A 20-year-old woman with no significant medical history presented to the ED with a several-month history of worsening abdominal pain. She reported that although she previously had been evaluated at multiple EDs, no cause of her abdominal pain had been identified. The patient further noted that the pain had significantly increased the day of this presentation.
Figure 1
Physical examination revealed guarding and rebound tenderness in the midabdomen. Computed tomography (CT) studies of the abdomen and pelvis were performed; representative scout and axial images of the upper abdomen are shown above (Figures 1 and 2).
Figure 2What is the suspected diagnosis?
Answer
The scout image of the abdomen revealed a distended stomach (white arrows, Figure 3), which displaced multiple loops of small bowel into the lower abdomen. The axial image through the upper abdomen showed air and solid material within the distended stomach (white arrows, Figure 4). Multiple foci of extraluminal (free) air were seen anteriorly (white asterisks, Figure 4). A coronal reformat of the CT better demonstrated the distended stomach filled with debris (white arrows, Figure 5), extraluminal air (white asterisk, Figure 5), and pneumatosis (air within the walls of multiple small bowel loops; red arrows, Figure 5).
These findings indicated a bowel obstruction and perforation due to the presence of a gastric bezoar. Upon further questioning, the patient admitted to a stress-related habit of eating her own hair (trichophagia) over the past 3 to 4 months.
Figure 3
Bezoars
Gastric bezoars are aggregates of nondigestible material that collect within the gastrointestinal system, usually fruit/vegetable matter (phytobezoars) or hair (trichobezoars). Phytobezoars are most common in patients with a history of reduced gastric motility and/or prior gastric surgery. Trichobezoars, similar to the one seen in this case, typically occur in young women and/or patients with psychiatric illness.1
Gastric bezoars are typically located in the gastric body but may extend into the small bowel and cause bowel obstruction. Trichobezoars that extend into the small bowel are referred to as “Rapunzel syndrome” (based on the fairy tale of the princess with long hair).
Figure 4
Clinical Presentation
Patients with gastric bezoars often present to the ED with nonspecific complaints of abdominal pain, including early satiety, weight loss, signs of anemia, abdominal pain, bloating, and symptoms of small bowel obstruction (SBO).2 Obtaining a thorough history is important to identify trichophagia, as only a small percentage of patients have evidence of alopecia on examination.
Figure 5
Workup
The workup for patients with gastric bezoars typically involves multiple imaging modalities. While abdominal radiography may demonstrate distention of the stomach, these findings are often nonspecific, and the characteristic feature of a mass with a diffusely mottled appearance is visualized in less than 20% of cases.
Computed tomography is the test of choice for detecting a bezoar, with a reported sensitivity of 97%.3 This modality is also useful for assessing the size of a bezoar and evaluating for complications such as SBO, perforation (free-air), or pneumatosis—all of which were revealed on this patient’s CT studies.
Treatment
The treatment for patients with large or obstructing gastric bezoars is surgical resection; both open and laparoscopic techniques have been described in the literature.2,4 The patient in this case was admitted to the hospital, where she underwent surgical removal of the bezoar. She was discharged home on hospital day 6 with outpatient psychiatric follow-up.
References
1. Guniganti P, Bradenham CH, Raptis C, Menias CO, Mellnick VM. Radiographics. 2015;35(7):1909-1921. doi:10.1148/rg.2015150062. 2. Fallon SC, Slater BJ, Larimer EL, Brandt ML, Lopez ME. The surgical management of Rapunzel syndrome: a case series and literature review. J Pediatr Surg. 2013;48(4):830-834. doi:10.1016/j.jpedsurg.2012.07.046. 3. Ripollés T, García-Aguayo J, Martínez MJ, Gil P. Gastrointestinal Bezoars: Sonographic and CT Characteristics. AJR Am J Roentgenol. 2001;177(1):65-69. doi:10.2214/ajr.177.1.1770065. 4. Flaherty DC, Aguilar F, Pradhan B, Grewal H. Rapunzel syndrome due to ingested hair extensions: Surgical and psychiatric considerations. Int J Surg Case Rep. 2015;17:155-157. doi:10.1016/j.ijscr.2015.11.009.
An otherwise healthy 20-year-old woman presented for evaluation of severe chronic abdominal pain.
An otherwise healthy 20-year-old woman presented for evaluation of severe chronic abdominal pain.
A 20-year-old woman with no significant medical history presented to the ED with a several-month history of worsening abdominal pain. She reported that although she previously had been evaluated at multiple EDs, no cause of her abdominal pain had been identified. The patient further noted that the pain had significantly increased the day of this presentation.
Figure 1
Physical examination revealed guarding and rebound tenderness in the midabdomen. Computed tomography (CT) studies of the abdomen and pelvis were performed; representative scout and axial images of the upper abdomen are shown above (Figures 1 and 2).
Figure 2What is the suspected diagnosis?
Answer
The scout image of the abdomen revealed a distended stomach (white arrows, Figure 3), which displaced multiple loops of small bowel into the lower abdomen. The axial image through the upper abdomen showed air and solid material within the distended stomach (white arrows, Figure 4). Multiple foci of extraluminal (free) air were seen anteriorly (white asterisks, Figure 4). A coronal reformat of the CT better demonstrated the distended stomach filled with debris (white arrows, Figure 5), extraluminal air (white asterisk, Figure 5), and pneumatosis (air within the walls of multiple small bowel loops; red arrows, Figure 5).
These findings indicated a bowel obstruction and perforation due to the presence of a gastric bezoar. Upon further questioning, the patient admitted to a stress-related habit of eating her own hair (trichophagia) over the past 3 to 4 months.
Figure 3
Bezoars
Gastric bezoars are aggregates of nondigestible material that collect within the gastrointestinal system, usually fruit/vegetable matter (phytobezoars) or hair (trichobezoars). Phytobezoars are most common in patients with a history of reduced gastric motility and/or prior gastric surgery. Trichobezoars, similar to the one seen in this case, typically occur in young women and/or patients with psychiatric illness.1
Gastric bezoars are typically located in the gastric body but may extend into the small bowel and cause bowel obstruction. Trichobezoars that extend into the small bowel are referred to as “Rapunzel syndrome” (based on the fairy tale of the princess with long hair).
Figure 4
Clinical Presentation
Patients with gastric bezoars often present to the ED with nonspecific complaints of abdominal pain, including early satiety, weight loss, signs of anemia, abdominal pain, bloating, and symptoms of small bowel obstruction (SBO).2 Obtaining a thorough history is important to identify trichophagia, as only a small percentage of patients have evidence of alopecia on examination.
Figure 5
Workup
The workup for patients with gastric bezoars typically involves multiple imaging modalities. While abdominal radiography may demonstrate distention of the stomach, these findings are often nonspecific, and the characteristic feature of a mass with a diffusely mottled appearance is visualized in less than 20% of cases.
Computed tomography is the test of choice for detecting a bezoar, with a reported sensitivity of 97%.3 This modality is also useful for assessing the size of a bezoar and evaluating for complications such as SBO, perforation (free-air), or pneumatosis—all of which were revealed on this patient’s CT studies.
Treatment
The treatment for patients with large or obstructing gastric bezoars is surgical resection; both open and laparoscopic techniques have been described in the literature.2,4 The patient in this case was admitted to the hospital, where she underwent surgical removal of the bezoar. She was discharged home on hospital day 6 with outpatient psychiatric follow-up.
A 20-year-old woman with no significant medical history presented to the ED with a several-month history of worsening abdominal pain. She reported that although she previously had been evaluated at multiple EDs, no cause of her abdominal pain had been identified. The patient further noted that the pain had significantly increased the day of this presentation.
Figure 1
Physical examination revealed guarding and rebound tenderness in the midabdomen. Computed tomography (CT) studies of the abdomen and pelvis were performed; representative scout and axial images of the upper abdomen are shown above (Figures 1 and 2).
Figure 2What is the suspected diagnosis?
Answer
The scout image of the abdomen revealed a distended stomach (white arrows, Figure 3), which displaced multiple loops of small bowel into the lower abdomen. The axial image through the upper abdomen showed air and solid material within the distended stomach (white arrows, Figure 4). Multiple foci of extraluminal (free) air were seen anteriorly (white asterisks, Figure 4). A coronal reformat of the CT better demonstrated the distended stomach filled with debris (white arrows, Figure 5), extraluminal air (white asterisk, Figure 5), and pneumatosis (air within the walls of multiple small bowel loops; red arrows, Figure 5).
These findings indicated a bowel obstruction and perforation due to the presence of a gastric bezoar. Upon further questioning, the patient admitted to a stress-related habit of eating her own hair (trichophagia) over the past 3 to 4 months.
Figure 3
Bezoars
Gastric bezoars are aggregates of nondigestible material that collect within the gastrointestinal system, usually fruit/vegetable matter (phytobezoars) or hair (trichobezoars). Phytobezoars are most common in patients with a history of reduced gastric motility and/or prior gastric surgery. Trichobezoars, similar to the one seen in this case, typically occur in young women and/or patients with psychiatric illness.1
Gastric bezoars are typically located in the gastric body but may extend into the small bowel and cause bowel obstruction. Trichobezoars that extend into the small bowel are referred to as “Rapunzel syndrome” (based on the fairy tale of the princess with long hair).
Figure 4
Clinical Presentation
Patients with gastric bezoars often present to the ED with nonspecific complaints of abdominal pain, including early satiety, weight loss, signs of anemia, abdominal pain, bloating, and symptoms of small bowel obstruction (SBO).2 Obtaining a thorough history is important to identify trichophagia, as only a small percentage of patients have evidence of alopecia on examination.
Figure 5
Workup
The workup for patients with gastric bezoars typically involves multiple imaging modalities. While abdominal radiography may demonstrate distention of the stomach, these findings are often nonspecific, and the characteristic feature of a mass with a diffusely mottled appearance is visualized in less than 20% of cases.
Computed tomography is the test of choice for detecting a bezoar, with a reported sensitivity of 97%.3 This modality is also useful for assessing the size of a bezoar and evaluating for complications such as SBO, perforation (free-air), or pneumatosis—all of which were revealed on this patient’s CT studies.
Treatment
The treatment for patients with large or obstructing gastric bezoars is surgical resection; both open and laparoscopic techniques have been described in the literature.2,4 The patient in this case was admitted to the hospital, where she underwent surgical removal of the bezoar. She was discharged home on hospital day 6 with outpatient psychiatric follow-up.
References
1. Guniganti P, Bradenham CH, Raptis C, Menias CO, Mellnick VM. Radiographics. 2015;35(7):1909-1921. doi:10.1148/rg.2015150062. 2. Fallon SC, Slater BJ, Larimer EL, Brandt ML, Lopez ME. The surgical management of Rapunzel syndrome: a case series and literature review. J Pediatr Surg. 2013;48(4):830-834. doi:10.1016/j.jpedsurg.2012.07.046. 3. Ripollés T, García-Aguayo J, Martínez MJ, Gil P. Gastrointestinal Bezoars: Sonographic and CT Characteristics. AJR Am J Roentgenol. 2001;177(1):65-69. doi:10.2214/ajr.177.1.1770065. 4. Flaherty DC, Aguilar F, Pradhan B, Grewal H. Rapunzel syndrome due to ingested hair extensions: Surgical and psychiatric considerations. Int J Surg Case Rep. 2015;17:155-157. doi:10.1016/j.ijscr.2015.11.009.
References
1. Guniganti P, Bradenham CH, Raptis C, Menias CO, Mellnick VM. Radiographics. 2015;35(7):1909-1921. doi:10.1148/rg.2015150062. 2. Fallon SC, Slater BJ, Larimer EL, Brandt ML, Lopez ME. The surgical management of Rapunzel syndrome: a case series and literature review. J Pediatr Surg. 2013;48(4):830-834. doi:10.1016/j.jpedsurg.2012.07.046. 3. Ripollés T, García-Aguayo J, Martínez MJ, Gil P. Gastrointestinal Bezoars: Sonographic and CT Characteristics. AJR Am J Roentgenol. 2001;177(1):65-69. doi:10.2214/ajr.177.1.1770065. 4. Flaherty DC, Aguilar F, Pradhan B, Grewal H. Rapunzel syndrome due to ingested hair extensions: Surgical and psychiatric considerations. Int J Surg Case Rep. 2015;17:155-157. doi:10.1016/j.ijscr.2015.11.009.
Figure 3.A 49-year-old man with a history of human immunodeficiency virus infection, untreated hepatitis C, endocarditis, and bilateral total hip arthroplasty (THA) presented to the ED with fever, chills, and a nonproductive cough, which he stated began 2 days prior. The patient was not able to walk due to worsening low back and bilateral leg pain.
Laboratory studies revealed leukocytosis with a left shift. Chest radiographs were negative for pneumonia. A magnetic resonance image (MRI) of the lumbar spine was obtained to evaluate for diskitis osteomyelitis. A radiograph of the pelvis was also obtained to evaluate the patient’s THAs, and a computed tomography scan (CT) of the abdomen and pelvis with contrast was obtained for further evaluation. Representative CT, radiographic, and MRI images are shown at left (Figures 1-3).
What is the suspected diagnosis?
Answer
The MRI of the lumbar spine demonstrated no evidence of diskitis osteomyelitis. However, T2-weighted axial images showed enlarged heterogeneous bilateral psoas muscles with bright signal, indicating the presence of fluid (white arrows, Figure 4).
Figure 4.
Figure 5.
On the pelvic radiographs, both femoral heads appeared off-center within the acetabular cups (red arrows, Figure 5).This eccentric positioning indicated wear of the polyethylene in the THAs that normally occupies the space between the acetabular cup and the femoral head. In addition, focal lucency in the right acetabulum indicated breakdown of the bone, a condition referred to as osteolysis (white asterisk, Figure 5).
An abdominopelvic CT scan with contrast was performed and confirmed the findings of polyethylene wear and osteolysis. The CT scan also demonstrated large bilateral hip joint effusions (white arrows, Figure 6), decompressed along distended bilateral iliopsoas bursae (red asterisks, Figure 6), and communicating with the bilateral psoas muscle collections (red arrows, Figure 6).
Osteolysis With Iliopsoas Bursitis
Bursae are fluid-filled sacs lined by synovial tissue located throughout the body to reduce friction at sites of movement between muscles, bones, and tendons. Bursitis develops when these sacs become inflamed and/or infected and fill with fluid. The iliopsoas bursa lies between the anterior capsule of the hip and the psoas tendon, iliacus tendon, and muscle fibers.1,2 This bursa frequently communicates with the hip joint.3,4 Iliopsoas bursal distension has been reported following THA in the setting of polyethylene wear,5 and aseptic bursitis is a commonly seen incidental finding at the time of revision surgery.6
Figure 6.
In this patient, long-standing polyethylene-induced synovitis had markedly expanded the hip joints and iliopsoas bursae, eventually resulting in superinfection, which accounted for the patient’s symptoms.
Treatment
Based on the imaging findings, interventional radiology services were contacted. The interventional radiologist drained the bilateral psoas abscesses. Cultures of the fluid were positive for both methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-susceptible S aureus (MSSA). The patient was admitted to the hospital for treatment of MRSA and MSSA with intravenous antibiotic therapy. He recovered from the infection and was discharged on hospital day 2, with instructions to follow up with an orthopedic surgeon to discuss eventual revision of the bilateral THAs.
References
1. Chandler SB. The iliopsoas bursa in man. Anatom Record. 1934;58(3),235-240. doi:10.1002/ar.1090580304. 2. Tatu L, Parratte B, Vuillier F, Diop M, Monnier G. Descriptive anatomy of the femoral portion of the iliopsoas muscle. Anatomical basis of anterior snapping of the hip. Surg Radiol Anat. 2001;23(6):371-374. 3. Meaney JF, Cassar-Pullicino VN, Etherington R, Ritchie DA, McCall IW, Whitehouse GH. Ilio-psoas bursa enlargement. Clin Radiol. 1992;45(3):161-168. 4. Warren R, Kaye JJ, Salvati EA. Arthrographic demonstration of an enlarged iliopsoas bursa complicating osteoarthritis of the hip. A case report. J Bone Joint Surg Am. 1975;57(3):413-415. 5. Cheung YM, Gupte CM, Beverly MJ. Iliopsoas bursitis following total hip replacement. Arch Orthop Trauma Surg. 2004;124(10):720-723. Epub 2004 Oct 23. doi:10.1007/s00402-004-0751-9. 6. Howie DW, Cain CM, Cornish BL. Pseudo-abscess of the psoas bursa in failed double-cup arthroplasty of the hip. J Bone Joint Surg Br. 1991;73:29-32.
A 49-year-old man with multiple comorbidities presented with a 2-day history of fever and nonproductive cough.
A 49-year-old man with multiple comorbidities presented with a 2-day history of fever and nonproductive cough.
Figure 1.
Figure 2.
Figure 3.A 49-year-old man with a history of human immunodeficiency virus infection, untreated hepatitis C, endocarditis, and bilateral total hip arthroplasty (THA) presented to the ED with fever, chills, and a nonproductive cough, which he stated began 2 days prior. The patient was not able to walk due to worsening low back and bilateral leg pain.
Laboratory studies revealed leukocytosis with a left shift. Chest radiographs were negative for pneumonia. A magnetic resonance image (MRI) of the lumbar spine was obtained to evaluate for diskitis osteomyelitis. A radiograph of the pelvis was also obtained to evaluate the patient’s THAs, and a computed tomography scan (CT) of the abdomen and pelvis with contrast was obtained for further evaluation. Representative CT, radiographic, and MRI images are shown at left (Figures 1-3).
What is the suspected diagnosis?
Answer
The MRI of the lumbar spine demonstrated no evidence of diskitis osteomyelitis. However, T2-weighted axial images showed enlarged heterogeneous bilateral psoas muscles with bright signal, indicating the presence of fluid (white arrows, Figure 4).
Figure 4.
Figure 5.
On the pelvic radiographs, both femoral heads appeared off-center within the acetabular cups (red arrows, Figure 5).This eccentric positioning indicated wear of the polyethylene in the THAs that normally occupies the space between the acetabular cup and the femoral head. In addition, focal lucency in the right acetabulum indicated breakdown of the bone, a condition referred to as osteolysis (white asterisk, Figure 5).
An abdominopelvic CT scan with contrast was performed and confirmed the findings of polyethylene wear and osteolysis. The CT scan also demonstrated large bilateral hip joint effusions (white arrows, Figure 6), decompressed along distended bilateral iliopsoas bursae (red asterisks, Figure 6), and communicating with the bilateral psoas muscle collections (red arrows, Figure 6).
Osteolysis With Iliopsoas Bursitis
Bursae are fluid-filled sacs lined by synovial tissue located throughout the body to reduce friction at sites of movement between muscles, bones, and tendons. Bursitis develops when these sacs become inflamed and/or infected and fill with fluid. The iliopsoas bursa lies between the anterior capsule of the hip and the psoas tendon, iliacus tendon, and muscle fibers.1,2 This bursa frequently communicates with the hip joint.3,4 Iliopsoas bursal distension has been reported following THA in the setting of polyethylene wear,5 and aseptic bursitis is a commonly seen incidental finding at the time of revision surgery.6
Figure 6.
In this patient, long-standing polyethylene-induced synovitis had markedly expanded the hip joints and iliopsoas bursae, eventually resulting in superinfection, which accounted for the patient’s symptoms.
Treatment
Based on the imaging findings, interventional radiology services were contacted. The interventional radiologist drained the bilateral psoas abscesses. Cultures of the fluid were positive for both methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-susceptible S aureus (MSSA). The patient was admitted to the hospital for treatment of MRSA and MSSA with intravenous antibiotic therapy. He recovered from the infection and was discharged on hospital day 2, with instructions to follow up with an orthopedic surgeon to discuss eventual revision of the bilateral THAs.
Figure 1.
Figure 2.
Figure 3.A 49-year-old man with a history of human immunodeficiency virus infection, untreated hepatitis C, endocarditis, and bilateral total hip arthroplasty (THA) presented to the ED with fever, chills, and a nonproductive cough, which he stated began 2 days prior. The patient was not able to walk due to worsening low back and bilateral leg pain.
Laboratory studies revealed leukocytosis with a left shift. Chest radiographs were negative for pneumonia. A magnetic resonance image (MRI) of the lumbar spine was obtained to evaluate for diskitis osteomyelitis. A radiograph of the pelvis was also obtained to evaluate the patient’s THAs, and a computed tomography scan (CT) of the abdomen and pelvis with contrast was obtained for further evaluation. Representative CT, radiographic, and MRI images are shown at left (Figures 1-3).
What is the suspected diagnosis?
Answer
The MRI of the lumbar spine demonstrated no evidence of diskitis osteomyelitis. However, T2-weighted axial images showed enlarged heterogeneous bilateral psoas muscles with bright signal, indicating the presence of fluid (white arrows, Figure 4).
Figure 4.
Figure 5.
On the pelvic radiographs, both femoral heads appeared off-center within the acetabular cups (red arrows, Figure 5).This eccentric positioning indicated wear of the polyethylene in the THAs that normally occupies the space between the acetabular cup and the femoral head. In addition, focal lucency in the right acetabulum indicated breakdown of the bone, a condition referred to as osteolysis (white asterisk, Figure 5).
An abdominopelvic CT scan with contrast was performed and confirmed the findings of polyethylene wear and osteolysis. The CT scan also demonstrated large bilateral hip joint effusions (white arrows, Figure 6), decompressed along distended bilateral iliopsoas bursae (red asterisks, Figure 6), and communicating with the bilateral psoas muscle collections (red arrows, Figure 6).
Osteolysis With Iliopsoas Bursitis
Bursae are fluid-filled sacs lined by synovial tissue located throughout the body to reduce friction at sites of movement between muscles, bones, and tendons. Bursitis develops when these sacs become inflamed and/or infected and fill with fluid. The iliopsoas bursa lies between the anterior capsule of the hip and the psoas tendon, iliacus tendon, and muscle fibers.1,2 This bursa frequently communicates with the hip joint.3,4 Iliopsoas bursal distension has been reported following THA in the setting of polyethylene wear,5 and aseptic bursitis is a commonly seen incidental finding at the time of revision surgery.6
Figure 6.
In this patient, long-standing polyethylene-induced synovitis had markedly expanded the hip joints and iliopsoas bursae, eventually resulting in superinfection, which accounted for the patient’s symptoms.
Treatment
Based on the imaging findings, interventional radiology services were contacted. The interventional radiologist drained the bilateral psoas abscesses. Cultures of the fluid were positive for both methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-susceptible S aureus (MSSA). The patient was admitted to the hospital for treatment of MRSA and MSSA with intravenous antibiotic therapy. He recovered from the infection and was discharged on hospital day 2, with instructions to follow up with an orthopedic surgeon to discuss eventual revision of the bilateral THAs.
References
1. Chandler SB. The iliopsoas bursa in man. Anatom Record. 1934;58(3),235-240. doi:10.1002/ar.1090580304. 2. Tatu L, Parratte B, Vuillier F, Diop M, Monnier G. Descriptive anatomy of the femoral portion of the iliopsoas muscle. Anatomical basis of anterior snapping of the hip. Surg Radiol Anat. 2001;23(6):371-374. 3. Meaney JF, Cassar-Pullicino VN, Etherington R, Ritchie DA, McCall IW, Whitehouse GH. Ilio-psoas bursa enlargement. Clin Radiol. 1992;45(3):161-168. 4. Warren R, Kaye JJ, Salvati EA. Arthrographic demonstration of an enlarged iliopsoas bursa complicating osteoarthritis of the hip. A case report. J Bone Joint Surg Am. 1975;57(3):413-415. 5. Cheung YM, Gupte CM, Beverly MJ. Iliopsoas bursitis following total hip replacement. Arch Orthop Trauma Surg. 2004;124(10):720-723. Epub 2004 Oct 23. doi:10.1007/s00402-004-0751-9. 6. Howie DW, Cain CM, Cornish BL. Pseudo-abscess of the psoas bursa in failed double-cup arthroplasty of the hip. J Bone Joint Surg Br. 1991;73:29-32.
References
1. Chandler SB. The iliopsoas bursa in man. Anatom Record. 1934;58(3),235-240. doi:10.1002/ar.1090580304. 2. Tatu L, Parratte B, Vuillier F, Diop M, Monnier G. Descriptive anatomy of the femoral portion of the iliopsoas muscle. Anatomical basis of anterior snapping of the hip. Surg Radiol Anat. 2001;23(6):371-374. 3. Meaney JF, Cassar-Pullicino VN, Etherington R, Ritchie DA, McCall IW, Whitehouse GH. Ilio-psoas bursa enlargement. Clin Radiol. 1992;45(3):161-168. 4. Warren R, Kaye JJ, Salvati EA. Arthrographic demonstration of an enlarged iliopsoas bursa complicating osteoarthritis of the hip. A case report. J Bone Joint Surg Am. 1975;57(3):413-415. 5. Cheung YM, Gupte CM, Beverly MJ. Iliopsoas bursitis following total hip replacement. Arch Orthop Trauma Surg. 2004;124(10):720-723. Epub 2004 Oct 23. doi:10.1007/s00402-004-0751-9. 6. Howie DW, Cain CM, Cornish BL. Pseudo-abscess of the psoas bursa in failed double-cup arthroplasty of the hip. J Bone Joint Surg Br. 1991;73:29-32.
A 79-year-old woman presented to the ED with acute shortness of breath. Of note, she had been recently discharged from our hospital after an open reduction and internal fixation of an intertrochanteric fracture of the right hip. The patient’s postoperative course was uncomplicated, and she was discharged home after a brief inpatient stay.
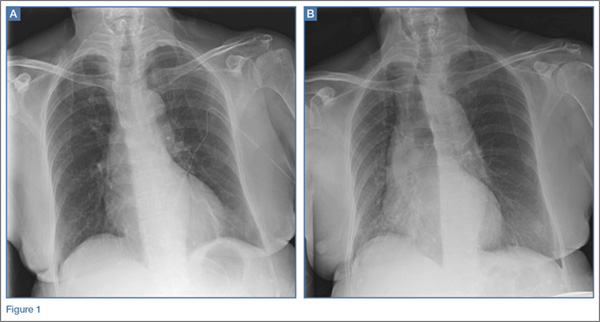
On physical examination, the patient was diaphoretic and tachypneic; oxygen saturation was 68% on room air, but increased to 100% saturation with supplemental oxygen through a nonrebreather mask. Radiographs from the patient’s inpatient hospital stay (Figure 1a) as well as ED visit (Figure 1b) were reviewed; representative images are shown above.
What is the diagnosis? What additional imaging tests may be useful to confirm the diagnosis?
Answer
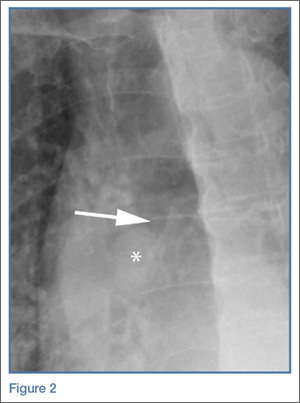
The radiographs taken at the time of the patient’s discharge were normal. The radiograph of the chest obtained in the ED, however, demonstrated a distinct cut-off of the right mainstem bronchus, referred to as a bronchial cut-off sign (white arrow, Figure 2), with a rounded density projecting over the right mainstem bronchus (white asterisk, Figure 2). These radiographic appearances suggested the presence of an aspirated foreign body.
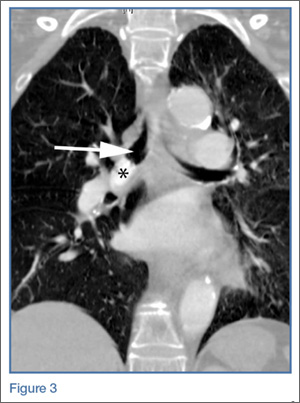
A computed tomography (CT) scan of the chest with contrast was performed to further evaluate the radiographic opacity and to exclude pulmonary embolism (PE), as this patient was at risk for such. The CT scan revealed no evidence of PE but confirmed the diagnosis of an aspirated foreign body. A high-density tablet (black asterisk, Figure 3) was noted to be completely occluding the right mainstem bronchus (white arrow, Figure 3) with resultant mild hyperinflation of the right lung. Upon further questioning, the patient stated that she had choked on a calcium tablet earlier in the day, but thought that the pill had finally “gone down.”
Since aspiration of foreign bodies is far more common in children,1,2 the diagnosis often is not considered in adults who present with acute onset of shortness of breath. In adults, the most significant predisposing factor to aspiration is alcoholism. However, foreign body aspiration may arise in various clinical scenarios, including in patients with structural abnormalities, in those with neuromuscular disease, and in the postoperative setting. The most common aspirated foreign bodies are food and broken tooth fragments/periodontal devices (eg, periodontal splint).2
Presentation is varied and depends upon the nature and volume of the aspirated foreign body, which may contribute to the airway obstruction or an inflammatory bronchopneumonia. The posterior segment of the upper lobes and the superior segments of the lower lobes are the most commonly involved sites, with the right lung preferentially involved over the left lung.3
The diagnosis of foreign body aspiration begins with an appropriate clinical history. Given our patient’s recent orthopedic surgery, PE was an understandable diagnostic consideration. As with any patient acutely short of breath, radiographs are the initial diagnostic imaging study of choice. An abrupt truncation of a bronchus on radiography suggests obstruction related to a mucous plugging, cancer, or foreign body aspiration. Other findings of foreign body aspiration include segmental/lobar hyperinflation and/or atelectasis.3 In many scenarios, the aspirated foreign body may not be radiodense, which limits the utility and diagnostic accuracy of radiography. Computed tomography improves diagnostic precision and time to diagnosis by directly visualizing the airway lumen and improving visualization of radiolucent objects.4
Treatment for obstructive aspiration depends upon the location and nature of the aspirated object. However, bedside bronchoscopy and extraction of the foreign object is the mainstay of treatment, and is how this patient was treated. Rapid diagnosis and treatment is key to alleviating obstruction and preventing potential complications of hemoptysis and infection.
References
1. Marom EM, McAdams HP, Erasmus JJ, Goodman PC. The many faces of pulmonary aspiration. AJR Am J Roentgenol. 1999;172(1):121-128.
3. Franquet T, Giménez A, Rosón N, Torrubia S, Sabaté JM, Pérez C. Aspiration diseases: Findings, pitfalls, and differential diagnosis. Radiographics. 2000;20(3):673-685.
4. Newton JP, Abel RW, Lloyd CH, Yemm R. The use of computed tomography in the detection of radiolucent denture base material in the chest. J Oral Rehabil. 1987;14(2):193-202.
A 79-year-old woman presented for evaluation of acute shortness of breath.
A 79-year-old woman presented for evaluation of acute shortness of breath.
A 79-year-old woman presented to the ED with acute shortness of breath. Of note, she had been recently discharged from our hospital after an open reduction and internal fixation of an intertrochanteric fracture of the right hip. The patient’s postoperative course was uncomplicated, and she was discharged home after a brief inpatient stay.
On physical examination, the patient was diaphoretic and tachypneic; oxygen saturation was 68% on room air, but increased to 100% saturation with supplemental oxygen through a nonrebreather mask. Radiographs from the patient’s inpatient hospital stay (Figure 1a) as well as ED visit (Figure 1b) were reviewed; representative images are shown above.
What is the diagnosis? What additional imaging tests may be useful to confirm the diagnosis?
Answer
The radiographs taken at the time of the patient’s discharge were normal. The radiograph of the chest obtained in the ED, however, demonstrated a distinct cut-off of the right mainstem bronchus, referred to as a bronchial cut-off sign (white arrow, Figure 2), with a rounded density projecting over the right mainstem bronchus (white asterisk, Figure 2). These radiographic appearances suggested the presence of an aspirated foreign body.
A computed tomography (CT) scan of the chest with contrast was performed to further evaluate the radiographic opacity and to exclude pulmonary embolism (PE), as this patient was at risk for such. The CT scan revealed no evidence of PE but confirmed the diagnosis of an aspirated foreign body. A high-density tablet (black asterisk, Figure 3) was noted to be completely occluding the right mainstem bronchus (white arrow, Figure 3) with resultant mild hyperinflation of the right lung. Upon further questioning, the patient stated that she had choked on a calcium tablet earlier in the day, but thought that the pill had finally “gone down.”
Since aspiration of foreign bodies is far more common in children,1,2 the diagnosis often is not considered in adults who present with acute onset of shortness of breath. In adults, the most significant predisposing factor to aspiration is alcoholism. However, foreign body aspiration may arise in various clinical scenarios, including in patients with structural abnormalities, in those with neuromuscular disease, and in the postoperative setting. The most common aspirated foreign bodies are food and broken tooth fragments/periodontal devices (eg, periodontal splint).2
Presentation is varied and depends upon the nature and volume of the aspirated foreign body, which may contribute to the airway obstruction or an inflammatory bronchopneumonia. The posterior segment of the upper lobes and the superior segments of the lower lobes are the most commonly involved sites, with the right lung preferentially involved over the left lung.3
The diagnosis of foreign body aspiration begins with an appropriate clinical history. Given our patient’s recent orthopedic surgery, PE was an understandable diagnostic consideration. As with any patient acutely short of breath, radiographs are the initial diagnostic imaging study of choice. An abrupt truncation of a bronchus on radiography suggests obstruction related to a mucous plugging, cancer, or foreign body aspiration. Other findings of foreign body aspiration include segmental/lobar hyperinflation and/or atelectasis.3 In many scenarios, the aspirated foreign body may not be radiodense, which limits the utility and diagnostic accuracy of radiography. Computed tomography improves diagnostic precision and time to diagnosis by directly visualizing the airway lumen and improving visualization of radiolucent objects.4
Treatment for obstructive aspiration depends upon the location and nature of the aspirated object. However, bedside bronchoscopy and extraction of the foreign object is the mainstay of treatment, and is how this patient was treated. Rapid diagnosis and treatment is key to alleviating obstruction and preventing potential complications of hemoptysis and infection.
A 79-year-old woman presented to the ED with acute shortness of breath. Of note, she had been recently discharged from our hospital after an open reduction and internal fixation of an intertrochanteric fracture of the right hip. The patient’s postoperative course was uncomplicated, and she was discharged home after a brief inpatient stay.
On physical examination, the patient was diaphoretic and tachypneic; oxygen saturation was 68% on room air, but increased to 100% saturation with supplemental oxygen through a nonrebreather mask. Radiographs from the patient’s inpatient hospital stay (Figure 1a) as well as ED visit (Figure 1b) were reviewed; representative images are shown above.
What is the diagnosis? What additional imaging tests may be useful to confirm the diagnosis?
Answer
The radiographs taken at the time of the patient’s discharge were normal. The radiograph of the chest obtained in the ED, however, demonstrated a distinct cut-off of the right mainstem bronchus, referred to as a bronchial cut-off sign (white arrow, Figure 2), with a rounded density projecting over the right mainstem bronchus (white asterisk, Figure 2). These radiographic appearances suggested the presence of an aspirated foreign body.
A computed tomography (CT) scan of the chest with contrast was performed to further evaluate the radiographic opacity and to exclude pulmonary embolism (PE), as this patient was at risk for such. The CT scan revealed no evidence of PE but confirmed the diagnosis of an aspirated foreign body. A high-density tablet (black asterisk, Figure 3) was noted to be completely occluding the right mainstem bronchus (white arrow, Figure 3) with resultant mild hyperinflation of the right lung. Upon further questioning, the patient stated that she had choked on a calcium tablet earlier in the day, but thought that the pill had finally “gone down.”
Since aspiration of foreign bodies is far more common in children,1,2 the diagnosis often is not considered in adults who present with acute onset of shortness of breath. In adults, the most significant predisposing factor to aspiration is alcoholism. However, foreign body aspiration may arise in various clinical scenarios, including in patients with structural abnormalities, in those with neuromuscular disease, and in the postoperative setting. The most common aspirated foreign bodies are food and broken tooth fragments/periodontal devices (eg, periodontal splint).2
Presentation is varied and depends upon the nature and volume of the aspirated foreign body, which may contribute to the airway obstruction or an inflammatory bronchopneumonia. The posterior segment of the upper lobes and the superior segments of the lower lobes are the most commonly involved sites, with the right lung preferentially involved over the left lung.3
The diagnosis of foreign body aspiration begins with an appropriate clinical history. Given our patient’s recent orthopedic surgery, PE was an understandable diagnostic consideration. As with any patient acutely short of breath, radiographs are the initial diagnostic imaging study of choice. An abrupt truncation of a bronchus on radiography suggests obstruction related to a mucous plugging, cancer, or foreign body aspiration. Other findings of foreign body aspiration include segmental/lobar hyperinflation and/or atelectasis.3 In many scenarios, the aspirated foreign body may not be radiodense, which limits the utility and diagnostic accuracy of radiography. Computed tomography improves diagnostic precision and time to diagnosis by directly visualizing the airway lumen and improving visualization of radiolucent objects.4
Treatment for obstructive aspiration depends upon the location and nature of the aspirated object. However, bedside bronchoscopy and extraction of the foreign object is the mainstay of treatment, and is how this patient was treated. Rapid diagnosis and treatment is key to alleviating obstruction and preventing potential complications of hemoptysis and infection.
References
1. Marom EM, McAdams HP, Erasmus JJ, Goodman PC. The many faces of pulmonary aspiration. AJR Am J Roentgenol. 1999;172(1):121-128.
3. Franquet T, Giménez A, Rosón N, Torrubia S, Sabaté JM, Pérez C. Aspiration diseases: Findings, pitfalls, and differential diagnosis. Radiographics. 2000;20(3):673-685.
4. Newton JP, Abel RW, Lloyd CH, Yemm R. The use of computed tomography in the detection of radiolucent denture base material in the chest. J Oral Rehabil. 1987;14(2):193-202.
References
1. Marom EM, McAdams HP, Erasmus JJ, Goodman PC. The many faces of pulmonary aspiration. AJR Am J Roentgenol. 1999;172(1):121-128.
3. Franquet T, Giménez A, Rosón N, Torrubia S, Sabaté JM, Pérez C. Aspiration diseases: Findings, pitfalls, and differential diagnosis. Radiographics. 2000;20(3):673-685.
4. Newton JP, Abel RW, Lloyd CH, Yemm R. The use of computed tomography in the detection of radiolucent denture base material in the chest. J Oral Rehabil. 1987;14(2):193-202.