe that the real payoff is not in dollars, but in improved quality of care as well as public recognition of their outcomes. (CMS has agreed not to reveal the names of the 130 lowest-performing hospitals, but the top performers are enjoying positive publicity.)
“Quality is the key motivator,” says Bill M. Hazelwood, MD, FCCP, McLeod Regional Medical Center, Florence, S.C. “Money doesn’t do anything for me—I’m sure my administrators think differently. But our efforts have paid off in lives saved and in people getting home quicker.”
Winning Ways
Hackensack University Medical Center (N.J.) and McLeod Regional Medical Center each scored in the top 20% for all five clinical conditions. Hackensack earned the largest total bonus for the first year, receiving $848,000. A hospitalist from each of these institutions shares insights into their success.
Gerard A. Burns, MD, MBA, director of medical informatics at Hackensack University Medical Center, explains that meeting the quality measures set by Medicare for the project was not new. “Some are process measures like giving aspirin, and some are outcome measures, like our mortality rates,” he says. “Many are tried and true, and not totally foreign to all hospitals. We’ve seen these things before.”
A few of the measures require no additional work from staff. “Some are automatically calculated by the Premier databases,” says Dr. Burns. “There’s no data collection involved in some of these.”
Every week or month, each hospital downloads all of the coded data. The facility also receives results on how they are doing. “We get quarterly reports to see where we’re doing well and where we’re not doing well,” says Dr. Burns. “We may see too many re-admits, and ask, ‘What’s going on?’ We’ll take a closer look. Each time is a great opportunity to improve our scores.”
Many, if not most, of the participating hospitals saw immediate improvements for multiple quality measures. The problem is that now that the project is in its last year, it’s more difficult to find ways to improve.
“The big push from here on out is fine-tuning and finding new areas for improvement,” says Dr. Hazelwood. “We hope to plug in new information and improve outcomes. And, by its nature, we’ll have to increase the number of protocols. They help us in the hustle and bustle of daily practice.”
How Hospitalists Help
In a handful of top-ranked hospitals, hospitalists play an active role in helping to meet the quality measures.
“Our hospitalists contribute in three ways,” says Dr. Burns. “We have five full-time hospitalists in the emergency department to assist our ED physicians and admitting physicians. They use specific disease order sets with built-in processes for medications, etc. Using a hospitalist to assist or write these orders is one more layer on the team to ensure we do the right thing.”
In addition, hospitalists at Hackensack are often included in new multidisciplinary team rounds. “We have multidisciplinary teams of a physician—sometimes a hospitalist—along with a nurse manager, a case manager, a social worker, a nutritionist, and sometimes a pharmacist,” explains Dr. Burns. “The team discusses each patient and tries to facilitate the physician’s plan of care. They may have to bring in a coding person to help figure out the coding rules.”
And having hospitalists involved with patients admitted without primary care physicians is “a tremendous help,” according to Dr. Burns, “because they really focus on our care measures. And each month, we have new residents come in, and the hospitalists train them on the project.”
As for McLeod Regional Medical Center, Dr. Hazelwood says, “Hospitalists are big admitters to the hospital—especially for those unassigned patients. And like other physicians, we are involved in various physician-led committees that develop our protocol for change.”
Are top-ranking hospitals sharing their bonus earnings with participating hospitalists and other physicians? “As far as I know, that has not happened, and it will not happen,” says Charles Riccobono, MD, chairman of the Performance Improvement Department at Hackensack. “I would hope that [bonus] money will filter down to support other quality projects, but I don’t know if the funds have been earmarked for anything specific.”
The Future Impact
The outcome of The Premier Hospital Quality Incentive Demonstration Project will shape any pay-for-performance guidelines that Medicare sets for hospitals around the country, including new or revised protocols and data collection hospital-wide. Final information will be available soon after the project ends this fall. Meanwhile, all data collected on the quality measures is available on the CMS Web site at www.cms.hhs.gov/HospitalQualityInits/35_HospitalPremier.asp. TH
A Return Visit to Mercy's Pay-For-Performance Program
Within a year of the implementation of a performance-based incentive program for its hospitalists, Mercy Hospital in Springfield, Mass., found itself leading the state in key composite compliance measures. Mercy was No. 2 on the list for two quarters in a row when MassPRO (the federally designated Quality Improvement Organization for Massachusetts) rated all 63 hospitals in the state on performance on quality indicators for heart failure, pneumonia, and MI.
Mercy Hospital ranked second in the state for both the fourth quarter of 2004 and the first quarter of 2005, whereas a different hospital ranked first for each quarter—and Massachusetts is the second-ranked state in the United States in these indicators.
How did Mercy rise so quickly to the top? Win Whitcomb, MD, who heads the hospitalist program at Mercy Hospital, credits the quality-based incentive program he helped initiate. “We had rapid improvement because we had a dedicated group of hospitalists and they were incentivized,” says Dr. Whitcomb.
Pay-for-Performance Program
A full 75% of the inpatients at Mercy Hospital are under the care of 10 hospitalists employed by the Mercy Inpatient Medicine Service (MIMS). As outlined in an article Dr. Whitcomb wrote for the July/August 2005 issue of The Hospitalist (“Physician Pay-for-Performance Comes to the Hospital”), MIMS implemented a unique incentive program for their hospitalists in January 2004.
The pay-for-performance, quality-based incentive program promised that each physician would receive a cash bonus every six months of more than 7.5% of his or her salary—but only if Mercy Medical Center reached the following targets for all hospital patients by the end of 2004:
- A 45% rate of pneumococcal vaccine screening and administration for all pneumonia patients;
- An 85% rate of documentation of ejection fraction for all heart failure patients; and
- Less than 40% rate of ejection fraction for heart failure patients and prescription of an ACE-inhibitor upon discharge (or documentation of a contraindication).
Dr. Whitcomb’s article shows how the MIMS group exceeded each of these quality improvement goals by the end of 2004. The MassPRO ranking shows how well they did in comparison with other hospitals in their state.
“The MassPRO recommendation for our performance is for the whole hospital—not just hospitalists,” says Dr. Whitcomb. “This is a good example of how hospitalists can carry the hospital. We also have traditional PCPs [primary care physicians] who are eager to measure up to our hospitalists; I feed back information to them, too.”
Update on the Incentive Program
MIMS is not resting on its laurels; they have continued to expand and update the incentive program. According to Bipinchandra Mistry, MD, MRCP, the current leader of the incentive program, 2005 has seen the addition of quality markers for reduction of decubitus ulcer rates, reduction of postoperative urinary tract infections, and discharge instructions for CHF. The annual bonus for physicians will be increased accordingly if these new markers are met.
“Of course, we must also maintain the previous quality markers at the same time,” explains Dr. Mistry.
Dr. Mistry attributes the success of the incentive program to its tie-in with a quality department. “The key is to have a person in your quality department involved to keep an eye on [markers in an incentive program] and see what barriers are coming up,” he says. “Otherwise, it’s harder for a group to forge ahead.”
Of the pay bonus that is tied to the markers, 30% relies on reaching the quality markers. “I think 30% to 40% is a reasonable target,” says Dr. Mistry.
Because these particular measures are difficult for the MIMS hospitalists to monitor alone, a quality improvement group headed by Dr. Whitcomb worked to include both a separate hospitalist group as well as PCPs. All were held accountable for quality through the addition of a “night-time coverage fee” that would be forgiven when the new quality goals were met.
Time will tell if the MIMS pay-for-performance program continues to pay off in increased quality of care for patients. TH
Contributing Writer Jane Jerrard is based in Chicago.
Within a year of the implementation of a performance-based incentive program for its hospitalists, Mercy Hospital in Springfield, Mass., found itself leading the state in key composite compliance measures. Mercy was No. 2 on the list for two quarters in a row when MassPRO (the federally designated Quality Improvement Organization for Massachusetts) rated all 63 hospitals in the state on performance on quality indicators for heart failure, pneumonia, and MI.
Mercy Hospital ranked second in the state for both the fourth quarter of 2004 and the first quarter of 2005, whereas a different hospital ranked first for each quarter—and Massachusetts is the second-ranked state in the United States in these indicators.
How did Mercy rise so quickly to the top? Win Whitcomb, MD, who heads the hospitalist program at Mercy Hospital, credits the quality-based incentive program he helped initiate. “We had rapid improvement because we had a dedicated group of hospitalists and they were incentivized,” says Dr. Whitcomb.
Pay-for-Performance Program
A full 75% of the inpatients at Mercy Hospital are under the care of 10 hospitalists employed by the Mercy Inpatient Medicine Service (MIMS). As outlined in an article Dr. Whitcomb wrote for the July/August 2005 issue of The Hospitalist (“Physician Pay-for-Performance Comes to the Hospital”), MIMS implemented a unique incentive program for their hospitalists in January 2004.
The pay-for-performance, quality-based incentive program promised that each physician would receive a cash bonus every six months of more than 7.5% of his or her salary—but only if Mercy Medical Center reached the following targets for all hospital patients by the end of 2004:
- A 45% rate of pneumococcal vaccine screening and administration for all pneumonia patients;
- An 85% rate of documentation of ejection fraction for all heart failure patients; and
- Less than 40% rate of ejection fraction for heart failure patients and prescription of an ACE-inhibitor upon discharge (or documentation of a contraindication).
Dr. Whitcomb’s article shows how the MIMS group exceeded each of these quality improvement goals by the end of 2004. The MassPRO ranking shows how well they did in comparison with other hospitals in their state.
“The MassPRO recommendation for our performance is for the whole hospital—not just hospitalists,” says Dr. Whitcomb. “This is a good example of how hospitalists can carry the hospital. We also have traditional PCPs [primary care physicians] who are eager to measure up to our hospitalists; I feed back information to them, too.”
Update on the Incentive Program
MIMS is not resting on its laurels; they have continued to expand and update the incentive program. According to Bipinchandra Mistry, MD, MRCP, the current leader of the incentive program, 2005 has seen the addition of quality markers for reduction of decubitus ulcer rates, reduction of postoperative urinary tract infections, and discharge instructions for CHF. The annual bonus for physicians will be increased accordingly if these new markers are met.
“Of course, we must also maintain the previous quality markers at the same time,” explains Dr. Mistry.
Dr. Mistry attributes the success of the incentive program to its tie-in with a quality department. “The key is to have a person in your quality department involved to keep an eye on [markers in an incentive program] and see what barriers are coming up,” he says. “Otherwise, it’s harder for a group to forge ahead.”
Of the pay bonus that is tied to the markers, 30% relies on reaching the quality markers. “I think 30% to 40% is a reasonable target,” says Dr. Mistry.
Because these particular measures are difficult for the MIMS hospitalists to monitor alone, a quality improvement group headed by Dr. Whitcomb worked to include both a separate hospitalist group as well as PCPs. All were held accountable for quality through the addition of a “night-time coverage fee” that would be forgiven when the new quality goals were met.
Time will tell if the MIMS pay-for-performance program continues to pay off in increased quality of care for patients. TH
Contributing Writer Jane Jerrard is based in Chicago.
Within a year of the implementation of a performance-based incentive program for its hospitalists, Mercy Hospital in Springfield, Mass., found itself leading the state in key composite compliance measures. Mercy was No. 2 on the list for two quarters in a row when MassPRO (the federally designated Quality Improvement Organization for Massachusetts) rated all 63 hospitals in the state on performance on quality indicators for heart failure, pneumonia, and MI.
Mercy Hospital ranked second in the state for both the fourth quarter of 2004 and the first quarter of 2005, whereas a different hospital ranked first for each quarter—and Massachusetts is the second-ranked state in the United States in these indicators.
How did Mercy rise so quickly to the top? Win Whitcomb, MD, who heads the hospitalist program at Mercy Hospital, credits the quality-based incentive program he helped initiate. “We had rapid improvement because we had a dedicated group of hospitalists and they were incentivized,” says Dr. Whitcomb.
Pay-for-Performance Program
A full 75% of the inpatients at Mercy Hospital are under the care of 10 hospitalists employed by the Mercy Inpatient Medicine Service (MIMS). As outlined in an article Dr. Whitcomb wrote for the July/August 2005 issue of The Hospitalist (“Physician Pay-for-Performance Comes to the Hospital”), MIMS implemented a unique incentive program for their hospitalists in January 2004.
The pay-for-performance, quality-based incentive program promised that each physician would receive a cash bonus every six months of more than 7.5% of his or her salary—but only if Mercy Medical Center reached the following targets for all hospital patients by the end of 2004:
- A 45% rate of pneumococcal vaccine screening and administration for all pneumonia patients;
- An 85% rate of documentation of ejection fraction for all heart failure patients; and
- Less than 40% rate of ejection fraction for heart failure patients and prescription of an ACE-inhibitor upon discharge (or documentation of a contraindication).
Dr. Whitcomb’s article shows how the MIMS group exceeded each of these quality improvement goals by the end of 2004. The MassPRO ranking shows how well they did in comparison with other hospitals in their state.
“The MassPRO recommendation for our performance is for the whole hospital—not just hospitalists,” says Dr. Whitcomb. “This is a good example of how hospitalists can carry the hospital. We also have traditional PCPs [primary care physicians] who are eager to measure up to our hospitalists; I feed back information to them, too.”
Update on the Incentive Program
MIMS is not resting on its laurels; they have continued to expand and update the incentive program. According to Bipinchandra Mistry, MD, MRCP, the current leader of the incentive program, 2005 has seen the addition of quality markers for reduction of decubitus ulcer rates, reduction of postoperative urinary tract infections, and discharge instructions for CHF. The annual bonus for physicians will be increased accordingly if these new markers are met.
“Of course, we must also maintain the previous quality markers at the same time,” explains Dr. Mistry.
Dr. Mistry attributes the success of the incentive program to its tie-in with a quality department. “The key is to have a person in your quality department involved to keep an eye on [markers in an incentive program] and see what barriers are coming up,” he says. “Otherwise, it’s harder for a group to forge ahead.”
Of the pay bonus that is tied to the markers, 30% relies on reaching the quality markers. “I think 30% to 40% is a reasonable target,” says Dr. Mistry.
Because these particular measures are difficult for the MIMS hospitalists to monitor alone, a quality improvement group headed by Dr. Whitcomb worked to include both a separate hospitalist group as well as PCPs. All were held accountable for quality through the addition of a “night-time coverage fee” that would be forgiven when the new quality goals were met.
Time will tell if the MIMS pay-for-performance program continues to pay off in increased quality of care for patients. TH
Contributing Writer Jane Jerrard is based in Chicago.
VTE Victory
What is your hospital doing to mark DVT Awareness Month this year? Consider that last year a Virginia hospital used this occasion to educate their staff on VTE, which encompasses both DVT and PE. This training was the first step in the implementation of a multidisciplinary, hospital-wide process that resulted in the vast majority of patients receiving proper preventive treatment of this common killer.
According to the Society of Critical Care Medicine, VTE is the No. 1 preventable cause of hospital-associated death for medical inpatients. Most hospitals are struggling to decrease the number of DVTs and PEs in their patient population by teaching or reminding staff to check for risk factors in each patient and, if necessary, provide VTE prophylaxis. While this seems like a simple solution, anyone who’s currently struggling to turn the numbers around this way can assure you that it is an uphill battle. The good news is that Carilion Medical Center in Roanoke, Va., may have found a key to winning that battle.
First Steps toward Improvement
Carilion Medical Center is 625-bed tertiary care facility that typically operates at peak census. With a level-one trauma center and a separate building housing the women’s and children’s hospital, Carilion offers every kind of care except burn treatment and full organ transplants.
“We recognized that VTE prophylaxis is a very important area and that we had not addressed it,” says James Franko, MD, FACP, medical director, General Medicine and Hospitalist Services.
Carilion’s first attempt to tackle the problem was not effective, but it laid the groundwork for later success.
“In April of 2004 we began working with a committee, conducting an investigation to see how frequently patients were receiving VTE prophylaxis,” recalls Dr. Franko. “We found that it was about 30%, based on patient population where more than 80% met the criteria for receiving this prophylaxis.”
The committee then broke down the data to examine who was ordering the VTE prophylaxis and found that there were three groups of physicians.
“There were those who almost always ordered the treatment, including our trauma surgeons,” says Dr. Franko. “Then there were those who did it sometimes and another group of those who never ordered it. We saw that this was obviously a good opportunity for education.”
Initial Research and Planning
In summer 2004, the group implemented a pilot program for screening every single patient on one floor of the hospital—a floor where physicians were predominantly hospitalists. The pilot involved including an information sheet on each medical chart with a list of VTE risk and exclusion criteria. The results: “We saw only a modest increase in prophylaxis,” says Dr. Franko.
So he pushed to find a better way to focus attention on VTE prophylaxis, this time using the channel that Carilion Medical Center has in place to address quality improvement issues.
“Someone can pitch an idea to our Quality Council and ask for a charter team,” explains Kris Peters, RN, human resources education consultant for Carilion Medical Center. “That team is given a time frame and asked to perform research and make recommendations. We have a charter team for pneumonia, for heart failure, for MCI, … that’s worked well for us.”
In fall 2004, Carilion’s Quality Council commissioned a new charter team and gave them the mission of increasing the percentage of patients receiving VTE prophylaxis. The team consisted of Dr. Franko and other physicians, nursing staff, a pharmacist, researchers, a staff member from the medical records department, secretaries, and—as a late addition—Peters.
“There was strong emotional buy-in from everyone on the team,” recalls Dr. Franko, “because almost everyone has a family member or friend who have had an experience with a blood clot.”
Dr. Franko and other members of the team proceeded to gather information on the rates of use and made projections for prophylaxis. They also reviewed the first attempt to increase use.
“We realized that it was necessary to make this a mandatory approach, or there would be no improvement whatsoever,” says Dr. Franko.
One possibility the team explored and then rejected was incorporating VTE prophylaxis with a patient’s admission. “When patients are admitted, we fill out a very thorough nursing assessment form,” explains Dr. Franko. “This is a good point to gather the information, but we decided it was just too cumbersome.”
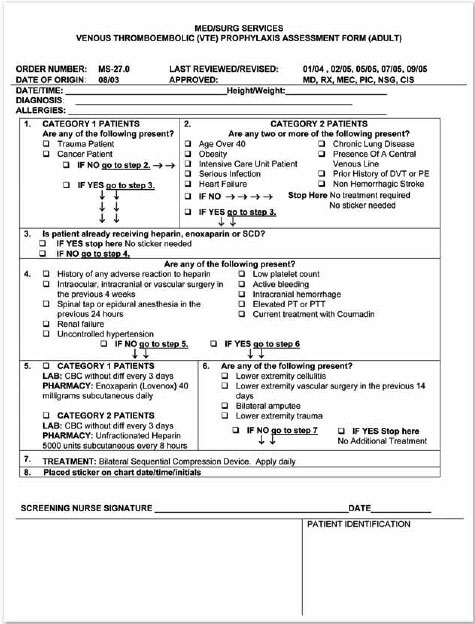
The team decided on the inclusion of a form with each patient’s medical chart that would lead the nursing staff through simple questions to determine whether the person should receive VTE prophylaxis. (See “VTE Prophylaxis Assessment Form [Adult],” at right.) The default is prophylaxis. “This was a bold step,” says Dr. Franko. With the form, “your patients are going to get VTE prophylaxis unless you tell us not to give it to them.”
Creating the VTE Prophylaxis Assessment Form
The multidisciplinary team needed to build the form using basic, easy-to-understand information. They began by breaking down the hospital’s patient population to determine who most needed the VTE prophylaxis. They found four groups:
- All trauma patients;
- All patients in ICU;
- Anyone with a diagnosis of cancer; and
- Anyone with a history of cancer. (See step 1 on the “VTE Prophylaxis Assessment Form,” at right.)
They also agreed that patients over age 40 with one other risk factor, such as smoking or drinking, would be considered at risk for DVT. (See step 2 on the “VTE Prophylaxis Assessment Form,” at right.)
“That is a significant percentage of our patients,” Dr. Franko points out. Because the women’s and children’s hospital is separate, a full 87% of Carilion’s patients are over 40.
The team then worked on exclusion factors that would eliminate patients in these groups from receiving prophylaxis. They agreed that patients with any of these exclusion criteria would automatically not receive prophylaxis. (See step 4 on the “VTE Prophylaxis Assessment Form,” at right.)
“We really struggled with how to administer the VTE prophylaxis,” admits Dr. Franko. “It was projected at one point that if we put all at-risk patients on low-molecular-weight heparins, we would increase our pharmacy’s budget by $3 million.”
With a great deal of reliance on the American College of Chest Physicians (ACCP) guidelines for VTE prophylaxis, the charter team decided on three treatment categories: low-molecular-weight heparins (enoxaparin, specifically), unfractionated heparins, and sequential compression devices (SCDs). (See step 5 on the “VTE Prophylaxis Assessment Form,” at right.)
“We use a lot of SCDs on our trauma patients,” says Dr. Franko, “but we still had to order more.” After talking to the hospital’s vascular surgeons and other staff, the charter team decided on patients to exclude from medications, including amputees and those who’d had recent vascular surgery. (See step 6 on the “VTE Prophylaxis Assessment Form,” at right.)
If the form indicates that prophylaxis is necessary, then the last step in completing the form is to have a physician add a bright pink sticker with his or her initials and the date and time.
“The pharmacy will prescribe with only that sticker on the chart,” says Dr. Franko. “Patients can get treatment earlier rather than later.”
Implementing the Form
The charter team still had to decide how the form would be presented to physicians and nursing staff. “We learned that there are no such things as standing orders,” says Dr. Franko. “But we can make the form a permanent part of each patient record, so that it cannot be discarded.”
The next hurdle was educating the staff, particularly nurses, on the new quality-improvement program. The team timed the implementation of the new process so that it began in March 2005, DVT Awareness Month. “We used the posters and giveaways provided by the Coalition to Prevent DVT to boost awareness in the staff,” says Peters. In April and May, the form went live.
“We used it for three months, then got information back from the nursing staff,” recalls Peters. “We went back to the committee with some suggested changes.” One of those changes was the inclusion of step 3: information on whether the patient was already receiving VTE prophylaxis.
The second wave of staff education began in late November, and the nursing staff continues to address the form in their bimonthly meetings. “Nurses fear the form, because they think it’s an order,” says Peters. “The top [of the form] will be done, but the bottom will be completely blank.”
She is working to educate nurses so that they are more comfortable with the form, and she has created an e-learning module with detailed information to supplement the form.
“This was a wonderful multidisciplinary effort,” says Dr. Franko. “I feel that the nursing service in particular has done a superb job. They get all the credit for this.”
Carolyn Webster, RN, vice president, Carilion Medical Center Nursing Operations, adds, “I’m happy that patients are being treated.”
First Findings: Dramatic Improvement
In May 2005, within two months after implementing the form, the charter team pulled 70 random patient charts to check their progress.
“We found that we had increased the percent of prophylaxis by SCD, low-molecular-weight heparins and unfractionated heparin [from 30%] to 60%,” says Dr. Franko. “And in June and July of 2005, we pulled 70 charts again. Eighty-seven percent of the patients had received prophylaxis. We were pleased with that increase.”
An Ongoing Process
When this period of education is over and any changes are made to the form and the process, the charter team will continue to meet once or twice a year to track progress and watch for problems.
“I’m not convinced that we’re going to sustain those numbers,” says Dr. Franko of the 87% success rate. “I hope we can keep the score up, but it’s going to take constant re-education.”
One positive factor was that the hospital’s staff is now well educated about VTE prophylaxis, so awareness continues to remain high.
The project will continue—and it will continue to be a work in progress. “We’re always relying on staff feedback to make [the form] more user-friendly,” says Dr. Franko. “And the prophylaxis may change over time, too.” TH
Contributing Writer Jane Jerrard is based in Chicago.
What is your hospital doing to mark DVT Awareness Month this year? Consider that last year a Virginia hospital used this occasion to educate their staff on VTE, which encompasses both DVT and PE. This training was the first step in the implementation of a multidisciplinary, hospital-wide process that resulted in the vast majority of patients receiving proper preventive treatment of this common killer.
According to the Society of Critical Care Medicine, VTE is the No. 1 preventable cause of hospital-associated death for medical inpatients. Most hospitals are struggling to decrease the number of DVTs and PEs in their patient population by teaching or reminding staff to check for risk factors in each patient and, if necessary, provide VTE prophylaxis. While this seems like a simple solution, anyone who’s currently struggling to turn the numbers around this way can assure you that it is an uphill battle. The good news is that Carilion Medical Center in Roanoke, Va., may have found a key to winning that battle.
First Steps toward Improvement
Carilion Medical Center is 625-bed tertiary care facility that typically operates at peak census. With a level-one trauma center and a separate building housing the women’s and children’s hospital, Carilion offers every kind of care except burn treatment and full organ transplants.
“We recognized that VTE prophylaxis is a very important area and that we had not addressed it,” says James Franko, MD, FACP, medical director, General Medicine and Hospitalist Services.
Carilion’s first attempt to tackle the problem was not effective, but it laid the groundwork for later success.
“In April of 2004 we began working with a committee, conducting an investigation to see how frequently patients were receiving VTE prophylaxis,” recalls Dr. Franko. “We found that it was about 30%, based on patient population where more than 80% met the criteria for receiving this prophylaxis.”
The committee then broke down the data to examine who was ordering the VTE prophylaxis and found that there were three groups of physicians.
“There were those who almost always ordered the treatment, including our trauma surgeons,” says Dr. Franko. “Then there were those who did it sometimes and another group of those who never ordered it. We saw that this was obviously a good opportunity for education.”
Initial Research and Planning
In summer 2004, the group implemented a pilot program for screening every single patient on one floor of the hospital—a floor where physicians were predominantly hospitalists. The pilot involved including an information sheet on each medical chart with a list of VTE risk and exclusion criteria. The results: “We saw only a modest increase in prophylaxis,” says Dr. Franko.
So he pushed to find a better way to focus attention on VTE prophylaxis, this time using the channel that Carilion Medical Center has in place to address quality improvement issues.
“Someone can pitch an idea to our Quality Council and ask for a charter team,” explains Kris Peters, RN, human resources education consultant for Carilion Medical Center. “That team is given a time frame and asked to perform research and make recommendations. We have a charter team for pneumonia, for heart failure, for MCI, … that’s worked well for us.”
In fall 2004, Carilion’s Quality Council commissioned a new charter team and gave them the mission of increasing the percentage of patients receiving VTE prophylaxis. The team consisted of Dr. Franko and other physicians, nursing staff, a pharmacist, researchers, a staff member from the medical records department, secretaries, and—as a late addition—Peters.
“There was strong emotional buy-in from everyone on the team,” recalls Dr. Franko, “because almost everyone has a family member or friend who have had an experience with a blood clot.”
Dr. Franko and other members of the team proceeded to gather information on the rates of use and made projections for prophylaxis. They also reviewed the first attempt to increase use.
“We realized that it was necessary to make this a mandatory approach, or there would be no improvement whatsoever,” says Dr. Franko.
One possibility the team explored and then rejected was incorporating VTE prophylaxis with a patient’s admission. “When patients are admitted, we fill out a very thorough nursing assessment form,” explains Dr. Franko. “This is a good point to gather the information, but we decided it was just too cumbersome.”
The team decided on the inclusion of a form with each patient’s medical chart that would lead the nursing staff through simple questions to determine whether the person should receive VTE prophylaxis. (See “VTE Prophylaxis Assessment Form [Adult],” at right.) The default is prophylaxis. “This was a bold step,” says Dr. Franko. With the form, “your patients are going to get VTE prophylaxis unless you tell us not to give it to them.”
Creating the VTE Prophylaxis Assessment Form
The multidisciplinary team needed to build the form using basic, easy-to-understand information. They began by breaking down the hospital’s patient population to determine who most needed the VTE prophylaxis. They found four groups:
- All trauma patients;
- All patients in ICU;
- Anyone with a diagnosis of cancer; and
- Anyone with a history of cancer. (See step 1 on the “VTE Prophylaxis Assessment Form,” at right.)
They also agreed that patients over age 40 with one other risk factor, such as smoking or drinking, would be considered at risk for DVT. (See step 2 on the “VTE Prophylaxis Assessment Form,” at right.)
“That is a significant percentage of our patients,” Dr. Franko points out. Because the women’s and children’s hospital is separate, a full 87% of Carilion’s patients are over 40.
The team then worked on exclusion factors that would eliminate patients in these groups from receiving prophylaxis. They agreed that patients with any of these exclusion criteria would automatically not receive prophylaxis. (See step 4 on the “VTE Prophylaxis Assessment Form,” at right.)
“We really struggled with how to administer the VTE prophylaxis,” admits Dr. Franko. “It was projected at one point that if we put all at-risk patients on low-molecular-weight heparins, we would increase our pharmacy’s budget by $3 million.”
With a great deal of reliance on the American College of Chest Physicians (ACCP) guidelines for VTE prophylaxis, the charter team decided on three treatment categories: low-molecular-weight heparins (enoxaparin, specifically), unfractionated heparins, and sequential compression devices (SCDs). (See step 5 on the “VTE Prophylaxis Assessment Form,” at right.)
“We use a lot of SCDs on our trauma patients,” says Dr. Franko, “but we still had to order more.” After talking to the hospital’s vascular surgeons and other staff, the charter team decided on patients to exclude from medications, including amputees and those who’d had recent vascular surgery. (See step 6 on the “VTE Prophylaxis Assessment Form,” at right.)
If the form indicates that prophylaxis is necessary, then the last step in completing the form is to have a physician add a bright pink sticker with his or her initials and the date and time.
“The pharmacy will prescribe with only that sticker on the chart,” says Dr. Franko. “Patients can get treatment earlier rather than later.”
Implementing the Form
The charter team still had to decide how the form would be presented to physicians and nursing staff. “We learned that there are no such things as standing orders,” says Dr. Franko. “But we can make the form a permanent part of each patient record, so that it cannot be discarded.”
The next hurdle was educating the staff, particularly nurses, on the new quality-improvement program. The team timed the implementation of the new process so that it began in March 2005, DVT Awareness Month. “We used the posters and giveaways provided by the Coalition to Prevent DVT to boost awareness in the staff,” says Peters. In April and May, the form went live.
“We used it for three months, then got information back from the nursing staff,” recalls Peters. “We went back to the committee with some suggested changes.” One of those changes was the inclusion of step 3: information on whether the patient was already receiving VTE prophylaxis.
The second wave of staff education began in late November, and the nursing staff continues to address the form in their bimonthly meetings. “Nurses fear the form, because they think it’s an order,” says Peters. “The top [of the form] will be done, but the bottom will be completely blank.”
She is working to educate nurses so that they are more comfortable with the form, and she has created an e-learning module with detailed information to supplement the form.
“This was a wonderful multidisciplinary effort,” says Dr. Franko. “I feel that the nursing service in particular has done a superb job. They get all the credit for this.”
Carolyn Webster, RN, vice president, Carilion Medical Center Nursing Operations, adds, “I’m happy that patients are being treated.”
First Findings: Dramatic Improvement
In May 2005, within two months after implementing the form, the charter team pulled 70 random patient charts to check their progress.
“We found that we had increased the percent of prophylaxis by SCD, low-molecular-weight heparins and unfractionated heparin [from 30%] to 60%,” says Dr. Franko. “And in June and July of 2005, we pulled 70 charts again. Eighty-seven percent of the patients had received prophylaxis. We were pleased with that increase.”
An Ongoing Process
When this period of education is over and any changes are made to the form and the process, the charter team will continue to meet once or twice a year to track progress and watch for problems.
“I’m not convinced that we’re going to sustain those numbers,” says Dr. Franko of the 87% success rate. “I hope we can keep the score up, but it’s going to take constant re-education.”
One positive factor was that the hospital’s staff is now well educated about VTE prophylaxis, so awareness continues to remain high.
The project will continue—and it will continue to be a work in progress. “We’re always relying on staff feedback to make [the form] more user-friendly,” says Dr. Franko. “And the prophylaxis may change over time, too.” TH
Contributing Writer Jane Jerrard is based in Chicago.
What is your hospital doing to mark DVT Awareness Month this year? Consider that last year a Virginia hospital used this occasion to educate their staff on VTE, which encompasses both DVT and PE. This training was the first step in the implementation of a multidisciplinary, hospital-wide process that resulted in the vast majority of patients receiving proper preventive treatment of this common killer.
According to the Society of Critical Care Medicine, VTE is the No. 1 preventable cause of hospital-associated death for medical inpatients. Most hospitals are struggling to decrease the number of DVTs and PEs in their patient population by teaching or reminding staff to check for risk factors in each patient and, if necessary, provide VTE prophylaxis. While this seems like a simple solution, anyone who’s currently struggling to turn the numbers around this way can assure you that it is an uphill battle. The good news is that Carilion Medical Center in Roanoke, Va., may have found a key to winning that battle.
First Steps toward Improvement
Carilion Medical Center is 625-bed tertiary care facility that typically operates at peak census. With a level-one trauma center and a separate building housing the women’s and children’s hospital, Carilion offers every kind of care except burn treatment and full organ transplants.
“We recognized that VTE prophylaxis is a very important area and that we had not addressed it,” says James Franko, MD, FACP, medical director, General Medicine and Hospitalist Services.
Carilion’s first attempt to tackle the problem was not effective, but it laid the groundwork for later success.
“In April of 2004 we began working with a committee, conducting an investigation to see how frequently patients were receiving VTE prophylaxis,” recalls Dr. Franko. “We found that it was about 30%, based on patient population where more than 80% met the criteria for receiving this prophylaxis.”
The committee then broke down the data to examine who was ordering the VTE prophylaxis and found that there were three groups of physicians.
“There were those who almost always ordered the treatment, including our trauma surgeons,” says Dr. Franko. “Then there were those who did it sometimes and another group of those who never ordered it. We saw that this was obviously a good opportunity for education.”
Initial Research and Planning
In summer 2004, the group implemented a pilot program for screening every single patient on one floor of the hospital—a floor where physicians were predominantly hospitalists. The pilot involved including an information sheet on each medical chart with a list of VTE risk and exclusion criteria. The results: “We saw only a modest increase in prophylaxis,” says Dr. Franko.
So he pushed to find a better way to focus attention on VTE prophylaxis, this time using the channel that Carilion Medical Center has in place to address quality improvement issues.
“Someone can pitch an idea to our Quality Council and ask for a charter team,” explains Kris Peters, RN, human resources education consultant for Carilion Medical Center. “That team is given a time frame and asked to perform research and make recommendations. We have a charter team for pneumonia, for heart failure, for MCI, … that’s worked well for us.”
In fall 2004, Carilion’s Quality Council commissioned a new charter team and gave them the mission of increasing the percentage of patients receiving VTE prophylaxis. The team consisted of Dr. Franko and other physicians, nursing staff, a pharmacist, researchers, a staff member from the medical records department, secretaries, and—as a late addition—Peters.
“There was strong emotional buy-in from everyone on the team,” recalls Dr. Franko, “because almost everyone has a family member or friend who have had an experience with a blood clot.”
Dr. Franko and other members of the team proceeded to gather information on the rates of use and made projections for prophylaxis. They also reviewed the first attempt to increase use.
“We realized that it was necessary to make this a mandatory approach, or there would be no improvement whatsoever,” says Dr. Franko.
One possibility the team explored and then rejected was incorporating VTE prophylaxis with a patient’s admission. “When patients are admitted, we fill out a very thorough nursing assessment form,” explains Dr. Franko. “This is a good point to gather the information, but we decided it was just too cumbersome.”
The team decided on the inclusion of a form with each patient’s medical chart that would lead the nursing staff through simple questions to determine whether the person should receive VTE prophylaxis. (See “VTE Prophylaxis Assessment Form [Adult],” at right.) The default is prophylaxis. “This was a bold step,” says Dr. Franko. With the form, “your patients are going to get VTE prophylaxis unless you tell us not to give it to them.”
Creating the VTE Prophylaxis Assessment Form
The multidisciplinary team needed to build the form using basic, easy-to-understand information. They began by breaking down the hospital’s patient population to determine who most needed the VTE prophylaxis. They found four groups:
- All trauma patients;
- All patients in ICU;
- Anyone with a diagnosis of cancer; and
- Anyone with a history of cancer. (See step 1 on the “VTE Prophylaxis Assessment Form,” at right.)
They also agreed that patients over age 40 with one other risk factor, such as smoking or drinking, would be considered at risk for DVT. (See step 2 on the “VTE Prophylaxis Assessment Form,” at right.)
“That is a significant percentage of our patients,” Dr. Franko points out. Because the women’s and children’s hospital is separate, a full 87% of Carilion’s patients are over 40.
The team then worked on exclusion factors that would eliminate patients in these groups from receiving prophylaxis. They agreed that patients with any of these exclusion criteria would automatically not receive prophylaxis. (See step 4 on the “VTE Prophylaxis Assessment Form,” at right.)
“We really struggled with how to administer the VTE prophylaxis,” admits Dr. Franko. “It was projected at one point that if we put all at-risk patients on low-molecular-weight heparins, we would increase our pharmacy’s budget by $3 million.”
With a great deal of reliance on the American College of Chest Physicians (ACCP) guidelines for VTE prophylaxis, the charter team decided on three treatment categories: low-molecular-weight heparins (enoxaparin, specifically), unfractionated heparins, and sequential compression devices (SCDs). (See step 5 on the “VTE Prophylaxis Assessment Form,” at right.)
“We use a lot of SCDs on our trauma patients,” says Dr. Franko, “but we still had to order more.” After talking to the hospital’s vascular surgeons and other staff, the charter team decided on patients to exclude from medications, including amputees and those who’d had recent vascular surgery. (See step 6 on the “VTE Prophylaxis Assessment Form,” at right.)
If the form indicates that prophylaxis is necessary, then the last step in completing the form is to have a physician add a bright pink sticker with his or her initials and the date and time.
“The pharmacy will prescribe with only that sticker on the chart,” says Dr. Franko. “Patients can get treatment earlier rather than later.”
Implementing the Form
The charter team still had to decide how the form would be presented to physicians and nursing staff. “We learned that there are no such things as standing orders,” says Dr. Franko. “But we can make the form a permanent part of each patient record, so that it cannot be discarded.”
The next hurdle was educating the staff, particularly nurses, on the new quality-improvement program. The team timed the implementation of the new process so that it began in March 2005, DVT Awareness Month. “We used the posters and giveaways provided by the Coalition to Prevent DVT to boost awareness in the staff,” says Peters. In April and May, the form went live.
“We used it for three months, then got information back from the nursing staff,” recalls Peters. “We went back to the committee with some suggested changes.” One of those changes was the inclusion of step 3: information on whether the patient was already receiving VTE prophylaxis.
The second wave of staff education began in late November, and the nursing staff continues to address the form in their bimonthly meetings. “Nurses fear the form, because they think it’s an order,” says Peters. “The top [of the form] will be done, but the bottom will be completely blank.”
She is working to educate nurses so that they are more comfortable with the form, and she has created an e-learning module with detailed information to supplement the form.
“This was a wonderful multidisciplinary effort,” says Dr. Franko. “I feel that the nursing service in particular has done a superb job. They get all the credit for this.”
Carolyn Webster, RN, vice president, Carilion Medical Center Nursing Operations, adds, “I’m happy that patients are being treated.”
First Findings: Dramatic Improvement
In May 2005, within two months after implementing the form, the charter team pulled 70 random patient charts to check their progress.
“We found that we had increased the percent of prophylaxis by SCD, low-molecular-weight heparins and unfractionated heparin [from 30%] to 60%,” says Dr. Franko. “And in June and July of 2005, we pulled 70 charts again. Eighty-seven percent of the patients had received prophylaxis. We were pleased with that increase.”
An Ongoing Process
When this period of education is over and any changes are made to the form and the process, the charter team will continue to meet once or twice a year to track progress and watch for problems.
“I’m not convinced that we’re going to sustain those numbers,” says Dr. Franko of the 87% success rate. “I hope we can keep the score up, but it’s going to take constant re-education.”
One positive factor was that the hospital’s staff is now well educated about VTE prophylaxis, so awareness continues to remain high.
The project will continue—and it will continue to be a work in progress. “We’re always relying on staff feedback to make [the form] more user-friendly,” says Dr. Franko. “And the prophylaxis may change over time, too.” TH
Contributing Writer Jane Jerrard is based in Chicago.
The End of General Hospitals
Where will you be in 20 years? If you’re a young hospitalist, you may work in an enormous state-of-the-art hospital complex that includes the latest technologies, the best in amenities, and a well-thought-out design that will meet your needs and those of other staff for years to come.
“There are a lot of different approaches” to designing the hospital facility of the future, says George R. Tingwald, MD, AIA, ACHA, director of healthcare design at Skidmore, Owings, and Merrill in San Francisco. “The difference depends on whether you look at it from a constructability standpoint versus a much more consumer-based focus. Though many think they have the right approach, it’s hard to say that everybody’s decided on a single solution.”
The Future Looks … Big
It’s not just the hospital facility itself that will change in the future. The number of hospitals in each community may change as well—and the hospitals will be considerably larger.
“We will probably see fewer but larger hospitals in the future,” predicts Dr. Tingwald. “We’re in an era where we’re seeing significant growth in the number of inpatients served. Because of the baby boom and increasing longevity in Americans we’re already seeing an increase, and it’s going to continue. We’ll definitely see more hospital beds in the future.”
The type of patients who fill those hospital beds will change as well.
“We’ll continue to see sicker and sicker patients in those hospital beds,” says Dr. Tingwald. “More people will be managed on an outpatient basis as more diagnostic and treatment procedures will be done as outpatients. Look at breast cancer: From initial detection to diagnosis to biopsy to lumpectomy to chemotherapy or radiation treatment, to cure, or end-of-life care, each step can now be done on an outpatient basis.”
What does this mean? “Someone can have a very significant, multiepisodic disease and never stay in the hospital—unless there are complications,” explains Dr. Tingwald. “Therefore, we’ll have only very acute patients in the hospital. The hospital will basically become an intensive care unit.”
In the past, approximately 10% of a hospital’s beds were in the ICU. That percentage is rising—an indication of things to come. That percentage is now around 20% or 30% and growing, especially in major centers. Only seriously ill people will be admitted—but even they won’t spend a lot of time in the hospital. They will die, recover to a point where they can be moved to rehabilitation or other support facility, or be sent home.
What about the prediction that there will be fewer hospitals in the future? Dr. Tingwald predicts that technology and expertise will weed out some facilities.
“We used to have a lot of what I would call general hospitals—meaning every one was the same,” he explains. “That’s changing radically. The institutions with the expertise and wherewithal to develop technical sophistication, such as university hospitals and specialty hospitals, are doing well. Those that don’t have that sophistication can’t keep up. The big centers are growing because they have the equipment and the expertise. The smaller ones are failing.”
This trend may come as a surprise to some in healthcare, in light of previous predictions. “This is different than the futurists were saying 10 or 20 years ago, when predictions were for more home-based and community-based care,” says Dr. Tingwald. “The reverse has happened. The latest equipment is not available to everyone, let alone smaller, unaffiliated hospitals. And the people that can work with that technology are few and far between.”
The addition of new technology will have some effect on the size of the hospital. “You need a lot of physical space for wiring,” admits Dr. Tingwald. “But the ‘brains’ of the technology can be offsite at a separate IT center or data center.”
Focus on Family-Centered Care
Perhaps the most noticeable differences in the hospital facility of the future will be those related to a change in services, design, and attitude toward providing amenities for patients and their families.
“Patient-centered care, or its close cousin—family-centered care—is a significant trend in healthcare design now, and that significantly impacts the design of facilities,” states Dr. Tingwald. “The most important aspect is having all private rooms. Almost no new construction includes shared patient rooms. The key element of this care is family involvement, and that includes families rooming in with patients. You can’t physically or psychologically do this in a shared room.”
He points out that this trend includes all room types: “It started in pediatrics, but has gone into general acute care settings, intensive care settings, and now neonatal intensive care units.”
What are the pros and cons of a move toward all private rooms? “It takes up room, but it’s proving not to be significantly more costly,” says Dr. Tingwald. “Private rooms are more expensive to build, but in the end they’re less expensive to operate. In an all-private room hospital you can increase your occupancy to 80% or even 90% because you’re not trying to match up patients by gender and age. Also, nursing isn’t moving patients to get the bed mixes right. Studies show that nurses spend up to 40% of their time in transfers. And finally, private rooms have increased market share considerably.”
Another aspect of family centered care is the addition of technologies and services that cater to patient comfort and even enjoyment. “Anything someone has at home or wants in a hotel, families and patients are demanding, including room service,” says Dr. Tingwald. “Patients can decide when and what they want to eat [within their prescribed diet], and families can order food. In some hospitals, patients can already order food using a plasma screen in their room. This is showing to be an economically viable alternative. There’s less food waste, and patients are much happier.”
You’ll also see patient rooms with plasma screen televisions and DVD players, equipped for movies on demand, educational content—even the ability for physicians to view X-rays and other diagnostics on screen, and for families waiting in the room to communicate with physicians in the operating room.
“These are consumer-driven things, but they’re not luxuries,” insists Dr. Tingwald. “They’re often things that save time, increase the ability for education, and significantly decrease errors.”
Another argument for adding amenities like plasma screen TVs and room service: “In healthcare you think adding this technology must be too expensive,” says Dr. Tingwald, “but if you walk into a fast-food place, the person behind the counter uses a touch screen. Everybody else has done this already. Facilities that don’t partake in these transitions are not going to survive.”
Other family-centered improvements include major changes in patient registration. “Most registration can be done from home, over the Internet,” he says. “At Northwestern Memorial Hospital [in Chicago], patients have an encoded card they swipe when they drive into the parking garage, and the receptionist knows they’re coming and gets their room ready before they arrive.”
In the future, more facilities will offer options like these to make the registration process easy and fast.
The hospital of the future will feature a friendlier environment, with landscaping and nice views from patient rooms, artwork and amenities that are important in the healing process. They will also include an emphasis on alternative treatments, says Dr. Tingwald, “from massage to aromatherapy to spaces for yoga or meditation.”
Plan for Flexibility
The key to the design of the hospital of the future will be its ability to change without building additions, remodeling, or rehabbing.
“We’re no longer planning a facility in a static way, thinking that things will not change. Flexibility and adaptability are planned from the beginning,” explains Dr. Tingwald. “You’ll see a lot more generic room types—rooms that are all a single size, but adaptable. A private patient room might be initially planned for acute care, but it can be adapted for an ICU room with minimal or no remodeling.”
This holds true for other room types as well. “In diagnostic and treatment spaces, we plan for one, or no more than two, sizes of space,” he says. “You don’t know if in the future more procedures will be surgical or non-invasive, so rooms are planned to handle both functions. Also, the kingdoms are coming down and divisions between diagnostic departments are blending.”
The Johns Hopkins Hospital (Baltimore), the University of California, Los Angeles Medical Center, and California Pacific Medical Center in San Francisco are all designing “platform floors,” where surgery, interventional imaging, cardiac catheterization, and other procedure-based services share preoperative and postoperative areas and have single access.
“These floors provide adjacency of services allowing a lot more flexibility and decreased redundancy,” explains Dr. Tingwald. “Also, there aren’t as many patient transfers, and a key to patient-centered care is less movement of the patient.”
Built-in flexibility is designed to accommodate scalability as well. “In the planning process, we anticipate higher volumes in an emergency or disaster,” he says. “We plan how to expand the emergency room, and we make rooms larger than we used to. That way, if volumes increase quickly, you could put two, three, maybe more patients in a space. Nurses hate when you say that, but we have to have timely solutions that are affordable. This approach can be considered on nursing units as well, with these ‘super singles’ able to handle a second patient during a February flu outbreak, for example. That’s better than having an entire wing of the hospital that’s only used during winter months, patients stuck in the emergency department for days, or patients in the halls.”
A Design with Built-In Patient Safety
The physical design of the hospital of the future will better address and correct issues with patient safety. “Whatever design elements can minimize errors and improve outcomes are being studied intensively right now,” says Dr. Tingwald. “For example, we used to mirror many room types so that walls could share plumbing, etc. One room would be the mirror image of the one next to it, requiring the staff to learn different layouts, which increases time of response and possible errors. Now, we try to make procedure rooms as similar as possible to reduce the potential for error.”
There are design elements that limit the possibility of hospital-borne infection, including ultraviolet light and biologic surfaces. There is also a greater emphasis on including track systems for lifts for getting patients out of bed and moving them without injury to the patient or the staff.
Consider Hospitalists and Other Staff
How will the hospital of the future accommodate hospitalists?
“We’re certainly seeing more hospitalists,” says Dr. Tingwald. “As you have sicker patients in the hospital, it’s harder for their primary care physicians to manage them, so we’re going to see even more hospitalists. This means that we have to provide space for them; both offices, because they don’t have other office space, and sleeping accommodations, which means private rooms with bath, as well as lounge space.”
Hospitals will provide appealing space for physicians because it will help them recruit hospitalists. Improving lounges and other staff spaces will be a goal of future hospital designs.
“There will be a lot more emphasis on good environments for work and for support services,” predicts Dr. Tingwald. “This will increase the attraction and retention of top staff. You’ll see things like fitness centers, and basic additions like enough parking spaces.”
As hospital facilities move toward more patient-centered care, with flexible layouts and space designed for patient safety, the working environment is certain to become more conducive to providing good care and working efficiently. It will also become more comfortable, convenient, and pleasant for hospitalists and other staff. And that is something to look forward to. TH
Writer Jane Jerrard wrote the first three installments of the “Future” series.
FLASHBACK
Cadaver Particles
—Ignaz Semmelweis, 1861
Death stalked the halls of the First Division of the Allegemeine Krankenhaus (Vienna General Hospital), a large teaching hospital in Austria. Healthy post-partum women suddenly become febrile and died from puerperal sepsis (childbed fever). In the mid-19th century, this problem was seen in hospitals across Europe, though rarely in home deliveries. It was a seemingly insoluble dilemma. Opinions varied on the etiology. Was it miasmas, the paint on the walls, were the beds too close, or was it clogged milk glands? Complacency and acceptance of status quo were, to some, the easiest solution.
In the mid-1800s Hungarian Physician Ignaz Semmelweis was given an appointment as an assistant in obstetrics at the Allegemeine Krankenhaus. He had adopted the Austrian paradigm of clinical and pathologic anatomy. The answer to any question lay in the autopsy. It seemed like the more autopsies they did, the more women died. The death of Semmelweis’ colleague, Jakob Kolletschka (who was initially injured when his knife slipped during an autopsy of a woman who died of puerperal fever and then died himself of symptoms similar to those that killed the woman) gave Semmelweis the vital clue.
He realized that something carried on unwashed surgeons’ hands from infected cadavers caused the disease to occur in the women. These “cadaver particles” were transmitted from the morning autopsies to the women on the wards by the unwashed hands of students and faculty. Adopting proper hygiene could save thousands of lives. Properly washed hands were the simple answer. This also explained the mystery of why the puerperal fever rate was lower on the midwife-run wards where they did not do autopsies.
Decades before Pasteur and Lister, accepting that their own hands brought death was a bitter pill for the great men of obstetrics to swallow. Unfortunately for Semmelweis and the women who continued to die, it was years before Oliver Wendell Holmes incontrovertibly published his essay, “The Contagiousness of Puerperal Fever” in 1843 in the New England Quarterly Journal of Medicine. That essay showed the source of puerperal fever. Despite his clinical success Semmelweis was unable to persuade his fellow physicians.
The nosocomial spread of infection on unwashed hands rings true to this day. We spend our days gloved, gowned, and masked in the battle against MRSA, VRE, and other pathogens. Whether soap or alcohol, when we scrub our hands we should remember that it is more than a ritual. It’s a duty to prevent the spread of disease.
—Jamie Newman, MD, FACP
Where will you be in 20 years? If you’re a young hospitalist, you may work in an enormous state-of-the-art hospital complex that includes the latest technologies, the best in amenities, and a well-thought-out design that will meet your needs and those of other staff for years to come.
“There are a lot of different approaches” to designing the hospital facility of the future, says George R. Tingwald, MD, AIA, ACHA, director of healthcare design at Skidmore, Owings, and Merrill in San Francisco. “The difference depends on whether you look at it from a constructability standpoint versus a much more consumer-based focus. Though many think they have the right approach, it’s hard to say that everybody’s decided on a single solution.”
The Future Looks … Big
It’s not just the hospital facility itself that will change in the future. The number of hospitals in each community may change as well—and the hospitals will be considerably larger.
“We will probably see fewer but larger hospitals in the future,” predicts Dr. Tingwald. “We’re in an era where we’re seeing significant growth in the number of inpatients served. Because of the baby boom and increasing longevity in Americans we’re already seeing an increase, and it’s going to continue. We’ll definitely see more hospital beds in the future.”
The type of patients who fill those hospital beds will change as well.
“We’ll continue to see sicker and sicker patients in those hospital beds,” says Dr. Tingwald. “More people will be managed on an outpatient basis as more diagnostic and treatment procedures will be done as outpatients. Look at breast cancer: From initial detection to diagnosis to biopsy to lumpectomy to chemotherapy or radiation treatment, to cure, or end-of-life care, each step can now be done on an outpatient basis.”
What does this mean? “Someone can have a very significant, multiepisodic disease and never stay in the hospital—unless there are complications,” explains Dr. Tingwald. “Therefore, we’ll have only very acute patients in the hospital. The hospital will basically become an intensive care unit.”
In the past, approximately 10% of a hospital’s beds were in the ICU. That percentage is rising—an indication of things to come. That percentage is now around 20% or 30% and growing, especially in major centers. Only seriously ill people will be admitted—but even they won’t spend a lot of time in the hospital. They will die, recover to a point where they can be moved to rehabilitation or other support facility, or be sent home.
What about the prediction that there will be fewer hospitals in the future? Dr. Tingwald predicts that technology and expertise will weed out some facilities.
“We used to have a lot of what I would call general hospitals—meaning every one was the same,” he explains. “That’s changing radically. The institutions with the expertise and wherewithal to develop technical sophistication, such as university hospitals and specialty hospitals, are doing well. Those that don’t have that sophistication can’t keep up. The big centers are growing because they have the equipment and the expertise. The smaller ones are failing.”
This trend may come as a surprise to some in healthcare, in light of previous predictions. “This is different than the futurists were saying 10 or 20 years ago, when predictions were for more home-based and community-based care,” says Dr. Tingwald. “The reverse has happened. The latest equipment is not available to everyone, let alone smaller, unaffiliated hospitals. And the people that can work with that technology are few and far between.”
The addition of new technology will have some effect on the size of the hospital. “You need a lot of physical space for wiring,” admits Dr. Tingwald. “But the ‘brains’ of the technology can be offsite at a separate IT center or data center.”
Focus on Family-Centered Care
Perhaps the most noticeable differences in the hospital facility of the future will be those related to a change in services, design, and attitude toward providing amenities for patients and their families.
“Patient-centered care, or its close cousin—family-centered care—is a significant trend in healthcare design now, and that significantly impacts the design of facilities,” states Dr. Tingwald. “The most important aspect is having all private rooms. Almost no new construction includes shared patient rooms. The key element of this care is family involvement, and that includes families rooming in with patients. You can’t physically or psychologically do this in a shared room.”
He points out that this trend includes all room types: “It started in pediatrics, but has gone into general acute care settings, intensive care settings, and now neonatal intensive care units.”
What are the pros and cons of a move toward all private rooms? “It takes up room, but it’s proving not to be significantly more costly,” says Dr. Tingwald. “Private rooms are more expensive to build, but in the end they’re less expensive to operate. In an all-private room hospital you can increase your occupancy to 80% or even 90% because you’re not trying to match up patients by gender and age. Also, nursing isn’t moving patients to get the bed mixes right. Studies show that nurses spend up to 40% of their time in transfers. And finally, private rooms have increased market share considerably.”
Another aspect of family centered care is the addition of technologies and services that cater to patient comfort and even enjoyment. “Anything someone has at home or wants in a hotel, families and patients are demanding, including room service,” says Dr. Tingwald. “Patients can decide when and what they want to eat [within their prescribed diet], and families can order food. In some hospitals, patients can already order food using a plasma screen in their room. This is showing to be an economically viable alternative. There’s less food waste, and patients are much happier.”
You’ll also see patient rooms with plasma screen televisions and DVD players, equipped for movies on demand, educational content—even the ability for physicians to view X-rays and other diagnostics on screen, and for families waiting in the room to communicate with physicians in the operating room.
“These are consumer-driven things, but they’re not luxuries,” insists Dr. Tingwald. “They’re often things that save time, increase the ability for education, and significantly decrease errors.”
Another argument for adding amenities like plasma screen TVs and room service: “In healthcare you think adding this technology must be too expensive,” says Dr. Tingwald, “but if you walk into a fast-food place, the person behind the counter uses a touch screen. Everybody else has done this already. Facilities that don’t partake in these transitions are not going to survive.”
Other family-centered improvements include major changes in patient registration. “Most registration can be done from home, over the Internet,” he says. “At Northwestern Memorial Hospital [in Chicago], patients have an encoded card they swipe when they drive into the parking garage, and the receptionist knows they’re coming and gets their room ready before they arrive.”
In the future, more facilities will offer options like these to make the registration process easy and fast.
The hospital of the future will feature a friendlier environment, with landscaping and nice views from patient rooms, artwork and amenities that are important in the healing process. They will also include an emphasis on alternative treatments, says Dr. Tingwald, “from massage to aromatherapy to spaces for yoga or meditation.”
Plan for Flexibility
The key to the design of the hospital of the future will be its ability to change without building additions, remodeling, or rehabbing.
“We’re no longer planning a facility in a static way, thinking that things will not change. Flexibility and adaptability are planned from the beginning,” explains Dr. Tingwald. “You’ll see a lot more generic room types—rooms that are all a single size, but adaptable. A private patient room might be initially planned for acute care, but it can be adapted for an ICU room with minimal or no remodeling.”
This holds true for other room types as well. “In diagnostic and treatment spaces, we plan for one, or no more than two, sizes of space,” he says. “You don’t know if in the future more procedures will be surgical or non-invasive, so rooms are planned to handle both functions. Also, the kingdoms are coming down and divisions between diagnostic departments are blending.”
The Johns Hopkins Hospital (Baltimore), the University of California, Los Angeles Medical Center, and California Pacific Medical Center in San Francisco are all designing “platform floors,” where surgery, interventional imaging, cardiac catheterization, and other procedure-based services share preoperative and postoperative areas and have single access.
“These floors provide adjacency of services allowing a lot more flexibility and decreased redundancy,” explains Dr. Tingwald. “Also, there aren’t as many patient transfers, and a key to patient-centered care is less movement of the patient.”
Built-in flexibility is designed to accommodate scalability as well. “In the planning process, we anticipate higher volumes in an emergency or disaster,” he says. “We plan how to expand the emergency room, and we make rooms larger than we used to. That way, if volumes increase quickly, you could put two, three, maybe more patients in a space. Nurses hate when you say that, but we have to have timely solutions that are affordable. This approach can be considered on nursing units as well, with these ‘super singles’ able to handle a second patient during a February flu outbreak, for example. That’s better than having an entire wing of the hospital that’s only used during winter months, patients stuck in the emergency department for days, or patients in the halls.”
A Design with Built-In Patient Safety
The physical design of the hospital of the future will better address and correct issues with patient safety. “Whatever design elements can minimize errors and improve outcomes are being studied intensively right now,” says Dr. Tingwald. “For example, we used to mirror many room types so that walls could share plumbing, etc. One room would be the mirror image of the one next to it, requiring the staff to learn different layouts, which increases time of response and possible errors. Now, we try to make procedure rooms as similar as possible to reduce the potential for error.”
There are design elements that limit the possibility of hospital-borne infection, including ultraviolet light and biologic surfaces. There is also a greater emphasis on including track systems for lifts for getting patients out of bed and moving them without injury to the patient or the staff.
Consider Hospitalists and Other Staff
How will the hospital of the future accommodate hospitalists?
“We’re certainly seeing more hospitalists,” says Dr. Tingwald. “As you have sicker patients in the hospital, it’s harder for their primary care physicians to manage them, so we’re going to see even more hospitalists. This means that we have to provide space for them; both offices, because they don’t have other office space, and sleeping accommodations, which means private rooms with bath, as well as lounge space.”
Hospitals will provide appealing space for physicians because it will help them recruit hospitalists. Improving lounges and other staff spaces will be a goal of future hospital designs.
“There will be a lot more emphasis on good environments for work and for support services,” predicts Dr. Tingwald. “This will increase the attraction and retention of top staff. You’ll see things like fitness centers, and basic additions like enough parking spaces.”
As hospital facilities move toward more patient-centered care, with flexible layouts and space designed for patient safety, the working environment is certain to become more conducive to providing good care and working efficiently. It will also become more comfortable, convenient, and pleasant for hospitalists and other staff. And that is something to look forward to. TH
Writer Jane Jerrard wrote the first three installments of the “Future” series.
FLASHBACK
Cadaver Particles
—Ignaz Semmelweis, 1861
Death stalked the halls of the First Division of the Allegemeine Krankenhaus (Vienna General Hospital), a large teaching hospital in Austria. Healthy post-partum women suddenly become febrile and died from puerperal sepsis (childbed fever). In the mid-19th century, this problem was seen in hospitals across Europe, though rarely in home deliveries. It was a seemingly insoluble dilemma. Opinions varied on the etiology. Was it miasmas, the paint on the walls, were the beds too close, or was it clogged milk glands? Complacency and acceptance of status quo were, to some, the easiest solution.
In the mid-1800s Hungarian Physician Ignaz Semmelweis was given an appointment as an assistant in obstetrics at the Allegemeine Krankenhaus. He had adopted the Austrian paradigm of clinical and pathologic anatomy. The answer to any question lay in the autopsy. It seemed like the more autopsies they did, the more women died. The death of Semmelweis’ colleague, Jakob Kolletschka (who was initially injured when his knife slipped during an autopsy of a woman who died of puerperal fever and then died himself of symptoms similar to those that killed the woman) gave Semmelweis the vital clue.
He realized that something carried on unwashed surgeons’ hands from infected cadavers caused the disease to occur in the women. These “cadaver particles” were transmitted from the morning autopsies to the women on the wards by the unwashed hands of students and faculty. Adopting proper hygiene could save thousands of lives. Properly washed hands were the simple answer. This also explained the mystery of why the puerperal fever rate was lower on the midwife-run wards where they did not do autopsies.
Decades before Pasteur and Lister, accepting that their own hands brought death was a bitter pill for the great men of obstetrics to swallow. Unfortunately for Semmelweis and the women who continued to die, it was years before Oliver Wendell Holmes incontrovertibly published his essay, “The Contagiousness of Puerperal Fever” in 1843 in the New England Quarterly Journal of Medicine. That essay showed the source of puerperal fever. Despite his clinical success Semmelweis was unable to persuade his fellow physicians.
The nosocomial spread of infection on unwashed hands rings true to this day. We spend our days gloved, gowned, and masked in the battle against MRSA, VRE, and other pathogens. Whether soap or alcohol, when we scrub our hands we should remember that it is more than a ritual. It’s a duty to prevent the spread of disease.
—Jamie Newman, MD, FACP
Where will you be in 20 years? If you’re a young hospitalist, you may work in an enormous state-of-the-art hospital complex that includes the latest technologies, the best in amenities, and a well-thought-out design that will meet your needs and those of other staff for years to come.
“There are a lot of different approaches” to designing the hospital facility of the future, says George R. Tingwald, MD, AIA, ACHA, director of healthcare design at Skidmore, Owings, and Merrill in San Francisco. “The difference depends on whether you look at it from a constructability standpoint versus a much more consumer-based focus. Though many think they have the right approach, it’s hard to say that everybody’s decided on a single solution.”
The Future Looks … Big
It’s not just the hospital facility itself that will change in the future. The number of hospitals in each community may change as well—and the hospitals will be considerably larger.
“We will probably see fewer but larger hospitals in the future,” predicts Dr. Tingwald. “We’re in an era where we’re seeing significant growth in the number of inpatients served. Because of the baby boom and increasing longevity in Americans we’re already seeing an increase, and it’s going to continue. We’ll definitely see more hospital beds in the future.”
The type of patients who fill those hospital beds will change as well.
“We’ll continue to see sicker and sicker patients in those hospital beds,” says Dr. Tingwald. “More people will be managed on an outpatient basis as more diagnostic and treatment procedures will be done as outpatients. Look at breast cancer: From initial detection to diagnosis to biopsy to lumpectomy to chemotherapy or radiation treatment, to cure, or end-of-life care, each step can now be done on an outpatient basis.”
What does this mean? “Someone can have a very significant, multiepisodic disease and never stay in the hospital—unless there are complications,” explains Dr. Tingwald. “Therefore, we’ll have only very acute patients in the hospital. The hospital will basically become an intensive care unit.”
In the past, approximately 10% of a hospital’s beds were in the ICU. That percentage is rising—an indication of things to come. That percentage is now around 20% or 30% and growing, especially in major centers. Only seriously ill people will be admitted—but even they won’t spend a lot of time in the hospital. They will die, recover to a point where they can be moved to rehabilitation or other support facility, or be sent home.
What about the prediction that there will be fewer hospitals in the future? Dr. Tingwald predicts that technology and expertise will weed out some facilities.
“We used to have a lot of what I would call general hospitals—meaning every one was the same,” he explains. “That’s changing radically. The institutions with the expertise and wherewithal to develop technical sophistication, such as university hospitals and specialty hospitals, are doing well. Those that don’t have that sophistication can’t keep up. The big centers are growing because they have the equipment and the expertise. The smaller ones are failing.”
This trend may come as a surprise to some in healthcare, in light of previous predictions. “This is different than the futurists were saying 10 or 20 years ago, when predictions were for more home-based and community-based care,” says Dr. Tingwald. “The reverse has happened. The latest equipment is not available to everyone, let alone smaller, unaffiliated hospitals. And the people that can work with that technology are few and far between.”
The addition of new technology will have some effect on the size of the hospital. “You need a lot of physical space for wiring,” admits Dr. Tingwald. “But the ‘brains’ of the technology can be offsite at a separate IT center or data center.”
Focus on Family-Centered Care
Perhaps the most noticeable differences in the hospital facility of the future will be those related to a change in services, design, and attitude toward providing amenities for patients and their families.
“Patient-centered care, or its close cousin—family-centered care—is a significant trend in healthcare design now, and that significantly impacts the design of facilities,” states Dr. Tingwald. “The most important aspect is having all private rooms. Almost no new construction includes shared patient rooms. The key element of this care is family involvement, and that includes families rooming in with patients. You can’t physically or psychologically do this in a shared room.”
He points out that this trend includes all room types: “It started in pediatrics, but has gone into general acute care settings, intensive care settings, and now neonatal intensive care units.”
What are the pros and cons of a move toward all private rooms? “It takes up room, but it’s proving not to be significantly more costly,” says Dr. Tingwald. “Private rooms are more expensive to build, but in the end they’re less expensive to operate. In an all-private room hospital you can increase your occupancy to 80% or even 90% because you’re not trying to match up patients by gender and age. Also, nursing isn’t moving patients to get the bed mixes right. Studies show that nurses spend up to 40% of their time in transfers. And finally, private rooms have increased market share considerably.”
Another aspect of family centered care is the addition of technologies and services that cater to patient comfort and even enjoyment. “Anything someone has at home or wants in a hotel, families and patients are demanding, including room service,” says Dr. Tingwald. “Patients can decide when and what they want to eat [within their prescribed diet], and families can order food. In some hospitals, patients can already order food using a plasma screen in their room. This is showing to be an economically viable alternative. There’s less food waste, and patients are much happier.”
You’ll also see patient rooms with plasma screen televisions and DVD players, equipped for movies on demand, educational content—even the ability for physicians to view X-rays and other diagnostics on screen, and for families waiting in the room to communicate with physicians in the operating room.
“These are consumer-driven things, but they’re not luxuries,” insists Dr. Tingwald. “They’re often things that save time, increase the ability for education, and significantly decrease errors.”
Another argument for adding amenities like plasma screen TVs and room service: “In healthcare you think adding this technology must be too expensive,” says Dr. Tingwald, “but if you walk into a fast-food place, the person behind the counter uses a touch screen. Everybody else has done this already. Facilities that don’t partake in these transitions are not going to survive.”
Other family-centered improvements include major changes in patient registration. “Most registration can be done from home, over the Internet,” he says. “At Northwestern Memorial Hospital [in Chicago], patients have an encoded card they swipe when they drive into the parking garage, and the receptionist knows they’re coming and gets their room ready before they arrive.”
In the future, more facilities will offer options like these to make the registration process easy and fast.
The hospital of the future will feature a friendlier environment, with landscaping and nice views from patient rooms, artwork and amenities that are important in the healing process. They will also include an emphasis on alternative treatments, says Dr. Tingwald, “from massage to aromatherapy to spaces for yoga or meditation.”
Plan for Flexibility
The key to the design of the hospital of the future will be its ability to change without building additions, remodeling, or rehabbing.
“We’re no longer planning a facility in a static way, thinking that things will not change. Flexibility and adaptability are planned from the beginning,” explains Dr. Tingwald. “You’ll see a lot more generic room types—rooms that are all a single size, but adaptable. A private patient room might be initially planned for acute care, but it can be adapted for an ICU room with minimal or no remodeling.”
This holds true for other room types as well. “In diagnostic and treatment spaces, we plan for one, or no more than two, sizes of space,” he says. “You don’t know if in the future more procedures will be surgical or non-invasive, so rooms are planned to handle both functions. Also, the kingdoms are coming down and divisions between diagnostic departments are blending.”
The Johns Hopkins Hospital (Baltimore), the University of California, Los Angeles Medical Center, and California Pacific Medical Center in San Francisco are all designing “platform floors,” where surgery, interventional imaging, cardiac catheterization, and other procedure-based services share preoperative and postoperative areas and have single access.
“These floors provide adjacency of services allowing a lot more flexibility and decreased redundancy,” explains Dr. Tingwald. “Also, there aren’t as many patient transfers, and a key to patient-centered care is less movement of the patient.”
Built-in flexibility is designed to accommodate scalability as well. “In the planning process, we anticipate higher volumes in an emergency or disaster,” he says. “We plan how to expand the emergency room, and we make rooms larger than we used to. That way, if volumes increase quickly, you could put two, three, maybe more patients in a space. Nurses hate when you say that, but we have to have timely solutions that are affordable. This approach can be considered on nursing units as well, with these ‘super singles’ able to handle a second patient during a February flu outbreak, for example. That’s better than having an entire wing of the hospital that’s only used during winter months, patients stuck in the emergency department for days, or patients in the halls.”
A Design with Built-In Patient Safety
The physical design of the hospital of the future will better address and correct issues with patient safety. “Whatever design elements can minimize errors and improve outcomes are being studied intensively right now,” says Dr. Tingwald. “For example, we used to mirror many room types so that walls could share plumbing, etc. One room would be the mirror image of the one next to it, requiring the staff to learn different layouts, which increases time of response and possible errors. Now, we try to make procedure rooms as similar as possible to reduce the potential for error.”
There are design elements that limit the possibility of hospital-borne infection, including ultraviolet light and biologic surfaces. There is also a greater emphasis on including track systems for lifts for getting patients out of bed and moving them without injury to the patient or the staff.
Consider Hospitalists and Other Staff
How will the hospital of the future accommodate hospitalists?
“We’re certainly seeing more hospitalists,” says Dr. Tingwald. “As you have sicker patients in the hospital, it’s harder for their primary care physicians to manage them, so we’re going to see even more hospitalists. This means that we have to provide space for them; both offices, because they don’t have other office space, and sleeping accommodations, which means private rooms with bath, as well as lounge space.”
Hospitals will provide appealing space for physicians because it will help them recruit hospitalists. Improving lounges and other staff spaces will be a goal of future hospital designs.
“There will be a lot more emphasis on good environments for work and for support services,” predicts Dr. Tingwald. “This will increase the attraction and retention of top staff. You’ll see things like fitness centers, and basic additions like enough parking spaces.”
As hospital facilities move toward more patient-centered care, with flexible layouts and space designed for patient safety, the working environment is certain to become more conducive to providing good care and working efficiently. It will also become more comfortable, convenient, and pleasant for hospitalists and other staff. And that is something to look forward to. TH
Writer Jane Jerrard wrote the first three installments of the “Future” series.
FLASHBACK
Cadaver Particles
—Ignaz Semmelweis, 1861
Death stalked the halls of the First Division of the Allegemeine Krankenhaus (Vienna General Hospital), a large teaching hospital in Austria. Healthy post-partum women suddenly become febrile and died from puerperal sepsis (childbed fever). In the mid-19th century, this problem was seen in hospitals across Europe, though rarely in home deliveries. It was a seemingly insoluble dilemma. Opinions varied on the etiology. Was it miasmas, the paint on the walls, were the beds too close, or was it clogged milk glands? Complacency and acceptance of status quo were, to some, the easiest solution.
In the mid-1800s Hungarian Physician Ignaz Semmelweis was given an appointment as an assistant in obstetrics at the Allegemeine Krankenhaus. He had adopted the Austrian paradigm of clinical and pathologic anatomy. The answer to any question lay in the autopsy. It seemed like the more autopsies they did, the more women died. The death of Semmelweis’ colleague, Jakob Kolletschka (who was initially injured when his knife slipped during an autopsy of a woman who died of puerperal fever and then died himself of symptoms similar to those that killed the woman) gave Semmelweis the vital clue.
He realized that something carried on unwashed surgeons’ hands from infected cadavers caused the disease to occur in the women. These “cadaver particles” were transmitted from the morning autopsies to the women on the wards by the unwashed hands of students and faculty. Adopting proper hygiene could save thousands of lives. Properly washed hands were the simple answer. This also explained the mystery of why the puerperal fever rate was lower on the midwife-run wards where they did not do autopsies.
Decades before Pasteur and Lister, accepting that their own hands brought death was a bitter pill for the great men of obstetrics to swallow. Unfortunately for Semmelweis and the women who continued to die, it was years before Oliver Wendell Holmes incontrovertibly published his essay, “The Contagiousness of Puerperal Fever” in 1843 in the New England Quarterly Journal of Medicine. That essay showed the source of puerperal fever. Despite his clinical success Semmelweis was unable to persuade his fellow physicians.
The nosocomial spread of infection on unwashed hands rings true to this day. We spend our days gloved, gowned, and masked in the battle against MRSA, VRE, and other pathogens. Whether soap or alcohol, when we scrub our hands we should remember that it is more than a ritual. It’s a duty to prevent the spread of disease.
—Jamie Newman, MD, FACP
The Future of Critical Care
Critical care is starting to face some tough obstacles, and the ICU of the future will be shaped by these problems—namely an aging population and a shrinking field of expert critical care practitioners. Because of these impending changes, in 20 or 30 years your hospital’s ICU must look different and work differently in order to handle a steady influx of critically ill patients.
This installment of our “Hospital of the Future” series will examine how the hospital of the future will deal effectively with the supply-and-demand quandary that is already becoming apparent in the ICU. It will also examine future possibilities for staffing structure, introduction of critical care guidelines, and groundbreaking technical solutions. Prospects for critical care may look questionable now, but solutions are available. And the future just might be brighter than expected.
Supply and Demand of Critical Care Demands Change
Current trends in both the U.S. population and the demographics of critical care staff dictate that critical care must change—and fast. With millions of baby boomers aging, demand for critical care facilities within hospitals will increase.
“There’s little question that critical care is used disproportionately by the elderly,” says Timothy Buchman, MD, PhD, FACS, FCCM, past president of the Society of Critical Care Medicine (SCCM) and professor at Washington University School of Medicine, St. Louis. “The demand can only increase as the population ages.”
At the same time, there are already too few critical care providers in the United States. “If we designed an ideal ICU for every hospital in the country, we could only staff about one-third of them” right now, says Thomas Rainey, MD, FCCM, president, CriticalMed, Inc., Bethesda, Md.
Critical care experts are, of course, the key to quality care in the ICU. But the population of both specially trained intensivists and experienced ICU nurses is declining. The average age of an ICU nurse is now 47, and they are not replaced fast enough.
“Critical care nursing is brutally hard work; it’s physically, emotionally, and spiritually grueling,” points out Dr. Buchman. “The challenge is keeping experienced nurses from leaving because they’re burned out. We need to keep their knowledge and experience, possibly by creating new positions where their knowledge, experience, and accumulated wisdom can be used to benefit the next generations of patients and providers.”
As for physicians, fewer are choosing critical care, which will likely lead to significant staffing issues. “The number of doctors choosing a career in critical care is leveling off,” says Dr. Buchman. Part of the problem is an educational system that helps medical students choose a specialty.
“We have a direct training path to many specialties through residencies,” he says. “There is no residency in critical care medicine. Instead, we ask people to initially train as something else. We’ve created an educational barrier.”
The upshot of these trends, says Dr. Rainey, is that “the graying population and the loss of [critical care] staff is a collision waiting to happen.”
Dr. Buchman adds, “The question is: How do people organize themselves and leverage technology to address this gap and improve the quality of care?”
How Technology Fits In
In 2001, Richard L. Craft, MSEE, wrote of “Trends in Technology and the Future Intensive Care Unit” ( . 2001;29[8 suppl]): “ … advances in networking are likely to redefine the physical and organizational boundaries of the critical care unit. No longer a self-contained entity … tomorrow’s critical care units are likely to regularly draw on resources—both human and technological—located outside the unit’s physical space.”
The solution to staffing shortages in ICUs lies in using technology that is already available to hospitals.
“Remote monitoring will help leverage existing manpower,” says Dr. Rainey. One option is electronic ICUs—or eICUs, which allow an intensivist and ICU nurse to monitor and manage part or all of the patient population in their organization’s ICU(s) from off-site, if applicable. This remote monitoring supplements on-site hospital staff, but allows fewer specialists access to more patients.
“eICU with smart alerts, physiologic status boards, [and] color-coded assessments of response to protocolized care may help hospitalists and intensivists on-site manage increasingly busy and acute ICUs,” says Dr. Buchman. “The greatest impact will be to facilitate the transformation of data into information and to highlight factors that are of greatest immediate importance.”
In addition to maximizing medical staff, eICU systems can also leverage technical support. Craft writes, “… it is easy to foresee a day when a network of hospitals might centralize its critical care application servers and patient record servers in one location to reduce IT staff overhead, standardize clinical protocols, and automate corporation-wide quality control mechanisms.”
With an eICU system, cameras, monitors, and communication devices provide information on each patient, and can even provide treatment recommendations or guidelines.
“eICU systems are evolving now,” says Dr. Buchman. “They synthesize data streams and allow us to stratify information with respect to how important it is. We’ve [already] had a few components, such as bedside hemodynamic monitors. For each individual patient, a sophisticated system should be able to take data from multiple systems, integrate it, and provide a snapshot of how that patient is doing. Take that throughout the entire ICU and have a display that presents instant pictures of how the ICU is doing. [Have] inventories presented in parallel to providers so they can see where problems are.”
Dr. Buchman predicts that in the future ICU care providers will take on more duties as managers of care.
“ICU providers will go through an evolution like airline pilots did,” he says. “These days, airline transport pilots don’t spend a lot of time actually flying the plane. There are plenty of autopilots and subsystems that do that. The pilot now spends most of her time managing the system, and intervenes as necessary to bring everything into harmony. I think this same type of sophisticated presentation will evolve in the ICU to provide a safer environment that uses the available human resource most efficiently. It won’t save on manpower, but it will greatly increase patient safety.”
J. Christopher Farmer, MD, FCCM, Division of Pulmonary and Critical Care, Mayo Clinic College of Medicine, Rochester, Minn., agrees—especially as relates to disaster response.
“We need technology that doesn’t rely on human factors,” says Dr. Farmer. During a hospital’s disaster response, “we miss things because we don’t notice them. We need automation of systems that will push information to us as computerized analysis; systems that look at everything, including lab results, and postulate on that information. This would help in critical care and could be used in disaster settings as well.”
Dr. Farmer’s vision includes automatic monitoring. “Ideally, I’d like to see every patient have a patch that reads their heart rate, oxygen levels, etc.,” he says. “This 100% monitoring of every patient is applicable in disaster medicine because otherwise you need a person to manually hook up monitors and check vitals on each patient.”
The evolution of ICU technology must focus on bridging the gap between limited staff and growing patient population as well as the gap between adequate care and excellent care.
“Technology is there to serve the patient first, but most importantly, to serve the care alliance of patients and practitioners,” says Dr. Buchman “I think some [advancements] are simply technical toys that are replacing what humans can already do.”
Technology can help identify a disease outbreak or other disaster faster than humans can. Some hospital systems are using surveillance systems that link across their facilities to find patterns. These systems can be used to find medical errors, but they can also act as bio-disease surveillance systems, which can be used to identify a sudden outbreak.
“Say three different hospitals each admit one patient with diarrhea,” says Dr. Farmer. “What if this is the beginning of an outbreak of something? A system that links across hospitals can find these patterns.”
The Critical Care Team of the Future
Today’s most highly developed ICUs are utilizing trained critical care teams to ensure the best possible care. In the future, all ICUs will follow this model in order to improve patient safety and efficiency of care.
These teams can include “not only physicians and nurses, but also respiratory therapists, nutritional support staff, and pharmacists, who collectively function as a highly integrated team, following protocols,” says Dr. Buchman. “This team formulates a patient plan together and evaluates the impact of that plan. I think we’re seeing more of that now, and we’re going to see a lot more of it. It’s a continuum; a growth process.
“This is not restricted to medical care; it will include social and spiritual care as well, with a team of case managers, social workers, and chaplains,” he continues. “These professionals contribute to the integrated care plans.”
Dr. Rainey agrees. “We’ll see a reorganization of physician services into an intensivist team model,” he predicts. “The development we’ve seen over the last 20 years is that outcomes are better with a unit-based special team that manages patients in cooperation with the primary care physician. In fact, this approach has shown something like a 30% decrease in risk for mortality.”
This team approach also applies to hospital disaster preparedness. In his white paper “Hospital Disaster Medical Response: Aligning Everyday Requirements with Emergency Casualty Care,” Dr. Farmer says, “ … we are witnessing the rapid development and emergence of medical emergency teams, or rapid response teams within the hospital. … These teams are intended to monitor inpatients and intervene before physiological deterioration supervenes. One might ask, in the event of a medical disaster, could these teams be repurposed for sophisticated casualty care and ICU expansion? We think it is logical that these types of critical care ‘outreach’ teams, in conjunction with noncritical care hospital personnel, could be leveraged as an effective strategy to extend ICU capabilities during a disaster.”
Having a complete team of ICU providers address each patient’s needs will vastly improve quality of care, but these teams must have some guidelines to follow in order to ensure that they work at maximum efficiency.
Critical Care Guidelines: An Integral Component
Critical care experts shy away from such buzzwords and phrases as “standardization of care” in regard to ICU practices, but they do agree that universal guidelines will be the norm in the future.
“We’ll see the development of drastically improved outcomes, and reduction in harm through reliable processes,” says Dr. Rainey. “We can see, for example, that five things need to be done to every ventilated patient. With development of reliable processes in place, we can see that we will close the gap between intent and actual execution.”
Dr. Farmer agrees. “We do clinical guidelines for everyday issues, so I don’t see why we can’t do the same thing” for critical care and disaster preparedness.
Critical care is ripe for integrating clinical practice guidelines. “There are certain types of interventions that are near universal in ICUs,” says Dr. Buchman. “How we sedate patients, how we relieve pain, how we liberate someone from mechanical support … having touchstones or guidelines for these interventions will help. This is complementary to standardization of care.
“Here’s an example: A patient is admitted with a myocardial infarction. We would treat him with beta-blockers, nitrates, heparin, and aspirin. We don’t think of a standard dose of beta-blockers because the dose must be titrated to [have an] effect on the individual patient,” he continues. “How this individualization is done safely involves organizational guidelines. Systematic implementation of such guidelines will be the difference between good ICUs and great ICUs. The implementation is a continuous four-step process—learn the recommendations, deliver the care, measure the outcomes, and find ways to improve.”
Hospitalists and Critical Care
In concert with technologic advancement and improved guidelines, one major solution to the staffing shortage is hospitalists. According to Dr. Farmer, a large portion of critical care services across the country is provided by family practitioners and general internists. The demographics of the population, combined with the current system of training, ensure inadequate staffing. That shortage could be filled by hospitalists. For many hospitalists ICU care is already an important and satisfying arm of their practice. It may become necessary in the future to define skill sets to work in critical care areas. Hospitalists are well positioned to fill that need.
Looking Ahead
The area of critical care may be moving more quickly toward the future than other hospital functions because it must do so in order to continue to work at all. The success of achieving a future of quality care, patient safety, and adequate staffing rests on a different approach with providers and technology.
“We have to learn to work smarter to leverage new technology and the expertise of all other experts in other fields,” says Dr. Buchman of the future of critical care.TH
Chicago-based Jane Jerrard will write future installments of this series.
FLASHBACK:
An Ill Wind
An 1883 tornado strikes a familiar chord in today’s hurricane-ridden times

“An ill wind”—these were the opening words spoken by William Worrall, MD, at the official opening ceremony for St. Mary’s Hospital in Rochester, Minn. The hospital had been conceived following the destruction wrought on Rochester by a tornado that had left 37 dead and more than 200 injured six years earlier.
Aug. 12, 1883, was a particularly hot day, and many residents must have been hopeful of relief as they saw black clouds looming to the west late that evening. That evening Dr. William Mayo’s sons, Will and Charlie, were headed to the slaughterhouse northwest of town in the part of Rochester then known as the Lower Town to purchase a sheep’s head for eye dissections. The butchers had closed early because of the impending storm and advised the young Mayos to head back posthaste.
The cyclone descended just as they crossed a bridge, which was torn loose of its moorings, over the Zumbro River. They witnessed buildings smashed to bits, a grain elevator toppled, and railroad cars wrecked by the destructive force. They were almost killed by a heavy cornice that had ripped off the Cook House and smashed into their buggy. The Cook House was adjacent to the Cook Block that housed the offices of the Doctors Mayo. Though their buggy was destroyed, they survived and took shelter with their horse in a blacksmith’s shop.
They survived the storm, but others were not so lucky. One-third of the buildings in town were destroyed or damaged with more than half in Lower Town, a predominantly working class neighborhood. They immediately began to care for the wounded brought to the clinic offices. Their father had taken charge of relief efforts in Lower Town, the worst hit part of the city. Victims were brought to a local hotel, where they were quickly triaged and treated according to need.
The physicians in town shared a common goal though they were not always united in their methods. The routine use of an emetic for all trauma patients was advocated by one physician to the opprobrium of the elder Dr. Mayo, who quickly insisted on establishment of clear leadership. He also recruited the assistance of Sister Alfred Moes, who had offered her convent to shelter the sick and homeless and her nuns as nurses for the injured.
The anti-Catholic prejudices of the day necessitated Dr. W. Mayo asking that it be announced that Sister Alfred was offering shelter in her “house” and not in a convent. Other relief efforts such as offering food and provisions to the needy were established in available rooms across town. Recovery of bodies, funeral services, and burials were quickly conducted. Rebuilding efforts were speedily begun with fundraising activities bringing in enough funds to feed and clothe hundreds, rebuild more than 100 houses, and provide money for furniture.
The tornado had highlighted the need for a hospital in Rochester and Sister Alfred ultimately requested that Dr. W. Mayo assist in this venture. The Sisters of Saint Francis raised money and built Saint Mary’s Hospital—the first in Rochester.
The destruction and chaos caused by Hurricane Katrina has brought much pain to our nation. In the early aftermath there appeared to be a dearth of leadership, and questions arose regarding an apparent lack of preparedness and poor response to the carnage caused by the storm. Undoubtedly there will be many investigations into what went wrong. History may help answer these questions, but should also provide reassurance that good can come out of the debris of an ill wind.
—Jamie Newman, MD, FACP, and Adeboye B. Ogunseitan, MD
Critical care is starting to face some tough obstacles, and the ICU of the future will be shaped by these problems—namely an aging population and a shrinking field of expert critical care practitioners. Because of these impending changes, in 20 or 30 years your hospital’s ICU must look different and work differently in order to handle a steady influx of critically ill patients.
This installment of our “Hospital of the Future” series will examine how the hospital of the future will deal effectively with the supply-and-demand quandary that is already becoming apparent in the ICU. It will also examine future possibilities for staffing structure, introduction of critical care guidelines, and groundbreaking technical solutions. Prospects for critical care may look questionable now, but solutions are available. And the future just might be brighter than expected.
Supply and Demand of Critical Care Demands Change
Current trends in both the U.S. population and the demographics of critical care staff dictate that critical care must change—and fast. With millions of baby boomers aging, demand for critical care facilities within hospitals will increase.
“There’s little question that critical care is used disproportionately by the elderly,” says Timothy Buchman, MD, PhD, FACS, FCCM, past president of the Society of Critical Care Medicine (SCCM) and professor at Washington University School of Medicine, St. Louis. “The demand can only increase as the population ages.”
At the same time, there are already too few critical care providers in the United States. “If we designed an ideal ICU for every hospital in the country, we could only staff about one-third of them” right now, says Thomas Rainey, MD, FCCM, president, CriticalMed, Inc., Bethesda, Md.
Critical care experts are, of course, the key to quality care in the ICU. But the population of both specially trained intensivists and experienced ICU nurses is declining. The average age of an ICU nurse is now 47, and they are not replaced fast enough.
“Critical care nursing is brutally hard work; it’s physically, emotionally, and spiritually grueling,” points out Dr. Buchman. “The challenge is keeping experienced nurses from leaving because they’re burned out. We need to keep their knowledge and experience, possibly by creating new positions where their knowledge, experience, and accumulated wisdom can be used to benefit the next generations of patients and providers.”
As for physicians, fewer are choosing critical care, which will likely lead to significant staffing issues. “The number of doctors choosing a career in critical care is leveling off,” says Dr. Buchman. Part of the problem is an educational system that helps medical students choose a specialty.
“We have a direct training path to many specialties through residencies,” he says. “There is no residency in critical care medicine. Instead, we ask people to initially train as something else. We’ve created an educational barrier.”
The upshot of these trends, says Dr. Rainey, is that “the graying population and the loss of [critical care] staff is a collision waiting to happen.”
Dr. Buchman adds, “The question is: How do people organize themselves and leverage technology to address this gap and improve the quality of care?”
How Technology Fits In
In 2001, Richard L. Craft, MSEE, wrote of “Trends in Technology and the Future Intensive Care Unit” ( . 2001;29[8 suppl]): “ … advances in networking are likely to redefine the physical and organizational boundaries of the critical care unit. No longer a self-contained entity … tomorrow’s critical care units are likely to regularly draw on resources—both human and technological—located outside the unit’s physical space.”
The solution to staffing shortages in ICUs lies in using technology that is already available to hospitals.
“Remote monitoring will help leverage existing manpower,” says Dr. Rainey. One option is electronic ICUs—or eICUs, which allow an intensivist and ICU nurse to monitor and manage part or all of the patient population in their organization’s ICU(s) from off-site, if applicable. This remote monitoring supplements on-site hospital staff, but allows fewer specialists access to more patients.
“eICU with smart alerts, physiologic status boards, [and] color-coded assessments of response to protocolized care may help hospitalists and intensivists on-site manage increasingly busy and acute ICUs,” says Dr. Buchman. “The greatest impact will be to facilitate the transformation of data into information and to highlight factors that are of greatest immediate importance.”
In addition to maximizing medical staff, eICU systems can also leverage technical support. Craft writes, “… it is easy to foresee a day when a network of hospitals might centralize its critical care application servers and patient record servers in one location to reduce IT staff overhead, standardize clinical protocols, and automate corporation-wide quality control mechanisms.”
With an eICU system, cameras, monitors, and communication devices provide information on each patient, and can even provide treatment recommendations or guidelines.
“eICU systems are evolving now,” says Dr. Buchman. “They synthesize data streams and allow us to stratify information with respect to how important it is. We’ve [already] had a few components, such as bedside hemodynamic monitors. For each individual patient, a sophisticated system should be able to take data from multiple systems, integrate it, and provide a snapshot of how that patient is doing. Take that throughout the entire ICU and have a display that presents instant pictures of how the ICU is doing. [Have] inventories presented in parallel to providers so they can see where problems are.”
Dr. Buchman predicts that in the future ICU care providers will take on more duties as managers of care.
“ICU providers will go through an evolution like airline pilots did,” he says. “These days, airline transport pilots don’t spend a lot of time actually flying the plane. There are plenty of autopilots and subsystems that do that. The pilot now spends most of her time managing the system, and intervenes as necessary to bring everything into harmony. I think this same type of sophisticated presentation will evolve in the ICU to provide a safer environment that uses the available human resource most efficiently. It won’t save on manpower, but it will greatly increase patient safety.”
J. Christopher Farmer, MD, FCCM, Division of Pulmonary and Critical Care, Mayo Clinic College of Medicine, Rochester, Minn., agrees—especially as relates to disaster response.
“We need technology that doesn’t rely on human factors,” says Dr. Farmer. During a hospital’s disaster response, “we miss things because we don’t notice them. We need automation of systems that will push information to us as computerized analysis; systems that look at everything, including lab results, and postulate on that information. This would help in critical care and could be used in disaster settings as well.”
Dr. Farmer’s vision includes automatic monitoring. “Ideally, I’d like to see every patient have a patch that reads their heart rate, oxygen levels, etc.,” he says. “This 100% monitoring of every patient is applicable in disaster medicine because otherwise you need a person to manually hook up monitors and check vitals on each patient.”
The evolution of ICU technology must focus on bridging the gap between limited staff and growing patient population as well as the gap between adequate care and excellent care.
“Technology is there to serve the patient first, but most importantly, to serve the care alliance of patients and practitioners,” says Dr. Buchman “I think some [advancements] are simply technical toys that are replacing what humans can already do.”
Technology can help identify a disease outbreak or other disaster faster than humans can. Some hospital systems are using surveillance systems that link across their facilities to find patterns. These systems can be used to find medical errors, but they can also act as bio-disease surveillance systems, which can be used to identify a sudden outbreak.
“Say three different hospitals each admit one patient with diarrhea,” says Dr. Farmer. “What if this is the beginning of an outbreak of something? A system that links across hospitals can find these patterns.”
The Critical Care Team of the Future
Today’s most highly developed ICUs are utilizing trained critical care teams to ensure the best possible care. In the future, all ICUs will follow this model in order to improve patient safety and efficiency of care.
These teams can include “not only physicians and nurses, but also respiratory therapists, nutritional support staff, and pharmacists, who collectively function as a highly integrated team, following protocols,” says Dr. Buchman. “This team formulates a patient plan together and evaluates the impact of that plan. I think we’re seeing more of that now, and we’re going to see a lot more of it. It’s a continuum; a growth process.
“This is not restricted to medical care; it will include social and spiritual care as well, with a team of case managers, social workers, and chaplains,” he continues. “These professionals contribute to the integrated care plans.”
Dr. Rainey agrees. “We’ll see a reorganization of physician services into an intensivist team model,” he predicts. “The development we’ve seen over the last 20 years is that outcomes are better with a unit-based special team that manages patients in cooperation with the primary care physician. In fact, this approach has shown something like a 30% decrease in risk for mortality.”
This team approach also applies to hospital disaster preparedness. In his white paper “Hospital Disaster Medical Response: Aligning Everyday Requirements with Emergency Casualty Care,” Dr. Farmer says, “ … we are witnessing the rapid development and emergence of medical emergency teams, or rapid response teams within the hospital. … These teams are intended to monitor inpatients and intervene before physiological deterioration supervenes. One might ask, in the event of a medical disaster, could these teams be repurposed for sophisticated casualty care and ICU expansion? We think it is logical that these types of critical care ‘outreach’ teams, in conjunction with noncritical care hospital personnel, could be leveraged as an effective strategy to extend ICU capabilities during a disaster.”
Having a complete team of ICU providers address each patient’s needs will vastly improve quality of care, but these teams must have some guidelines to follow in order to ensure that they work at maximum efficiency.
Critical Care Guidelines: An Integral Component
Critical care experts shy away from such buzzwords and phrases as “standardization of care” in regard to ICU practices, but they do agree that universal guidelines will be the norm in the future.
“We’ll see the development of drastically improved outcomes, and reduction in harm through reliable processes,” says Dr. Rainey. “We can see, for example, that five things need to be done to every ventilated patient. With development of reliable processes in place, we can see that we will close the gap between intent and actual execution.”
Dr. Farmer agrees. “We do clinical guidelines for everyday issues, so I don’t see why we can’t do the same thing” for critical care and disaster preparedness.
Critical care is ripe for integrating clinical practice guidelines. “There are certain types of interventions that are near universal in ICUs,” says Dr. Buchman. “How we sedate patients, how we relieve pain, how we liberate someone from mechanical support … having touchstones or guidelines for these interventions will help. This is complementary to standardization of care.
“Here’s an example: A patient is admitted with a myocardial infarction. We would treat him with beta-blockers, nitrates, heparin, and aspirin. We don’t think of a standard dose of beta-blockers because the dose must be titrated to [have an] effect on the individual patient,” he continues. “How this individualization is done safely involves organizational guidelines. Systematic implementation of such guidelines will be the difference between good ICUs and great ICUs. The implementation is a continuous four-step process—learn the recommendations, deliver the care, measure the outcomes, and find ways to improve.”
Hospitalists and Critical Care
In concert with technologic advancement and improved guidelines, one major solution to the staffing shortage is hospitalists. According to Dr. Farmer, a large portion of critical care services across the country is provided by family practitioners and general internists. The demographics of the population, combined with the current system of training, ensure inadequate staffing. That shortage could be filled by hospitalists. For many hospitalists ICU care is already an important and satisfying arm of their practice. It may become necessary in the future to define skill sets to work in critical care areas. Hospitalists are well positioned to fill that need.
Looking Ahead
The area of critical care may be moving more quickly toward the future than other hospital functions because it must do so in order to continue to work at all. The success of achieving a future of quality care, patient safety, and adequate staffing rests on a different approach with providers and technology.
“We have to learn to work smarter to leverage new technology and the expertise of all other experts in other fields,” says Dr. Buchman of the future of critical care.TH
Chicago-based Jane Jerrard will write future installments of this series.
FLASHBACK:
An Ill Wind
An 1883 tornado strikes a familiar chord in today’s hurricane-ridden times
“An ill wind”—these were the opening words spoken by William Worrall, MD, at the official opening ceremony for St. Mary’s Hospital in Rochester, Minn. The hospital had been conceived following the destruction wrought on Rochester by a tornado that had left 37 dead and more than 200 injured six years earlier.
Aug. 12, 1883, was a particularly hot day, and many residents must have been hopeful of relief as they saw black clouds looming to the west late that evening. That evening Dr. William Mayo’s sons, Will and Charlie, were headed to the slaughterhouse northwest of town in the part of Rochester then known as the Lower Town to purchase a sheep’s head for eye dissections. The butchers had closed early because of the impending storm and advised the young Mayos to head back posthaste.
The cyclone descended just as they crossed a bridge, which was torn loose of its moorings, over the Zumbro River. They witnessed buildings smashed to bits, a grain elevator toppled, and railroad cars wrecked by the destructive force. They were almost killed by a heavy cornice that had ripped off the Cook House and smashed into their buggy. The Cook House was adjacent to the Cook Block that housed the offices of the Doctors Mayo. Though their buggy was destroyed, they survived and took shelter with their horse in a blacksmith’s shop.
They survived the storm, but others were not so lucky. One-third of the buildings in town were destroyed or damaged with more than half in Lower Town, a predominantly working class neighborhood. They immediately began to care for the wounded brought to the clinic offices. Their father had taken charge of relief efforts in Lower Town, the worst hit part of the city. Victims were brought to a local hotel, where they were quickly triaged and treated according to need.
The physicians in town shared a common goal though they were not always united in their methods. The routine use of an emetic for all trauma patients was advocated by one physician to the opprobrium of the elder Dr. Mayo, who quickly insisted on establishment of clear leadership. He also recruited the assistance of Sister Alfred Moes, who had offered her convent to shelter the sick and homeless and her nuns as nurses for the injured.
The anti-Catholic prejudices of the day necessitated Dr. W. Mayo asking that it be announced that Sister Alfred was offering shelter in her “house” and not in a convent. Other relief efforts such as offering food and provisions to the needy were established in available rooms across town. Recovery of bodies, funeral services, and burials were quickly conducted. Rebuilding efforts were speedily begun with fundraising activities bringing in enough funds to feed and clothe hundreds, rebuild more than 100 houses, and provide money for furniture.
The tornado had highlighted the need for a hospital in Rochester and Sister Alfred ultimately requested that Dr. W. Mayo assist in this venture. The Sisters of Saint Francis raised money and built Saint Mary’s Hospital—the first in Rochester.
The destruction and chaos caused by Hurricane Katrina has brought much pain to our nation. In the early aftermath there appeared to be a dearth of leadership, and questions arose regarding an apparent lack of preparedness and poor response to the carnage caused by the storm. Undoubtedly there will be many investigations into what went wrong. History may help answer these questions, but should also provide reassurance that good can come out of the debris of an ill wind.
—Jamie Newman, MD, FACP, and Adeboye B. Ogunseitan, MD
Critical care is starting to face some tough obstacles, and the ICU of the future will be shaped by these problems—namely an aging population and a shrinking field of expert critical care practitioners. Because of these impending changes, in 20 or 30 years your hospital’s ICU must look different and work differently in order to handle a steady influx of critically ill patients.
This installment of our “Hospital of the Future” series will examine how the hospital of the future will deal effectively with the supply-and-demand quandary that is already becoming apparent in the ICU. It will also examine future possibilities for staffing structure, introduction of critical care guidelines, and groundbreaking technical solutions. Prospects for critical care may look questionable now, but solutions are available. And the future just might be brighter than expected.
Supply and Demand of Critical Care Demands Change
Current trends in both the U.S. population and the demographics of critical care staff dictate that critical care must change—and fast. With millions of baby boomers aging, demand for critical care facilities within hospitals will increase.
“There’s little question that critical care is used disproportionately by the elderly,” says Timothy Buchman, MD, PhD, FACS, FCCM, past president of the Society of Critical Care Medicine (SCCM) and professor at Washington University School of Medicine, St. Louis. “The demand can only increase as the population ages.”
At the same time, there are already too few critical care providers in the United States. “If we designed an ideal ICU for every hospital in the country, we could only staff about one-third of them” right now, says Thomas Rainey, MD, FCCM, president, CriticalMed, Inc., Bethesda, Md.
Critical care experts are, of course, the key to quality care in the ICU. But the population of both specially trained intensivists and experienced ICU nurses is declining. The average age of an ICU nurse is now 47, and they are not replaced fast enough.
“Critical care nursing is brutally hard work; it’s physically, emotionally, and spiritually grueling,” points out Dr. Buchman. “The challenge is keeping experienced nurses from leaving because they’re burned out. We need to keep their knowledge and experience, possibly by creating new positions where their knowledge, experience, and accumulated wisdom can be used to benefit the next generations of patients and providers.”
As for physicians, fewer are choosing critical care, which will likely lead to significant staffing issues. “The number of doctors choosing a career in critical care is leveling off,” says Dr. Buchman. Part of the problem is an educational system that helps medical students choose a specialty.
“We have a direct training path to many specialties through residencies,” he says. “There is no residency in critical care medicine. Instead, we ask people to initially train as something else. We’ve created an educational barrier.”
The upshot of these trends, says Dr. Rainey, is that “the graying population and the loss of [critical care] staff is a collision waiting to happen.”
Dr. Buchman adds, “The question is: How do people organize themselves and leverage technology to address this gap and improve the quality of care?”
How Technology Fits In
In 2001, Richard L. Craft, MSEE, wrote of “Trends in Technology and the Future Intensive Care Unit” ( . 2001;29[8 suppl]): “ … advances in networking are likely to redefine the physical and organizational boundaries of the critical care unit. No longer a self-contained entity … tomorrow’s critical care units are likely to regularly draw on resources—both human and technological—located outside the unit’s physical space.”
The solution to staffing shortages in ICUs lies in using technology that is already available to hospitals.
“Remote monitoring will help leverage existing manpower,” says Dr. Rainey. One option is electronic ICUs—or eICUs, which allow an intensivist and ICU nurse to monitor and manage part or all of the patient population in their organization’s ICU(s) from off-site, if applicable. This remote monitoring supplements on-site hospital staff, but allows fewer specialists access to more patients.
“eICU with smart alerts, physiologic status boards, [and] color-coded assessments of response to protocolized care may help hospitalists and intensivists on-site manage increasingly busy and acute ICUs,” says Dr. Buchman. “The greatest impact will be to facilitate the transformation of data into information and to highlight factors that are of greatest immediate importance.”
In addition to maximizing medical staff, eICU systems can also leverage technical support. Craft writes, “… it is easy to foresee a day when a network of hospitals might centralize its critical care application servers and patient record servers in one location to reduce IT staff overhead, standardize clinical protocols, and automate corporation-wide quality control mechanisms.”
With an eICU system, cameras, monitors, and communication devices provide information on each patient, and can even provide treatment recommendations or guidelines.
“eICU systems are evolving now,” says Dr. Buchman. “They synthesize data streams and allow us to stratify information with respect to how important it is. We’ve [already] had a few components, such as bedside hemodynamic monitors. For each individual patient, a sophisticated system should be able to take data from multiple systems, integrate it, and provide a snapshot of how that patient is doing. Take that throughout the entire ICU and have a display that presents instant pictures of how the ICU is doing. [Have] inventories presented in parallel to providers so they can see where problems are.”
Dr. Buchman predicts that in the future ICU care providers will take on more duties as managers of care.
“ICU providers will go through an evolution like airline pilots did,” he says. “These days, airline transport pilots don’t spend a lot of time actually flying the plane. There are plenty of autopilots and subsystems that do that. The pilot now spends most of her time managing the system, and intervenes as necessary to bring everything into harmony. I think this same type of sophisticated presentation will evolve in the ICU to provide a safer environment that uses the available human resource most efficiently. It won’t save on manpower, but it will greatly increase patient safety.”
J. Christopher Farmer, MD, FCCM, Division of Pulmonary and Critical Care, Mayo Clinic College of Medicine, Rochester, Minn., agrees—especially as relates to disaster response.
“We need technology that doesn’t rely on human factors,” says Dr. Farmer. During a hospital’s disaster response, “we miss things because we don’t notice them. We need automation of systems that will push information to us as computerized analysis; systems that look at everything, including lab results, and postulate on that information. This would help in critical care and could be used in disaster settings as well.”
Dr. Farmer’s vision includes automatic monitoring. “Ideally, I’d like to see every patient have a patch that reads their heart rate, oxygen levels, etc.,” he says. “This 100% monitoring of every patient is applicable in disaster medicine because otherwise you need a person to manually hook up monitors and check vitals on each patient.”
The evolution of ICU technology must focus on bridging the gap between limited staff and growing patient population as well as the gap between adequate care and excellent care.
“Technology is there to serve the patient first, but most importantly, to serve the care alliance of patients and practitioners,” says Dr. Buchman “I think some [advancements] are simply technical toys that are replacing what humans can already do.”
Technology can help identify a disease outbreak or other disaster faster than humans can. Some hospital systems are using surveillance systems that link across their facilities to find patterns. These systems can be used to find medical errors, but they can also act as bio-disease surveillance systems, which can be used to identify a sudden outbreak.
“Say three different hospitals each admit one patient with diarrhea,” says Dr. Farmer. “What if this is the beginning of an outbreak of something? A system that links across hospitals can find these patterns.”
The Critical Care Team of the Future
Today’s most highly developed ICUs are utilizing trained critical care teams to ensure the best possible care. In the future, all ICUs will follow this model in order to improve patient safety and efficiency of care.
These teams can include “not only physicians and nurses, but also respiratory therapists, nutritional support staff, and pharmacists, who collectively function as a highly integrated team, following protocols,” says Dr. Buchman. “This team formulates a patient plan together and evaluates the impact of that plan. I think we’re seeing more of that now, and we’re going to see a lot more of it. It’s a continuum; a growth process.
“This is not restricted to medical care; it will include social and spiritual care as well, with a team of case managers, social workers, and chaplains,” he continues. “These professionals contribute to the integrated care plans.”
Dr. Rainey agrees. “We’ll see a reorganization of physician services into an intensivist team model,” he predicts. “The development we’ve seen over the last 20 years is that outcomes are better with a unit-based special team that manages patients in cooperation with the primary care physician. In fact, this approach has shown something like a 30% decrease in risk for mortality.”
This team approach also applies to hospital disaster preparedness. In his white paper “Hospital Disaster Medical Response: Aligning Everyday Requirements with Emergency Casualty Care,” Dr. Farmer says, “ … we are witnessing the rapid development and emergence of medical emergency teams, or rapid response teams within the hospital. … These teams are intended to monitor inpatients and intervene before physiological deterioration supervenes. One might ask, in the event of a medical disaster, could these teams be repurposed for sophisticated casualty care and ICU expansion? We think it is logical that these types of critical care ‘outreach’ teams, in conjunction with noncritical care hospital personnel, could be leveraged as an effective strategy to extend ICU capabilities during a disaster.”
Having a complete team of ICU providers address each patient’s needs will vastly improve quality of care, but these teams must have some guidelines to follow in order to ensure that they work at maximum efficiency.
Critical Care Guidelines: An Integral Component
Critical care experts shy away from such buzzwords and phrases as “standardization of care” in regard to ICU practices, but they do agree that universal guidelines will be the norm in the future.
“We’ll see the development of drastically improved outcomes, and reduction in harm through reliable processes,” says Dr. Rainey. “We can see, for example, that five things need to be done to every ventilated patient. With development of reliable processes in place, we can see that we will close the gap between intent and actual execution.”
Dr. Farmer agrees. “We do clinical guidelines for everyday issues, so I don’t see why we can’t do the same thing” for critical care and disaster preparedness.
Critical care is ripe for integrating clinical practice guidelines. “There are certain types of interventions that are near universal in ICUs,” says Dr. Buchman. “How we sedate patients, how we relieve pain, how we liberate someone from mechanical support … having touchstones or guidelines for these interventions will help. This is complementary to standardization of care.
“Here’s an example: A patient is admitted with a myocardial infarction. We would treat him with beta-blockers, nitrates, heparin, and aspirin. We don’t think of a standard dose of beta-blockers because the dose must be titrated to [have an] effect on the individual patient,” he continues. “How this individualization is done safely involves organizational guidelines. Systematic implementation of such guidelines will be the difference between good ICUs and great ICUs. The implementation is a continuous four-step process—learn the recommendations, deliver the care, measure the outcomes, and find ways to improve.”
Hospitalists and Critical Care
In concert with technologic advancement and improved guidelines, one major solution to the staffing shortage is hospitalists. According to Dr. Farmer, a large portion of critical care services across the country is provided by family practitioners and general internists. The demographics of the population, combined with the current system of training, ensure inadequate staffing. That shortage could be filled by hospitalists. For many hospitalists ICU care is already an important and satisfying arm of their practice. It may become necessary in the future to define skill sets to work in critical care areas. Hospitalists are well positioned to fill that need.
Looking Ahead
The area of critical care may be moving more quickly toward the future than other hospital functions because it must do so in order to continue to work at all. The success of achieving a future of quality care, patient safety, and adequate staffing rests on a different approach with providers and technology.
“We have to learn to work smarter to leverage new technology and the expertise of all other experts in other fields,” says Dr. Buchman of the future of critical care.TH
Chicago-based Jane Jerrard will write future installments of this series.
FLASHBACK:
An Ill Wind
An 1883 tornado strikes a familiar chord in today’s hurricane-ridden times
“An ill wind”—these were the opening words spoken by William Worrall, MD, at the official opening ceremony for St. Mary’s Hospital in Rochester, Minn. The hospital had been conceived following the destruction wrought on Rochester by a tornado that had left 37 dead and more than 200 injured six years earlier.
Aug. 12, 1883, was a particularly hot day, and many residents must have been hopeful of relief as they saw black clouds looming to the west late that evening. That evening Dr. William Mayo’s sons, Will and Charlie, were headed to the slaughterhouse northwest of town in the part of Rochester then known as the Lower Town to purchase a sheep’s head for eye dissections. The butchers had closed early because of the impending storm and advised the young Mayos to head back posthaste.
The cyclone descended just as they crossed a bridge, which was torn loose of its moorings, over the Zumbro River. They witnessed buildings smashed to bits, a grain elevator toppled, and railroad cars wrecked by the destructive force. They were almost killed by a heavy cornice that had ripped off the Cook House and smashed into their buggy. The Cook House was adjacent to the Cook Block that housed the offices of the Doctors Mayo. Though their buggy was destroyed, they survived and took shelter with their horse in a blacksmith’s shop.
They survived the storm, but others were not so lucky. One-third of the buildings in town were destroyed or damaged with more than half in Lower Town, a predominantly working class neighborhood. They immediately began to care for the wounded brought to the clinic offices. Their father had taken charge of relief efforts in Lower Town, the worst hit part of the city. Victims were brought to a local hotel, where they were quickly triaged and treated according to need.
The physicians in town shared a common goal though they were not always united in their methods. The routine use of an emetic for all trauma patients was advocated by one physician to the opprobrium of the elder Dr. Mayo, who quickly insisted on establishment of clear leadership. He also recruited the assistance of Sister Alfred Moes, who had offered her convent to shelter the sick and homeless and her nuns as nurses for the injured.
The anti-Catholic prejudices of the day necessitated Dr. W. Mayo asking that it be announced that Sister Alfred was offering shelter in her “house” and not in a convent. Other relief efforts such as offering food and provisions to the needy were established in available rooms across town. Recovery of bodies, funeral services, and burials were quickly conducted. Rebuilding efforts were speedily begun with fundraising activities bringing in enough funds to feed and clothe hundreds, rebuild more than 100 houses, and provide money for furniture.
The tornado had highlighted the need for a hospital in Rochester and Sister Alfred ultimately requested that Dr. W. Mayo assist in this venture. The Sisters of Saint Francis raised money and built Saint Mary’s Hospital—the first in Rochester.
The destruction and chaos caused by Hurricane Katrina has brought much pain to our nation. In the early aftermath there appeared to be a dearth of leadership, and questions arose regarding an apparent lack of preparedness and poor response to the carnage caused by the storm. Undoubtedly there will be many investigations into what went wrong. History may help answer these questions, but should also provide reassurance that good can come out of the debris of an ill wind.
—Jamie Newman, MD, FACP, and Adeboye B. Ogunseitan, MD
Moving Out
This article is the second in a series on the hospital of the future, designed to get our readers thinking and planning ahead for their own facilities.
Hospitals across the country wrestle with improving their discharge process, whether the goal is gaining a more time- and cost-effective outcome for the facility, or improving quality measures for patients upon departure, or both.
“A lot of people are attacking discharge problems from a lot of different angles,” says Vineet Arora, MD, academic hospitalist and researcher, University of Chicago Pritzker School of Medicine.
What will hospital discharge look like in the future? Based on current research, trials, and trends, it seems there are few surprises down the road in this area. The changes will come in the form of fine-tuning critical areas in the process rather than implementing new technology to radically change the way we release patients. Positive changes seem to be people-based rather than computer-based.
“Everybody’s on the technology bandwagon, but we have to understand the processes first,” says Lakshmi Halasyamani, MD, associate chair for the Department of Internal Medicine, St. Joseph Mercy Hospital, Ann Arbor, Mich. “Better technology won’t make care safer or more efficient. We have to examine how we organize care delivery, then look at technology. Otherwise it replicates the inefficiencies we have now.”
Here are some predictions for how the discharge process will be improved in the hospital of the future.
THE DISCHARGE PROCESS WILL BE SMOOTHER AND SAFER
Most hospital-based professionals agree that discharge is an area of care that needs more attention.
“Every day that you’re [in the hospital], we spend a little less time with you,” says Dr. Halasyamani. “We undervalue the risk of discharging patients; we need to focus on [the patients] more. The nurse calls us, and we get the discharge done as quickly as possible.”
In the hospital of the future, the discharge process will be driven by specific structured guidelines that ensure patients safety when they leave the hospital. Every discharge will involve a multidisciplinary team, with members signing off that the patient is not only ready to leave the hospital, but informed about their condition and any next steps, and has necessary medications or prescriptions in hand.
As for improving efficiency, minor changes can make a big difference. Chad Whelan, MD, assistant professor of medicine, University of Chicago Hospitals, is part of a task force working on how to move hospital discharges earlier in the day.
“An earlier discharge is better for everyone, including the patient—especially if they’re being transferred to another facility,” he points out. “One thing we’re looking at is the way diagnostic tests are categorized. Everything falls into two categories now: emergency diagnostics and everything else.”
Dr. Whelan and the taskforce have asked departments, including radiology and other labs, to create a third category: for patients waiting for a test before they can be discharged. All it takes is one question on the part of the service provider: “Is this patient waiting for these results before she can go home?” to move that patient to the front of the line.
Another recommendation Dr. Whelan’s task force will make involves staffing up. “Like we ramp nursing staff up and down depending on the census, we are looking at doing that with case managers and ward clerks to handle heavy discharge times,” he says.
David J. Rosenman, MD, senior associate consultant, Hospital Internal Medicine, Mayo Clinic in Rochester, Minn., suggests that paperwork might also be changed. “The discharge summary of the future will be more visual,” he predicts. “There are ways of displaying information that are more sophisticated and probably more helpful than static lists and linear prose alone.”
EMPOWERED PATIENTS
One change we are likely to see is patients taking on the responsibility of their own medical information. Ideally, the patients themselves will make caring for—and discharging—them easier and more efficient by sharing complete information on their current medications and other healthcare details that are often forgotten or overlooked by a provider or caregiver.
“The future of discharge lies with our ability to arm patients with their own information,” says Dr. Arora. “The more empowered the patient is, the better the outcome.” Personal health records (PHRs) are one solution. MyPHR is one online product, offered free by the American Health Information Management Association (AHIMA). Roughly 30 companies currently offer paid subscription PHR services to consumers. Peoplechart Corporation (San Francisco) is one of them and provides a single source of information controlled by the patient.
“We’re a pioneer of the PHR idea,” says Megan Mok, president and founder, Peoplechart Corporation. “There are not that many out there.”
Healthcare consumers can subscribe to a variety of Peoplechart tools and services (including initial collection of their records) that allow them to gain access to their comprehensive medical records via the Internet—or phone, if they choose—and to grant any given healthcare provider access to part or all of their records.
“Everything is patient-initiated and patient-controlled,” explains Mok. “There’s a big difference from systems controlled by providers, which may allow patients access, but not ownership.”
PHRs typically offer a comprehensive, integrated overview of an individual’s health data, including information that individuals add themselves on their symptoms and prescriptions, along with information such as diagnoses and lab results. Once a discharged patient updates her PHR, she can share her complete hospital records with her primary care physician, physical therapist, rehab facility, or whatever caregiver requires the information. This will save time and effort for all healthcare providers, and, more importantly, ensures that essential information is available.
Regardless of whether a patient has a PHR, physicians and other staff must ensure that the individual leaves the hospital with complete information on their care and medications.
“Discharge is a quality measure,” says Dr. Arora. “We need a multidisciplinary approach to address what each patient needs to go home.”
DEMYSTIFIED MEDICATIONS
In the very near future, the 2006 JCAHO standard for medication reconciliation will eliminate many problems with medications after discharge.
“This standard is extremely important,” says Dr. Rosenman. “Almost half of medication errors occur at transition points in a patient’s care. Reconciling medication lists—especially at these points—is critical to ensuring patient safety.”
The medication reconciliation form could conceivably morph into something broader in the future. “It would be nice for the medical record to be a living document that evolved with each encounter over the course of a patient’s life,” says Dr. Rosenman. “People may someday carry replaceable, updatable, credit-card-like medical cards or chips. In the meantime, we need to do our very best to keep medication lists and related data accurate and complete.”
While the patient will own his or her medical information, “the burden for ensuring the med list is accurate falls entirely on the healthcare organization,” insists Dr. Halasyamani. “This is a ripe opportunity to partner with the patients themselves. They and their families own the information. We have to help patients be stakeholders and give them the tools to manage their ever-changing medications and their healthcare.”
Many paper-based and computerized tools exist now, but there is no obvious standout product or method physicians can provide to patients that will ensure they take their prescriptions correctly on an ongoing basis.
“Health systems will have to develop a standard” for helping patients manage their medications, says Dr. Halasyamani. “Strategies must be low-tech but get the job done. They must resonate with things that patients already do, like paying bills.”

COMMUNICATION STILL CRITICAL
One step in the discharge process that ensures a smooth transition for inpatient to outpatient is communication with the professionals, facilities, or caregivers who will take over the patient’s care.
“The gap in care after discharge puts patients at risk for adverse events,” warns Dr. Arora. “One reason for this vulnerable gap is the flow of information between settings and teams of providers.” In the future, hospitals will better manage this essential transfer of information.
Typically, the patient’s primary care physician wants information from the hospital at admission and at discharge, and, if the primary care physician wishes, in between.
“We need to improve communications with primary care physicians in a way that respects their wishes for communication,” says Dr. Arora. The UCSF Hospitalist Group is already working on this.
“Until recently, we provided fax copies of our notes to primary care physicians. Now we have a new dictation system,” says Steven Pantilat, MD, FACP, SHM president. “We did a survey that found that most physicians want telephone contact at admission and at discharge, plus any major occurrences in between. The ability to exchange information in real time is important—and e-mail is not realtime.”
How does a hospitalist keep track of everyone’s communication preferences? “The hospitalist simply has to figure out what each primary care physician wants,” stresses Dr. Pantilat. “My sense is that in any hospital, there is a limited number of doctors or practices to deal with. How do you keep them all straight? Well, the same way a hospitalist keeps all the various nurses straight—you just do. It’s your business.”
PLANNED FOLLOW-UP
In the future, nearly every discharged patient will be contacted within two or three days by the hospitalist or another hospital medical staff. This may come in the form of a phone call to the patient to check on their overall health, symptoms, and medications. Or it may be a more hands-on approach.
The UCSF Medical Center has established a follow-up service to provide care to patients during the transition period immediately following discharge.
“This service was designed for patients who couldn’t otherwise be followed up on or those who would benefit from seeing the doctor who treated them in the hospital,” explains Dr. Pantilat, who initiated the idea for the service. “For example, if a patient with DVT was discharged, is the swelling smaller? The primary care physician can’t say—he didn’t see it.”
Out of more than 2,600 discharges during 1997-1998, the first year that the follow-up service existed, only 47 patients were prescribed with follow-up visits. “It was never meant to be a highly utilized service,” says Dr. Pantilat, “but to be a highly expandable, flexible service that addresses the needs of specific patients.” Of those 47 patients, four were readmitted to the hospital—one directly from the follow-up visit—compared with a national readmission average of 14%.
“We see these patients in the ED,” says Dr. Pantilat. “It’s the only department that’s open 24/7, and the ED has some extra bed capacity.”
When the hospitalist feels a follow-up is necessary, he or she schedules a visit with the patient before discharge for midmorning one or two days after discharge. (Midmorning is typically a slow time in the emergency department.) He then faxes the appointment information to the emergency department, so that when the patient shows up, she is preregistered. The emergency department telephones the hospitalist when the patient arrives, and that doctor then comes down to see the patient. The emergency department physicians have nothing to do with these follow-ups, though the nursing staff might be asked to help. Also, follow-up visits are considered an outpatient service and charged as such. “The follow-up service was established and run at virtually no cost,” says Dr. Pantilat.
Even if every hospital doesn’t arrange in-person follow-ups, there will be some form of contact after discharge. “Hospitals providing care in transition will expand a lot,” he explains, “whether it’s phone calls from a nurse or other healthcare professional or some other contact during that gap until a patient can re-establish with their primary care physician. Not every patient needs this, but a lot would benefit.”
THE HOSPITALIST ROLE IN DISCHARGE
As we move toward creating a better discharge process, hospitalists will be at the center of that change and the process itself.
“The hospitalist is the keeper of information,” says Dr. Arora. “They know why certain care decisions were made. This movement depends on the flow of information to help design systems to help implement communication.”
There are some barriers to a smooth discharge process that only hospitalists can eliminate. “The increased use of hospitalists means that patients are not familiar with their doctor” in the hospital, says Dr. Arora. “When they leave the hospital, some information stays behind. They don’t know who to call for that follow-up lab work prescribed in the hospital. … The hospitalist needs to do a better job of telling patients who they are and how to reach them after discharge. A systems-based solution, or solutions, is needed.”
It is up to hospitalists to ensure that their discharge system works, that each patient leaves with an understanding of next steps in their care and knows who to call for which specific follow-up step, and with contact information if they (or their primary care physician) need to reach their hospitalist.
Dr. Halasyamani believes that hospitalists are well positioned to implement change in general within their systems. “The hospitalist is in the trenches, in a position to see what changes have to take place,” she says. “It’s their role to inform their management of better processes.
Each of us needs to be a waver of the banner for new standards—it’s not good enough to just scribble prescriptions”
CONCLUSION
The future is coming fast, for improved hospital discharge as well as other everyday processes. “We’re learning that discharge should be a more structured, formal process,” says Dr. Whelan. “We’d like to move to a safer, more complete and more efficient way of handling it.”
Consider what your own facility is doing regarding discharging patients. If there is room for improvement, can you envision a way to bring that process into the future? TH
Jane Jerrard will continue writing the “Hospital of the Future” series this fall.
Flashback:
Colonial Hospitalists
250 years of admissions and discharge

The hospital-based physician must deal with many arcane and Byzantine criteria for admission, care, and discharge of patients. There are regulations for record-keeping and concerns about length of stay. Becoming a staff member may involve physician credentialing, and practitioners from other states or countries have to meet more rigorous standards.
This previous paragraph was not written about modern-day America. These issues are lifted from the “Rules and Regulations of the Pennsylvania Hospital” approved by the Board of Managers in 1752.1 The Pennsylvania Hospital was founded that year under the guidance of Benjamin Franklin. The facility was dedicated to care for the sick and poor. Among the biggest obstacles to its creation was fundraising. Franklin’s accounts of the early years of this institution included a final page with a useful form for donating money.
ADMISSION AND DISCHARGE CRITERIA
In 1752 there were 15 rules for admission and discharge of patients, as well as regulations for patients’ behavior while hospitalized. Among the most interesting:
- No patients can be admitted if deemed incurable, lunaticks [sic] excepted, nor any case not requiring special services of a hospital.
- No admits for smallpox, itch, or other infectious distempers unless proper apartments [isolation] available. Admits found to have the above will be discharged.
- No admits of women with small children. Hospital will not maintain childcare facilities.
- Persons admitted as above must provide funds for their own burial in case of their own demise.
- 5. One bed to be held for a trauma case.
- Patients will be discharged when cured or judged incurable
- All cured patients must sign a release stating their cure and the benefit received from the hospital for use by the hospital managers.
- No patient may leave the facility without a physician release. They may not swear or curse, get drunk, behave rudely or indecently, on pain of expulsion at first admonition.
- No patient may gamble or beg.
- Patients will aide in nursing other patients when able. This will include washing and ironing the linen and cleaning the rooms.
The Hospital Management Board was responsible for choosing a staff of six practitioners to manage these patients. There were guidelines for who could fill this job.
RULES FOR CHOICE OF PHYSICIANS AND SURGEONS
There were the rules in place in 1752 for choosing physicians and surgeons who could work in the hospital; the most interesting was that applying practitioners must be 27 years old, have served an apprenticeship in Philadelphia, have studied “physick” or surgery for seven years or more, and have undergone an exam by six hospital practitioners. Visiting practitioners had to reside in the city for three years before applying and then had to qualify under the same criteria.
LENGTH OF STAY
There was a significant interest in abstracting the admit diagnosis, length of stay, and outcome. The disposition of patients admitted during the first two years of the hospital’s existence, ending in April 1754 was presented in a modern format.
There were 117 admissions, with 60 cures. Eleven patients were relieved, though not cured. Seven were deemed incurable, 10 were taken away by friends, and 10 died. Three were discharged for irregular behavior, and 16 remained hospitalized.
The most common admission diagnosis was ulcers, representing almost a third of all admits, followed by lunacy. Other frequent diagnoses were dropsy (congestive heart disease), scrophulous and scorbutic diseases (extrapulmonary tuberculosis and scurvy) and rheumatism.
The highest mortality was for consumption, at 100%. The two patients admitted with flux (diarrhea) and prolapsus ani also died. Dropsy carried a 33% mortality rate, without the benefit of the latest medical innovation, foxglove (digitalis), which would be described a few decades later.2 Also notable is death from scurvy, the cure for which was described in 1753 by James Lind.3
The managers were pleased with the performance of the facility. They believed that their efforts had resulted in “good” for the 60 persons afflicted with “various distempers” who were cured and that many had received considerable relief. This was accomplished despite the limited amount of funds available, thanks to careful attendance afforded to the sick and poor, as well as proper diet and availability of medicines. Based on these favorable reports, the Board of Managers requested further funding.
Two hundred and fifty years later, physicians face many of the same issues, including admission and discharge criteria, concerns about funding, and practice regulation. Their actions continue to be monitored, and it is likely that the same will be true in the future. Hospital administrators remain frugal, and we are admonished, in the words of Benjamin Franklin, writing in Poor Richard’s Almanac, “A penny saved is a penny earned.”
—Jamie Newman, MD, FACP
REFERENCES
- Franklin B. Some Account of the Pennsylvania Hospital 1754. (Facsimile Edition.) Baltimore: The Johns Hopkins Press; 1954.
- Withering W. An Account of the Foxglove and Some of Its Medical Uses. Birmingham, England: M. Swinney; 1785.
- Lind J. A Treatise of the Scurvy. Edinburgh, Scotland: Sands, Murray and Cochran; 1753.
This article is the second in a series on the hospital of the future, designed to get our readers thinking and planning ahead for their own facilities.
Hospitals across the country wrestle with improving their discharge process, whether the goal is gaining a more time- and cost-effective outcome for the facility, or improving quality measures for patients upon departure, or both.
“A lot of people are attacking discharge problems from a lot of different angles,” says Vineet Arora, MD, academic hospitalist and researcher, University of Chicago Pritzker School of Medicine.
What will hospital discharge look like in the future? Based on current research, trials, and trends, it seems there are few surprises down the road in this area. The changes will come in the form of fine-tuning critical areas in the process rather than implementing new technology to radically change the way we release patients. Positive changes seem to be people-based rather than computer-based.
“Everybody’s on the technology bandwagon, but we have to understand the processes first,” says Lakshmi Halasyamani, MD, associate chair for the Department of Internal Medicine, St. Joseph Mercy Hospital, Ann Arbor, Mich. “Better technology won’t make care safer or more efficient. We have to examine how we organize care delivery, then look at technology. Otherwise it replicates the inefficiencies we have now.”
Here are some predictions for how the discharge process will be improved in the hospital of the future.
THE DISCHARGE PROCESS WILL BE SMOOTHER AND SAFER
Most hospital-based professionals agree that discharge is an area of care that needs more attention.
“Every day that you’re [in the hospital], we spend a little less time with you,” says Dr. Halasyamani. “We undervalue the risk of discharging patients; we need to focus on [the patients] more. The nurse calls us, and we get the discharge done as quickly as possible.”
In the hospital of the future, the discharge process will be driven by specific structured guidelines that ensure patients safety when they leave the hospital. Every discharge will involve a multidisciplinary team, with members signing off that the patient is not only ready to leave the hospital, but informed about their condition and any next steps, and has necessary medications or prescriptions in hand.
As for improving efficiency, minor changes can make a big difference. Chad Whelan, MD, assistant professor of medicine, University of Chicago Hospitals, is part of a task force working on how to move hospital discharges earlier in the day.
“An earlier discharge is better for everyone, including the patient—especially if they’re being transferred to another facility,” he points out. “One thing we’re looking at is the way diagnostic tests are categorized. Everything falls into two categories now: emergency diagnostics and everything else.”
Dr. Whelan and the taskforce have asked departments, including radiology and other labs, to create a third category: for patients waiting for a test before they can be discharged. All it takes is one question on the part of the service provider: “Is this patient waiting for these results before she can go home?” to move that patient to the front of the line.
Another recommendation Dr. Whelan’s task force will make involves staffing up. “Like we ramp nursing staff up and down depending on the census, we are looking at doing that with case managers and ward clerks to handle heavy discharge times,” he says.
David J. Rosenman, MD, senior associate consultant, Hospital Internal Medicine, Mayo Clinic in Rochester, Minn., suggests that paperwork might also be changed. “The discharge summary of the future will be more visual,” he predicts. “There are ways of displaying information that are more sophisticated and probably more helpful than static lists and linear prose alone.”
EMPOWERED PATIENTS
One change we are likely to see is patients taking on the responsibility of their own medical information. Ideally, the patients themselves will make caring for—and discharging—them easier and more efficient by sharing complete information on their current medications and other healthcare details that are often forgotten or overlooked by a provider or caregiver.
“The future of discharge lies with our ability to arm patients with their own information,” says Dr. Arora. “The more empowered the patient is, the better the outcome.” Personal health records (PHRs) are one solution. MyPHR is one online product, offered free by the American Health Information Management Association (AHIMA). Roughly 30 companies currently offer paid subscription PHR services to consumers. Peoplechart Corporation (San Francisco) is one of them and provides a single source of information controlled by the patient.
“We’re a pioneer of the PHR idea,” says Megan Mok, president and founder, Peoplechart Corporation. “There are not that many out there.”
Healthcare consumers can subscribe to a variety of Peoplechart tools and services (including initial collection of their records) that allow them to gain access to their comprehensive medical records via the Internet—or phone, if they choose—and to grant any given healthcare provider access to part or all of their records.
“Everything is patient-initiated and patient-controlled,” explains Mok. “There’s a big difference from systems controlled by providers, which may allow patients access, but not ownership.”
PHRs typically offer a comprehensive, integrated overview of an individual’s health data, including information that individuals add themselves on their symptoms and prescriptions, along with information such as diagnoses and lab results. Once a discharged patient updates her PHR, she can share her complete hospital records with her primary care physician, physical therapist, rehab facility, or whatever caregiver requires the information. This will save time and effort for all healthcare providers, and, more importantly, ensures that essential information is available.
Regardless of whether a patient has a PHR, physicians and other staff must ensure that the individual leaves the hospital with complete information on their care and medications.
“Discharge is a quality measure,” says Dr. Arora. “We need a multidisciplinary approach to address what each patient needs to go home.”
DEMYSTIFIED MEDICATIONS
In the very near future, the 2006 JCAHO standard for medication reconciliation will eliminate many problems with medications after discharge.
“This standard is extremely important,” says Dr. Rosenman. “Almost half of medication errors occur at transition points in a patient’s care. Reconciling medication lists—especially at these points—is critical to ensuring patient safety.”
The medication reconciliation form could conceivably morph into something broader in the future. “It would be nice for the medical record to be a living document that evolved with each encounter over the course of a patient’s life,” says Dr. Rosenman. “People may someday carry replaceable, updatable, credit-card-like medical cards or chips. In the meantime, we need to do our very best to keep medication lists and related data accurate and complete.”
While the patient will own his or her medical information, “the burden for ensuring the med list is accurate falls entirely on the healthcare organization,” insists Dr. Halasyamani. “This is a ripe opportunity to partner with the patients themselves. They and their families own the information. We have to help patients be stakeholders and give them the tools to manage their ever-changing medications and their healthcare.”
Many paper-based and computerized tools exist now, but there is no obvious standout product or method physicians can provide to patients that will ensure they take their prescriptions correctly on an ongoing basis.
“Health systems will have to develop a standard” for helping patients manage their medications, says Dr. Halasyamani. “Strategies must be low-tech but get the job done. They must resonate with things that patients already do, like paying bills.”
COMMUNICATION STILL CRITICAL
One step in the discharge process that ensures a smooth transition for inpatient to outpatient is communication with the professionals, facilities, or caregivers who will take over the patient’s care.
“The gap in care after discharge puts patients at risk for adverse events,” warns Dr. Arora. “One reason for this vulnerable gap is the flow of information between settings and teams of providers.” In the future, hospitals will better manage this essential transfer of information.
Typically, the patient’s primary care physician wants information from the hospital at admission and at discharge, and, if the primary care physician wishes, in between.
“We need to improve communications with primary care physicians in a way that respects their wishes for communication,” says Dr. Arora. The UCSF Hospitalist Group is already working on this.
“Until recently, we provided fax copies of our notes to primary care physicians. Now we have a new dictation system,” says Steven Pantilat, MD, FACP, SHM president. “We did a survey that found that most physicians want telephone contact at admission and at discharge, plus any major occurrences in between. The ability to exchange information in real time is important—and e-mail is not realtime.”
How does a hospitalist keep track of everyone’s communication preferences? “The hospitalist simply has to figure out what each primary care physician wants,” stresses Dr. Pantilat. “My sense is that in any hospital, there is a limited number of doctors or practices to deal with. How do you keep them all straight? Well, the same way a hospitalist keeps all the various nurses straight—you just do. It’s your business.”
PLANNED FOLLOW-UP
In the future, nearly every discharged patient will be contacted within two or three days by the hospitalist or another hospital medical staff. This may come in the form of a phone call to the patient to check on their overall health, symptoms, and medications. Or it may be a more hands-on approach.
The UCSF Medical Center has established a follow-up service to provide care to patients during the transition period immediately following discharge.
“This service was designed for patients who couldn’t otherwise be followed up on or those who would benefit from seeing the doctor who treated them in the hospital,” explains Dr. Pantilat, who initiated the idea for the service. “For example, if a patient with DVT was discharged, is the swelling smaller? The primary care physician can’t say—he didn’t see it.”
Out of more than 2,600 discharges during 1997-1998, the first year that the follow-up service existed, only 47 patients were prescribed with follow-up visits. “It was never meant to be a highly utilized service,” says Dr. Pantilat, “but to be a highly expandable, flexible service that addresses the needs of specific patients.” Of those 47 patients, four were readmitted to the hospital—one directly from the follow-up visit—compared with a national readmission average of 14%.
“We see these patients in the ED,” says Dr. Pantilat. “It’s the only department that’s open 24/7, and the ED has some extra bed capacity.”
When the hospitalist feels a follow-up is necessary, he or she schedules a visit with the patient before discharge for midmorning one or two days after discharge. (Midmorning is typically a slow time in the emergency department.) He then faxes the appointment information to the emergency department, so that when the patient shows up, she is preregistered. The emergency department telephones the hospitalist when the patient arrives, and that doctor then comes down to see the patient. The emergency department physicians have nothing to do with these follow-ups, though the nursing staff might be asked to help. Also, follow-up visits are considered an outpatient service and charged as such. “The follow-up service was established and run at virtually no cost,” says Dr. Pantilat.
Even if every hospital doesn’t arrange in-person follow-ups, there will be some form of contact after discharge. “Hospitals providing care in transition will expand a lot,” he explains, “whether it’s phone calls from a nurse or other healthcare professional or some other contact during that gap until a patient can re-establish with their primary care physician. Not every patient needs this, but a lot would benefit.”
THE HOSPITALIST ROLE IN DISCHARGE
As we move toward creating a better discharge process, hospitalists will be at the center of that change and the process itself.
“The hospitalist is the keeper of information,” says Dr. Arora. “They know why certain care decisions were made. This movement depends on the flow of information to help design systems to help implement communication.”
There are some barriers to a smooth discharge process that only hospitalists can eliminate. “The increased use of hospitalists means that patients are not familiar with their doctor” in the hospital, says Dr. Arora. “When they leave the hospital, some information stays behind. They don’t know who to call for that follow-up lab work prescribed in the hospital. … The hospitalist needs to do a better job of telling patients who they are and how to reach them after discharge. A systems-based solution, or solutions, is needed.”
It is up to hospitalists to ensure that their discharge system works, that each patient leaves with an understanding of next steps in their care and knows who to call for which specific follow-up step, and with contact information if they (or their primary care physician) need to reach their hospitalist.
Dr. Halasyamani believes that hospitalists are well positioned to implement change in general within their systems. “The hospitalist is in the trenches, in a position to see what changes have to take place,” she says. “It’s their role to inform their management of better processes.
Each of us needs to be a waver of the banner for new standards—it’s not good enough to just scribble prescriptions”
CONCLUSION
The future is coming fast, for improved hospital discharge as well as other everyday processes. “We’re learning that discharge should be a more structured, formal process,” says Dr. Whelan. “We’d like to move to a safer, more complete and more efficient way of handling it.”
Consider what your own facility is doing regarding discharging patients. If there is room for improvement, can you envision a way to bring that process into the future? TH
Jane Jerrard will continue writing the “Hospital of the Future” series this fall.
Flashback:
Colonial Hospitalists
250 years of admissions and discharge
The hospital-based physician must deal with many arcane and Byzantine criteria for admission, care, and discharge of patients. There are regulations for record-keeping and concerns about length of stay. Becoming a staff member may involve physician credentialing, and practitioners from other states or countries have to meet more rigorous standards.
This previous paragraph was not written about modern-day America. These issues are lifted from the “Rules and Regulations of the Pennsylvania Hospital” approved by the Board of Managers in 1752.1 The Pennsylvania Hospital was founded that year under the guidance of Benjamin Franklin. The facility was dedicated to care for the sick and poor. Among the biggest obstacles to its creation was fundraising. Franklin’s accounts of the early years of this institution included a final page with a useful form for donating money.
ADMISSION AND DISCHARGE CRITERIA
In 1752 there were 15 rules for admission and discharge of patients, as well as regulations for patients’ behavior while hospitalized. Among the most interesting:
- No patients can be admitted if deemed incurable, lunaticks [sic] excepted, nor any case not requiring special services of a hospital.
- No admits for smallpox, itch, or other infectious distempers unless proper apartments [isolation] available. Admits found to have the above will be discharged.
- No admits of women with small children. Hospital will not maintain childcare facilities.
- Persons admitted as above must provide funds for their own burial in case of their own demise.
- 5. One bed to be held for a trauma case.
- Patients will be discharged when cured or judged incurable
- All cured patients must sign a release stating their cure and the benefit received from the hospital for use by the hospital managers.
- No patient may leave the facility without a physician release. They may not swear or curse, get drunk, behave rudely or indecently, on pain of expulsion at first admonition.
- No patient may gamble or beg.
- Patients will aide in nursing other patients when able. This will include washing and ironing the linen and cleaning the rooms.
The Hospital Management Board was responsible for choosing a staff of six practitioners to manage these patients. There were guidelines for who could fill this job.
RULES FOR CHOICE OF PHYSICIANS AND SURGEONS
There were the rules in place in 1752 for choosing physicians and surgeons who could work in the hospital; the most interesting was that applying practitioners must be 27 years old, have served an apprenticeship in Philadelphia, have studied “physick” or surgery for seven years or more, and have undergone an exam by six hospital practitioners. Visiting practitioners had to reside in the city for three years before applying and then had to qualify under the same criteria.
LENGTH OF STAY
There was a significant interest in abstracting the admit diagnosis, length of stay, and outcome. The disposition of patients admitted during the first two years of the hospital’s existence, ending in April 1754 was presented in a modern format.
There were 117 admissions, with 60 cures. Eleven patients were relieved, though not cured. Seven were deemed incurable, 10 were taken away by friends, and 10 died. Three were discharged for irregular behavior, and 16 remained hospitalized.
The most common admission diagnosis was ulcers, representing almost a third of all admits, followed by lunacy. Other frequent diagnoses were dropsy (congestive heart disease), scrophulous and scorbutic diseases (extrapulmonary tuberculosis and scurvy) and rheumatism.
The highest mortality was for consumption, at 100%. The two patients admitted with flux (diarrhea) and prolapsus ani also died. Dropsy carried a 33% mortality rate, without the benefit of the latest medical innovation, foxglove (digitalis), which would be described a few decades later.2 Also notable is death from scurvy, the cure for which was described in 1753 by James Lind.3
The managers were pleased with the performance of the facility. They believed that their efforts had resulted in “good” for the 60 persons afflicted with “various distempers” who were cured and that many had received considerable relief. This was accomplished despite the limited amount of funds available, thanks to careful attendance afforded to the sick and poor, as well as proper diet and availability of medicines. Based on these favorable reports, the Board of Managers requested further funding.
Two hundred and fifty years later, physicians face many of the same issues, including admission and discharge criteria, concerns about funding, and practice regulation. Their actions continue to be monitored, and it is likely that the same will be true in the future. Hospital administrators remain frugal, and we are admonished, in the words of Benjamin Franklin, writing in Poor Richard’s Almanac, “A penny saved is a penny earned.”
—Jamie Newman, MD, FACP
REFERENCES
- Franklin B. Some Account of the Pennsylvania Hospital 1754. (Facsimile Edition.) Baltimore: The Johns Hopkins Press; 1954.
- Withering W. An Account of the Foxglove and Some of Its Medical Uses. Birmingham, England: M. Swinney; 1785.
- Lind J. A Treatise of the Scurvy. Edinburgh, Scotland: Sands, Murray and Cochran; 1753.
This article is the second in a series on the hospital of the future, designed to get our readers thinking and planning ahead for their own facilities.
Hospitals across the country wrestle with improving their discharge process, whether the goal is gaining a more time- and cost-effective outcome for the facility, or improving quality measures for patients upon departure, or both.
“A lot of people are attacking discharge problems from a lot of different angles,” says Vineet Arora, MD, academic hospitalist and researcher, University of Chicago Pritzker School of Medicine.
What will hospital discharge look like in the future? Based on current research, trials, and trends, it seems there are few surprises down the road in this area. The changes will come in the form of fine-tuning critical areas in the process rather than implementing new technology to radically change the way we release patients. Positive changes seem to be people-based rather than computer-based.
“Everybody’s on the technology bandwagon, but we have to understand the processes first,” says Lakshmi Halasyamani, MD, associate chair for the Department of Internal Medicine, St. Joseph Mercy Hospital, Ann Arbor, Mich. “Better technology won’t make care safer or more efficient. We have to examine how we organize care delivery, then look at technology. Otherwise it replicates the inefficiencies we have now.”
Here are some predictions for how the discharge process will be improved in the hospital of the future.
THE DISCHARGE PROCESS WILL BE SMOOTHER AND SAFER
Most hospital-based professionals agree that discharge is an area of care that needs more attention.
“Every day that you’re [in the hospital], we spend a little less time with you,” says Dr. Halasyamani. “We undervalue the risk of discharging patients; we need to focus on [the patients] more. The nurse calls us, and we get the discharge done as quickly as possible.”
In the hospital of the future, the discharge process will be driven by specific structured guidelines that ensure patients safety when they leave the hospital. Every discharge will involve a multidisciplinary team, with members signing off that the patient is not only ready to leave the hospital, but informed about their condition and any next steps, and has necessary medications or prescriptions in hand.
As for improving efficiency, minor changes can make a big difference. Chad Whelan, MD, assistant professor of medicine, University of Chicago Hospitals, is part of a task force working on how to move hospital discharges earlier in the day.
“An earlier discharge is better for everyone, including the patient—especially if they’re being transferred to another facility,” he points out. “One thing we’re looking at is the way diagnostic tests are categorized. Everything falls into two categories now: emergency diagnostics and everything else.”
Dr. Whelan and the taskforce have asked departments, including radiology and other labs, to create a third category: for patients waiting for a test before they can be discharged. All it takes is one question on the part of the service provider: “Is this patient waiting for these results before she can go home?” to move that patient to the front of the line.
Another recommendation Dr. Whelan’s task force will make involves staffing up. “Like we ramp nursing staff up and down depending on the census, we are looking at doing that with case managers and ward clerks to handle heavy discharge times,” he says.
David J. Rosenman, MD, senior associate consultant, Hospital Internal Medicine, Mayo Clinic in Rochester, Minn., suggests that paperwork might also be changed. “The discharge summary of the future will be more visual,” he predicts. “There are ways of displaying information that are more sophisticated and probably more helpful than static lists and linear prose alone.”
EMPOWERED PATIENTS
One change we are likely to see is patients taking on the responsibility of their own medical information. Ideally, the patients themselves will make caring for—and discharging—them easier and more efficient by sharing complete information on their current medications and other healthcare details that are often forgotten or overlooked by a provider or caregiver.
“The future of discharge lies with our ability to arm patients with their own information,” says Dr. Arora. “The more empowered the patient is, the better the outcome.” Personal health records (PHRs) are one solution. MyPHR is one online product, offered free by the American Health Information Management Association (AHIMA). Roughly 30 companies currently offer paid subscription PHR services to consumers. Peoplechart Corporation (San Francisco) is one of them and provides a single source of information controlled by the patient.
“We’re a pioneer of the PHR idea,” says Megan Mok, president and founder, Peoplechart Corporation. “There are not that many out there.”
Healthcare consumers can subscribe to a variety of Peoplechart tools and services (including initial collection of their records) that allow them to gain access to their comprehensive medical records via the Internet—or phone, if they choose—and to grant any given healthcare provider access to part or all of their records.
“Everything is patient-initiated and patient-controlled,” explains Mok. “There’s a big difference from systems controlled by providers, which may allow patients access, but not ownership.”
PHRs typically offer a comprehensive, integrated overview of an individual’s health data, including information that individuals add themselves on their symptoms and prescriptions, along with information such as diagnoses and lab results. Once a discharged patient updates her PHR, she can share her complete hospital records with her primary care physician, physical therapist, rehab facility, or whatever caregiver requires the information. This will save time and effort for all healthcare providers, and, more importantly, ensures that essential information is available.
Regardless of whether a patient has a PHR, physicians and other staff must ensure that the individual leaves the hospital with complete information on their care and medications.
“Discharge is a quality measure,” says Dr. Arora. “We need a multidisciplinary approach to address what each patient needs to go home.”
DEMYSTIFIED MEDICATIONS
In the very near future, the 2006 JCAHO standard for medication reconciliation will eliminate many problems with medications after discharge.
“This standard is extremely important,” says Dr. Rosenman. “Almost half of medication errors occur at transition points in a patient’s care. Reconciling medication lists—especially at these points—is critical to ensuring patient safety.”
The medication reconciliation form could conceivably morph into something broader in the future. “It would be nice for the medical record to be a living document that evolved with each encounter over the course of a patient’s life,” says Dr. Rosenman. “People may someday carry replaceable, updatable, credit-card-like medical cards or chips. In the meantime, we need to do our very best to keep medication lists and related data accurate and complete.”
While the patient will own his or her medical information, “the burden for ensuring the med list is accurate falls entirely on the healthcare organization,” insists Dr. Halasyamani. “This is a ripe opportunity to partner with the patients themselves. They and their families own the information. We have to help patients be stakeholders and give them the tools to manage their ever-changing medications and their healthcare.”
Many paper-based and computerized tools exist now, but there is no obvious standout product or method physicians can provide to patients that will ensure they take their prescriptions correctly on an ongoing basis.
“Health systems will have to develop a standard” for helping patients manage their medications, says Dr. Halasyamani. “Strategies must be low-tech but get the job done. They must resonate with things that patients already do, like paying bills.”
COMMUNICATION STILL CRITICAL
One step in the discharge process that ensures a smooth transition for inpatient to outpatient is communication with the professionals, facilities, or caregivers who will take over the patient’s care.
“The gap in care after discharge puts patients at risk for adverse events,” warns Dr. Arora. “One reason for this vulnerable gap is the flow of information between settings and teams of providers.” In the future, hospitals will better manage this essential transfer of information.
Typically, the patient’s primary care physician wants information from the hospital at admission and at discharge, and, if the primary care physician wishes, in between.
“We need to improve communications with primary care physicians in a way that respects their wishes for communication,” says Dr. Arora. The UCSF Hospitalist Group is already working on this.
“Until recently, we provided fax copies of our notes to primary care physicians. Now we have a new dictation system,” says Steven Pantilat, MD, FACP, SHM president. “We did a survey that found that most physicians want telephone contact at admission and at discharge, plus any major occurrences in between. The ability to exchange information in real time is important—and e-mail is not realtime.”
How does a hospitalist keep track of everyone’s communication preferences? “The hospitalist simply has to figure out what each primary care physician wants,” stresses Dr. Pantilat. “My sense is that in any hospital, there is a limited number of doctors or practices to deal with. How do you keep them all straight? Well, the same way a hospitalist keeps all the various nurses straight—you just do. It’s your business.”
PLANNED FOLLOW-UP
In the future, nearly every discharged patient will be contacted within two or three days by the hospitalist or another hospital medical staff. This may come in the form of a phone call to the patient to check on their overall health, symptoms, and medications. Or it may be a more hands-on approach.
The UCSF Medical Center has established a follow-up service to provide care to patients during the transition period immediately following discharge.
“This service was designed for patients who couldn’t otherwise be followed up on or those who would benefit from seeing the doctor who treated them in the hospital,” explains Dr. Pantilat, who initiated the idea for the service. “For example, if a patient with DVT was discharged, is the swelling smaller? The primary care physician can’t say—he didn’t see it.”
Out of more than 2,600 discharges during 1997-1998, the first year that the follow-up service existed, only 47 patients were prescribed with follow-up visits. “It was never meant to be a highly utilized service,” says Dr. Pantilat, “but to be a highly expandable, flexible service that addresses the needs of specific patients.” Of those 47 patients, four were readmitted to the hospital—one directly from the follow-up visit—compared with a national readmission average of 14%.
“We see these patients in the ED,” says Dr. Pantilat. “It’s the only department that’s open 24/7, and the ED has some extra bed capacity.”
When the hospitalist feels a follow-up is necessary, he or she schedules a visit with the patient before discharge for midmorning one or two days after discharge. (Midmorning is typically a slow time in the emergency department.) He then faxes the appointment information to the emergency department, so that when the patient shows up, she is preregistered. The emergency department telephones the hospitalist when the patient arrives, and that doctor then comes down to see the patient. The emergency department physicians have nothing to do with these follow-ups, though the nursing staff might be asked to help. Also, follow-up visits are considered an outpatient service and charged as such. “The follow-up service was established and run at virtually no cost,” says Dr. Pantilat.
Even if every hospital doesn’t arrange in-person follow-ups, there will be some form of contact after discharge. “Hospitals providing care in transition will expand a lot,” he explains, “whether it’s phone calls from a nurse or other healthcare professional or some other contact during that gap until a patient can re-establish with their primary care physician. Not every patient needs this, but a lot would benefit.”
THE HOSPITALIST ROLE IN DISCHARGE
As we move toward creating a better discharge process, hospitalists will be at the center of that change and the process itself.
“The hospitalist is the keeper of information,” says Dr. Arora. “They know why certain care decisions were made. This movement depends on the flow of information to help design systems to help implement communication.”
There are some barriers to a smooth discharge process that only hospitalists can eliminate. “The increased use of hospitalists means that patients are not familiar with their doctor” in the hospital, says Dr. Arora. “When they leave the hospital, some information stays behind. They don’t know who to call for that follow-up lab work prescribed in the hospital. … The hospitalist needs to do a better job of telling patients who they are and how to reach them after discharge. A systems-based solution, or solutions, is needed.”
It is up to hospitalists to ensure that their discharge system works, that each patient leaves with an understanding of next steps in their care and knows who to call for which specific follow-up step, and with contact information if they (or their primary care physician) need to reach their hospitalist.
Dr. Halasyamani believes that hospitalists are well positioned to implement change in general within their systems. “The hospitalist is in the trenches, in a position to see what changes have to take place,” she says. “It’s their role to inform their management of better processes.
Each of us needs to be a waver of the banner for new standards—it’s not good enough to just scribble prescriptions”
CONCLUSION
The future is coming fast, for improved hospital discharge as well as other everyday processes. “We’re learning that discharge should be a more structured, formal process,” says Dr. Whelan. “We’d like to move to a safer, more complete and more efficient way of handling it.”
Consider what your own facility is doing regarding discharging patients. If there is room for improvement, can you envision a way to bring that process into the future? TH
Jane Jerrard will continue writing the “Hospital of the Future” series this fall.
Flashback:
Colonial Hospitalists
250 years of admissions and discharge
The hospital-based physician must deal with many arcane and Byzantine criteria for admission, care, and discharge of patients. There are regulations for record-keeping and concerns about length of stay. Becoming a staff member may involve physician credentialing, and practitioners from other states or countries have to meet more rigorous standards.
This previous paragraph was not written about modern-day America. These issues are lifted from the “Rules and Regulations of the Pennsylvania Hospital” approved by the Board of Managers in 1752.1 The Pennsylvania Hospital was founded that year under the guidance of Benjamin Franklin. The facility was dedicated to care for the sick and poor. Among the biggest obstacles to its creation was fundraising. Franklin’s accounts of the early years of this institution included a final page with a useful form for donating money.
ADMISSION AND DISCHARGE CRITERIA
In 1752 there were 15 rules for admission and discharge of patients, as well as regulations for patients’ behavior while hospitalized. Among the most interesting:
- No patients can be admitted if deemed incurable, lunaticks [sic] excepted, nor any case not requiring special services of a hospital.
- No admits for smallpox, itch, or other infectious distempers unless proper apartments [isolation] available. Admits found to have the above will be discharged.
- No admits of women with small children. Hospital will not maintain childcare facilities.
- Persons admitted as above must provide funds for their own burial in case of their own demise.
- 5. One bed to be held for a trauma case.
- Patients will be discharged when cured or judged incurable
- All cured patients must sign a release stating their cure and the benefit received from the hospital for use by the hospital managers.
- No patient may leave the facility without a physician release. They may not swear or curse, get drunk, behave rudely or indecently, on pain of expulsion at first admonition.
- No patient may gamble or beg.
- Patients will aide in nursing other patients when able. This will include washing and ironing the linen and cleaning the rooms.
The Hospital Management Board was responsible for choosing a staff of six practitioners to manage these patients. There were guidelines for who could fill this job.
RULES FOR CHOICE OF PHYSICIANS AND SURGEONS
There were the rules in place in 1752 for choosing physicians and surgeons who could work in the hospital; the most interesting was that applying practitioners must be 27 years old, have served an apprenticeship in Philadelphia, have studied “physick” or surgery for seven years or more, and have undergone an exam by six hospital practitioners. Visiting practitioners had to reside in the city for three years before applying and then had to qualify under the same criteria.
LENGTH OF STAY
There was a significant interest in abstracting the admit diagnosis, length of stay, and outcome. The disposition of patients admitted during the first two years of the hospital’s existence, ending in April 1754 was presented in a modern format.
There were 117 admissions, with 60 cures. Eleven patients were relieved, though not cured. Seven were deemed incurable, 10 were taken away by friends, and 10 died. Three were discharged for irregular behavior, and 16 remained hospitalized.
The most common admission diagnosis was ulcers, representing almost a third of all admits, followed by lunacy. Other frequent diagnoses were dropsy (congestive heart disease), scrophulous and scorbutic diseases (extrapulmonary tuberculosis and scurvy) and rheumatism.
The highest mortality was for consumption, at 100%. The two patients admitted with flux (diarrhea) and prolapsus ani also died. Dropsy carried a 33% mortality rate, without the benefit of the latest medical innovation, foxglove (digitalis), which would be described a few decades later.2 Also notable is death from scurvy, the cure for which was described in 1753 by James Lind.3
The managers were pleased with the performance of the facility. They believed that their efforts had resulted in “good” for the 60 persons afflicted with “various distempers” who were cured and that many had received considerable relief. This was accomplished despite the limited amount of funds available, thanks to careful attendance afforded to the sick and poor, as well as proper diet and availability of medicines. Based on these favorable reports, the Board of Managers requested further funding.
Two hundred and fifty years later, physicians face many of the same issues, including admission and discharge criteria, concerns about funding, and practice regulation. Their actions continue to be monitored, and it is likely that the same will be true in the future. Hospital administrators remain frugal, and we are admonished, in the words of Benjamin Franklin, writing in Poor Richard’s Almanac, “A penny saved is a penny earned.”
—Jamie Newman, MD, FACP
REFERENCES
- Franklin B. Some Account of the Pennsylvania Hospital 1754. (Facsimile Edition.) Baltimore: The Johns Hopkins Press; 1954.
- Withering W. An Account of the Foxglove and Some of Its Medical Uses. Birmingham, England: M. Swinney; 1785.
- Lind J. A Treatise of the Scurvy. Edinburgh, Scotland: Sands, Murray and Cochran; 1753.
The Hospital of the Future
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
What will the hospital of the future look like? How will it function differently than it does today? What will the patient’s experience be like? What role will hospitalists play?
Imagining the hospital of the future may be an exercise in idealism for many of us, but specialists around the world are currently at work redesigning and improving many different components of the modern hospital, from changing how medical professionals work together to introducing new technologies such as “smart clothing” that house a patient’s medication history and needs.
What’s more, hospital-centric organizations, experts, and participants are moving ahead with new approaches, theories, and technology. As time passes, we’ll see which ideas and theories shake out as the best and most practical.
—Larry Wellikson, MD, FACP
What a Hospital will Look Like
The Hospitalist began focusing on what the future will look like earlier this year. “The vision of a re-engineered hospital with patient-centered care, delivered by a fully empowered team of professionals, which is data- driven with clear quality measurements, where better performance is rewarded by better compensation, is coming to a hospital near you during your professional career,” wrote SHM CEO Larry Wellikson, MD, FACP, in our March/April 2005 issue.1
Dr. Wellikson then pointed out that “the current system is primarily physician-centered and driven by increasing units of activity rather than how well the job is done. … In order to change this complex system many institutions will need to be overhauled. The physical plant of the hospital may need to change … .”
Other healthcare professionals have specific dreams or goals for the future. Robin Orr, MPH, president of The Robin Orr Group, Tiburon, Calif., works with healthcare organizations to affect patient-centered care.
“You have to look at an entire culture to truly affect lasting change,” she explains. “This change will encompass the physical environment of the hospital, the patient’s access to information, and, of course, the human side—everyone from doctors to the guy who sweeps the floor.”
Sean Thomas, MD, assistant professor and chief, Division of Medical Informatics, Department of Medicine, John A. Burns School of Medicine, University of Hawaii at Manoa (Honolulu), envisions changing the way physicians review and interpret patient information.
“There’s a constant increase in the amount and complexity of clinical information collected on each patient, and this will only continue to grow,” says Dr. Thomas. “Right now the chart consists of static, self-contained narratives on the care of patients. Little bits of important information are buried in the prose of physician notes ... H&Ps, progress notes, study interpretations—pathology, imaging studies, etc.
“In order to find these bits of info, a physician must read—or likely scan—these documents and pull out what is important,” he continues. “This is a time-consuming process, and the physician runs the risk of missing vital information.”
Dr. Thomas has a vision of “smart” computer software that can pull information into a clinical abstract that provides a dynamic view of the patient’s status. This change calls for re-education of physicians and advances in technology—both of which are realistically attainable.
Regardless of their specific goals for change, most healthcare professionals agree: Improving patient care is the first priority, but so are heightening efficiency, improving costs, and reducing errors in hospitals.
Works in Progress
Numerous professional organizations are working to advance some or all aspects of hospital medicine and administration. Some of the work that is currently underway includes:
- The Institute for Healthcare Improvement (IHI) hosted the 1st Annual International Summit on Redesigning Hospital Care, June 2005 in San Diego, where medical professionals and hospital executives attended sessions on critical care, patient safety, flow, and workforce development.
- The Agency for Healthcare Research and Quality (AHRQ) awarded 108 grants totaling $139 million to advance the use of information technology in healthcare to reduce medical errors, improve the quality of patient care, and reduce the cost of healthcare.
AHRQ also created a National Resource Center for Health Information Technology and is facilitating expert and peer-to-peer collaborative learning and fostering the growth of online communities who are planning, implementing, and researching health information technology (IT).
- Denver Health (DH) has received a $350,000 hospital redesign grant—an Integrated Delivery System Research Network Project Award, which is part of the AHRQ. Its focus will be removing silos of care, or independent treatment groups, between and across hospital disciplines. DH is redesigning its internal and external processes, as well as its infrastructure.
DH is receiving input from operational, organizational, and regulatory experts (among them representatives from the Joint Commission on Accreditation of Healthcare Organizations, CMS, IHI, Microsoft, Siemens, and Ritz Carlton), providers and administrators, patients and their families. DH is creating a hospital command center to collect, control, and disperse information from a central location. It’s also focusing on improving operating room turnover time to accommodate more surgeries.
Hospitalists as Change Agents
Who will be involved in redesigning the hospital? Currently the major players in designing and implementing change include professional, nonprofit, and government associations (such as those listed above), universities, and independent healthcare consulting groups. Many groups work directly with hospitals on pilot programs for change.
Once change reaches the hospital level, different professionals can become involved, including administrators, physicians, and nursing staff.
But what role can (and should) hospitalists play in getting their institution to become a hospital of the future? “In looking farther to the future, one role that hospitalists may increasingly assume is that of change agent,” says David L. Bernd in “The Future Role of Hospitalists.”2 “The nature of the hospitalist’s work ideally situates him to act as a change agent, enabling him to identify process management initiatives and corral physician support. As a result, hospitalists will increasingly serve as administrative partners and leaders of medical staff initiatives to help facilitate organizational change. … hospitalists themselves may become the solution to some of the systems that need changing.”
Dr. Wellikson agrees: “Hospitalists, who for the most part are in the beginning of a 20- to 30-year professional career, are primed to play significant roles in this changing dynamic.
Next Month: an In-depth Look
In a series of articles over the next year or so, The Hospitalist will examine specific aspects of the hospital of the future. Experts and leading thinkers will provide their perspectives and plans regarding everything from what the hospital of the future will look like in terms of its physical layout, to how the admissions process might work, to the role that specialty hospitals will play.
Our series will envision the future of medical records and medications, critical care, patient flow, and how teamwork and collaboration might change the way medical personnel work.
In addition, each month we’ll contrast this vision of the future with a look into the distant past of hospitals (see “Flashback: The power of words,” below), providing a glimpse of the earliest beginnings of the institution and the medical profession.
This series on the hospital of the future is designed to encourage you to think progressively and plan ahead. Change waits for no one in hospital medicine, as we all know. Hospitalists must be poised to become active participants in those changes. So stay tuned; the future is coming. TH
Jane Jerrard is an editorial change agent based in Chicago.
References
- Wellikson L. SHM point of view. The Hospitalist. 2005;2:5.
- Bernd DL. The future role of hospitalists. How hospitalists add value. The Hospitalist. 2005;9(S1):4.
"A Hospitalist Saved My Life"
When Robin Orr was admitted to the ED of Santa Barbara Cottage Hospital (Calif.), she brought a long history of experience with hospitals, both as a patient and in her professional life. Orr is a cancer survivor who had undergone back surgery several months earlier and had suffered from increasing back pain since the surgery. Late one Friday night in June 24, 2005, the pain was so intense that Orr’s care partner, Sue Cook, brought her to the ED. Orr was given morphine and taken to a room for the remainder of the night.
Who Is Robin Orr?
Orr was no ordinary hospital patient. With nearly three decades of experience as a healthcare professional working with hospitals, she was well aware of how hospitals should work—and how they often don’t work. After seven years as a hospital administrator, she went to graduate school for a master’s degree in public health, then spent 12 years as executive director for Planetree Health Resource Center, San Francisco, a nonprofit consumer healthcare organization that focuses on patient-centered care. While Orr was with Planetree the organization created a revolutionary demonstration project that brought patient-centered care to three model sites. The project centered on changing the hospitals’ physical environments as well as providing patients access to their own medical records.
Approximately 12 years ago, Orr left Planetree to start her own consulting practice. The Robin Orr Group (Santa Barbara, Calif.) works with healthcare organizations to effect patient-centered care. At the time she was admitted to the ED at Cottage Hospital, Orr’s consulting work was tapering off as she struggled with constant pain.

—Robin Orr
Enter the Hospitalist
At 7 a.m. on the Saturday the morning after Orr was admitted, Eric Trautwein, MD, checked on her. Dr. Trautwein is a hospitalist with the Samsun Santa Barbara Medical Foundation, which employs approximately 200 physicians in multiple specialties.
“Eric was a breathe of fresh air,” says Cook. “He … had read all her charts and immediately asked about the pain and got it under control.” Throughout the ordeal, Cook says “everyone would ask Robin what the pain level was, and she’d say ‘11,’ and they’d write it down. Eric did something about it.”
The next step, as Cook recalls, was a thorough examination. “I’ll never forget—he noticed that one knee reflex had a very subtle difference,” she says. “He wanted to double check that, saying he never made assumptions. He immediately got tests scheduled for that day, which was a Saturday. That never happens.”
Orr was scheduled for an immediate CAT scan, PET scan, and MRI. The results were available by Monday: The tests showed a mass of 4.5 x 3 cm to the left retroperitoneum adjacent to the aorta, consistent with metastatic disease.
After months of dealing with healthcare professionals who focused on and treated Orr’s pain, both Orr and Cook believe that the hospitalist’s diligence in performing a thorough exam and insistence on immediate tests were remarkable.
“A hospitalist saved my life,” Orr says confidently.
Dr. Trautwein doesn’t feel his exam and diagnosis were unusual.
“I’m not sure I did anything special,” he says. “I know for sure that my partners would have done the same things I did, and so would most hospitalists.”
After the Test Results
At the end of the weekend during Orr’s stay, Dr. Trautwein’s shift ended and his partner, Jeffrey Yim, MD, took over. Before the change, Dr. Trautwein assured the women that he’d go over Orr’s case with his partner, and that he would stay in touch. This is standard procedure among the hospitalists in their practice.
“We’ll ask if there’s anything they want us to convey to the new doctor” before we go off shift, says Dr. Yim.
The hospitalists at Samsun Santa Barbara Medical Foundation take great care with transitions during shift changes because they are aware that mistakes can happen if communication is incomplete.
“Hand-offs are one of our biggest challenges,” says Dr. Yim. “Ours aren’t formalized, but we follow a standard practice of leaving what we call an ‘off-service note.’ This is very comprehensive, almost like a discharge note, and includes all important details. In addition, the outgoing and incoming hospitalists have a sign-off conversation, either in person or over the phone, to cover any social issues or dynamics. With Robin, for example, pain control was an issue.”
Dr. Yim told Orr and Cook the results of the tests.
“Dr. Yim came in on Tuesday, and it was like passing a baton in an Olympic race,” recalls Cook, who is an expert and author on customer service. “Both [of the hospitalists] have empathy, [a skill that is] relevant and timely, and a sense of urgency.”
Orr agrees that Dr. Yim’s care was as helpful as Dr. Trautwein’s.
“Both hospitalists made sure I was treated as a human being; they weren’t just treating my pain,” she says. “Dr. Yim made sure I got what I needed at discharge, which was very necessary. He was on top of it and made sure it included follow-up.”
In Praise of Hospitalists
Despite her profession, Orr says she had never heard of hospitalists before meeting Dr. Trautwein. In addition to her gratitude to him for diagnosing her cancer, she was very impressed with how the role of hospitalist affected her care.
“I felt that having a hospitalist helped streamline the process,” she says. “I was admitted through the ED in the middle of a weekend night, when labs were closed and I had no access to my primary care physician. Despite the timing, there was continuity and follow-through, and there was speed of action.”
Orr was particularly impressed at how the various departments of the hospital worked together, with a hospitalist acting as her champion with all of them.
“[Eric] has a familiarity with hospital resources and knew who to call and when to call,” she says. “He passed the baton between people in such a way that I felt I would not be dropped between departments. There were great communications, and it helped with the ease of streamlining and continuity, and it certainly helped my peace of mind.
“From the perspective of a health professional, I could see that a hospitalist helps eliminate waste,” Orr continues. “I know that hospital resources are so precious, and when someone can help expedite a procedure or test, it’s extremely valuable.”
Orr had a first-hand view of how hospitalists streamline processes and influence care for individual patients. Her experience as a patient was an educational time for her, even with her substantial background working with hospitals.

The Hospitalist’s View
While Dr. Trautwein is pleased with the outcome of his assessment of Orr, he insists that he was doing his job. In fact, he believes the toughest part of being a hospitalist is not detecting hidden illnesses, but building trust.
“The biggest part of my day is communicating. I feel like I don’t have much time to establish trust with patients,” he admits. “That’s by far the hardest thing about the job. You only get one pass to go over their medical history, but you also have to build a rapport with them. It’s not easy.”
With each new patient he sees, Dr. Trautwein is aware that that person is wary of seeing a new doctor rather than their own primary care physician.
“A lot of people are skeptical when they see a new [doctor]—especially a young doctor,” he explains. “Sometimes, I’ll start by trying to talk about something unconnected with their condition, to try to connect with them as a person. Getting patients to trust you is one of the more difficult parts of the job, but it can lead to one of the greatest satisfactions.”
As a hospitalist, Dr. Trautwein has a clear view of his role versus that of a primary care physician, and sees the value in being available to hospitalized patients.
“Primary care physicians are squeezed from every direction and can’t be around their patients in the hospital all the time,” he says. “Hospitalists get the patients’ attention; it’s not hard to drop back into someone’s room. For the patient, that’s important. They see that we care about them, and we can make the face-to-face contact with them that used to be impossible.”
Dr. Trautwein makes a special effort to see each patient as often as he can, and to share information with them.
“I try to think about it from the patient’s perspective,” he says. “The major thing that patients are hungry for in a hospital is communication.”
As for his ability to get tests scheduled on a weekend, he says that Cottage Hospital “is a pretty responsive hospital in general. I don’t spend a lot of time banging my head against the wall with them. If I talk to a person directly, in person or on the phone, they’ll respond. It is unusual to have tests done on the weekend, but it was also unusual to have a patient who needs them so much.”
Dr. Trautwein understands that a normal day’s work for a physician can mean a life-changing diagnosis for a patient. Orr and Cook understand it, too, but from their perspective, a hospitalist doing his job can lead to a miracle.
Orr’s Recovery
At the time this article was written, Orr had completed a round of radiation and was recuperating as she awaits further test results. Despite her ordeal and her pain, her outlook is as positive as her praise of hospitalists. Looking back on her experience at Cottage Hospital Santa Barbara and Dr. Trautwein’s role, she says, “The outcome of all this was my peace of mind as a patient. You can’t buy that in a hospital anywhere in America today.” TH
Contributor Jane Jerrard writes the “Hospital of the Future” series for The Hospitalist.
When Robin Orr was admitted to the ED of Santa Barbara Cottage Hospital (Calif.), she brought a long history of experience with hospitals, both as a patient and in her professional life. Orr is a cancer survivor who had undergone back surgery several months earlier and had suffered from increasing back pain since the surgery. Late one Friday night in June 24, 2005, the pain was so intense that Orr’s care partner, Sue Cook, brought her to the ED. Orr was given morphine and taken to a room for the remainder of the night.
Who Is Robin Orr?
Orr was no ordinary hospital patient. With nearly three decades of experience as a healthcare professional working with hospitals, she was well aware of how hospitals should work—and how they often don’t work. After seven years as a hospital administrator, she went to graduate school for a master’s degree in public health, then spent 12 years as executive director for Planetree Health Resource Center, San Francisco, a nonprofit consumer healthcare organization that focuses on patient-centered care. While Orr was with Planetree the organization created a revolutionary demonstration project that brought patient-centered care to three model sites. The project centered on changing the hospitals’ physical environments as well as providing patients access to their own medical records.
Approximately 12 years ago, Orr left Planetree to start her own consulting practice. The Robin Orr Group (Santa Barbara, Calif.) works with healthcare organizations to effect patient-centered care. At the time she was admitted to the ED at Cottage Hospital, Orr’s consulting work was tapering off as she struggled with constant pain.
—Robin Orr
Enter the Hospitalist
At 7 a.m. on the Saturday the morning after Orr was admitted, Eric Trautwein, MD, checked on her. Dr. Trautwein is a hospitalist with the Samsun Santa Barbara Medical Foundation, which employs approximately 200 physicians in multiple specialties.
“Eric was a breathe of fresh air,” says Cook. “He … had read all her charts and immediately asked about the pain and got it under control.” Throughout the ordeal, Cook says “everyone would ask Robin what the pain level was, and she’d say ‘11,’ and they’d write it down. Eric did something about it.”
The next step, as Cook recalls, was a thorough examination. “I’ll never forget—he noticed that one knee reflex had a very subtle difference,” she says. “He wanted to double check that, saying he never made assumptions. He immediately got tests scheduled for that day, which was a Saturday. That never happens.”
Orr was scheduled for an immediate CAT scan, PET scan, and MRI. The results were available by Monday: The tests showed a mass of 4.5 x 3 cm to the left retroperitoneum adjacent to the aorta, consistent with metastatic disease.
After months of dealing with healthcare professionals who focused on and treated Orr’s pain, both Orr and Cook believe that the hospitalist’s diligence in performing a thorough exam and insistence on immediate tests were remarkable.
“A hospitalist saved my life,” Orr says confidently.
Dr. Trautwein doesn’t feel his exam and diagnosis were unusual.
“I’m not sure I did anything special,” he says. “I know for sure that my partners would have done the same things I did, and so would most hospitalists.”
After the Test Results
At the end of the weekend during Orr’s stay, Dr. Trautwein’s shift ended and his partner, Jeffrey Yim, MD, took over. Before the change, Dr. Trautwein assured the women that he’d go over Orr’s case with his partner, and that he would stay in touch. This is standard procedure among the hospitalists in their practice.
“We’ll ask if there’s anything they want us to convey to the new doctor” before we go off shift, says Dr. Yim.
The hospitalists at Samsun Santa Barbara Medical Foundation take great care with transitions during shift changes because they are aware that mistakes can happen if communication is incomplete.
“Hand-offs are one of our biggest challenges,” says Dr. Yim. “Ours aren’t formalized, but we follow a standard practice of leaving what we call an ‘off-service note.’ This is very comprehensive, almost like a discharge note, and includes all important details. In addition, the outgoing and incoming hospitalists have a sign-off conversation, either in person or over the phone, to cover any social issues or dynamics. With Robin, for example, pain control was an issue.”
Dr. Yim told Orr and Cook the results of the tests.
“Dr. Yim came in on Tuesday, and it was like passing a baton in an Olympic race,” recalls Cook, who is an expert and author on customer service. “Both [of the hospitalists] have empathy, [a skill that is] relevant and timely, and a sense of urgency.”
Orr agrees that Dr. Yim’s care was as helpful as Dr. Trautwein’s.
“Both hospitalists made sure I was treated as a human being; they weren’t just treating my pain,” she says. “Dr. Yim made sure I got what I needed at discharge, which was very necessary. He was on top of it and made sure it included follow-up.”
In Praise of Hospitalists
Despite her profession, Orr says she had never heard of hospitalists before meeting Dr. Trautwein. In addition to her gratitude to him for diagnosing her cancer, she was very impressed with how the role of hospitalist affected her care.
“I felt that having a hospitalist helped streamline the process,” she says. “I was admitted through the ED in the middle of a weekend night, when labs were closed and I had no access to my primary care physician. Despite the timing, there was continuity and follow-through, and there was speed of action.”
Orr was particularly impressed at how the various departments of the hospital worked together, with a hospitalist acting as her champion with all of them.
“[Eric] has a familiarity with hospital resources and knew who to call and when to call,” she says. “He passed the baton between people in such a way that I felt I would not be dropped between departments. There were great communications, and it helped with the ease of streamlining and continuity, and it certainly helped my peace of mind.
“From the perspective of a health professional, I could see that a hospitalist helps eliminate waste,” Orr continues. “I know that hospital resources are so precious, and when someone can help expedite a procedure or test, it’s extremely valuable.”
Orr had a first-hand view of how hospitalists streamline processes and influence care for individual patients. Her experience as a patient was an educational time for her, even with her substantial background working with hospitals.
The Hospitalist’s View
While Dr. Trautwein is pleased with the outcome of his assessment of Orr, he insists that he was doing his job. In fact, he believes the toughest part of being a hospitalist is not detecting hidden illnesses, but building trust.
“The biggest part of my day is communicating. I feel like I don’t have much time to establish trust with patients,” he admits. “That’s by far the hardest thing about the job. You only get one pass to go over their medical history, but you also have to build a rapport with them. It’s not easy.”
With each new patient he sees, Dr. Trautwein is aware that that person is wary of seeing a new doctor rather than their own primary care physician.
“A lot of people are skeptical when they see a new [doctor]—especially a young doctor,” he explains. “Sometimes, I’ll start by trying to talk about something unconnected with their condition, to try to connect with them as a person. Getting patients to trust you is one of the more difficult parts of the job, but it can lead to one of the greatest satisfactions.”
As a hospitalist, Dr. Trautwein has a clear view of his role versus that of a primary care physician, and sees the value in being available to hospitalized patients.
“Primary care physicians are squeezed from every direction and can’t be around their patients in the hospital all the time,” he says. “Hospitalists get the patients’ attention; it’s not hard to drop back into someone’s room. For the patient, that’s important. They see that we care about them, and we can make the face-to-face contact with them that used to be impossible.”
Dr. Trautwein makes a special effort to see each patient as often as he can, and to share information with them.
“I try to think about it from the patient’s perspective,” he says. “The major thing that patients are hungry for in a hospital is communication.”
As for his ability to get tests scheduled on a weekend, he says that Cottage Hospital “is a pretty responsive hospital in general. I don’t spend a lot of time banging my head against the wall with them. If I talk to a person directly, in person or on the phone, they’ll respond. It is unusual to have tests done on the weekend, but it was also unusual to have a patient who needs them so much.”
Dr. Trautwein understands that a normal day’s work for a physician can mean a life-changing diagnosis for a patient. Orr and Cook understand it, too, but from their perspective, a hospitalist doing his job can lead to a miracle.
Orr’s Recovery
At the time this article was written, Orr had completed a round of radiation and was recuperating as she awaits further test results. Despite her ordeal and her pain, her outlook is as positive as her praise of hospitalists. Looking back on her experience at Cottage Hospital Santa Barbara and Dr. Trautwein’s role, she says, “The outcome of all this was my peace of mind as a patient. You can’t buy that in a hospital anywhere in America today.” TH
Contributor Jane Jerrard writes the “Hospital of the Future” series for The Hospitalist.
When Robin Orr was admitted to the ED of Santa Barbara Cottage Hospital (Calif.), she brought a long history of experience with hospitals, both as a patient and in her professional life. Orr is a cancer survivor who had undergone back surgery several months earlier and had suffered from increasing back pain since the surgery. Late one Friday night in June 24, 2005, the pain was so intense that Orr’s care partner, Sue Cook, brought her to the ED. Orr was given morphine and taken to a room for the remainder of the night.
Who Is Robin Orr?
Orr was no ordinary hospital patient. With nearly three decades of experience as a healthcare professional working with hospitals, she was well aware of how hospitals should work—and how they often don’t work. After seven years as a hospital administrator, she went to graduate school for a master’s degree in public health, then spent 12 years as executive director for Planetree Health Resource Center, San Francisco, a nonprofit consumer healthcare organization that focuses on patient-centered care. While Orr was with Planetree the organization created a revolutionary demonstration project that brought patient-centered care to three model sites. The project centered on changing the hospitals’ physical environments as well as providing patients access to their own medical records.
Approximately 12 years ago, Orr left Planetree to start her own consulting practice. The Robin Orr Group (Santa Barbara, Calif.) works with healthcare organizations to effect patient-centered care. At the time she was admitted to the ED at Cottage Hospital, Orr’s consulting work was tapering off as she struggled with constant pain.
—Robin Orr
Enter the Hospitalist
At 7 a.m. on the Saturday the morning after Orr was admitted, Eric Trautwein, MD, checked on her. Dr. Trautwein is a hospitalist with the Samsun Santa Barbara Medical Foundation, which employs approximately 200 physicians in multiple specialties.
“Eric was a breathe of fresh air,” says Cook. “He … had read all her charts and immediately asked about the pain and got it under control.” Throughout the ordeal, Cook says “everyone would ask Robin what the pain level was, and she’d say ‘11,’ and they’d write it down. Eric did something about it.”
The next step, as Cook recalls, was a thorough examination. “I’ll never forget—he noticed that one knee reflex had a very subtle difference,” she says. “He wanted to double check that, saying he never made assumptions. He immediately got tests scheduled for that day, which was a Saturday. That never happens.”
Orr was scheduled for an immediate CAT scan, PET scan, and MRI. The results were available by Monday: The tests showed a mass of 4.5 x 3 cm to the left retroperitoneum adjacent to the aorta, consistent with metastatic disease.
After months of dealing with healthcare professionals who focused on and treated Orr’s pain, both Orr and Cook believe that the hospitalist’s diligence in performing a thorough exam and insistence on immediate tests were remarkable.
“A hospitalist saved my life,” Orr says confidently.
Dr. Trautwein doesn’t feel his exam and diagnosis were unusual.
“I’m not sure I did anything special,” he says. “I know for sure that my partners would have done the same things I did, and so would most hospitalists.”
After the Test Results
At the end of the weekend during Orr’s stay, Dr. Trautwein’s shift ended and his partner, Jeffrey Yim, MD, took over. Before the change, Dr. Trautwein assured the women that he’d go over Orr’s case with his partner, and that he would stay in touch. This is standard procedure among the hospitalists in their practice.
“We’ll ask if there’s anything they want us to convey to the new doctor” before we go off shift, says Dr. Yim.
The hospitalists at Samsun Santa Barbara Medical Foundation take great care with transitions during shift changes because they are aware that mistakes can happen if communication is incomplete.
“Hand-offs are one of our biggest challenges,” says Dr. Yim. “Ours aren’t formalized, but we follow a standard practice of leaving what we call an ‘off-service note.’ This is very comprehensive, almost like a discharge note, and includes all important details. In addition, the outgoing and incoming hospitalists have a sign-off conversation, either in person or over the phone, to cover any social issues or dynamics. With Robin, for example, pain control was an issue.”
Dr. Yim told Orr and Cook the results of the tests.
“Dr. Yim came in on Tuesday, and it was like passing a baton in an Olympic race,” recalls Cook, who is an expert and author on customer service. “Both [of the hospitalists] have empathy, [a skill that is] relevant and timely, and a sense of urgency.”
Orr agrees that Dr. Yim’s care was as helpful as Dr. Trautwein’s.
“Both hospitalists made sure I was treated as a human being; they weren’t just treating my pain,” she says. “Dr. Yim made sure I got what I needed at discharge, which was very necessary. He was on top of it and made sure it included follow-up.”
In Praise of Hospitalists
Despite her profession, Orr says she had never heard of hospitalists before meeting Dr. Trautwein. In addition to her gratitude to him for diagnosing her cancer, she was very impressed with how the role of hospitalist affected her care.
“I felt that having a hospitalist helped streamline the process,” she says. “I was admitted through the ED in the middle of a weekend night, when labs were closed and I had no access to my primary care physician. Despite the timing, there was continuity and follow-through, and there was speed of action.”
Orr was particularly impressed at how the various departments of the hospital worked together, with a hospitalist acting as her champion with all of them.
“[Eric] has a familiarity with hospital resources and knew who to call and when to call,” she says. “He passed the baton between people in such a way that I felt I would not be dropped between departments. There were great communications, and it helped with the ease of streamlining and continuity, and it certainly helped my peace of mind.
“From the perspective of a health professional, I could see that a hospitalist helps eliminate waste,” Orr continues. “I know that hospital resources are so precious, and when someone can help expedite a procedure or test, it’s extremely valuable.”
Orr had a first-hand view of how hospitalists streamline processes and influence care for individual patients. Her experience as a patient was an educational time for her, even with her substantial background working with hospitals.
The Hospitalist’s View
While Dr. Trautwein is pleased with the outcome of his assessment of Orr, he insists that he was doing his job. In fact, he believes the toughest part of being a hospitalist is not detecting hidden illnesses, but building trust.
“The biggest part of my day is communicating. I feel like I don’t have much time to establish trust with patients,” he admits. “That’s by far the hardest thing about the job. You only get one pass to go over their medical history, but you also have to build a rapport with them. It’s not easy.”
With each new patient he sees, Dr. Trautwein is aware that that person is wary of seeing a new doctor rather than their own primary care physician.
“A lot of people are skeptical when they see a new [doctor]—especially a young doctor,” he explains. “Sometimes, I’ll start by trying to talk about something unconnected with their condition, to try to connect with them as a person. Getting patients to trust you is one of the more difficult parts of the job, but it can lead to one of the greatest satisfactions.”
As a hospitalist, Dr. Trautwein has a clear view of his role versus that of a primary care physician, and sees the value in being available to hospitalized patients.
“Primary care physicians are squeezed from every direction and can’t be around their patients in the hospital all the time,” he says. “Hospitalists get the patients’ attention; it’s not hard to drop back into someone’s room. For the patient, that’s important. They see that we care about them, and we can make the face-to-face contact with them that used to be impossible.”
Dr. Trautwein makes a special effort to see each patient as often as he can, and to share information with them.
“I try to think about it from the patient’s perspective,” he says. “The major thing that patients are hungry for in a hospital is communication.”
As for his ability to get tests scheduled on a weekend, he says that Cottage Hospital “is a pretty responsive hospital in general. I don’t spend a lot of time banging my head against the wall with them. If I talk to a person directly, in person or on the phone, they’ll respond. It is unusual to have tests done on the weekend, but it was also unusual to have a patient who needs them so much.”
Dr. Trautwein understands that a normal day’s work for a physician can mean a life-changing diagnosis for a patient. Orr and Cook understand it, too, but from their perspective, a hospitalist doing his job can lead to a miracle.
Orr’s Recovery
At the time this article was written, Orr had completed a round of radiation and was recuperating as she awaits further test results. Despite her ordeal and her pain, her outlook is as positive as her praise of hospitalists. Looking back on her experience at Cottage Hospital Santa Barbara and Dr. Trautwein’s role, she says, “The outcome of all this was my peace of mind as a patient. You can’t buy that in a hospital anywhere in America today.” TH
Contributor Jane Jerrard writes the “Hospital of the Future” series for The Hospitalist.