Article

Ice Pack–Induced Perniosis: A Rare and Underrecognized Association
Perniosis, or chilblain, is characterized by skin lesions that occur as an abnormal reaction to exposure to cold and damp conditions. Ice pack–...
Article
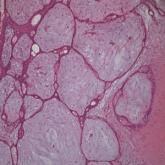
Concomitant Fibrofolliculoma and Trichodiscoma on the Abdomen
Fibrofolliculoma and trichodiscoma are adnexal tumors that arise from or around hair follicles and are two of the many characteristic features of...