User login
Using antipsychotics in patients with dementia
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
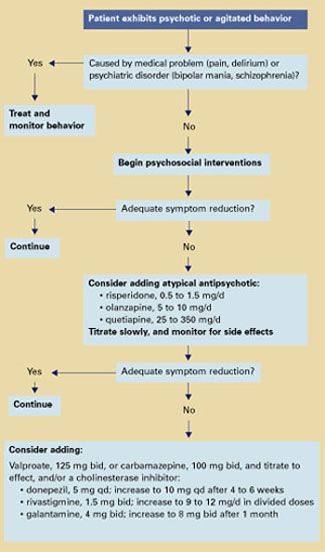
Algorithm Treating behavioral symptoms in patients with dementia
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
Algorithm Treating behavioral symptoms in patients with dementia
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
Algorithm Treating behavioral symptoms in patients with dementia
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|
Antipsychotic side effects
Atypical antipsychotics are more effective than conventional agents in treating negative symptoms and are associated with lower rates of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD).21
Tardive dyskinesia. All antipsychotics can cause TD, although the risk is about 10 times greater with conventionals than atypicals. With conventionals, the annual cumulative TD incidence for young adults is 4 to 5%,22 and rates are much higher for middle-aged and older adults receiving chronic therapy:
- 29% after 1 year
- 50% after 2 years
- 63% after 3 years.23
In older patients, use atypical rather than conventional antipsychotics to minimize TD risk. Observe carefully; if TD symptoms occur, cautiously withdraw the antipsychotic and consider trying another agent.
Other risks. Atypical antipsychotics may cause sedation, orthostatic hypotension (with an increased risk for falls), increased serum prolactin, and weight gain (Table 2).
Weight gain from atypical antipsychotics has been associated with adverse effects on glucose metabolism and increased risk for type 2 diabetes.24 Some might argue that weight gain associated with olanzapine and other atypicals might benefit low-weight older patients. The frail elderly need to increase muscle mass, however, and the atypicals are associated with increases in fat mass.
Increased serum prolactin with risperidone theoretically could lead to loss of bone density, but evidence of this effect in older patients does not exist.
Start low, go slow
Clozapine may help control treatment-resistant psychosis in patients with schizophrenia and manage patients with severe TD.25 However, clozapine’s increased risk of agranulocytosis, neurologic side effects (seizures, sedation, confusion), and anticholinergic effects limit its use in older patients, particularly those with neurodegenerative disorders (Table 2).
Dosing. In rare cases when using clozapine in older patients, start with 6.25 to 12.5 mg/d. Increase by 6.25 to 12.5 mg once or twice a week to 50 to 100 mg/d.
Risperidone has been used to treat agitation in older patients with dementia in two small studies:
In a 9-week, open-label trial, 15 patients (mean age 78) with dementia were given risperidone, 0.5 to 3 mg/d. Agitation improved significantly, as measured by the Cohen-Mansfield Agitation Inventory (CMAI)—a 29-item questionnaire completed by caregivers.26 CMAI scores at study’s end averaged 49.5, compared with 70.5 at baseline.27
A 12-week, placebo-controlled, doubleblind study examined risperidone—0.5, 1, or 2 mg/d—in 625 institutionalized patients (mean age 83) with dementia and agitation. Ninety-six patients had Functional Assessment Staging Rating Scale scores of 6A, indicating moderate to severe dementia. In patients receiving risperidone, these behavioral measures were significantly reduced:
- Behavior Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD) total scores, which measure behavior severity
- BEHAVE-AD psychosis subscale scores
- BEHAVE-AD aggressiveness scores
- CMAI verbal and aggression scores.
Adverse effects were reported at 82% for all three risperidone dosages and 85% for placebo. Side effects including somnolence, EPS, and peripheral edema were dose-related.12
Another trial compared risperidone or haloperidol, 0.5 to 4 mg/d, with placebo in treating 344 patients with behavioral symptoms of dementia. After 12 weeks of risperidone, mean dosage 1.1 mg/d:
- mean total BEHAVE-AD score decreased by 53%, compared with 37% in the placebo group
- CMAI score decreased by 32%, compared with 18% in the placebo group.
EPS were more severe with haloperidol than with risperidone or placebo.28
Risk of stroke. A small but significantly increased incidence of stroke and stroke-like events was recently reported in older patients with dementia when treated with risperidone. These events occurred in double-blind, placebocontrolled trials in patients (mean age 82) with Alzheimer’s, vascular, and mixed dementias.
Pharmacokinetic changes can influence concentrations of drugs in tissue compartments over time. Drug absorption declines with normal aging, but a clinically significant decrease in total absorption of psychotropics appears not to occur.13
In the liver, lipid-soluble psychotropics are metabolized into pharmacologically active or inactive metabolites. Some metabolic pathways, such as demethylation, may be influenced by age, leading to increased plasma concentrations of drugs and their metabolites.14,15 However, hydroxylation tends not to be affected by age.16
The ratio of body fat to water increases with aging,13 increasing the volume of distribution for lipid-soluble psychotropics. An age-related decrease in glomerular filtration accounts in part for increased accumulation of hydrophilic metabolites in some older patients.17,18
Pharmacodynamic changes with aging occur in neurotransmitter systems within cellular processing, such as at receptor or reuptake levels.19 These changes may exaggerate drug-drug interactions or affect complex neurotransmitter interactions.
The number of neurons in nigrostriatal pathways declines with age. Decreases are also seen in tyrosine hydroxylase activity, presynaptic dopamine D2 receptors, and dopamine levels—which may be particularly relevant to a discussion of antipsychotic medications.20
The net effect of these changes is the need to prescribe lower-than-usual starting and target dosages of many medications, including antipsychotics.
Most patients who experienced cerebrovascular events had one or more stroke risk factors, including diabetes, hypertension, atrial fibrillation, heart arrhythmia, atherosclerosis, or heart failure. They did not show a pattern of reduced blood pressure or orthostatic changes.12,29
Table 2
Antipsychotic side effects and dosages in older patients with dementia*
| Side effect | Clozapine (6.25 to 100 mg/d) | Risperidone (0.5 to 1.5 mg/d) | Olanzapine (5 to 10 mg/d) | Quetiapine (25 to 350 mg/d) |
|---|---|---|---|---|
| Orthostasis | ++++ | ++++ | +++ | ++ |
| Sedation | +++++ | ++ | +++ | ++ |
| Prolactin increase | 0 | +++ | + | 0 |
| Weight gain | ++++ | + | +++ | + |
| EPS | 0/+ | ++ | + | 0/+ |
| Tardive dyskinesia | 0 | + | + | ? |
| Anticholinergic effects | ++++ | + | + | 0 |
| Seizure risk | +++ | + | + | + |
| Hematologic effects | +++ | + | + | + |
| Source: Adapted from references 15 and 16. | ||||
| * Side-effect profiles and recommended dosages of ziprasidone and aripiprazole in older patients are not yet established. | ||||
| EPS: Extrapyramidal symptoms | ||||
| Key: | ||||
| 0 = none | ||||
| + = slight | ||||
| +++ = mild | ||||
| +++++ = marked | ||||
| 0/+ = none to slight | ||||
| ++ = very mild | ||||
| ++++ = moderate | ||||
Dosing. For older patients with dementia and psychosis, start risperidone at 0.25 to 0.5 mg/d and increase by no more than 0.25 to 0.5 mg once or twice per week. Do not exceed 3 mg/d. For agitation, a 1998 Expert Consensus Guideline Series panel2 recommended starting risperidone at 0.25 to 0.5 mg/d and increasing to an average of 0.5 to 1.5 mg/d.
Olanzapine. Two double-blind, placebo-controlled studies have examined olanzapine in treating agitation associated with dementia.
Saterlee et al30 compared olanzapine, mean 2.4 mg/d, with placebo in outpatients (mean age 79) with Alzheimer’s disease and psychosis. No significant differences were noted in hepatic transaminase levels, leukopenia, EPS, or orthostatic changes.
In a later study,13 nursing home patients (mean age 83) with Alzheimer’s disease, psychosis, and agitation were randomly assigned to receive olanzapine—5, 10, or 15 mg/d—or placebo. After 6 weeks, patients receiving olanzapine, 5 or 10 mg/d, showed significant improvement in Neuropsychiatric Inventory (NPI) total core scores. Olanzapine, 15 mg/d, was not significantly more effective than placebo.
Adverse events such as somnolence and abnormal gait occurred more often with olanzapine than placebo. The somnolence rate with olanzapine was 14% for 5 mg/d and 13% for 10 mg/d, compared with 3% for placebo. For abnormal gait, the rate with olanzapine was 11% for 5 mg/d and 7% for 10 mg/d, compared with 1% for placebo.
Dosing. Start olanzapine at 2.5 mg/d, and increase after 1 to 3 days to 5 mg/d. If symptoms are not adequately controlled, titrate by 2.5-mg increments to 10 mg/d.
Quetiapine. One open-label study14 examined using quetiapine in older patients with psychotic disorders. The study enrolled 184 patients (mean age 76) with Alzheimer’s disease, Parkinson’s disease, schizophrenia, vascular dementia, schizoaffective disorder, bipolar disorder, or major depression. Before the trial, patients were taking various conventional and atypical antipsychotics.
Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impressions (CGI) scores improved significantly after 52 weeks of quetiapine, median 137.5 mg/d. BPRS scores improved 20% in 49% of patients who completed the study.
Less than one-half (48%) of enrolled patients completed the study. Reasons for withdrawal included lack of efficacy (19%), adverse events or illness (15%; adverse events alone, 11%), lost to follow-up (13%), protocol noncompliance (3%), or diminished need for treatment (2%).
EPS occurred in 13% of patients. Mean total scores on the Simpson-Angus Rating Scale for Extrapyramidal Side Effects decreased 1.8 points, indicating reduced parkinsonian symptoms.
Dosing. Start quetiapine at 25 mg once at bedtime or bid; increase in 25-mg increments until the lowest effective dosage is achieved.
Ziprasidone. Little data exist on using ziprasidone in long-term care. In one recent study,31 ziprasidone (mean 100 mg/d) was given to 62 patients ages 64 to 92 with medical illnesses plus major depression, bipolar disorder, schizoaffective disorder, Alzheimer’s disease, or multi-infarct dementia. A retrospective chart review of 10 patients showed decreased agitation, as mean NPI scores declined from 76 to 33.
Sedation was the most common side effect. QTc findings, postural hypotension, and syncope rates did not change. Despite its limitations, this study suggests that ziprasidone is safe and effective in treating psychosis associated with dementia or other disorders.
Aripiprazole. As with ziprasidone, little data exist to guide the use of aripiprazole in older patients. In a randomized preliminary trial,32 192 noninstitutionalized patients with Alzheimer’s disease and psychosis were treated for 10 weeks with aripiprazole, mean 10 mg/d, or placebo.
At 8 and 10 weeks, BPRS psychosis subscale scores improved significantly in patients taking aripiprazole, compared with placebo. EPS and akathisia improved, and somnolence was the most common side effect. Although this study enrolled noninstitutionalized patients with dementia, the results suggest that aripiprazole may help treat long-term care residents with neurodegenerative disorders and behavioral disturbances.
Related resources
- Zaraa AS. Dementia update: Pharmacologic management of agitation and psychosis in older demented patients. Geriatrics 2003;58(10):48-53.
- Mills EJ, Chow TW. Randomized controlled trials in long-term care of residents with dementia: a systematic review. J Am Med Dir Assoc 2003;4(6):302-7.
- Alzheimer’s Association. Treating agitation. www.alz.org/PhysCare/Treating/agitation.htm
Drug brand names
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Donepezil • Aricept
- Galantamine • Reminyl
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Kasckow receives research support from, is a consultant to, or is a speaker for Eli Lilly & Co., Forest Laboratories, Solvay Pharmaceuticals, AstraZeneca Pharmaceuticals, Organon, Janssen Pharmaceutica, and Pfizer Inc.
Dr. Mulchahey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Mohamed receives research support form Forest Laboratories and is a speaker for Eli Lilly & Co.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.
1. Finkel S, Costa e Silva J, Cohen G, et al. Behavioral and psychological symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Am J Geriatr Psychiatry 1998;6:97-100.
2. The Expert Consensus Panel for Agitation in Dementia. Treatment of agitation in older persons with dementia. Postgrad Med 1998;4(suppl):1-88.
3. Cohen-Mansfield J. Nonpharmacologic interventions for inappropriate behaviors in dementia: a review, summary, and critique. Am J Geriatr Psychiatry 2001;9(4):361-81.
4. Davidson J. Pharmacologic treatment. In: Busse E, Blazer D (eds). Textbook of geriatric psychiatry (2nd ed). Washington DC: American Psychiatric Publishing, 1996:359-79.
5. Nies A, Robinson DS, Friedman MJ, et al. Relationship between age and tricyclic antidepressant plasma levels. Am J Psychiatry 1977;134(7):790-3.
6. Greenblatt DJ, Shader RJ. Benzodiazepine kinetics in the elderly. In: Usdin E (ed). Clinical pharmacology in psychiatry. New York: Elsevier, 1981;174-81.
7. Pollock BG, Perel JM, Altieri LP, et al. Debrisoquine hydroxylation phenotyping in geriatric psychopharmacology. Psychopharmacol Bull. 1992;28(2):163-8.
8. Nelson JC, Atillasoy E, Mazure C, Jatlow PI. Hydroxydesipramine in the elderly. J Clin Psychopharmacol 1988;8(6):428-33.
9. Young RC, Alexopoulos GS, Shamoian CA, et al. Plasma 10-hydroxynortriptyline in elderly depressed patients. Clin Pharmacol Ther 1984;35(4):540-4.
10. Cantillon M, Molchan SE, Little J. Pharmacological and neuroendocrine probes in neuropsychiatric illness. In: Coffey CE, Cummings JL (eds). Textbook of geriatric neuropsychiatry. Washington, DC: American Psychiatric Publishing, 1994.
11. Young RC, Meyers BS. Psychopharmacology. In: Sadovoy J, Lazarus LW, Jarvik LF, Grossberg GT (eds). Comprehensive review of geriatric psychiatry. Washington DC: American Psychiatric Publishing, 1996;755-817.
12. Katz IR, Jeste DV, Mintzer JE, et al. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. J Clin Psychiatry 1999;60(2):107-15.
13. Street JS, Clark WS, Gannon KS, et al. Olanzapine treatment of psychotic and behavioral symptoms in patients with Alzheimer disease in nursing care facilities: a double-blind, randomized, placebo-controlled trial. The HGEU Study Group. Arch Gen Psychiatry 2000;57(10):968-76.
14. Tariot PN, Salzman C, Yeung PP, et al. Long-term use of quetiapine in elderly patients with psychotic disorders. Clin Ther 2000;22(9):1068-84.
15. Casey DE. The relationship of pharmacology to side effects. J Clin Psychiatry 1997;58(suppl):55-62.
16. Pickar D. Prospects for pharmacotherapy of schizophrenia. Lancet 1995;345:557-62.
17. Kasckow JW, McElroy SL, Cameron RL, et al. A pilot study on the use of divalproex sodium in the treatment of behavioral agitation in elderly patients with dementia: assessment with the BEHAVE-AD and CGI rating scales. Curr Ther Res 1997;58(12):981-9.
18. Tariot PN, Erb R, Podgorski CA, et al. Efficacy and tolerability of carbamazepine for agitation and aggression in dementia. Am J Psychiatry 1998;155(1):54-61.
19. Kasckow JW. Cognitive enhancers for dementia: do they work? Current Psychiatry 2002;1(3):22-8.
20. Lacy C, Armstrong L, Goldman M, Lance L. (eds) Lexicomp drug information handbook. Hudson, OH: Lexicomp, 2003-2004:1225-27, 1189-90, 1026-27.
21. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47(6):716-19.
22. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
23. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients. A prospective longitudinal study of 266 outpatients. Arch Gen Psychiatry 1995;52(9):756-65.
24. Sernyak MJ, Leslie DL, Alarcon RD, et al. Association of diabetes mellitus with use of atypical neuroleptics in the treatment of schizophrenia. Am J Psychiatry 2002;159:561-6.
25. Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. JGeriatr Psychiatry Neurol 1995;8(1):12-15.
26. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in the nursing home. J Gerontol 1989;44(3):M77-84.
27. Lavretsky H, Sultzer D. A structured trial of risperidone for the treatment of agitation in dementia. Am J Geriatr Psychiatry 1998;6(2):127-35.
28. De Deyn PP, Rabheru K, Rasmussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53(5):946-55.
29. Brodaty H, Ames D, Snowdon J, et al. A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003;64(2):134-43.
30. Satterlee W, Reams SG, Burns PR, et al. A clinical update on olanzapine treatment in schizophrenia and in elderly Alzheimer’s disease patients (abstract). Psychopharmacol Bull 1995;31:534.-
31. Berkowitz A. Ziprasidone for elderly dementia: a case series (abstract). San Francisco, CA: American Psychiatric Association annual meeting, 2003.
32. De Deyn PP, Jeste D, Auby P, Carson W. Aripiprazole in dementia of the Alzheimer’s type (abstract). Honolulu, HI: American Association for Geriatric Psychiatry annual meeting, 2003.