User login
Calculating the Future of CMS Payments
Hospitalists and other physicians with Medicare patients are awaiting final word on proposed changes to the Medicare Physician Fee Schedule, due to take effect next year.
How, exactly, will the fee changes affect you? What will your revenue look like in 2007? You can find answers to these questions by understanding what the changes will be and by using a new online tool developed by the American College of Physicians (ACP).
A Look at the Proposed Payment Changes
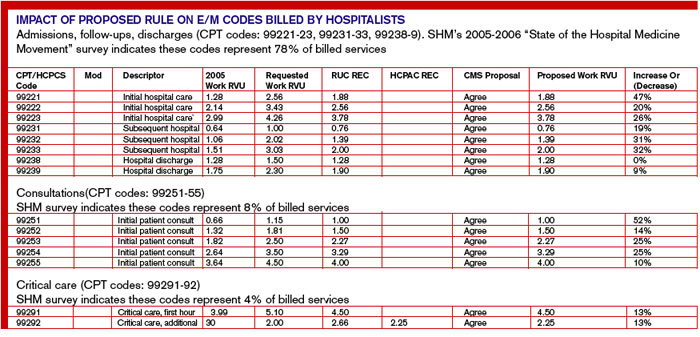
The Centers for Medicare and Medicaid Services (CMS) has proposed specific changes to the Medicare Physician Fee Schedule that would significantly increase payments for Medicare beneficiaries’ hospital visits, office visits, consultations, and other evaluation and management (E/M) services. If the proposed changes are enacted, Medicare payments would substantially increase for these services. How substantial are the increases? The work relative value unit (RVU) for initial hospital care (CPT code 99221) would increase by 47%, and the work RVU for subsequent hospital care (CPT code 99232) would increase by 31%. (For a detailed breakdown of the “Impact of the Proposed Rule on E/M Codes Billed by Hospitalists,” see p. 38.)
How will these proposed increases affect your income? The dollar amount is difficult to calculate, partly because, due to legislative restrictions, Medicare payments won’t increase by the same percentage as the E/M relative values. CMS can make only budget-neutral changes. This means it can’t increase payments by more than $20 million per year. Because the proposed 2007 changes exceed this amount—they come close to $4 billion—CMS has proposed an additional adjustment that reduces payment equally for all physician services in order to maintain 2007 expenditures at roughly their 2006 level. This adjustment means that payment for some low-level E/M services will decrease.
An Online Calculator Can Help
The ACP has developed an interactive revenue calculator to enable its members to estimate their reimbursements under the proposed changes. Available for members only on the ACP Web site (www.acponline.org/private/pmc/emimpact.html), the calculator estimates the potential revenue change for E/M services only.
“We thought [the calculator] would be helpful to our members,” explains Brian Whitman, senior analyst for Regulatory and Insurer Affairs, ACP. “The RVU changes are technical and complex, and it’s hard for a practicing physician to translate the changes. Doctors see dollars, not RVUs. Also, the changes all depend on the volume of Medicare patients they have and how they code.”
Physicians who use the ACP reimbursement calculator enter the number of visits they provide to Medicare beneficiaries in a typical week, categorized under individual CPT codes. The calculator then determines their Medicare revenue for 2006 and their projected Medicare revenue for 2007. Finally, it estimates how much their 2007 revenue will change in a typical week and in the upcoming year.
Of course, the Medicare payment received for many non-E/M services will decrease because, as stated earlier, the Medicare statute requires CMS to keep 2007 expenditures at roughly the same level as those generated in 2006.
After using the online calculator to determine their payments from the affected E/M codes, ACP members can then estimate their projected net revenue change. The ACP recommends that physicians estimate their 2006 Medicare revenue for all services not specifically listed in the calculator and then multiply that figure by 0.95 to account for the budget neutrality adjustment. They can then subtract that number from the total payment found in the online calculator to get an estimate of their net Medicare payment change in 2007.
The ACP’s reimbursement calculator is not designed to be precise; that would be impossible. “The calculator itself is an estimate,” warns Whitman. For one thing, the payments per RVU will not be certain until CMS publishes its final 2007 relative values. In addition, E/M service payments by private health plans that use the Medicare-approved RVUs for determining their own fee schedules are likely to increase.
What Happens Next?
CMS proposed the changes in June. According to the law, CMS must solicit comments from the public for 60 days. Some time after considering these comments, CMS will announce its final decision on the payment changes for E/M and other services. “They usually release their final rule in October or November,” says Whitman. CMS has proposed using the revised RVUs beginning January 1, 2007.
For the latest news on the proposed payment changes, check the SHM Web site at www.hospitalmedicine.org. If you’re a member of the ACP, check out the online reimbursement calculator at www.acponline.org/private/pmc/emimpact.html. TH
Hospitalists and other physicians with Medicare patients are awaiting final word on proposed changes to the Medicare Physician Fee Schedule, due to take effect next year.
How, exactly, will the fee changes affect you? What will your revenue look like in 2007? You can find answers to these questions by understanding what the changes will be and by using a new online tool developed by the American College of Physicians (ACP).
A Look at the Proposed Payment Changes
The Centers for Medicare and Medicaid Services (CMS) has proposed specific changes to the Medicare Physician Fee Schedule that would significantly increase payments for Medicare beneficiaries’ hospital visits, office visits, consultations, and other evaluation and management (E/M) services. If the proposed changes are enacted, Medicare payments would substantially increase for these services. How substantial are the increases? The work relative value unit (RVU) for initial hospital care (CPT code 99221) would increase by 47%, and the work RVU for subsequent hospital care (CPT code 99232) would increase by 31%. (For a detailed breakdown of the “Impact of the Proposed Rule on E/M Codes Billed by Hospitalists,” see p. 38.)
How will these proposed increases affect your income? The dollar amount is difficult to calculate, partly because, due to legislative restrictions, Medicare payments won’t increase by the same percentage as the E/M relative values. CMS can make only budget-neutral changes. This means it can’t increase payments by more than $20 million per year. Because the proposed 2007 changes exceed this amount—they come close to $4 billion—CMS has proposed an additional adjustment that reduces payment equally for all physician services in order to maintain 2007 expenditures at roughly their 2006 level. This adjustment means that payment for some low-level E/M services will decrease.
An Online Calculator Can Help
The ACP has developed an interactive revenue calculator to enable its members to estimate their reimbursements under the proposed changes. Available for members only on the ACP Web site (www.acponline.org/private/pmc/emimpact.html), the calculator estimates the potential revenue change for E/M services only.
“We thought [the calculator] would be helpful to our members,” explains Brian Whitman, senior analyst for Regulatory and Insurer Affairs, ACP. “The RVU changes are technical and complex, and it’s hard for a practicing physician to translate the changes. Doctors see dollars, not RVUs. Also, the changes all depend on the volume of Medicare patients they have and how they code.”
Physicians who use the ACP reimbursement calculator enter the number of visits they provide to Medicare beneficiaries in a typical week, categorized under individual CPT codes. The calculator then determines their Medicare revenue for 2006 and their projected Medicare revenue for 2007. Finally, it estimates how much their 2007 revenue will change in a typical week and in the upcoming year.
Of course, the Medicare payment received for many non-E/M services will decrease because, as stated earlier, the Medicare statute requires CMS to keep 2007 expenditures at roughly the same level as those generated in 2006.
After using the online calculator to determine their payments from the affected E/M codes, ACP members can then estimate their projected net revenue change. The ACP recommends that physicians estimate their 2006 Medicare revenue for all services not specifically listed in the calculator and then multiply that figure by 0.95 to account for the budget neutrality adjustment. They can then subtract that number from the total payment found in the online calculator to get an estimate of their net Medicare payment change in 2007.
The ACP’s reimbursement calculator is not designed to be precise; that would be impossible. “The calculator itself is an estimate,” warns Whitman. For one thing, the payments per RVU will not be certain until CMS publishes its final 2007 relative values. In addition, E/M service payments by private health plans that use the Medicare-approved RVUs for determining their own fee schedules are likely to increase.
What Happens Next?
CMS proposed the changes in June. According to the law, CMS must solicit comments from the public for 60 days. Some time after considering these comments, CMS will announce its final decision on the payment changes for E/M and other services. “They usually release their final rule in October or November,” says Whitman. CMS has proposed using the revised RVUs beginning January 1, 2007.
For the latest news on the proposed payment changes, check the SHM Web site at www.hospitalmedicine.org. If you’re a member of the ACP, check out the online reimbursement calculator at www.acponline.org/private/pmc/emimpact.html. TH
Hospitalists and other physicians with Medicare patients are awaiting final word on proposed changes to the Medicare Physician Fee Schedule, due to take effect next year.
How, exactly, will the fee changes affect you? What will your revenue look like in 2007? You can find answers to these questions by understanding what the changes will be and by using a new online tool developed by the American College of Physicians (ACP).
A Look at the Proposed Payment Changes
The Centers for Medicare and Medicaid Services (CMS) has proposed specific changes to the Medicare Physician Fee Schedule that would significantly increase payments for Medicare beneficiaries’ hospital visits, office visits, consultations, and other evaluation and management (E/M) services. If the proposed changes are enacted, Medicare payments would substantially increase for these services. How substantial are the increases? The work relative value unit (RVU) for initial hospital care (CPT code 99221) would increase by 47%, and the work RVU for subsequent hospital care (CPT code 99232) would increase by 31%. (For a detailed breakdown of the “Impact of the Proposed Rule on E/M Codes Billed by Hospitalists,” see p. 38.)
How will these proposed increases affect your income? The dollar amount is difficult to calculate, partly because, due to legislative restrictions, Medicare payments won’t increase by the same percentage as the E/M relative values. CMS can make only budget-neutral changes. This means it can’t increase payments by more than $20 million per year. Because the proposed 2007 changes exceed this amount—they come close to $4 billion—CMS has proposed an additional adjustment that reduces payment equally for all physician services in order to maintain 2007 expenditures at roughly their 2006 level. This adjustment means that payment for some low-level E/M services will decrease.
An Online Calculator Can Help
The ACP has developed an interactive revenue calculator to enable its members to estimate their reimbursements under the proposed changes. Available for members only on the ACP Web site (www.acponline.org/private/pmc/emimpact.html), the calculator estimates the potential revenue change for E/M services only.
“We thought [the calculator] would be helpful to our members,” explains Brian Whitman, senior analyst for Regulatory and Insurer Affairs, ACP. “The RVU changes are technical and complex, and it’s hard for a practicing physician to translate the changes. Doctors see dollars, not RVUs. Also, the changes all depend on the volume of Medicare patients they have and how they code.”
Physicians who use the ACP reimbursement calculator enter the number of visits they provide to Medicare beneficiaries in a typical week, categorized under individual CPT codes. The calculator then determines their Medicare revenue for 2006 and their projected Medicare revenue for 2007. Finally, it estimates how much their 2007 revenue will change in a typical week and in the upcoming year.
Of course, the Medicare payment received for many non-E/M services will decrease because, as stated earlier, the Medicare statute requires CMS to keep 2007 expenditures at roughly the same level as those generated in 2006.
After using the online calculator to determine their payments from the affected E/M codes, ACP members can then estimate their projected net revenue change. The ACP recommends that physicians estimate their 2006 Medicare revenue for all services not specifically listed in the calculator and then multiply that figure by 0.95 to account for the budget neutrality adjustment. They can then subtract that number from the total payment found in the online calculator to get an estimate of their net Medicare payment change in 2007.
The ACP’s reimbursement calculator is not designed to be precise; that would be impossible. “The calculator itself is an estimate,” warns Whitman. For one thing, the payments per RVU will not be certain until CMS publishes its final 2007 relative values. In addition, E/M service payments by private health plans that use the Medicare-approved RVUs for determining their own fee schedules are likely to increase.
What Happens Next?
CMS proposed the changes in June. According to the law, CMS must solicit comments from the public for 60 days. Some time after considering these comments, CMS will announce its final decision on the payment changes for E/M and other services. “They usually release their final rule in October or November,” says Whitman. CMS has proposed using the revised RVUs beginning January 1, 2007.
For the latest news on the proposed payment changes, check the SHM Web site at www.hospitalmedicine.org. If you’re a member of the ACP, check out the online reimbursement calculator at www.acponline.org/private/pmc/emimpact.html. TH
The Hospitalist Generation
If hospital medicine had to be associated with a single generation, it would most likely be generation X. According to SHM’s recently released 2005-2006 “Survey of Hospitalist Productivity and Compensation,” the average age of hospitalists is 37—the current average age of generation X. But more than the same life stage, this generation shares common characteristics, perspectives, and habits that seem consistent with hospitalists of all ages.
Meet Generation X
Generation X is the term for the generation born between 1965 and 1976. Because they were influenced by the same world events and social trends, this generation (as all generations) brings its own traits and values to the workplace. “The career hallmarks of this generation include their independence and enterprising desire to make things happen,” says Devon Scheef, a partner in The Learning Café (TLC@TheLearningCafe.net), a consulting firm that specializes in helping managers overcome generational differences.
According to The Learning Café, the 51 million members of generation X grew up in a much different world than previous generations. Divorce and two-income families created latchkey kids out of many in this generation, leading to traits of independence, resilience, and adaptability. Members of generation X feel strongly that they don't need someone looking over their shoulders.
This independence can make hospital medicine especially appealing to young physicians because they can often structure their daily work to suit themselves.
When Work Ethics Collide
Generation X and baby boomer workers most often butt heads over differing work ethics. This is true across all industries, including the medical field—in hospitals and other healthcare settings. Baby boomers tend to put in long hours and devote themselves to their work. “They [baby boomers] work hard—maybe too hard,” says Diane Thielfoldt, partner in The Learning Café. “This is the generation that increased our workweek from 40 hours to 70 or 80 hours.” And baby boomers often expect this level of dedication from their colleagues.
Generation Xers are not interested in working these hours; they do not equate long hours with job efficiency. One of the big draws of hospital medicine is the flexible schedule; a young physician can work a set schedule, such as seven-on, seven-off, and know that when she’s not working, she’s free to do what she wants.
Of generation X physicians, Lawrence G. Smith, FACP, chief academic officer, North Shore-Long Island Jewish Health System, says, “Led by women, this generation of [medical] students will work fewer hours and demand flexible employment opportunities.”1
Young physicians who choose private practice or other specialties may find it difficult to fight the work ethic expectations of older physicians and administrators. “Aging boomers—a terrible term for those in the 46- to 55-year-old bracket—have really run into a wall of work-life balance,” Scheef points out. “They are scaling back on work and looking ahead to retirement. This is hard for this go-go generation. Many are looking to the younger generation—we hear this in healthcare, particularly—to lighten their workload.”
How Generation X Works
Contrary to what many baby boomer bosses may think, members of generation X are terrific employees. They simply have their own way of getting things done.
“Gen Xers are in a new stage of life now, in their mid- to late 30s, and we’re seeing some interesting trends,” says Thielfoldt. “Gen Xers have an entrepreneurial spirit. This trend has become stronger as the generation has gotten older, which is surprising.” Some young hospitalists have taken this trend to the extreme, founding their own hospital medicine groups; others build their careers by creating and running new projects and committees. “They seem very oriented to ownership and accountability to define, create, and implement in their careers,” continues Thielfoldt. “Gen Xers are driven out of organizations when asked to focus on just one piece of the process.” Again, this fits in with the hospitalist personality.
At the same time, generation X values learning new skills or specialties. “As a generation, they tend to be very portfolio-oriented, in any industry,” says Thielfoldt. “They want to build a skills portfolio as they would a financial portfolio. They want expertise and new skills. This is more important to them than how much or how little time they work.”
Generation X may also find hospital medicine to be the perfect job because the management style suits them so well. “Gen Xers are very sensitive to micromanaging,” says Scheef. “And now that they have the confidence of experience, [the negative reaction to micromanaging by a supervisor] is worse. Instead of traditional managing, they are very receptive to expert coaching or formal mentoring. This can tie in really well with helping them develop that skills portfolio.”
Changes Are Coming
As more baby boomers retire and generation X becomes firmly established, healthcare and other industries may change the way they operate. “Gen Xers have growing families now. They have come to the work-life balance issue much earlier than any other generation,” says Thielfoldt. “And unlike previous generations, their top priority is spending time with their children. That sounds crazy, right? Boomers have doted on their children—but they spend their time at work, especially fathers. Gen X fathers spend more time on average with their kids than boomers did at the same age.” The eventual outcome: “Employers need to respect this as a top priority and provide flexible scheduling to allow it.”
Many hospital medicine programs are doing just that, searching for ways to adequately cover the patient census and workload and keep hospitalists happy.
Dr. Smith agrees that change must come to healthcare: “The future environment … must recognize that physician well-being and balance in life is a valid and important concern and does not negate the attainment of professionalism. It must reward excellence, not endurance.”1 TH
Jane Jerrard regularly writes “Career Development.”
References
- Smith, LG. Medical professionalism and the generation gap. Am J Med. 2005 Apr;118(4):439-442.
If hospital medicine had to be associated with a single generation, it would most likely be generation X. According to SHM’s recently released 2005-2006 “Survey of Hospitalist Productivity and Compensation,” the average age of hospitalists is 37—the current average age of generation X. But more than the same life stage, this generation shares common characteristics, perspectives, and habits that seem consistent with hospitalists of all ages.
Meet Generation X
Generation X is the term for the generation born between 1965 and 1976. Because they were influenced by the same world events and social trends, this generation (as all generations) brings its own traits and values to the workplace. “The career hallmarks of this generation include their independence and enterprising desire to make things happen,” says Devon Scheef, a partner in The Learning Café (TLC@TheLearningCafe.net), a consulting firm that specializes in helping managers overcome generational differences.
According to The Learning Café, the 51 million members of generation X grew up in a much different world than previous generations. Divorce and two-income families created latchkey kids out of many in this generation, leading to traits of independence, resilience, and adaptability. Members of generation X feel strongly that they don't need someone looking over their shoulders.
This independence can make hospital medicine especially appealing to young physicians because they can often structure their daily work to suit themselves.
When Work Ethics Collide
Generation X and baby boomer workers most often butt heads over differing work ethics. This is true across all industries, including the medical field—in hospitals and other healthcare settings. Baby boomers tend to put in long hours and devote themselves to their work. “They [baby boomers] work hard—maybe too hard,” says Diane Thielfoldt, partner in The Learning Café. “This is the generation that increased our workweek from 40 hours to 70 or 80 hours.” And baby boomers often expect this level of dedication from their colleagues.
Generation Xers are not interested in working these hours; they do not equate long hours with job efficiency. One of the big draws of hospital medicine is the flexible schedule; a young physician can work a set schedule, such as seven-on, seven-off, and know that when she’s not working, she’s free to do what she wants.
Of generation X physicians, Lawrence G. Smith, FACP, chief academic officer, North Shore-Long Island Jewish Health System, says, “Led by women, this generation of [medical] students will work fewer hours and demand flexible employment opportunities.”1
Young physicians who choose private practice or other specialties may find it difficult to fight the work ethic expectations of older physicians and administrators. “Aging boomers—a terrible term for those in the 46- to 55-year-old bracket—have really run into a wall of work-life balance,” Scheef points out. “They are scaling back on work and looking ahead to retirement. This is hard for this go-go generation. Many are looking to the younger generation—we hear this in healthcare, particularly—to lighten their workload.”
How Generation X Works
Contrary to what many baby boomer bosses may think, members of generation X are terrific employees. They simply have their own way of getting things done.
“Gen Xers are in a new stage of life now, in their mid- to late 30s, and we’re seeing some interesting trends,” says Thielfoldt. “Gen Xers have an entrepreneurial spirit. This trend has become stronger as the generation has gotten older, which is surprising.” Some young hospitalists have taken this trend to the extreme, founding their own hospital medicine groups; others build their careers by creating and running new projects and committees. “They seem very oriented to ownership and accountability to define, create, and implement in their careers,” continues Thielfoldt. “Gen Xers are driven out of organizations when asked to focus on just one piece of the process.” Again, this fits in with the hospitalist personality.
At the same time, generation X values learning new skills or specialties. “As a generation, they tend to be very portfolio-oriented, in any industry,” says Thielfoldt. “They want to build a skills portfolio as they would a financial portfolio. They want expertise and new skills. This is more important to them than how much or how little time they work.”
Generation X may also find hospital medicine to be the perfect job because the management style suits them so well. “Gen Xers are very sensitive to micromanaging,” says Scheef. “And now that they have the confidence of experience, [the negative reaction to micromanaging by a supervisor] is worse. Instead of traditional managing, they are very receptive to expert coaching or formal mentoring. This can tie in really well with helping them develop that skills portfolio.”
Changes Are Coming
As more baby boomers retire and generation X becomes firmly established, healthcare and other industries may change the way they operate. “Gen Xers have growing families now. They have come to the work-life balance issue much earlier than any other generation,” says Thielfoldt. “And unlike previous generations, their top priority is spending time with their children. That sounds crazy, right? Boomers have doted on their children—but they spend their time at work, especially fathers. Gen X fathers spend more time on average with their kids than boomers did at the same age.” The eventual outcome: “Employers need to respect this as a top priority and provide flexible scheduling to allow it.”
Many hospital medicine programs are doing just that, searching for ways to adequately cover the patient census and workload and keep hospitalists happy.
Dr. Smith agrees that change must come to healthcare: “The future environment … must recognize that physician well-being and balance in life is a valid and important concern and does not negate the attainment of professionalism. It must reward excellence, not endurance.”1 TH
Jane Jerrard regularly writes “Career Development.”
References
- Smith, LG. Medical professionalism and the generation gap. Am J Med. 2005 Apr;118(4):439-442.
If hospital medicine had to be associated with a single generation, it would most likely be generation X. According to SHM’s recently released 2005-2006 “Survey of Hospitalist Productivity and Compensation,” the average age of hospitalists is 37—the current average age of generation X. But more than the same life stage, this generation shares common characteristics, perspectives, and habits that seem consistent with hospitalists of all ages.
Meet Generation X
Generation X is the term for the generation born between 1965 and 1976. Because they were influenced by the same world events and social trends, this generation (as all generations) brings its own traits and values to the workplace. “The career hallmarks of this generation include their independence and enterprising desire to make things happen,” says Devon Scheef, a partner in The Learning Café (TLC@TheLearningCafe.net), a consulting firm that specializes in helping managers overcome generational differences.
According to The Learning Café, the 51 million members of generation X grew up in a much different world than previous generations. Divorce and two-income families created latchkey kids out of many in this generation, leading to traits of independence, resilience, and adaptability. Members of generation X feel strongly that they don't need someone looking over their shoulders.
This independence can make hospital medicine especially appealing to young physicians because they can often structure their daily work to suit themselves.
When Work Ethics Collide
Generation X and baby boomer workers most often butt heads over differing work ethics. This is true across all industries, including the medical field—in hospitals and other healthcare settings. Baby boomers tend to put in long hours and devote themselves to their work. “They [baby boomers] work hard—maybe too hard,” says Diane Thielfoldt, partner in The Learning Café. “This is the generation that increased our workweek from 40 hours to 70 or 80 hours.” And baby boomers often expect this level of dedication from their colleagues.
Generation Xers are not interested in working these hours; they do not equate long hours with job efficiency. One of the big draws of hospital medicine is the flexible schedule; a young physician can work a set schedule, such as seven-on, seven-off, and know that when she’s not working, she’s free to do what she wants.
Of generation X physicians, Lawrence G. Smith, FACP, chief academic officer, North Shore-Long Island Jewish Health System, says, “Led by women, this generation of [medical] students will work fewer hours and demand flexible employment opportunities.”1
Young physicians who choose private practice or other specialties may find it difficult to fight the work ethic expectations of older physicians and administrators. “Aging boomers—a terrible term for those in the 46- to 55-year-old bracket—have really run into a wall of work-life balance,” Scheef points out. “They are scaling back on work and looking ahead to retirement. This is hard for this go-go generation. Many are looking to the younger generation—we hear this in healthcare, particularly—to lighten their workload.”
How Generation X Works
Contrary to what many baby boomer bosses may think, members of generation X are terrific employees. They simply have their own way of getting things done.
“Gen Xers are in a new stage of life now, in their mid- to late 30s, and we’re seeing some interesting trends,” says Thielfoldt. “Gen Xers have an entrepreneurial spirit. This trend has become stronger as the generation has gotten older, which is surprising.” Some young hospitalists have taken this trend to the extreme, founding their own hospital medicine groups; others build their careers by creating and running new projects and committees. “They seem very oriented to ownership and accountability to define, create, and implement in their careers,” continues Thielfoldt. “Gen Xers are driven out of organizations when asked to focus on just one piece of the process.” Again, this fits in with the hospitalist personality.
At the same time, generation X values learning new skills or specialties. “As a generation, they tend to be very portfolio-oriented, in any industry,” says Thielfoldt. “They want to build a skills portfolio as they would a financial portfolio. They want expertise and new skills. This is more important to them than how much or how little time they work.”
Generation X may also find hospital medicine to be the perfect job because the management style suits them so well. “Gen Xers are very sensitive to micromanaging,” says Scheef. “And now that they have the confidence of experience, [the negative reaction to micromanaging by a supervisor] is worse. Instead of traditional managing, they are very receptive to expert coaching or formal mentoring. This can tie in really well with helping them develop that skills portfolio.”
Changes Are Coming
As more baby boomers retire and generation X becomes firmly established, healthcare and other industries may change the way they operate. “Gen Xers have growing families now. They have come to the work-life balance issue much earlier than any other generation,” says Thielfoldt. “And unlike previous generations, their top priority is spending time with their children. That sounds crazy, right? Boomers have doted on their children—but they spend their time at work, especially fathers. Gen X fathers spend more time on average with their kids than boomers did at the same age.” The eventual outcome: “Employers need to respect this as a top priority and provide flexible scheduling to allow it.”
Many hospital medicine programs are doing just that, searching for ways to adequately cover the patient census and workload and keep hospitalists happy.
Dr. Smith agrees that change must come to healthcare: “The future environment … must recognize that physician well-being and balance in life is a valid and important concern and does not negate the attainment of professionalism. It must reward excellence, not endurance.”1 TH
Jane Jerrard regularly writes “Career Development.”
References
- Smith, LG. Medical professionalism and the generation gap. Am J Med. 2005 Apr;118(4):439-442.
Shift Perspectives
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
Liability, Medical Error Legislation
Liability. To a physician, the word conjures the threat of a malpractice lawsuit and the reality of escalating insurance costs. But some protection may be at hand in the form of several laws recently passed by Congress that aim to relieve both threat and reality.
Hospitalists and Liability
For the time being, the majority of hospitalists are covered by their employer’s liability insurance, according to the cover article in the December 2005 issue of The Hospitalist (“A Malpractice Primer” p. 1). However, that doesn’t mean they’re unaffected by risk of malpractice suits.
—Mary A. Germann, RN, MN, CHE
Mary A. Germann, RN, MN, CHE, certified healthcare compliance officer and founder of Operations Solutions for Healthcare, Inc., a consulting firm based in Atlanta, has answered many liability questions from hospitalists and believes they are at least as worried about the issue as other physicians.
“Hospitalists tend to be concerned about their risk,” she says. “They want to know how to protect themselves. Even though they may not be ‘personally’ at risk, their medical license is still on the line."
Germann explains that hospitalists may in fact be more vulnerable to liability suits than other physicians. “In some ways [hospitalists] are more at risk because they are usually new to their patients,” she says. “They have not had the opportunity to build a relationship with a patient, and must create trust and open communications in a very short time. This weak link can increase a hospitalist’s vulnerability. Lack of information and communication is one of the biggest reasons reported that patients choose to sue.”
With this in mind, let’s take a look at current and pending legislation that will shape liability risk and claims for years to come.
The HEALTH Act of 2005
Passed into law in July of last year, the HEALTH Act (or Help Efficient, Accessible, Low-cost, Timely Healthcare Act), places multiple limits on liability claims. The law caps noneconomic damages in medical malpractice suits at $250,000 for compensating patient injury, limits attorneys’ contingency fees, and requires a finding of malicious intent to support an award of punitive damages. The law also exempts manufacturers and distributors of medical products from punitive damage awards if the U.S. Food and Drug Administration approved the product.
The Patient Safety and Quality Improvement Act of 2005
Also signed into law last July, this act establishes a voluntary, confidential reporting structure for use by physicians, hospitals, and other healthcare professional and entities. This law renders reported medical errors into confidential, privileged data and allows healthcare providers to report their medical errors under a “patient safety activity” umbrella that prohibits the information from being used in a civil action (i.e. liability case). All medical errors reported are covered by the law and not subject to subpoena, Freedom of Information Act request, or use in a disciplinary proceeding.
On reporting medical errors within a hospital system, Germann says, “This is really a joint effort; I don’t think any one entity or organization can do it by themselves. Hospitals have to have a system in place for reporting errors and near misses. Studies have shown that organizations that aggressively support error disclosure have a decreased incidence in the number of suits and a decrease in the compensation payouts.”
The National Medical Error Disclosure and Compensation Act of 2005
Also known as the MEDiC Act, this bill was introduced in the Senate in September 2005 by Senator Hillary Rodham Clinton (D-N.Y.) and Senator Barack Obama (D-Ill.).
Designed to extend the Patient Safety and Quality Improvement Act of 2005 and “promote a culture of safety within hospitals, health systems, clinics, and other sites of healthcare,” this act would establish a federal Office of Patient Safety and Health Care Quality to implement and oversee a new national patient safety database, as well as the MEDiC Program. This program would provide funding to those healthcare providers with systems to disclose medical errors to patients and offer fair compensation to patients if the provider is at fault.
In reducing administrative and legal costs for medical malpractice claims, the MEDiC Act would require participating medical liability insurance companies and healthcare providers to apply a percentage of their savings toward reducing medical errors. The bill also requires that, to the extent possible, some of these cost savings be passed along to providers as lower malpractice insurance premiums.
Although not specifically stated in the bill, a goal of the MEDiC Act is to provide an interim solution to the escalating costs of liability lawsuits.
“I think [medical error reporting] is a very good direction to take,” says Germann. “One of the major barriers to disclosing errors is fear of malpractice suits. To improve quality and decrease medical errors, it’s important for physicians to be able to disclose errors.”
In addition, she stresses that hospitalists and other physicians have little to fear in disclosure. “The majority of errors are not caused by incompetent physicians,” notes Germann. “They are secondary to system failures. Physicians must be able to expose these. And hospitalists see more system errors because they live within the system; they can be a great asset in helping hospital administrators improve quality and systems.”
The MEDiC Act has been under review by the Senate Committee on Health, Education, Labor, and Pensions since September.
So far, 2005 and 2006 have seen big changes in liability reform and in medical error reporting. Together, this legislation—perhaps in conjunction with future laws—will change the risks of liability faced by hospitalists. "No one law is going to solve the entire problem,” says Germann. “All of these together will make the improvements." TH
Jane Jerrard writes “Public Policy” every month for The Hospitalist.
Liability. To a physician, the word conjures the threat of a malpractice lawsuit and the reality of escalating insurance costs. But some protection may be at hand in the form of several laws recently passed by Congress that aim to relieve both threat and reality.
Hospitalists and Liability
For the time being, the majority of hospitalists are covered by their employer’s liability insurance, according to the cover article in the December 2005 issue of The Hospitalist (“A Malpractice Primer” p. 1). However, that doesn’t mean they’re unaffected by risk of malpractice suits.
—Mary A. Germann, RN, MN, CHE
Mary A. Germann, RN, MN, CHE, certified healthcare compliance officer and founder of Operations Solutions for Healthcare, Inc., a consulting firm based in Atlanta, has answered many liability questions from hospitalists and believes they are at least as worried about the issue as other physicians.
“Hospitalists tend to be concerned about their risk,” she says. “They want to know how to protect themselves. Even though they may not be ‘personally’ at risk, their medical license is still on the line."
Germann explains that hospitalists may in fact be more vulnerable to liability suits than other physicians. “In some ways [hospitalists] are more at risk because they are usually new to their patients,” she says. “They have not had the opportunity to build a relationship with a patient, and must create trust and open communications in a very short time. This weak link can increase a hospitalist’s vulnerability. Lack of information and communication is one of the biggest reasons reported that patients choose to sue.”
With this in mind, let’s take a look at current and pending legislation that will shape liability risk and claims for years to come.
The HEALTH Act of 2005
Passed into law in July of last year, the HEALTH Act (or Help Efficient, Accessible, Low-cost, Timely Healthcare Act), places multiple limits on liability claims. The law caps noneconomic damages in medical malpractice suits at $250,000 for compensating patient injury, limits attorneys’ contingency fees, and requires a finding of malicious intent to support an award of punitive damages. The law also exempts manufacturers and distributors of medical products from punitive damage awards if the U.S. Food and Drug Administration approved the product.
The Patient Safety and Quality Improvement Act of 2005
Also signed into law last July, this act establishes a voluntary, confidential reporting structure for use by physicians, hospitals, and other healthcare professional and entities. This law renders reported medical errors into confidential, privileged data and allows healthcare providers to report their medical errors under a “patient safety activity” umbrella that prohibits the information from being used in a civil action (i.e. liability case). All medical errors reported are covered by the law and not subject to subpoena, Freedom of Information Act request, or use in a disciplinary proceeding.
On reporting medical errors within a hospital system, Germann says, “This is really a joint effort; I don’t think any one entity or organization can do it by themselves. Hospitals have to have a system in place for reporting errors and near misses. Studies have shown that organizations that aggressively support error disclosure have a decreased incidence in the number of suits and a decrease in the compensation payouts.”
The National Medical Error Disclosure and Compensation Act of 2005
Also known as the MEDiC Act, this bill was introduced in the Senate in September 2005 by Senator Hillary Rodham Clinton (D-N.Y.) and Senator Barack Obama (D-Ill.).
Designed to extend the Patient Safety and Quality Improvement Act of 2005 and “promote a culture of safety within hospitals, health systems, clinics, and other sites of healthcare,” this act would establish a federal Office of Patient Safety and Health Care Quality to implement and oversee a new national patient safety database, as well as the MEDiC Program. This program would provide funding to those healthcare providers with systems to disclose medical errors to patients and offer fair compensation to patients if the provider is at fault.
In reducing administrative and legal costs for medical malpractice claims, the MEDiC Act would require participating medical liability insurance companies and healthcare providers to apply a percentage of their savings toward reducing medical errors. The bill also requires that, to the extent possible, some of these cost savings be passed along to providers as lower malpractice insurance premiums.
Although not specifically stated in the bill, a goal of the MEDiC Act is to provide an interim solution to the escalating costs of liability lawsuits.
“I think [medical error reporting] is a very good direction to take,” says Germann. “One of the major barriers to disclosing errors is fear of malpractice suits. To improve quality and decrease medical errors, it’s important for physicians to be able to disclose errors.”
In addition, she stresses that hospitalists and other physicians have little to fear in disclosure. “The majority of errors are not caused by incompetent physicians,” notes Germann. “They are secondary to system failures. Physicians must be able to expose these. And hospitalists see more system errors because they live within the system; they can be a great asset in helping hospital administrators improve quality and systems.”
The MEDiC Act has been under review by the Senate Committee on Health, Education, Labor, and Pensions since September.
So far, 2005 and 2006 have seen big changes in liability reform and in medical error reporting. Together, this legislation—perhaps in conjunction with future laws—will change the risks of liability faced by hospitalists. "No one law is going to solve the entire problem,” says Germann. “All of these together will make the improvements." TH
Jane Jerrard writes “Public Policy” every month for The Hospitalist.
Liability. To a physician, the word conjures the threat of a malpractice lawsuit and the reality of escalating insurance costs. But some protection may be at hand in the form of several laws recently passed by Congress that aim to relieve both threat and reality.
Hospitalists and Liability
For the time being, the majority of hospitalists are covered by their employer’s liability insurance, according to the cover article in the December 2005 issue of The Hospitalist (“A Malpractice Primer” p. 1). However, that doesn’t mean they’re unaffected by risk of malpractice suits.
—Mary A. Germann, RN, MN, CHE
Mary A. Germann, RN, MN, CHE, certified healthcare compliance officer and founder of Operations Solutions for Healthcare, Inc., a consulting firm based in Atlanta, has answered many liability questions from hospitalists and believes they are at least as worried about the issue as other physicians.
“Hospitalists tend to be concerned about their risk,” she says. “They want to know how to protect themselves. Even though they may not be ‘personally’ at risk, their medical license is still on the line."
Germann explains that hospitalists may in fact be more vulnerable to liability suits than other physicians. “In some ways [hospitalists] are more at risk because they are usually new to their patients,” she says. “They have not had the opportunity to build a relationship with a patient, and must create trust and open communications in a very short time. This weak link can increase a hospitalist’s vulnerability. Lack of information and communication is one of the biggest reasons reported that patients choose to sue.”
With this in mind, let’s take a look at current and pending legislation that will shape liability risk and claims for years to come.
The HEALTH Act of 2005
Passed into law in July of last year, the HEALTH Act (or Help Efficient, Accessible, Low-cost, Timely Healthcare Act), places multiple limits on liability claims. The law caps noneconomic damages in medical malpractice suits at $250,000 for compensating patient injury, limits attorneys’ contingency fees, and requires a finding of malicious intent to support an award of punitive damages. The law also exempts manufacturers and distributors of medical products from punitive damage awards if the U.S. Food and Drug Administration approved the product.
The Patient Safety and Quality Improvement Act of 2005
Also signed into law last July, this act establishes a voluntary, confidential reporting structure for use by physicians, hospitals, and other healthcare professional and entities. This law renders reported medical errors into confidential, privileged data and allows healthcare providers to report their medical errors under a “patient safety activity” umbrella that prohibits the information from being used in a civil action (i.e. liability case). All medical errors reported are covered by the law and not subject to subpoena, Freedom of Information Act request, or use in a disciplinary proceeding.
On reporting medical errors within a hospital system, Germann says, “This is really a joint effort; I don’t think any one entity or organization can do it by themselves. Hospitals have to have a system in place for reporting errors and near misses. Studies have shown that organizations that aggressively support error disclosure have a decreased incidence in the number of suits and a decrease in the compensation payouts.”
The National Medical Error Disclosure and Compensation Act of 2005
Also known as the MEDiC Act, this bill was introduced in the Senate in September 2005 by Senator Hillary Rodham Clinton (D-N.Y.) and Senator Barack Obama (D-Ill.).
Designed to extend the Patient Safety and Quality Improvement Act of 2005 and “promote a culture of safety within hospitals, health systems, clinics, and other sites of healthcare,” this act would establish a federal Office of Patient Safety and Health Care Quality to implement and oversee a new national patient safety database, as well as the MEDiC Program. This program would provide funding to those healthcare providers with systems to disclose medical errors to patients and offer fair compensation to patients if the provider is at fault.
In reducing administrative and legal costs for medical malpractice claims, the MEDiC Act would require participating medical liability insurance companies and healthcare providers to apply a percentage of their savings toward reducing medical errors. The bill also requires that, to the extent possible, some of these cost savings be passed along to providers as lower malpractice insurance premiums.
Although not specifically stated in the bill, a goal of the MEDiC Act is to provide an interim solution to the escalating costs of liability lawsuits.
“I think [medical error reporting] is a very good direction to take,” says Germann. “One of the major barriers to disclosing errors is fear of malpractice suits. To improve quality and decrease medical errors, it’s important for physicians to be able to disclose errors.”
In addition, she stresses that hospitalists and other physicians have little to fear in disclosure. “The majority of errors are not caused by incompetent physicians,” notes Germann. “They are secondary to system failures. Physicians must be able to expose these. And hospitalists see more system errors because they live within the system; they can be a great asset in helping hospital administrators improve quality and systems.”
The MEDiC Act has been under review by the Senate Committee on Health, Education, Labor, and Pensions since September.
So far, 2005 and 2006 have seen big changes in liability reform and in medical error reporting. Together, this legislation—perhaps in conjunction with future laws—will change the risks of liability faced by hospitalists. "No one law is going to solve the entire problem,” says Germann. “All of these together will make the improvements." TH
Jane Jerrard writes “Public Policy” every month for The Hospitalist.
Add Mentoring to Your Hospitalist Mix
Providing a mentoring program that pairs newly hired hospitalists with more experienced ones is beneficial for several reasons. Mentors can boost the comfort level of new hospitalists and improve likelihood of retention. They can also add continuity of culture and processes to a hospital medicine program.
This month we look at how—and why—Cogent Healthcare maintains its system-wide mentoring program. “Mentoring provides an added dimension to a traditional management structure,” explains Russell L. Holman, MD, senior vice president and national medical director, Cogent Healthcare, and president-elect of SHM. “Mentors can put a very personal, subjective, human element to learning. There’s almost an emotional component, as opposed to being more didactic.”
Case Study in Brief
Cogent’s mentoring program has evolved over time, but the organization tries to keep the program’s structure loose and informal. “In the world of mentoring research—which is largely the business world, not the healthcare world—it’s clear that mentoring relationships that develop naturally are more effective than those that are assigned,” says Dr. Holman.
Cogent teams mentor new programs, rather than individual hospitalists. However, their broad outline of the mentor/mentee relationship can be applied to a one-on-one scenario. At Cogent, an experienced hospitalist will visit a new facility at set times.
“With all programs, we schedule visits at certain intervals,” says Dr. Holman. “But there’s a fair amount of informal contact with the mentors on an as-needed basis.”
Each site visit lasts one to two days. “When a mentor is on-site, their only responsibility is to spend time with the physicians,” explains Dr. Holman. “And typically, at the end of each visit we look forward to evaluating it, getting feedback from the physicians as well as the mentor.”
During the site visit, all physicians in the program have complete, open access to the mentor. “It’s a group dynamic, but there’s as much one-on-one time as possible,” says Dr. Holman.
The intervals at which a mentor visits a program are standard, as are the topics covered—at least at first. “We look at critical phases in the life cycle of our programs,” says Dr. Holman. “When a program first starts, people are concerned with the nuts and bolts of operations, such as the use of guidelines, information systems, decision support tools, coding/billing, and even scheduling suggestions. A mentorship visit at this stage provides useful tips on operational implementation that are highly pragmatic.”
The next visit takes place within three to six months of the program’s implementation. At this point, says Dr. Holman, “there’s a comfortable workflow established but it’s likely that none of the physicians have worked together before. A mentor can talk about teamwork, including tips to bring consistency to the practice style.”
Next, after the program has been up and running for nine to 12 months, Dr. Holman says, “there’s enough experience in the program to speak more specifically to efficiency issues. An experienced hospitalist can provide focused mentorship on time-management skills, ways to extend your clinical reach, and ways to expand the number of patients you’re caring for. Most hospitalists are relatively young—many are within a year or two of completing their residency—so they’re still building these skills.”
At 12 months and beyond, the mentoring becomes much more customized to the specific needs of the individual program. “Maybe a program is trying to establish good working relationships with key departments within the hospital … or they want advanced clinical tools,” speculates Dr. Holman. “It may be that our hospitalists have been asked to lead an initiative, and they don’t have experience in leading hospital-wide initiatives. At this point, mentorship can reach a new level.”
Meet the Mentors
A mentor should be well versed in organizational processes, have clinical expertise and—if not an experienced teacher—should have well-honed people skills.
“Our mentors come from a profile of different folks, including the founding group of Cogent, a large practice in Los Angeles comprised of experienced hospitalists,” explains Dr. Holman. “Another group of mentors is our entire slate of medical directors, who have individual expertise in different areas. When mentors go on site visits, there’s no direct reporting, but they bring their expertise and facilitate networking.”
Cogent continues to widen its pool of available mentors, and is working to include physicians with special expertise. “We’re trying to build a diverse team [of mentors],” says Dr. Holman. “We look for clinical expertise in physicians who may not necessarily hold leadership roles. We try to predetermine which available mentor we think will be the best fit for a program, including personality, culture, and expertise.”
You Can Introduce Mentoring
You many not have the resources or number of physicians that Cogent has, but you can still start your own mentoring program. “Any program can look at a variety of resources to build a stable of mentors, or at least have a couple of mentors they can draw on,” insists Dr. Holman. “Look at other members of the medical staff that are experienced and role models for desirable qualities. Mentors can be within the healthcare field, but they don’t have to be physicians. One of my personal mentors for years was a director of human resources. You can even look outside healthcare.
“SHM is constantly looking at how to facilitate mentorship through venues like the Mentorship Breakfast at the Annual Meeting, and I still keep in touch with people I’ve met there,” he continues. “The SHM Annual Meeting is a terrific venue in general if you’re looking to connect members of your group (or yourself) with others from around the country.”
Implementing and maintaining a mentoring program may add to your workload, but it will pay off immediately. Just remember not to plan it out too carefully. “Mentoring is a constant work in progress,” concludes Dr. Holman. “We never want to see it as a static or inflexible entity. It’s a dynamic process driven by physician needs.” TH
Jane Jerrard writes “Career Development” each month for The Hospitalist
Providing a mentoring program that pairs newly hired hospitalists with more experienced ones is beneficial for several reasons. Mentors can boost the comfort level of new hospitalists and improve likelihood of retention. They can also add continuity of culture and processes to a hospital medicine program.
This month we look at how—and why—Cogent Healthcare maintains its system-wide mentoring program. “Mentoring provides an added dimension to a traditional management structure,” explains Russell L. Holman, MD, senior vice president and national medical director, Cogent Healthcare, and president-elect of SHM. “Mentors can put a very personal, subjective, human element to learning. There’s almost an emotional component, as opposed to being more didactic.”
Case Study in Brief
Cogent’s mentoring program has evolved over time, but the organization tries to keep the program’s structure loose and informal. “In the world of mentoring research—which is largely the business world, not the healthcare world—it’s clear that mentoring relationships that develop naturally are more effective than those that are assigned,” says Dr. Holman.
Cogent teams mentor new programs, rather than individual hospitalists. However, their broad outline of the mentor/mentee relationship can be applied to a one-on-one scenario. At Cogent, an experienced hospitalist will visit a new facility at set times.
“With all programs, we schedule visits at certain intervals,” says Dr. Holman. “But there’s a fair amount of informal contact with the mentors on an as-needed basis.”
Each site visit lasts one to two days. “When a mentor is on-site, their only responsibility is to spend time with the physicians,” explains Dr. Holman. “And typically, at the end of each visit we look forward to evaluating it, getting feedback from the physicians as well as the mentor.”
During the site visit, all physicians in the program have complete, open access to the mentor. “It’s a group dynamic, but there’s as much one-on-one time as possible,” says Dr. Holman.
The intervals at which a mentor visits a program are standard, as are the topics covered—at least at first. “We look at critical phases in the life cycle of our programs,” says Dr. Holman. “When a program first starts, people are concerned with the nuts and bolts of operations, such as the use of guidelines, information systems, decision support tools, coding/billing, and even scheduling suggestions. A mentorship visit at this stage provides useful tips on operational implementation that are highly pragmatic.”
The next visit takes place within three to six months of the program’s implementation. At this point, says Dr. Holman, “there’s a comfortable workflow established but it’s likely that none of the physicians have worked together before. A mentor can talk about teamwork, including tips to bring consistency to the practice style.”
Next, after the program has been up and running for nine to 12 months, Dr. Holman says, “there’s enough experience in the program to speak more specifically to efficiency issues. An experienced hospitalist can provide focused mentorship on time-management skills, ways to extend your clinical reach, and ways to expand the number of patients you’re caring for. Most hospitalists are relatively young—many are within a year or two of completing their residency—so they’re still building these skills.”
At 12 months and beyond, the mentoring becomes much more customized to the specific needs of the individual program. “Maybe a program is trying to establish good working relationships with key departments within the hospital … or they want advanced clinical tools,” speculates Dr. Holman. “It may be that our hospitalists have been asked to lead an initiative, and they don’t have experience in leading hospital-wide initiatives. At this point, mentorship can reach a new level.”
Meet the Mentors
A mentor should be well versed in organizational processes, have clinical expertise and—if not an experienced teacher—should have well-honed people skills.
“Our mentors come from a profile of different folks, including the founding group of Cogent, a large practice in Los Angeles comprised of experienced hospitalists,” explains Dr. Holman. “Another group of mentors is our entire slate of medical directors, who have individual expertise in different areas. When mentors go on site visits, there’s no direct reporting, but they bring their expertise and facilitate networking.”
Cogent continues to widen its pool of available mentors, and is working to include physicians with special expertise. “We’re trying to build a diverse team [of mentors],” says Dr. Holman. “We look for clinical expertise in physicians who may not necessarily hold leadership roles. We try to predetermine which available mentor we think will be the best fit for a program, including personality, culture, and expertise.”
You Can Introduce Mentoring
You many not have the resources or number of physicians that Cogent has, but you can still start your own mentoring program. “Any program can look at a variety of resources to build a stable of mentors, or at least have a couple of mentors they can draw on,” insists Dr. Holman. “Look at other members of the medical staff that are experienced and role models for desirable qualities. Mentors can be within the healthcare field, but they don’t have to be physicians. One of my personal mentors for years was a director of human resources. You can even look outside healthcare.
“SHM is constantly looking at how to facilitate mentorship through venues like the Mentorship Breakfast at the Annual Meeting, and I still keep in touch with people I’ve met there,” he continues. “The SHM Annual Meeting is a terrific venue in general if you’re looking to connect members of your group (or yourself) with others from around the country.”
Implementing and maintaining a mentoring program may add to your workload, but it will pay off immediately. Just remember not to plan it out too carefully. “Mentoring is a constant work in progress,” concludes Dr. Holman. “We never want to see it as a static or inflexible entity. It’s a dynamic process driven by physician needs.” TH
Jane Jerrard writes “Career Development” each month for The Hospitalist
Providing a mentoring program that pairs newly hired hospitalists with more experienced ones is beneficial for several reasons. Mentors can boost the comfort level of new hospitalists and improve likelihood of retention. They can also add continuity of culture and processes to a hospital medicine program.
This month we look at how—and why—Cogent Healthcare maintains its system-wide mentoring program. “Mentoring provides an added dimension to a traditional management structure,” explains Russell L. Holman, MD, senior vice president and national medical director, Cogent Healthcare, and president-elect of SHM. “Mentors can put a very personal, subjective, human element to learning. There’s almost an emotional component, as opposed to being more didactic.”
Case Study in Brief
Cogent’s mentoring program has evolved over time, but the organization tries to keep the program’s structure loose and informal. “In the world of mentoring research—which is largely the business world, not the healthcare world—it’s clear that mentoring relationships that develop naturally are more effective than those that are assigned,” says Dr. Holman.
Cogent teams mentor new programs, rather than individual hospitalists. However, their broad outline of the mentor/mentee relationship can be applied to a one-on-one scenario. At Cogent, an experienced hospitalist will visit a new facility at set times.
“With all programs, we schedule visits at certain intervals,” says Dr. Holman. “But there’s a fair amount of informal contact with the mentors on an as-needed basis.”
Each site visit lasts one to two days. “When a mentor is on-site, their only responsibility is to spend time with the physicians,” explains Dr. Holman. “And typically, at the end of each visit we look forward to evaluating it, getting feedback from the physicians as well as the mentor.”
During the site visit, all physicians in the program have complete, open access to the mentor. “It’s a group dynamic, but there’s as much one-on-one time as possible,” says Dr. Holman.
The intervals at which a mentor visits a program are standard, as are the topics covered—at least at first. “We look at critical phases in the life cycle of our programs,” says Dr. Holman. “When a program first starts, people are concerned with the nuts and bolts of operations, such as the use of guidelines, information systems, decision support tools, coding/billing, and even scheduling suggestions. A mentorship visit at this stage provides useful tips on operational implementation that are highly pragmatic.”
The next visit takes place within three to six months of the program’s implementation. At this point, says Dr. Holman, “there’s a comfortable workflow established but it’s likely that none of the physicians have worked together before. A mentor can talk about teamwork, including tips to bring consistency to the practice style.”
Next, after the program has been up and running for nine to 12 months, Dr. Holman says, “there’s enough experience in the program to speak more specifically to efficiency issues. An experienced hospitalist can provide focused mentorship on time-management skills, ways to extend your clinical reach, and ways to expand the number of patients you’re caring for. Most hospitalists are relatively young—many are within a year or two of completing their residency—so they’re still building these skills.”
At 12 months and beyond, the mentoring becomes much more customized to the specific needs of the individual program. “Maybe a program is trying to establish good working relationships with key departments within the hospital … or they want advanced clinical tools,” speculates Dr. Holman. “It may be that our hospitalists have been asked to lead an initiative, and they don’t have experience in leading hospital-wide initiatives. At this point, mentorship can reach a new level.”
Meet the Mentors
A mentor should be well versed in organizational processes, have clinical expertise and—if not an experienced teacher—should have well-honed people skills.
“Our mentors come from a profile of different folks, including the founding group of Cogent, a large practice in Los Angeles comprised of experienced hospitalists,” explains Dr. Holman. “Another group of mentors is our entire slate of medical directors, who have individual expertise in different areas. When mentors go on site visits, there’s no direct reporting, but they bring their expertise and facilitate networking.”
Cogent continues to widen its pool of available mentors, and is working to include physicians with special expertise. “We’re trying to build a diverse team [of mentors],” says Dr. Holman. “We look for clinical expertise in physicians who may not necessarily hold leadership roles. We try to predetermine which available mentor we think will be the best fit for a program, including personality, culture, and expertise.”
You Can Introduce Mentoring
You many not have the resources or number of physicians that Cogent has, but you can still start your own mentoring program. “Any program can look at a variety of resources to build a stable of mentors, or at least have a couple of mentors they can draw on,” insists Dr. Holman. “Look at other members of the medical staff that are experienced and role models for desirable qualities. Mentors can be within the healthcare field, but they don’t have to be physicians. One of my personal mentors for years was a director of human resources. You can even look outside healthcare.
“SHM is constantly looking at how to facilitate mentorship through venues like the Mentorship Breakfast at the Annual Meeting, and I still keep in touch with people I’ve met there,” he continues. “The SHM Annual Meeting is a terrific venue in general if you’re looking to connect members of your group (or yourself) with others from around the country.”
Implementing and maintaining a mentoring program may add to your workload, but it will pay off immediately. Just remember not to plan it out too carefully. “Mentoring is a constant work in progress,” concludes Dr. Holman. “We never want to see it as a static or inflexible entity. It’s a dynamic process driven by physician needs.” TH
Jane Jerrard writes “Career Development” each month for The Hospitalist
What's Up with Voluntary Reporting? - Part 2
This article is the second in a two-part series on the CMS Physician Voluntary Reporting Program. Part one appeared on p. 11 of the May 2006 issue.
Changes in Medicare reporting and payment are coming, and they’re coming fast. Regardless of whether you agree with where Medicare is heading or plan to participate in the first stage of these changes, you’re better off knowing what’s in store.
The first part of this article provided an overview of the Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid (CMS) initiated at the beginning of 2006, including how the reported quality measures apply—or don’t apply—to hospitalists.
Benefits of Reporting
Eric Siegal, MD, chair of SHM’s Public Policy Committee, is convinced that hospitalists should participate in PVRP, although he stresses that he does not speak for SHM on the matter.
“Hospital medicine has positioned itself as a champion of quality improvement,” he points out. “We talk the talk, so now we need to walk the walk [with voluntary reporting]. As a group of physicians who live and breathe this issue, we’ll have that much more credibility for supporting this program.”
Dr. Siegal not only believes hospitalists should report through PVRP, he thinks they will excel at doing so: “Because we’re already used to being measured, I have a suspicion that our adherence to these metrics is going to look very good. This will serve to bolster the argument that hospitalists add value to the care of hospitalized patients.”
Potential Problem Areas for Hospitalists
Hospitalists who participate in PVRP may face a bumpy road. “There are small problems,” admits Dr. Siegal. One of those is the disconnect between the 16 quality measures that physicians can report on and the role that hospitalists play.
“Of the 16 metrics in the starter set, maybe seven apply to hospitalists,” he explains.
Hospitalists may face another unique problem in meeting those measures: “We may have dilemmas over responsibility and reporting,” predicts Dr. Siegal. “For instance, we’re increasingly co-managing patients with surgeons. If a hospitalist wants to comply with a metric, but the surgeon disagrees, does the hospitalist take the hit? The same is true with something like administering aspirin on arrival for acute myocardial infarction. Is that my responsibility or the emergency physician’s?”
Another issue is the Healthcare Common Procedure Coding System (HCPCS) codes—or G-codes—that comprise each of the current PVRP’s 16 quality measures.
“The G-codes are cumbersome,” says Dr. Siegal. “There are G-codes for each measure, and there is talk about changing to a different system. So you may set up to report G-codes only to have the system change. But get used to it—this is a dynamic process that is definitely going to evolve.”
PVRP Is the Future
Dr. Siegal—and many others—believe that the PVRP will evolve into a broader reporting program and will ultimately transform into a mandatory pay-for-performance system for CMS. This may happen faster than CMS usually moves.
“Eventually there will be money tied to this,” he says. “Rumors are that payment modifiers may be tied to reporting as early as the fourth quarter of this year. As things go in the federal government, the evolution to value-based purchasing is moving at a lightning-fast pace—CMS is actually getting pushback from medical groups for moving too fast.”
Dr. Siegal adds that, “CMS is very interested in engaging physician organizations for their input. [CMS Administrator Mark B.] McClellan has done an admirable job of making this an interactive process.”
As PRVP evolves, it is likely to become more applicable to hospitalists.
“This is all part of a larger evolutionary trend in medicine,” explains Dr. Siegal. “Currently, hospitals and physicians are treated separately by CMS, and paid and incentivized differently. There’s growing realization that with rising costs and increased need for quality improvement hospitals and physicians need to have their incentives aligned. Things are going to change and it will take a long time for this to shake out.”
Because PVRP is the wave of the future for CMS payment, Dr. Siegal believes that hospitalists will be better off if they join in now. Voluntary reporting requires hospitalists to develop a new reporting infrastructure, and, as he says, “It’s better to do that now, with only 16 measures, than to have to do it later when there are 36 or 42.”
Dr. Siegal is convinced that hospitalists should support PVRP now, in its first stage. He also believes that SHM will begin to get involved. “We clearly need to be at this table,” he emphasizes. “Hospitalists are going to be the dominant providers of care to hospitalized Medicare patients. That said, SHM is still a relatively small society, and we don’t have the resources to engage every aspect of this debate. This is a huge and complex issue and SHM needs to use its limited resources wisely.”
SHM’s Public Policy Committee will continue to monitor what happens with PVRP and CMS, and SHM may eventually pursue membership in the national quality forums that are developing new metrics.
CMS provides details on the PVRP, including instructions on how to sign up, on their Web site at www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
This article is the second in a two-part series on the CMS Physician Voluntary Reporting Program. Part one appeared on p. 11 of the May 2006 issue.
Changes in Medicare reporting and payment are coming, and they’re coming fast. Regardless of whether you agree with where Medicare is heading or plan to participate in the first stage of these changes, you’re better off knowing what’s in store.
The first part of this article provided an overview of the Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid (CMS) initiated at the beginning of 2006, including how the reported quality measures apply—or don’t apply—to hospitalists.
Benefits of Reporting
Eric Siegal, MD, chair of SHM’s Public Policy Committee, is convinced that hospitalists should participate in PVRP, although he stresses that he does not speak for SHM on the matter.
“Hospital medicine has positioned itself as a champion of quality improvement,” he points out. “We talk the talk, so now we need to walk the walk [with voluntary reporting]. As a group of physicians who live and breathe this issue, we’ll have that much more credibility for supporting this program.”
Dr. Siegal not only believes hospitalists should report through PVRP, he thinks they will excel at doing so: “Because we’re already used to being measured, I have a suspicion that our adherence to these metrics is going to look very good. This will serve to bolster the argument that hospitalists add value to the care of hospitalized patients.”
Potential Problem Areas for Hospitalists
Hospitalists who participate in PVRP may face a bumpy road. “There are small problems,” admits Dr. Siegal. One of those is the disconnect between the 16 quality measures that physicians can report on and the role that hospitalists play.
“Of the 16 metrics in the starter set, maybe seven apply to hospitalists,” he explains.
Hospitalists may face another unique problem in meeting those measures: “We may have dilemmas over responsibility and reporting,” predicts Dr. Siegal. “For instance, we’re increasingly co-managing patients with surgeons. If a hospitalist wants to comply with a metric, but the surgeon disagrees, does the hospitalist take the hit? The same is true with something like administering aspirin on arrival for acute myocardial infarction. Is that my responsibility or the emergency physician’s?”
Another issue is the Healthcare Common Procedure Coding System (HCPCS) codes—or G-codes—that comprise each of the current PVRP’s 16 quality measures.
“The G-codes are cumbersome,” says Dr. Siegal. “There are G-codes for each measure, and there is talk about changing to a different system. So you may set up to report G-codes only to have the system change. But get used to it—this is a dynamic process that is definitely going to evolve.”
PVRP Is the Future
Dr. Siegal—and many others—believe that the PVRP will evolve into a broader reporting program and will ultimately transform into a mandatory pay-for-performance system for CMS. This may happen faster than CMS usually moves.
“Eventually there will be money tied to this,” he says. “Rumors are that payment modifiers may be tied to reporting as early as the fourth quarter of this year. As things go in the federal government, the evolution to value-based purchasing is moving at a lightning-fast pace—CMS is actually getting pushback from medical groups for moving too fast.”
Dr. Siegal adds that, “CMS is very interested in engaging physician organizations for their input. [CMS Administrator Mark B.] McClellan has done an admirable job of making this an interactive process.”
As PRVP evolves, it is likely to become more applicable to hospitalists.
“This is all part of a larger evolutionary trend in medicine,” explains Dr. Siegal. “Currently, hospitals and physicians are treated separately by CMS, and paid and incentivized differently. There’s growing realization that with rising costs and increased need for quality improvement hospitals and physicians need to have their incentives aligned. Things are going to change and it will take a long time for this to shake out.”
Because PVRP is the wave of the future for CMS payment, Dr. Siegal believes that hospitalists will be better off if they join in now. Voluntary reporting requires hospitalists to develop a new reporting infrastructure, and, as he says, “It’s better to do that now, with only 16 measures, than to have to do it later when there are 36 or 42.”
Dr. Siegal is convinced that hospitalists should support PVRP now, in its first stage. He also believes that SHM will begin to get involved. “We clearly need to be at this table,” he emphasizes. “Hospitalists are going to be the dominant providers of care to hospitalized Medicare patients. That said, SHM is still a relatively small society, and we don’t have the resources to engage every aspect of this debate. This is a huge and complex issue and SHM needs to use its limited resources wisely.”
SHM’s Public Policy Committee will continue to monitor what happens with PVRP and CMS, and SHM may eventually pursue membership in the national quality forums that are developing new metrics.
CMS provides details on the PVRP, including instructions on how to sign up, on their Web site at www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
This article is the second in a two-part series on the CMS Physician Voluntary Reporting Program. Part one appeared on p. 11 of the May 2006 issue.
Changes in Medicare reporting and payment are coming, and they’re coming fast. Regardless of whether you agree with where Medicare is heading or plan to participate in the first stage of these changes, you’re better off knowing what’s in store.
The first part of this article provided an overview of the Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid (CMS) initiated at the beginning of 2006, including how the reported quality measures apply—or don’t apply—to hospitalists.
Benefits of Reporting
Eric Siegal, MD, chair of SHM’s Public Policy Committee, is convinced that hospitalists should participate in PVRP, although he stresses that he does not speak for SHM on the matter.
“Hospital medicine has positioned itself as a champion of quality improvement,” he points out. “We talk the talk, so now we need to walk the walk [with voluntary reporting]. As a group of physicians who live and breathe this issue, we’ll have that much more credibility for supporting this program.”
Dr. Siegal not only believes hospitalists should report through PVRP, he thinks they will excel at doing so: “Because we’re already used to being measured, I have a suspicion that our adherence to these metrics is going to look very good. This will serve to bolster the argument that hospitalists add value to the care of hospitalized patients.”
Potential Problem Areas for Hospitalists
Hospitalists who participate in PVRP may face a bumpy road. “There are small problems,” admits Dr. Siegal. One of those is the disconnect between the 16 quality measures that physicians can report on and the role that hospitalists play.
“Of the 16 metrics in the starter set, maybe seven apply to hospitalists,” he explains.
Hospitalists may face another unique problem in meeting those measures: “We may have dilemmas over responsibility and reporting,” predicts Dr. Siegal. “For instance, we’re increasingly co-managing patients with surgeons. If a hospitalist wants to comply with a metric, but the surgeon disagrees, does the hospitalist take the hit? The same is true with something like administering aspirin on arrival for acute myocardial infarction. Is that my responsibility or the emergency physician’s?”
Another issue is the Healthcare Common Procedure Coding System (HCPCS) codes—or G-codes—that comprise each of the current PVRP’s 16 quality measures.
“The G-codes are cumbersome,” says Dr. Siegal. “There are G-codes for each measure, and there is talk about changing to a different system. So you may set up to report G-codes only to have the system change. But get used to it—this is a dynamic process that is definitely going to evolve.”
PVRP Is the Future
Dr. Siegal—and many others—believe that the PVRP will evolve into a broader reporting program and will ultimately transform into a mandatory pay-for-performance system for CMS. This may happen faster than CMS usually moves.
“Eventually there will be money tied to this,” he says. “Rumors are that payment modifiers may be tied to reporting as early as the fourth quarter of this year. As things go in the federal government, the evolution to value-based purchasing is moving at a lightning-fast pace—CMS is actually getting pushback from medical groups for moving too fast.”
Dr. Siegal adds that, “CMS is very interested in engaging physician organizations for their input. [CMS Administrator Mark B.] McClellan has done an admirable job of making this an interactive process.”
As PRVP evolves, it is likely to become more applicable to hospitalists.
“This is all part of a larger evolutionary trend in medicine,” explains Dr. Siegal. “Currently, hospitals and physicians are treated separately by CMS, and paid and incentivized differently. There’s growing realization that with rising costs and increased need for quality improvement hospitals and physicians need to have their incentives aligned. Things are going to change and it will take a long time for this to shake out.”
Because PVRP is the wave of the future for CMS payment, Dr. Siegal believes that hospitalists will be better off if they join in now. Voluntary reporting requires hospitalists to develop a new reporting infrastructure, and, as he says, “It’s better to do that now, with only 16 measures, than to have to do it later when there are 36 or 42.”
Dr. Siegal is convinced that hospitalists should support PVRP now, in its first stage. He also believes that SHM will begin to get involved. “We clearly need to be at this table,” he emphasizes. “Hospitalists are going to be the dominant providers of care to hospitalized Medicare patients. That said, SHM is still a relatively small society, and we don’t have the resources to engage every aspect of this debate. This is a huge and complex issue and SHM needs to use its limited resources wisely.”
SHM’s Public Policy Committee will continue to monitor what happens with PVRP and CMS, and SHM may eventually pursue membership in the national quality forums that are developing new metrics.
CMS provides details on the PVRP, including instructions on how to sign up, on their Web site at www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
What’s up with Voluntary Reporting?
This article is the first in a two-part series on the CMS Physician Voluntary Reporting Program. Part two will appear in the June issue.
How aware are you of impending policies and programs that will shape how you work and get compensated? Changes are on the horizon that will affect physicians in the immediate future, including their relationship with the Centers for Medicare and Medicaid (CMS).
Your future began to change on Jan. 3, 2006, when CMS activated its Physician Voluntary Reporting Program (PVRP). The program truly is voluntary—physicians are free to decide whether they want to participate. There is no financial reward for participation, but participants receive feedback from CMS that can help them improve clinical care and data accuracy. They also get in on the ground floor of a program that is almost certain to evolve into a mandatory reporting system, and possibly a CMS pay-for-performance program.
The American College of Physicians has stated that, “While physicians are under no obligation to participate in the voluntary program, practices that choose to do so may get a sneak preview of CMS’ future pay-for-performance plans.”
Although SHM has no official position on PVRP, Eric Siegal, MD, chair of SHM’s Public Policy Committee, says that the committee has spent a “fair amount of time” examining the program. The group is interested because, as Dr. Siegal says, “Reporting of quality outcomes is the wave of the future.”
—Eric Siegal, MD
An Overview of the Program
What are physicians volunteering to report to CMS? Participating doctors help capture data on the quality of care they provide to Medicare beneficiaries. They report on any (or any applicable) of 16 evidence-based quality measures, each one comprising two to four Healthcare Common Procedure Coding System (HCPCS) codes called G-codes. (See “16 Clinical Measures,” below, for a list of the quality measures.)
Voluntary reporting is done through the existing administrative system for claims. CMS then analyzes the data and measures the quality of services provided to Medicare patients, providing reporting physicians with confidential information on their performance.
Where Do Hospitalists Fit in?
The bright side for hospitalists is that they should have little problem with the reporting requirements of PVRP. “Hospitalists should be used to being measured, because hospitals have been reporting our adherence to quality measures through the [CMS] Hospital Compare Program,” says Dr. Siegal.
However, it’s obvious that PVRP is not designed for all physicians. “We’ve looked at the metrics, and the majority aren’t applicable to hospitalists,” points out Dr. Siegal. “But some are very relevant to us.” CMS is aware of hospitalists’ position regarding the program. Trent Heywood, deputy chief medical officer, CMS, says, “In this construct, hospitalists are in a unique situation. [They] are kind of in between—the question is whether they’re managing the patient. We’re asking things like how well was diabetes controlled and was the blood pressure controlled.”
Regardless of areas of mismatch, hospitalists can certainly participate in voluntary reporting. “I think that we should embrace the PVRP, even though only a few of the measures in the starter set are directly relevant to hospitalists,” says Dr. Siegal. “This program is the first step in a process that will dramatically change the way we are paid for our work. It will be easier to engage it now, when there are only a few metrics, than later when it’s much more pervasive.”
Meanwhile, CMS may need to juggle the reporting role of hospitalists as the program evolves. “What we don’t want to end up with is perverse incentives, where hospitals and physicians have different and potentially misaligned metrics to report,” stresses Dr. Siegal. “We have to make sure that our incentives are aligned. If possible, we should have a system that allows hospitals and hospitalists to share data and reduce the administrative burden required to report our compliance.”
Heywood agrees. “There will continue to be more dialogue about how to deal with this issue,” he says of the hospitalist role in PVRP. “How do we engage the hospitalist? Are they assumed to be on the hospital side or the physician side? We want all physicians on the same side, but that will take some time.”
Time will tell how voluntary reporting will work for hospitalists. Next month, part two of this article will examine the pros and cons of participating now.
For more information on the PVRP, including instructions on how to sign up, visit www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
This article is the first in a two-part series on the CMS Physician Voluntary Reporting Program. Part two will appear in the June issue.
How aware are you of impending policies and programs that will shape how you work and get compensated? Changes are on the horizon that will affect physicians in the immediate future, including their relationship with the Centers for Medicare and Medicaid (CMS).
Your future began to change on Jan. 3, 2006, when CMS activated its Physician Voluntary Reporting Program (PVRP). The program truly is voluntary—physicians are free to decide whether they want to participate. There is no financial reward for participation, but participants receive feedback from CMS that can help them improve clinical care and data accuracy. They also get in on the ground floor of a program that is almost certain to evolve into a mandatory reporting system, and possibly a CMS pay-for-performance program.
The American College of Physicians has stated that, “While physicians are under no obligation to participate in the voluntary program, practices that choose to do so may get a sneak preview of CMS’ future pay-for-performance plans.”
Although SHM has no official position on PVRP, Eric Siegal, MD, chair of SHM’s Public Policy Committee, says that the committee has spent a “fair amount of time” examining the program. The group is interested because, as Dr. Siegal says, “Reporting of quality outcomes is the wave of the future.”
—Eric Siegal, MD
An Overview of the Program
What are physicians volunteering to report to CMS? Participating doctors help capture data on the quality of care they provide to Medicare beneficiaries. They report on any (or any applicable) of 16 evidence-based quality measures, each one comprising two to four Healthcare Common Procedure Coding System (HCPCS) codes called G-codes. (See “16 Clinical Measures,” below, for a list of the quality measures.)
Voluntary reporting is done through the existing administrative system for claims. CMS then analyzes the data and measures the quality of services provided to Medicare patients, providing reporting physicians with confidential information on their performance.
Where Do Hospitalists Fit in?
The bright side for hospitalists is that they should have little problem with the reporting requirements of PVRP. “Hospitalists should be used to being measured, because hospitals have been reporting our adherence to quality measures through the [CMS] Hospital Compare Program,” says Dr. Siegal.
However, it’s obvious that PVRP is not designed for all physicians. “We’ve looked at the metrics, and the majority aren’t applicable to hospitalists,” points out Dr. Siegal. “But some are very relevant to us.” CMS is aware of hospitalists’ position regarding the program. Trent Heywood, deputy chief medical officer, CMS, says, “In this construct, hospitalists are in a unique situation. [They] are kind of in between—the question is whether they’re managing the patient. We’re asking things like how well was diabetes controlled and was the blood pressure controlled.”
Regardless of areas of mismatch, hospitalists can certainly participate in voluntary reporting. “I think that we should embrace the PVRP, even though only a few of the measures in the starter set are directly relevant to hospitalists,” says Dr. Siegal. “This program is the first step in a process that will dramatically change the way we are paid for our work. It will be easier to engage it now, when there are only a few metrics, than later when it’s much more pervasive.”
Meanwhile, CMS may need to juggle the reporting role of hospitalists as the program evolves. “What we don’t want to end up with is perverse incentives, where hospitals and physicians have different and potentially misaligned metrics to report,” stresses Dr. Siegal. “We have to make sure that our incentives are aligned. If possible, we should have a system that allows hospitals and hospitalists to share data and reduce the administrative burden required to report our compliance.”
Heywood agrees. “There will continue to be more dialogue about how to deal with this issue,” he says of the hospitalist role in PVRP. “How do we engage the hospitalist? Are they assumed to be on the hospital side or the physician side? We want all physicians on the same side, but that will take some time.”
Time will tell how voluntary reporting will work for hospitalists. Next month, part two of this article will examine the pros and cons of participating now.
For more information on the PVRP, including instructions on how to sign up, visit www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
This article is the first in a two-part series on the CMS Physician Voluntary Reporting Program. Part two will appear in the June issue.
How aware are you of impending policies and programs that will shape how you work and get compensated? Changes are on the horizon that will affect physicians in the immediate future, including their relationship with the Centers for Medicare and Medicaid (CMS).
Your future began to change on Jan. 3, 2006, when CMS activated its Physician Voluntary Reporting Program (PVRP). The program truly is voluntary—physicians are free to decide whether they want to participate. There is no financial reward for participation, but participants receive feedback from CMS that can help them improve clinical care and data accuracy. They also get in on the ground floor of a program that is almost certain to evolve into a mandatory reporting system, and possibly a CMS pay-for-performance program.
The American College of Physicians has stated that, “While physicians are under no obligation to participate in the voluntary program, practices that choose to do so may get a sneak preview of CMS’ future pay-for-performance plans.”
Although SHM has no official position on PVRP, Eric Siegal, MD, chair of SHM’s Public Policy Committee, says that the committee has spent a “fair amount of time” examining the program. The group is interested because, as Dr. Siegal says, “Reporting of quality outcomes is the wave of the future.”
—Eric Siegal, MD
An Overview of the Program
What are physicians volunteering to report to CMS? Participating doctors help capture data on the quality of care they provide to Medicare beneficiaries. They report on any (or any applicable) of 16 evidence-based quality measures, each one comprising two to four Healthcare Common Procedure Coding System (HCPCS) codes called G-codes. (See “16 Clinical Measures,” below, for a list of the quality measures.)
Voluntary reporting is done through the existing administrative system for claims. CMS then analyzes the data and measures the quality of services provided to Medicare patients, providing reporting physicians with confidential information on their performance.
Where Do Hospitalists Fit in?
The bright side for hospitalists is that they should have little problem with the reporting requirements of PVRP. “Hospitalists should be used to being measured, because hospitals have been reporting our adherence to quality measures through the [CMS] Hospital Compare Program,” says Dr. Siegal.
However, it’s obvious that PVRP is not designed for all physicians. “We’ve looked at the metrics, and the majority aren’t applicable to hospitalists,” points out Dr. Siegal. “But some are very relevant to us.” CMS is aware of hospitalists’ position regarding the program. Trent Heywood, deputy chief medical officer, CMS, says, “In this construct, hospitalists are in a unique situation. [They] are kind of in between—the question is whether they’re managing the patient. We’re asking things like how well was diabetes controlled and was the blood pressure controlled.”
Regardless of areas of mismatch, hospitalists can certainly participate in voluntary reporting. “I think that we should embrace the PVRP, even though only a few of the measures in the starter set are directly relevant to hospitalists,” says Dr. Siegal. “This program is the first step in a process that will dramatically change the way we are paid for our work. It will be easier to engage it now, when there are only a few metrics, than later when it’s much more pervasive.”
Meanwhile, CMS may need to juggle the reporting role of hospitalists as the program evolves. “What we don’t want to end up with is perverse incentives, where hospitals and physicians have different and potentially misaligned metrics to report,” stresses Dr. Siegal. “We have to make sure that our incentives are aligned. If possible, we should have a system that allows hospitals and hospitalists to share data and reduce the administrative burden required to report our compliance.”
Heywood agrees. “There will continue to be more dialogue about how to deal with this issue,” he says of the hospitalist role in PVRP. “How do we engage the hospitalist? Are they assumed to be on the hospital side or the physician side? We want all physicians on the same side, but that will take some time.”
Time will tell how voluntary reporting will work for hospitalists. Next month, part two of this article will examine the pros and cons of participating now.
For more information on the PVRP, including instructions on how to sign up, visit www.cms.hhs.gov/PVRP/01_Overview.asp. TH
Jane Jerrard regularly writes the “Public Policy” department.
Retention Recommendations
Retaining good hospitalists is one of the major factors in building a successful hospital medicine group—but it’s also one of the biggest challenges faced in the industry today. Why is hospitalist retention a problem, and what can be done to ensure your hospitalists stay for the long haul?
“As in any profession, there are some [hospitalists] who constantly look for bigger and better opportunities in the employment world,” admits Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Sometimes this involves individuals looking for a better practice fit or for a better financial compensation package. In addition, hospitalist medicine can lead to burnout if the practice is not created or operated in a prudent manner, thus leading to turnover.”
Retention Is Crucial
Why is it so important to retain your hospitalists? For one thing, keeping physicians in your program for the long term can directly decrease costs, time, and effort related to recruitment and training.
More importantly, by decreasing staff turnover, retention can stabilize your hospitalist program. “A stable staff is influential in maintaining the providers’ focus on the practice mission, goals and objectives, and values,” points out Dr. Simone. “It de-emphasizes personal agendas, which may develop if an individual was looking to move on to another practice or up the ladder at the expense of the practice and fellow providers, and allows the practice team to gel over time. This is in some ways similar to a professional sports team, where chemistry and trust in one’s teammates are created over time.”
You can get your own hospitalist team to gel by retaining physicians for years if you initiate a program with that very goal.
How-Tos of Retention Programs
“There are a lot of [hospitalist] programs that haven’t developed retention programs at the outset,” says Dr. Simone. “They may be behind the eight ball, but they can and should create one. Successful programs identify their practice mission, values, and objectives, and clearly and concisely spell them out. This policy can then be utilized with the existing staff to align the team’s values and can also be used in recruiting future candidates.”
Once you have a solid written mission and vision statement, check to see if your hospitalists share the same values. Have your clinical director or an administrator sit down with providers one-on-one and find out their vision, values, and objectives. If what you hear differs from the core values of the practice, then you must develop a plan on which you can all agree.
“You may also have to consider altering some of the program’s vision and objectives, if appropriate,” says Dr. Simone.
Scheduling: A Core Value
Your group’s values can be reflected in the schedule you set for staff. “The practice structure and schedule plays a very important role in provider retention,” says Dr. Simone. “In general, various schedule types work for different individuals, and—in all probability—the provider will seek out the practices that offer a particular schedule to their liking.”
A hospital group that values time over money may offer larger chunks of time off. “We’ve found that our recruitment and retention improved when we went to a schedule of seven days on, seven off,” says Dr. Simone. “A lot of individuals are attracted to this because it gives them a week at a time to spend with their families or to pursue other interests, such as travel or educational pursuits.”
Whatever schedule you choose, there are some basic tenets Dr. Simone recommends, including:
- Create a schedule that is consistent and stable rather than constantly changing;
- Make sure the schedule is perceived as fair for all providers;
- Ensure that all providers get appropriate time off;
- Give providers enough flexibility to participate in other projects such as teaching, subspecialty clinics, administrative duties, or special projects; and
- Adhere to a schedule that promotes/accommodates a safe patient to provider ratio.
Salary and Bonuses
Money does matter in retention. As long as the pay you offer is perceived as fair, you have a good start. “In the end, you can only afford what your finances dictate,” says Dr. Simone. “Smaller hospitals may fall short on salary, so it’s important for them to recognize their strengths and sell them in order to compete.”
Your hospitalists may be attracted to participate in an incentive program that rewards them for hard work and productivity. “Incentives help change behavior, and people are stimulated when they have direct control over their own pay,” says Dr. Simone. “There are hospitalist programs with incentive plans, but many programs aren’t sure how to incentivize. You don’t want to reward doctors solely on the amount of work they do.”
For instance, a hospital-based program that rewards hospitalists on the basis of how many patients they admit is basically encouraging them to hospitalize every patient they see.
“I recommend finding a way to reward quality work and dedication, while not neglecting productivity,” says Dr. Simone. “In my opinion, the focus needs to be on increasing the program’s ability to standardize care following evidence-based protocols, encouraging participation in the value-added services that hospitalists are so good at, like participating in a rapid response team or a code blue team, acting as hospital leaders, educating hospital staff and residents, etc.”
Feeling Connected
Unlike many other physicians, hospitalists don’t get many opportunities to connect with patients or a community.
“In my opinion, a hospitalist’s professional job satisfaction and retention is influenced by the perception of feeling connected to the practice and providers, patients, colleagues, and the hospital,” says Dr. Simone. “There are various characteristics of an employment arrangement that may help an individual feel connected. When an employee feels connected, he/she will typically dedicate themselves to the mission of the company and perform at or above expectations.”
Create or revisit your group’s retention program today. By ensuring that the values and objectives of your practice are clearly stated, and catering to those values and objectives in scheduling and other management practices, you can begin to build your retention. TH
Jane Jerrard writes the “Career Development” column every month for The Hospitalist.
Retaining good hospitalists is one of the major factors in building a successful hospital medicine group—but it’s also one of the biggest challenges faced in the industry today. Why is hospitalist retention a problem, and what can be done to ensure your hospitalists stay for the long haul?
“As in any profession, there are some [hospitalists] who constantly look for bigger and better opportunities in the employment world,” admits Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Sometimes this involves individuals looking for a better practice fit or for a better financial compensation package. In addition, hospitalist medicine can lead to burnout if the practice is not created or operated in a prudent manner, thus leading to turnover.”
Retention Is Crucial
Why is it so important to retain your hospitalists? For one thing, keeping physicians in your program for the long term can directly decrease costs, time, and effort related to recruitment and training.
More importantly, by decreasing staff turnover, retention can stabilize your hospitalist program. “A stable staff is influential in maintaining the providers’ focus on the practice mission, goals and objectives, and values,” points out Dr. Simone. “It de-emphasizes personal agendas, which may develop if an individual was looking to move on to another practice or up the ladder at the expense of the practice and fellow providers, and allows the practice team to gel over time. This is in some ways similar to a professional sports team, where chemistry and trust in one’s teammates are created over time.”
You can get your own hospitalist team to gel by retaining physicians for years if you initiate a program with that very goal.
How-Tos of Retention Programs
“There are a lot of [hospitalist] programs that haven’t developed retention programs at the outset,” says Dr. Simone. “They may be behind the eight ball, but they can and should create one. Successful programs identify their practice mission, values, and objectives, and clearly and concisely spell them out. This policy can then be utilized with the existing staff to align the team’s values and can also be used in recruiting future candidates.”
Once you have a solid written mission and vision statement, check to see if your hospitalists share the same values. Have your clinical director or an administrator sit down with providers one-on-one and find out their vision, values, and objectives. If what you hear differs from the core values of the practice, then you must develop a plan on which you can all agree.
“You may also have to consider altering some of the program’s vision and objectives, if appropriate,” says Dr. Simone.
Scheduling: A Core Value
Your group’s values can be reflected in the schedule you set for staff. “The practice structure and schedule plays a very important role in provider retention,” says Dr. Simone. “In general, various schedule types work for different individuals, and—in all probability—the provider will seek out the practices that offer a particular schedule to their liking.”
A hospital group that values time over money may offer larger chunks of time off. “We’ve found that our recruitment and retention improved when we went to a schedule of seven days on, seven off,” says Dr. Simone. “A lot of individuals are attracted to this because it gives them a week at a time to spend with their families or to pursue other interests, such as travel or educational pursuits.”
Whatever schedule you choose, there are some basic tenets Dr. Simone recommends, including:
- Create a schedule that is consistent and stable rather than constantly changing;
- Make sure the schedule is perceived as fair for all providers;
- Ensure that all providers get appropriate time off;
- Give providers enough flexibility to participate in other projects such as teaching, subspecialty clinics, administrative duties, or special projects; and
- Adhere to a schedule that promotes/accommodates a safe patient to provider ratio.
Salary and Bonuses
Money does matter in retention. As long as the pay you offer is perceived as fair, you have a good start. “In the end, you can only afford what your finances dictate,” says Dr. Simone. “Smaller hospitals may fall short on salary, so it’s important for them to recognize their strengths and sell them in order to compete.”
Your hospitalists may be attracted to participate in an incentive program that rewards them for hard work and productivity. “Incentives help change behavior, and people are stimulated when they have direct control over their own pay,” says Dr. Simone. “There are hospitalist programs with incentive plans, but many programs aren’t sure how to incentivize. You don’t want to reward doctors solely on the amount of work they do.”
For instance, a hospital-based program that rewards hospitalists on the basis of how many patients they admit is basically encouraging them to hospitalize every patient they see.
“I recommend finding a way to reward quality work and dedication, while not neglecting productivity,” says Dr. Simone. “In my opinion, the focus needs to be on increasing the program’s ability to standardize care following evidence-based protocols, encouraging participation in the value-added services that hospitalists are so good at, like participating in a rapid response team or a code blue team, acting as hospital leaders, educating hospital staff and residents, etc.”
Feeling Connected
Unlike many other physicians, hospitalists don’t get many opportunities to connect with patients or a community.
“In my opinion, a hospitalist’s professional job satisfaction and retention is influenced by the perception of feeling connected to the practice and providers, patients, colleagues, and the hospital,” says Dr. Simone. “There are various characteristics of an employment arrangement that may help an individual feel connected. When an employee feels connected, he/she will typically dedicate themselves to the mission of the company and perform at or above expectations.”
Create or revisit your group’s retention program today. By ensuring that the values and objectives of your practice are clearly stated, and catering to those values and objectives in scheduling and other management practices, you can begin to build your retention. TH
Jane Jerrard writes the “Career Development” column every month for The Hospitalist.
Retaining good hospitalists is one of the major factors in building a successful hospital medicine group—but it’s also one of the biggest challenges faced in the industry today. Why is hospitalist retention a problem, and what can be done to ensure your hospitalists stay for the long haul?
“As in any profession, there are some [hospitalists] who constantly look for bigger and better opportunities in the employment world,” admits Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Sometimes this involves individuals looking for a better practice fit or for a better financial compensation package. In addition, hospitalist medicine can lead to burnout if the practice is not created or operated in a prudent manner, thus leading to turnover.”
Retention Is Crucial
Why is it so important to retain your hospitalists? For one thing, keeping physicians in your program for the long term can directly decrease costs, time, and effort related to recruitment and training.
More importantly, by decreasing staff turnover, retention can stabilize your hospitalist program. “A stable staff is influential in maintaining the providers’ focus on the practice mission, goals and objectives, and values,” points out Dr. Simone. “It de-emphasizes personal agendas, which may develop if an individual was looking to move on to another practice or up the ladder at the expense of the practice and fellow providers, and allows the practice team to gel over time. This is in some ways similar to a professional sports team, where chemistry and trust in one’s teammates are created over time.”
You can get your own hospitalist team to gel by retaining physicians for years if you initiate a program with that very goal.
How-Tos of Retention Programs
“There are a lot of [hospitalist] programs that haven’t developed retention programs at the outset,” says Dr. Simone. “They may be behind the eight ball, but they can and should create one. Successful programs identify their practice mission, values, and objectives, and clearly and concisely spell them out. This policy can then be utilized with the existing staff to align the team’s values and can also be used in recruiting future candidates.”
Once you have a solid written mission and vision statement, check to see if your hospitalists share the same values. Have your clinical director or an administrator sit down with providers one-on-one and find out their vision, values, and objectives. If what you hear differs from the core values of the practice, then you must develop a plan on which you can all agree.
“You may also have to consider altering some of the program’s vision and objectives, if appropriate,” says Dr. Simone.
Scheduling: A Core Value
Your group’s values can be reflected in the schedule you set for staff. “The practice structure and schedule plays a very important role in provider retention,” says Dr. Simone. “In general, various schedule types work for different individuals, and—in all probability—the provider will seek out the practices that offer a particular schedule to their liking.”
A hospital group that values time over money may offer larger chunks of time off. “We’ve found that our recruitment and retention improved when we went to a schedule of seven days on, seven off,” says Dr. Simone. “A lot of individuals are attracted to this because it gives them a week at a time to spend with their families or to pursue other interests, such as travel or educational pursuits.”
Whatever schedule you choose, there are some basic tenets Dr. Simone recommends, including:
- Create a schedule that is consistent and stable rather than constantly changing;
- Make sure the schedule is perceived as fair for all providers;
- Ensure that all providers get appropriate time off;
- Give providers enough flexibility to participate in other projects such as teaching, subspecialty clinics, administrative duties, or special projects; and
- Adhere to a schedule that promotes/accommodates a safe patient to provider ratio.
Salary and Bonuses
Money does matter in retention. As long as the pay you offer is perceived as fair, you have a good start. “In the end, you can only afford what your finances dictate,” says Dr. Simone. “Smaller hospitals may fall short on salary, so it’s important for them to recognize their strengths and sell them in order to compete.”
Your hospitalists may be attracted to participate in an incentive program that rewards them for hard work and productivity. “Incentives help change behavior, and people are stimulated when they have direct control over their own pay,” says Dr. Simone. “There are hospitalist programs with incentive plans, but many programs aren’t sure how to incentivize. You don’t want to reward doctors solely on the amount of work they do.”
For instance, a hospital-based program that rewards hospitalists on the basis of how many patients they admit is basically encouraging them to hospitalize every patient they see.
“I recommend finding a way to reward quality work and dedication, while not neglecting productivity,” says Dr. Simone. “In my opinion, the focus needs to be on increasing the program’s ability to standardize care following evidence-based protocols, encouraging participation in the value-added services that hospitalists are so good at, like participating in a rapid response team or a code blue team, acting as hospital leaders, educating hospital staff and residents, etc.”
Feeling Connected
Unlike many other physicians, hospitalists don’t get many opportunities to connect with patients or a community.
“In my opinion, a hospitalist’s professional job satisfaction and retention is influenced by the perception of feeling connected to the practice and providers, patients, colleagues, and the hospital,” says Dr. Simone. “There are various characteristics of an employment arrangement that may help an individual feel connected. When an employee feels connected, he/she will typically dedicate themselves to the mission of the company and perform at or above expectations.”
Create or revisit your group’s retention program today. By ensuring that the values and objectives of your practice are clearly stated, and catering to those values and objectives in scheduling and other management practices, you can begin to build your retention. TH
Jane Jerrard writes the “Career Development” column every month for The Hospitalist.
Recruitment Revised
Recruiting hospitalists—or any other medical personnel—is all about supply and demand. Right now, the demand for hospitalists exceeds the supply. Many hospital medicine groups are growing rapidly, and more such groups are being created across the country. These groups are aggressively recruiting residents and physicians from the relatively small pool of hospitalists for hire, even as they lament the lack of candidates.
“Recruiting hospitalists is as competitive as I’ve ever seen,” says Vikas Parekh, MD, assistant professor and director, Non-House-staff Hospitalist Services, Department of Internal Medicine, University of Michigan, Ann Arbor. “This even trumps the primary care crisis of years ago.”
The Carrot: Repayment of Student Loans
Like many healthcare organizations today, the University of Michigan’s Department of Internal Medicine has a fast-growing hospitalist program, and continues to seek out additional physicians. “Our group of hospitalists went from zero to 16 by the end of this year—all in two years,” explains Dr. Parekh. “We’ve literally doubled each year.”
The university has implemented a unique method that provides an advantage against competition in recruiting new hospitalists. Beginning in 2006, they are offering a “loan forgiveness” program for new hires to their hospitalist program. Any hospitalist who joins the program this year can get up to $50,000 of student loans paid off by the university.
“The university did this about 10 years ago, when primary care had a similar problem,” recalls Dr. Parekh. “It was very successful.”
Hospitalists at the University of Michigan believe they have a unique benefit for recruitment. “I don’t know if any other hospitalist programs are doing this—there aren’t many [loan forgiveness programs] for physicians in general,” says Dr. Parekh.
How Loan Forgiveness Works
The University of Michigan loan forgiveness program will pay back any student loans—with a limit of $10,000 per year for five years. The university makes direct payments to the loaning institutions, which are typically federal government agencies. The newly hired physician is not under contract to stay until his or her loan is paid. “It works year to year,” explains Dr. Parekh.
The value of loan forgiveness can be overlooked. “People negotiate salary, but they don’t think of this,” says Scott A. Flanders, MD, associate professor and director, Hospitalist Program, Department of Internal Medicine, University of Michigan. “When you add up the value of benefits and loan forgiveness, that can add up to $50,000 to your compensation.”
Offering loan forgiveness on a set amount is more economical than offering a higher starting salary. The employer can set the cap on how much they’re willing to pay, thus controlling the investment in each new hire.
Recruitment Realities
The University of Michigan hospitalist program has been recruiting physicians through the university’s residency program, as well as advertisements in national journals.
“We’ve had a lot of success locally, but we’ve also seen response from around the country,” says Dr. Parekh. “We’ve had good success already; we’ve already recruited 75% of the physicians, in part due to the loan forgiveness program.”
The concept of lifting student loans from the shoulders of new physicians is a perfect fit for hospitalists in particular. “Hospital medicine is a young field, so by definition the physicians are young,” Dr. Parekh points out.
Dr. Flanders adds, “You’re not going to attract 40- or 50-year-old physicians who want to go into academics. But this [might] apply to someone shifting from one academic field to another.”
One problem that loan forgiveness can’t solve, however, is the number of residents choosing hospital medicine. “Internal medicine needs to get more people to pursue hospital medicine,” says Dr. Flanders. “And as it is, there’s only a small trickle of people pursuing internal medicine.”
The short supply of trained hospitalists severely affects the ability of hospital medicine groups to find and hire new physicians. Investing in value-added offerings such as loan forgiveness may prove worth the cost, if the investment brings quality candidates to your group. TH
Contributor Jane Jerrard regularly writes for “Career Development.”
Recruiting hospitalists—or any other medical personnel—is all about supply and demand. Right now, the demand for hospitalists exceeds the supply. Many hospital medicine groups are growing rapidly, and more such groups are being created across the country. These groups are aggressively recruiting residents and physicians from the relatively small pool of hospitalists for hire, even as they lament the lack of candidates.
“Recruiting hospitalists is as competitive as I’ve ever seen,” says Vikas Parekh, MD, assistant professor and director, Non-House-staff Hospitalist Services, Department of Internal Medicine, University of Michigan, Ann Arbor. “This even trumps the primary care crisis of years ago.”
The Carrot: Repayment of Student Loans
Like many healthcare organizations today, the University of Michigan’s Department of Internal Medicine has a fast-growing hospitalist program, and continues to seek out additional physicians. “Our group of hospitalists went from zero to 16 by the end of this year—all in two years,” explains Dr. Parekh. “We’ve literally doubled each year.”
The university has implemented a unique method that provides an advantage against competition in recruiting new hospitalists. Beginning in 2006, they are offering a “loan forgiveness” program for new hires to their hospitalist program. Any hospitalist who joins the program this year can get up to $50,000 of student loans paid off by the university.
“The university did this about 10 years ago, when primary care had a similar problem,” recalls Dr. Parekh. “It was very successful.”
Hospitalists at the University of Michigan believe they have a unique benefit for recruitment. “I don’t know if any other hospitalist programs are doing this—there aren’t many [loan forgiveness programs] for physicians in general,” says Dr. Parekh.
How Loan Forgiveness Works
The University of Michigan loan forgiveness program will pay back any student loans—with a limit of $10,000 per year for five years. The university makes direct payments to the loaning institutions, which are typically federal government agencies. The newly hired physician is not under contract to stay until his or her loan is paid. “It works year to year,” explains Dr. Parekh.
The value of loan forgiveness can be overlooked. “People negotiate salary, but they don’t think of this,” says Scott A. Flanders, MD, associate professor and director, Hospitalist Program, Department of Internal Medicine, University of Michigan. “When you add up the value of benefits and loan forgiveness, that can add up to $50,000 to your compensation.”
Offering loan forgiveness on a set amount is more economical than offering a higher starting salary. The employer can set the cap on how much they’re willing to pay, thus controlling the investment in each new hire.
Recruitment Realities
The University of Michigan hospitalist program has been recruiting physicians through the university’s residency program, as well as advertisements in national journals.
“We’ve had a lot of success locally, but we’ve also seen response from around the country,” says Dr. Parekh. “We’ve had good success already; we’ve already recruited 75% of the physicians, in part due to the loan forgiveness program.”
The concept of lifting student loans from the shoulders of new physicians is a perfect fit for hospitalists in particular. “Hospital medicine is a young field, so by definition the physicians are young,” Dr. Parekh points out.
Dr. Flanders adds, “You’re not going to attract 40- or 50-year-old physicians who want to go into academics. But this [might] apply to someone shifting from one academic field to another.”
One problem that loan forgiveness can’t solve, however, is the number of residents choosing hospital medicine. “Internal medicine needs to get more people to pursue hospital medicine,” says Dr. Flanders. “And as it is, there’s only a small trickle of people pursuing internal medicine.”
The short supply of trained hospitalists severely affects the ability of hospital medicine groups to find and hire new physicians. Investing in value-added offerings such as loan forgiveness may prove worth the cost, if the investment brings quality candidates to your group. TH
Contributor Jane Jerrard regularly writes for “Career Development.”
Recruiting hospitalists—or any other medical personnel—is all about supply and demand. Right now, the demand for hospitalists exceeds the supply. Many hospital medicine groups are growing rapidly, and more such groups are being created across the country. These groups are aggressively recruiting residents and physicians from the relatively small pool of hospitalists for hire, even as they lament the lack of candidates.
“Recruiting hospitalists is as competitive as I’ve ever seen,” says Vikas Parekh, MD, assistant professor and director, Non-House-staff Hospitalist Services, Department of Internal Medicine, University of Michigan, Ann Arbor. “This even trumps the primary care crisis of years ago.”
The Carrot: Repayment of Student Loans
Like many healthcare organizations today, the University of Michigan’s Department of Internal Medicine has a fast-growing hospitalist program, and continues to seek out additional physicians. “Our group of hospitalists went from zero to 16 by the end of this year—all in two years,” explains Dr. Parekh. “We’ve literally doubled each year.”
The university has implemented a unique method that provides an advantage against competition in recruiting new hospitalists. Beginning in 2006, they are offering a “loan forgiveness” program for new hires to their hospitalist program. Any hospitalist who joins the program this year can get up to $50,000 of student loans paid off by the university.
“The university did this about 10 years ago, when primary care had a similar problem,” recalls Dr. Parekh. “It was very successful.”
Hospitalists at the University of Michigan believe they have a unique benefit for recruitment. “I don’t know if any other hospitalist programs are doing this—there aren’t many [loan forgiveness programs] for physicians in general,” says Dr. Parekh.
How Loan Forgiveness Works
The University of Michigan loan forgiveness program will pay back any student loans—with a limit of $10,000 per year for five years. The university makes direct payments to the loaning institutions, which are typically federal government agencies. The newly hired physician is not under contract to stay until his or her loan is paid. “It works year to year,” explains Dr. Parekh.
The value of loan forgiveness can be overlooked. “People negotiate salary, but they don’t think of this,” says Scott A. Flanders, MD, associate professor and director, Hospitalist Program, Department of Internal Medicine, University of Michigan. “When you add up the value of benefits and loan forgiveness, that can add up to $50,000 to your compensation.”
Offering loan forgiveness on a set amount is more economical than offering a higher starting salary. The employer can set the cap on how much they’re willing to pay, thus controlling the investment in each new hire.
Recruitment Realities
The University of Michigan hospitalist program has been recruiting physicians through the university’s residency program, as well as advertisements in national journals.
“We’ve had a lot of success locally, but we’ve also seen response from around the country,” says Dr. Parekh. “We’ve had good success already; we’ve already recruited 75% of the physicians, in part due to the loan forgiveness program.”
The concept of lifting student loans from the shoulders of new physicians is a perfect fit for hospitalists in particular. “Hospital medicine is a young field, so by definition the physicians are young,” Dr. Parekh points out.
Dr. Flanders adds, “You’re not going to attract 40- or 50-year-old physicians who want to go into academics. But this [might] apply to someone shifting from one academic field to another.”
One problem that loan forgiveness can’t solve, however, is the number of residents choosing hospital medicine. “Internal medicine needs to get more people to pursue hospital medicine,” says Dr. Flanders. “And as it is, there’s only a small trickle of people pursuing internal medicine.”
The short supply of trained hospitalists severely affects the ability of hospital medicine groups to find and hire new physicians. Investing in value-added offerings such as loan forgiveness may prove worth the cost, if the investment brings quality candidates to your group. TH
Contributor Jane Jerrard regularly writes for “Career Development.”
Meeting Expectations
Spring is in the air: Flowers are blooming, trees are budding, and the SHM Annual Meeting is fast approaching.
Held Wednesday, May 3, through Friday, May 5, 2006, in Washington, D.C., the 9th Annual Meeting will include comprehensive education designed for hospitalists, networking with physicians from around the country, and chatting with your representatives in Congress. (See “Legislative Advocacy Day Debuts,” p. 10.)
“The SHM Annual Meeting is the largest gathering of all the stakeholders in hospital medicine, presenting a unique networking opportunity,” says Larry Wellikson, MD, FACP, CEO of SHM. “In 2006 we’re using the meeting’s location in our nation’s capitol to help hospitalists to be advocates for their patients and their specialty by meeting with their elected Members of Congress.”
The focus of the meeting, as always, will be the education offered. “Whatever your specialty, this meeting allows you to get something out of it,” says Alpesh Amin, MD, course director for the Annual Meeting. “There will be something for beginning hospitalists as well as more mature hospitalists. We’ll cover a lot of core topics.”
Education Covers Core Competencies
The basis for all education offered during the meeting is SHM’s new core competencies, developed by the Education Committee and released in January 2006. (The Core Competencies in Hospital Medicine: A Framework for Curriculum Development debuted in a supplement to the first issue of the Journal of Hospital Medicine.) The goal is to have these core competencies serve as the backbone for how hospitalists are recruited, trained, and certified in hospital medicine, as well as to standardize expectations for learning and proficiency.
“Our goal was to include [the core competencies] as a base for developing sessions, workshops, and lectures” at the Annual Meeting, says Dr. Amin. “We’re asking speakers to incorporate relevant core competencies into their lectures.”
To learn more about the new framework, Annual Meeting attendees can come to a session about the core competencies offered on Thursday, May 4 from 10:10 to 10:35 a.m.
Choose from Multiple Learning Tracks
Attendees at the Annual Meeting can customize their educational experience by choosing sessions from one or more of six general tracks:
Adult clinical: This track emphasizes recent advances that should be incorporated into the hospitalist’s approach to clinical care delivery. Sessions will cover diabetes management, acute coronary syndromes, chronic heart failure, addiction medicine, resuscitation, and much more.
Pediatric clinical: This track covers pediatric hospitalist practice management as well as current clinical issues. Sessions will cover controversies surrounding management of respiratory illnesses and the febrile infant, as well as practice management topics such as contract and salary negotiation and billing and coding.
Academic: This track covers the unique challenges faced by hospitalists in academic medical centers, including dealing with the 80-hour workweek and developing a curriculum for quality improvement and patient safety. The track also covers how to structure a research project and how to write for scientific publications.
Quality: This track addresses the imperative around development and implementation of improvement efforts in the hospital. Practical sessions cover improving physician/nurse communication, rapid response teams, and improving VTE prophylaxis.
Operational: This track covers some of the latest information and ideas for organizational infrastructure in topics such as value-added services, hospitalist burnout, performance management and advances in staffing projections.
New track! Developmental: This new track focuses on career satisfaction, building palliative care services, creating a hospitalist procedure service, and developing and implementing a perioperative care and consultative medicine program.
Regardless of which track or tracks you choose, you’ll have ample opportunity to improve your clinical skills, address operational issues with possible solutions for your hospital medicine group, and be prepared to lead change and innovation at your hospital.
Attendees should also note: You can earn a maximum of 13.25 category 1 credits toward the AMA Physician’s Recognition Award—plus additional credits for pre-courses. (See “Four Pre-Courses Offer In-Depth Education,” above.)
Nationwide Networking
In addition to dozens of educational sessions, the Annual Meeting includes many opportunities to network with colleagues from across the country, including leading experts and trendsetters. Networking events provide natural settings to search for a job or potential candidate, make connections, and get answers to clinical and organizational dilemmas. You can also network with more than 100 exhibitors in the Exhibit Hall to find new information and solutions.
“The networking aspect is beneficial,” says Dr. Amin. “The Mentorship Breakfast on the second day is particularly valuable.” The Mentorship Breakfast matches new or aspiring hospitalists—or those experiencing new challenges in their practice—with experienced hospitalist mentors for small-group discussions. Pre-registration is required for the breakfast. (For more information, visit www.hospitalmedicine.org.)
Another excellent event for networking is Thursday afternoon’s Special Interest Forums. Meet hospitalists with similar interests:
- Community-based hospitalists;
- Medical directors/leadership;
- Pediatric hospitalists;
- Family practice hospitalists;
- Geriatric hospitalists;
- Women in hospital medicine;
- Early career hospitalists;
- Nurse practitioners and physician assistants;
- Education;
- Research; and
- History of medicine.
In addition to the Special Interest Forums, you’ll have the opportunity to meet other hospitalists at a “town hall meeting.” Scheduled for Friday, the town hall meeting will feature a facilitated discussion of pressing topics in hospital medicine, as chosen by those in attendance.
Whether you attend the meeting or not, rest assured that everyone who comes to Washington, D.C., in May will help to advance the profession through learning the new core competencies, through sharing ideas and solutions, and through continuing to make an impact as hospitalists.
For more information on the Annual Meeting and to register online, visit www.hospitalmedicine.org. TH
Spring is in the air: Flowers are blooming, trees are budding, and the SHM Annual Meeting is fast approaching.
Held Wednesday, May 3, through Friday, May 5, 2006, in Washington, D.C., the 9th Annual Meeting will include comprehensive education designed for hospitalists, networking with physicians from around the country, and chatting with your representatives in Congress. (See “Legislative Advocacy Day Debuts,” p. 10.)
“The SHM Annual Meeting is the largest gathering of all the stakeholders in hospital medicine, presenting a unique networking opportunity,” says Larry Wellikson, MD, FACP, CEO of SHM. “In 2006 we’re using the meeting’s location in our nation’s capitol to help hospitalists to be advocates for their patients and their specialty by meeting with their elected Members of Congress.”
The focus of the meeting, as always, will be the education offered. “Whatever your specialty, this meeting allows you to get something out of it,” says Alpesh Amin, MD, course director for the Annual Meeting. “There will be something for beginning hospitalists as well as more mature hospitalists. We’ll cover a lot of core topics.”
Education Covers Core Competencies
The basis for all education offered during the meeting is SHM’s new core competencies, developed by the Education Committee and released in January 2006. (The Core Competencies in Hospital Medicine: A Framework for Curriculum Development debuted in a supplement to the first issue of the Journal of Hospital Medicine.) The goal is to have these core competencies serve as the backbone for how hospitalists are recruited, trained, and certified in hospital medicine, as well as to standardize expectations for learning and proficiency.
“Our goal was to include [the core competencies] as a base for developing sessions, workshops, and lectures” at the Annual Meeting, says Dr. Amin. “We’re asking speakers to incorporate relevant core competencies into their lectures.”
To learn more about the new framework, Annual Meeting attendees can come to a session about the core competencies offered on Thursday, May 4 from 10:10 to 10:35 a.m.
Choose from Multiple Learning Tracks
Attendees at the Annual Meeting can customize their educational experience by choosing sessions from one or more of six general tracks:
Adult clinical: This track emphasizes recent advances that should be incorporated into the hospitalist’s approach to clinical care delivery. Sessions will cover diabetes management, acute coronary syndromes, chronic heart failure, addiction medicine, resuscitation, and much more.
Pediatric clinical: This track covers pediatric hospitalist practice management as well as current clinical issues. Sessions will cover controversies surrounding management of respiratory illnesses and the febrile infant, as well as practice management topics such as contract and salary negotiation and billing and coding.
Academic: This track covers the unique challenges faced by hospitalists in academic medical centers, including dealing with the 80-hour workweek and developing a curriculum for quality improvement and patient safety. The track also covers how to structure a research project and how to write for scientific publications.
Quality: This track addresses the imperative around development and implementation of improvement efforts in the hospital. Practical sessions cover improving physician/nurse communication, rapid response teams, and improving VTE prophylaxis.
Operational: This track covers some of the latest information and ideas for organizational infrastructure in topics such as value-added services, hospitalist burnout, performance management and advances in staffing projections.
New track! Developmental: This new track focuses on career satisfaction, building palliative care services, creating a hospitalist procedure service, and developing and implementing a perioperative care and consultative medicine program.
Regardless of which track or tracks you choose, you’ll have ample opportunity to improve your clinical skills, address operational issues with possible solutions for your hospital medicine group, and be prepared to lead change and innovation at your hospital.
Attendees should also note: You can earn a maximum of 13.25 category 1 credits toward the AMA Physician’s Recognition Award—plus additional credits for pre-courses. (See “Four Pre-Courses Offer In-Depth Education,” above.)
Nationwide Networking
In addition to dozens of educational sessions, the Annual Meeting includes many opportunities to network with colleagues from across the country, including leading experts and trendsetters. Networking events provide natural settings to search for a job or potential candidate, make connections, and get answers to clinical and organizational dilemmas. You can also network with more than 100 exhibitors in the Exhibit Hall to find new information and solutions.
“The networking aspect is beneficial,” says Dr. Amin. “The Mentorship Breakfast on the second day is particularly valuable.” The Mentorship Breakfast matches new or aspiring hospitalists—or those experiencing new challenges in their practice—with experienced hospitalist mentors for small-group discussions. Pre-registration is required for the breakfast. (For more information, visit www.hospitalmedicine.org.)
Another excellent event for networking is Thursday afternoon’s Special Interest Forums. Meet hospitalists with similar interests:
- Community-based hospitalists;
- Medical directors/leadership;
- Pediatric hospitalists;
- Family practice hospitalists;
- Geriatric hospitalists;
- Women in hospital medicine;
- Early career hospitalists;
- Nurse practitioners and physician assistants;
- Education;
- Research; and
- History of medicine.
In addition to the Special Interest Forums, you’ll have the opportunity to meet other hospitalists at a “town hall meeting.” Scheduled for Friday, the town hall meeting will feature a facilitated discussion of pressing topics in hospital medicine, as chosen by those in attendance.
Whether you attend the meeting or not, rest assured that everyone who comes to Washington, D.C., in May will help to advance the profession through learning the new core competencies, through sharing ideas and solutions, and through continuing to make an impact as hospitalists.
For more information on the Annual Meeting and to register online, visit www.hospitalmedicine.org. TH
Spring is in the air: Flowers are blooming, trees are budding, and the SHM Annual Meeting is fast approaching.
Held Wednesday, May 3, through Friday, May 5, 2006, in Washington, D.C., the 9th Annual Meeting will include comprehensive education designed for hospitalists, networking with physicians from around the country, and chatting with your representatives in Congress. (See “Legislative Advocacy Day Debuts,” p. 10.)
“The SHM Annual Meeting is the largest gathering of all the stakeholders in hospital medicine, presenting a unique networking opportunity,” says Larry Wellikson, MD, FACP, CEO of SHM. “In 2006 we’re using the meeting’s location in our nation’s capitol to help hospitalists to be advocates for their patients and their specialty by meeting with their elected Members of Congress.”
The focus of the meeting, as always, will be the education offered. “Whatever your specialty, this meeting allows you to get something out of it,” says Alpesh Amin, MD, course director for the Annual Meeting. “There will be something for beginning hospitalists as well as more mature hospitalists. We’ll cover a lot of core topics.”
Education Covers Core Competencies
The basis for all education offered during the meeting is SHM’s new core competencies, developed by the Education Committee and released in January 2006. (The Core Competencies in Hospital Medicine: A Framework for Curriculum Development debuted in a supplement to the first issue of the Journal of Hospital Medicine.) The goal is to have these core competencies serve as the backbone for how hospitalists are recruited, trained, and certified in hospital medicine, as well as to standardize expectations for learning and proficiency.
“Our goal was to include [the core competencies] as a base for developing sessions, workshops, and lectures” at the Annual Meeting, says Dr. Amin. “We’re asking speakers to incorporate relevant core competencies into their lectures.”
To learn more about the new framework, Annual Meeting attendees can come to a session about the core competencies offered on Thursday, May 4 from 10:10 to 10:35 a.m.
Choose from Multiple Learning Tracks
Attendees at the Annual Meeting can customize their educational experience by choosing sessions from one or more of six general tracks:
Adult clinical: This track emphasizes recent advances that should be incorporated into the hospitalist’s approach to clinical care delivery. Sessions will cover diabetes management, acute coronary syndromes, chronic heart failure, addiction medicine, resuscitation, and much more.
Pediatric clinical: This track covers pediatric hospitalist practice management as well as current clinical issues. Sessions will cover controversies surrounding management of respiratory illnesses and the febrile infant, as well as practice management topics such as contract and salary negotiation and billing and coding.
Academic: This track covers the unique challenges faced by hospitalists in academic medical centers, including dealing with the 80-hour workweek and developing a curriculum for quality improvement and patient safety. The track also covers how to structure a research project and how to write for scientific publications.
Quality: This track addresses the imperative around development and implementation of improvement efforts in the hospital. Practical sessions cover improving physician/nurse communication, rapid response teams, and improving VTE prophylaxis.
Operational: This track covers some of the latest information and ideas for organizational infrastructure in topics such as value-added services, hospitalist burnout, performance management and advances in staffing projections.
New track! Developmental: This new track focuses on career satisfaction, building palliative care services, creating a hospitalist procedure service, and developing and implementing a perioperative care and consultative medicine program.
Regardless of which track or tracks you choose, you’ll have ample opportunity to improve your clinical skills, address operational issues with possible solutions for your hospital medicine group, and be prepared to lead change and innovation at your hospital.
Attendees should also note: You can earn a maximum of 13.25 category 1 credits toward the AMA Physician’s Recognition Award—plus additional credits for pre-courses. (See “Four Pre-Courses Offer In-Depth Education,” above.)
Nationwide Networking
In addition to dozens of educational sessions, the Annual Meeting includes many opportunities to network with colleagues from across the country, including leading experts and trendsetters. Networking events provide natural settings to search for a job or potential candidate, make connections, and get answers to clinical and organizational dilemmas. You can also network with more than 100 exhibitors in the Exhibit Hall to find new information and solutions.
“The networking aspect is beneficial,” says Dr. Amin. “The Mentorship Breakfast on the second day is particularly valuable.” The Mentorship Breakfast matches new or aspiring hospitalists—or those experiencing new challenges in their practice—with experienced hospitalist mentors for small-group discussions. Pre-registration is required for the breakfast. (For more information, visit www.hospitalmedicine.org.)
Another excellent event for networking is Thursday afternoon’s Special Interest Forums. Meet hospitalists with similar interests:
- Community-based hospitalists;
- Medical directors/leadership;
- Pediatric hospitalists;
- Family practice hospitalists;
- Geriatric hospitalists;
- Women in hospital medicine;
- Early career hospitalists;
- Nurse practitioners and physician assistants;
- Education;
- Research; and
- History of medicine.
In addition to the Special Interest Forums, you’ll have the opportunity to meet other hospitalists at a “town hall meeting.” Scheduled for Friday, the town hall meeting will feature a facilitated discussion of pressing topics in hospital medicine, as chosen by those in attendance.
Whether you attend the meeting or not, rest assured that everyone who comes to Washington, D.C., in May will help to advance the profession through learning the new core competencies, through sharing ideas and solutions, and through continuing to make an impact as hospitalists.
For more information on the Annual Meeting and to register online, visit www.hospitalmedicine.org. TH