News

COVID-related immunization gaps portend return of preventable infections
Reversal of herd immunity is possible in the face of growing vaccine hesitancy.
News

U.S. mothers underestimate role breastfeeding plays in curbing breast cancer
Only 36% of U.S. mothers currently breastfeed as recommended.
News
Gender surgical outcomes differ following puberty suppression
Results indicate puberty suppression may aid technical feasibility of varied surgical techniques.
News

Two consecutive negative FUBC results clear S. aureus bacteremia
The majority of cases had a limited duration of less than 48 hours of bacteremia.
News
Prophylactic HIV treatment in female STI patients is rare
Female patients with STIs are more likely to contract HIV, regardless of insurance status.
News

Menstrual irregularity appears to be predictor of early death
Cardiovascular disease and smoking increase risk.
News
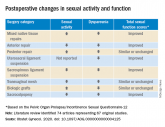
POP surgeries not tied to decreased sexual functioning
Pelvic organ prolapse surgeries should be planned with the goal of optimizing sexual function postoperatively.
News
Early hearing impairment interventions key to kindergarten readiness
Integrated data systems play key role in identifying relevant topics in academic outcomes for early intervention recipients.
News

Tobacco-free homes yield more tobacco-free youth
Smokeless products substantially reduce likelihood of parental suspicion and awareness.
News

Flu vaccine significantly cuts pediatric hospitalizations
More than half (58%) of hospitalized children had underlying medical conditions and 38% had at least one hospitalization in the past year.
News

Prescribe Halloween safety by region, current conditions
Setting a good example for our children is just as important as protecting them from the virus.
News

PHiD-CV with 4CMenB safe, effective for infants
Immunogenicity achieved with three-dose scheduling.
News

Racial, ethnic minorities often don’t practice sun protective behaviors
Cultural beliefs, stigma, and personal preferences may affect behaviors.
News

Key risk factors of pediatric cervical spinal injury identified
This needs to be validated in a large multicenter study.
News
Penicillin-susceptible Streptococcus pneumoniae most common cause of bacteremic CAP
Narrow-spectrum aminopenicillins should be used specifically to treat children hospitalized from suspected bacterial CAP.