User login
Community-acquired Bacterial Respiratory Tract Infections: Consensus Recommendations
- To minimize development and spread of antibiotic resistance, it is important to administer the correct antibacterial, by the best route, in the right amount, at optimum intervals, and for the appropriate duration.
- Streptococcus pneumoniae and Haemophilus influenzae are the 2 most common bacterial pathogens observed in community-acquired respiratory tract infections.
- Surveillance studies indicate increasing rates of in vitro resistance by S pneumoniae to many β-lactam and macrolide antibiotics.
- To minimize risk of resistance-associated recurrence or relapse, antibacterial agents should be prescribed in accordance with existing guidelines and local resistance patterns. Patient compliance with dosage and duration of therapy should be fostered.
- Preliminary data suggest that high-dose, short-course antibacterial therapy may be as effective as longer courses of low-dose therapy.
Community-acquired respiratory tract infections (CARTIs) are a reason for seeking medical attention. In 2001, there were 28.4 million office visits in the United States for an acute respiratory tract infection (excluding pharyngitis).1
Management of CARTIs poses several challenges. According to the World Health Organization (WHO), “for every 100 respiratory infections, only 20% require antibiotic treatment”2 —the remaining 80 infections most likely have a viral origin. Thus, antibacterial therapy should be avoided unless a bacterial cause has been confirmed or is deemed likely.
Once that determination has been made, clinicians need to separate patients who can be safely managed as outpatients from those who need to be hospitalized. Disease severity is, of course, an important consideration in this selection process.3-8
For management of patients who will not be hospitalized, the WHO and the Society for Healthcare Epidemiology of America/Infectious Diseases Society of America (SHEA/IDSA) offer the 3 Ds: administer the correct drug, at the right dose, and for the appropriate duration, to minimize development and spread of resistance.9,10 A recent consensus conference coordinated by the Primary Care Education Consortium and Texas Academy of Family Physicians elaborated on this mnemonic as it relates to outpatient management of 3 CARTIs: community-acquired pneumonia, acute bacterial exacerbations of chronic bronchitis, and acute bacterial rhinosinusitis. Its recommendations, which have been drawn largely from existing evidence-based guidelines, form the basis for this review.
Drug selection
Treatment with an antibacterial agent will not be medically warranted in the majority of patients with a CARTI. Many of these patients will, however, expect to go home with an antibiotic prescription. The primary care clinician can reduce such expectations and prevent unnecessary reconsultations by briefly addressing four issues: 1) the natural course of the viral illness, 2) the lack of effectiveness of antibiotics, 3) the problem of antibiotic resistance, and 4) the side effects of antibiotics.11
When selecting an antibacterial agent for patients with pneumonia, bronchitis, or rhinosinusitis for which a bacterial cause has been identified or deemed likely, several factors need to be taken into account, including the suspected or identified pathogens, local resistance patterns, previous therapy, patient allergies, and the patient’s ability to tolerate treatment failure. Many of these factors are considered by professional organizations that regularly develop guidelines for CARTIs based on the best available evidence. Perhaps most critical for decision-making in the primary care setting is an understanding of evolving microbiology and resistance patterns.
Common pathogens
There is considerable overlap among pathogens commonly found in CARTIs. Streptococcus pneumoniae and Haemophilus influenzae are most often observed in the outpatient setting.
Community-acquired pneumonia. In outpatients with mild illness, S pneumoniae, Mycoplasma pneumoniae, Chlamydia species (particularly Chlamydia pneumoniae, now called Chlamydophilia pneumoniae), and H influenzae are the most common pathogens.12,13 In patients younger than 50 years without significant comorbidity, Mycoplasma species are the most common pathogens. Older patients and those with significant comorbidity are more likely infected with S pneumoniae,13 a Gram-negative enteric bacillus, Pseudomonas aeruginosa, or Legionella.5,14
Bacterial bronchitis. In addition to S pneumoniae and H influenzae, Moraxella catarrhalis is a frequent pathogen in bacterial exacerbations of chronic bronchitis.15P aeruginosa and other Gram-negative bacilli are also seen, especially in patients with a severe acute exacerbation who have a forced expiratory volume in 1 second (FEV1) of 35% of predicted or less.16 Infection due to multiple pathogens occurs in a small percentage of all patients with chronic bronchitis, particularly those with severe exacerbations. Fewer than 10% of acute exacerbations are due to an atypical bacterium, usually C pneumoniae. M pneumoniae and Legionella pneumophila are implicated even less frequently.15
Bacterial rhinosinusitis.S pneumoniae and H influenzae also are frequent causes of acute bacterial rhinosinusitis. Other pathogens commonly seen in this condition include other Streptococcus species, M catarrhalis, oral anaerobes, Staphylococcus aureus in adults, and M catarrhalis, Streptococcus pyogenes, and anaerobes in children.17
Resistance
Antibiotic resistance is an important consideration in the management of CARTIs. There is little doubt that widespread use of antibiotics leads to in vitro bacterial resistance.18-20 However, because clinical success has been observed in the presence of pathogens with low-level resistance, there is some debate as to whether low-level antibiotic resistance has a significant effect on clinical outcomes.18,21-29 Even so, the US Centers for Disease Control and Prevention has determined that people who attend or work at child-care centers and those who recently used antimicrobial agents are at increased risk for infection with drug-resistant S pneumoniae.30 Moreover, the WHO has stated that infection with resistant pathogens prolongs illness and increases the probability of a fatal outcome.31
Several surveillance programs that monitor antibiotic resistance patterns—including the Alexander Project32 and Tracking Resistance in the United States Today (TRUST)33-36 —have confirmed widespread resistance to antibiotics commonly used to treat CARTIs in the United States. β-Lactam resistance due to penicillin-binding protein changes in S pneumoniae has increased significantly over the past decade. Generally, more than 30% of S pneumoniae are now resistant to penicillins and macrolides (including azithromycin and clarithromycin, the ‘advanced’ agents in this group). A smaller number (6%) are resistant to amoxicillin/clavulanate, although this appears to be a result of in vitro test parameters involving primarily strains with high-level β-lactam resistance. Some cephalosporins also show greater activity than penicillin against intermediately susceptible S pneumoniae, but are not effective against highly resistant strains. In contrast, fewer than 1% of all pneumococci are resistant to newer fluoroquinolones (the so-called respiratory fluoroquinolones, such as gatifloxacin, gemifloxacin, levofloxacin, moxifloxacin) and the ketolide telithromycin.
The prevalence of β-lactamase–producing strains of H influenzae appears to have leveled off. Approximately 30% of H influenzae strains are resistant to ampicillin, while fewer than 1% are resistant to amoxicillin/clavulanate, cefuroxime, macrolides, and newer fluoroquinolones.
More than 90% of M catarrhalis isolates produce β-lactamase, thereby conferring resistance to ampicillin and amoxicillin.
Significant geographical variation in resistance has been observed. The prevalence of penicillin-resistant S pneumoniae ranges from 8% in New England to 25% in the South Atlantic, while ampicillin-resistant H influenzae is seen most often in New England (35%) and least often in the Rocky Mountain region (24%).33,34,36 Significant differences within a community also have been observed.37 Thus, knowledge of local resistance patterns is necessary. This information generally is available from local hospitals, although such data may be more reflective of nosocomial pathogens, or state health departments.
Community-acquired pneumonia
The 2003 guidelines of the IDSA give advanced macrolides and respiratory fluoroquinolones a prominent role in the management of community-acquired pneumonia (TABLE 1).5 The IDSA reviewed data from more than 150 clinical trials conducted in adults over 15 years. The IDSA panel acknowledged the increasing in vitro resistance of S pneumoniae to the macrolides, but noted that reports of clinical failure have not paralleled this. The panel also pointed out the significantly lower rates of resistance to the respiratory fluoroquinolones and expressed concern that abuse of these agents could lead to increased resistance by S pneumoniae.
In a previously healthy person who has not taken an antibiotic in the last 3 months, the IDSA recommends a macrolide or doxycycline as first-line therapy, whereas a fluoroquinolone, high-dose amoxicillin/clavulanate, or a macrolide plus high-dose amoxicillin should be used if an antibiotic has been taken during the last 3 months. Patients with a significant comorbidity can be treated with a fluoroquinolone without regard to recent antibiotic use. Alternatively, a macrolide can be used alone in patients who have not taken an antibiotic in 3 months, but otherwise must be used in combination with high-dose amoxicillin. High-dose amoxicillin/clavulanate or cefpodoxime, cefprozil, or cefuroxime can be used in those with a significant comorbidity and recent antibiotic use.
TABLE 1
Initial empiric therapy in outpatients with community-acquired pneumonia
| Clinical characteristics | No recent antibiotic therapy | Antibiotics during past 3 months |
|---|---|---|
| Previously healthy |
|
|
| Comorbidities (chronic obstructive pulmonary disease, diabetes, renal failure, congestive heart failure, malignancy) |
|
|
| Suspected aspiration with infection |
| |
| Influenza with bacterial superinfection |
| |
| Adapted from Mandell et al.5 © 2003 Infectious Diseases Society of America. | ||
Bacterial bronchitis
A panel of primary care physicians and specialists convened by the Canadian Thoracic Society (CTS) reviewed nearly 400 published articles on acute bacterial exacerbations of chronic bronchitis, including evidence-based reviews such as the Cochrane Database. The 2003 CTS guidelines recommend that treatment be based on the risk for treatment failure (TABLE 2).8
Antibacterial treatment is not recommended for patients whose clinical history and symptoms suggest a viral infection (group 0) unless symptoms persist for more than 10 to 14 days. In those cases, bacterial superinfection with M pneumoniae, C pneumoniae, or Bordetella pertussis is possible. Patients with chronic bronchitis but without risk factors for treatment failure (group 1) may be treated with a variety of first-line agents, including azithromycin, clarithromycin, cefuroxime, cefprozil, cefixime, amoxicillin, doxycycline, or trimethoprim/sulfamethoxazole. For patients in group 1 who fail first-line therapy, and as first-line therapy for patients in group 2, a fluoroquinolone or amoxicillin/clavulanate is recommended. Patients in group 3 are more likely to be infected with a Gram-negative pathogen, such as Ps aeruginosa or Enterobacter species, and are least able to tolerate treatment failure. Hence, ciprofloxacin is appropriate in the outpatient setting.
TABLE 2
Initial empiric therapy in outpatients with acute bacterial exacerbations of chronic bronchitis
| Group | Clinical status | Symptoms/risk factors | Initial treatment | Alternative when 1st-line agent fails |
|---|---|---|---|---|
| 0 | Acute tracheobronchitis |
|
|
|
| 1 | Chronic bronchitis without risk factors |
|
|
|
| 2 | Chronic bronchitis with risk factors |
|
|
|
| 3 | Chronic suppurative bronchitis |
|
| |
| Adapted from Balter et al,8 with permission. The publisher of Can Respir J does not assume responsibility for errors or discrepancies that may have occurred. | ||||
Bacterial rhinosinusitis
The recommendations for management of acute bacterial rhinosinusitis issued by the Sinus and Allergy Health Partnership (SAHP), a not-for-profit organization created by the American Academy of Otolaryngic Allergy, the American Academy of Otolaryngology-Head and Neck Surgery, and the American Rhinologic Society, are based on a variety of factors. These include rate of spontaneous resolution, pathogen distribution, antibacterial resistance data, the importance of S pneumoniae in intracranial and extrasinus complications, and the ability of a patient to tolerate treatment failure (TABLE 3).17 The panel reviewed more than 150 published articles on management of children and adults with bacterial rhinosinusitis.
As in the pneumonia guidelines, recent antibiotic use is an important consideration when selecting an antibiotic since resistant pathogens are likely. β-Lactam agents play a major role as initial therapy in both children and adults. This recommendation is consistent with those of Williams et al who reviewed 49 clinical trials involving 13,660 patients. These investigators recommended 7 to 14 days of penicillin or amoxicillin for acute maxillary sinusitis confirmed radiographically or by aspiration.38
The SAHP recommended higher doses of amoxicillin (with or without clavulanate) in patients who have recently taken an antibiotic or who have moderate disease. Fluoroquinolones are recommended as alternatives in patients with mild disease who have not taken an antibiotic in the last 4 to 6 weeks. However, in patients with mild disease who have taken antibiotics recently or who have moderate disease, fluoroquinolones are recommended as first-line therapy. Macrolides are recommended only for patients with a β-lactam allergy since failure rates of 20% to 25% are possible. Lack of improvement or worsening symptoms after 72 hours should prompt reevaluation, may necessitate cultures and/or a CT scan, and should raise the possibility of causal organisms other than S pneumoniae, H influenzae, and M catarrhalis.
TABLE 3
Initial empiric therapy in outpatients with acute bacterial rhinosinusitis
| Initial therapy | Alternative agent if no improvement or worsening after 72 hours | |
|---|---|---|
| Mild disease, no antibiotic during past 4 to 6 weeks | ||
| Children |
|
|
| Children with β-lactam allergy |
|
|
| Adults |
|
|
| Adults with β-lactam allergy |
|
|
| Mild disease and antibiotic during past 4 to 6 weeks or moderate disease | ||
| Children |
|
|
| Children with β-lactam allergy |
|
|
| Adults |
|
|
| Adults with β-lactam allergy |
|
|
| Adapted from Anon et al17 © 2004, with permission from American Academy of Otolaryngology-Head and Neck Surgery Foundation, Inc. | ||
Dose and duration
While each of the three guidelines provides detailed recommendations regarding selection of an antibacterial agent, the dose and duration of therapy generally are not well defined. Fortunately, other sources provide guidance in these 2 areas.
First, an independent international panel of infectious diseases experts, whose goal was to identify ways to improve prescription of antibiotics for lower respiratory tract infections, stressed that an important purpose of therapy is to reduce bacterial load and, in fact, treat to bacteriologic cure.19 Antibiotic therapy that allows some bacteria to survive increases the risk of early recurrence or relapse and encourages resistance selection. Such therapy is, therefore, inappropriate. The panel concurred with the WHO and others that the likelihood of bacterial persistence increases when antibiotics are prescribed in low doses, especially if given over long periods.18,39-41 Prolonged low-dose antibiotic therapy, which has been common practice for many infections, is contrary to the WHO Global Strategy for Containment of Antimicrobial Resistance, which notes that single-agent therapy for a short duration is 1 of several actions that can be taken to minimize bacterial resistance.42 Shorter courses of antibiotic therapy also are consistent with SHEA/IDSA recommendations.10
The clinical appropriateness of this recommendation is reinforced by the changes that have occurred during the past decade in the management of selected urinary tract infections (UTIs). Some UTIs that previously had been treated with low-dose antibiotics for 10 to 14 days now are treated with only 1 or a few high doses of a single agent. Other infections for which clinical data support shorter courses of antibiotic therapy include uncomplicated cellulitis,43 ventilator-associated pneumonia,44 and meningococcal disease.45
Shorter-course antibacterial therapy for CARTIs increasingly has been the focus of clinical trials. The focus is not unreasonable. Many of the antibiotics used for CARTIs are very potent against the pathogens commonly encountered, penetrate infected tissues well, are available in oral formulations, and are generally well tolerated. However, to optimize an antibiotic’s bactericidal potential, it is necessary to base the dosing regimen on its pharmacodynamics. From a pharmacodynamic perspective, there are 2 groups of antibiotics, those with concentration-dependent killing and those with time-dependent killing. For agents with concentration-dependent killing, such as fluoroquinolones, ketolides, and aminoglycosides, the goal is to select a dose that achieves a higher peak concentration and/or a larger area under the plasma concentration curve, with acceptable tolerability. In contrast, antibiotics that rely on time-dependent killing, such as β-lactams, macrolides, azalides, tetracyclines, and some others, require extended durations of concentrations above the MIC90 of the bacterial pathogen(s). Consequently, multiple daily dosing may be preferable.46
Dose. A few studies have compared high-dose, short-course therapy with therapy using standard doses and durations (TABLE 4). To assess the impact of highdose, short-course therapy on post-treatment resistant pneumococcal carriage, Schrag compared amoxicillin given either as 90 mg/kg/day for 5 days (high-dose, short-course) or 40 mg/kg/day for 10 days (standard) in 797 children with a respiratory tract infection.47 At day 28, nasal carriage of penicillin-resistant S pneumoniae was detected in 24% of the high-dose, shortcourse group and in 32% of the standard group (relative risk, 0.77; P=0.03). Among the pneumococcal carriers, the risk of penicillin-resistant S pneumoniae was significantly lower in the high-dose, short-course group than in the standard therapy group (relative risk, 0.78; P=0.01)
Another study investigated high-dose, short-course therapy with levofloxacin in patients with mild to severe community-acquired pneumonia. Patients received levofloxacin 750 mg/d for 5 days or 500 mg/d for 10 days.48 The clinical success rates were 92.4% and 91.1%, respectively, while the bacteriologic eradication rates at 7 to 14 days post-therapy were 93.2% and 92.4%, respectively, thereby demonstrating that high-dose, shortcourse levofloxacin therapy is at least as effective as standard levofloxacin therapy.
Duration. Short-course therapy using standard doses of azithromycin, gemifloxacin, levofloxacin, moxifloxacin, and telithromycin has been investigated in clinical trials of CARTIs (FIGURE). In patients with community-acquired pneumonia, 5 days of therapy with telithromycin was shown to be equivalent to a 7-day course (both using a single daily dose of 800 mg), as well as to clarithromycin 500 mg bid for 10 days.49
In studies of acute exacerbations of chronic bronchitis, a 3-day course of azithromycin was equivalent to clarithromycin for 10 days50 and gemifloxacin for 5 days was equivalent to a sequential combination of ceftriaxone and cefuroxime axetil for up to 10 days.51 Levofloxacin for 3 days and azithromycin for 5 days provided equivalent outcomes,52 as did levofloxacin for 5 days and amoxicillin/clavulanate for 10 days.52 Moxifloxacin for 5 days provided results equivalent to those of 7 days of amoxicillin, clarithromycin, or cefuroxime axetil.53 Five days of telithromycin was shown to be equivalent to 10 days of amoxicillin/clavu-lanate54 or cefuroxime axetil.55
Studies of acute bacterial rhinosinusitis have demonstrated equivalent results with azithromycin for 3 days and amoxicillin/clavulanate for 10 days.50 Similarly, telithromycin for 5 days was equivalent to 10 days of telithromycin, amoxicillin/clavulanate, or cefuroxime axetil.56
These clinical trials demonstrate that short-course therapy achieves clinical cure and/or bacteriologic eradication rates that are at least equivalent to those of standard therapy, with no significant difference in safety. Symptomatic improvement is faster and total antibiotic exposure is reduced with short-course therapy.
A significant advantage of short-course antibacterial therapy is improved patient adherence. Adherence is 10% to 20% better with 5-day courses than with 10-day courses,47,57 and is significantly better with 1 or 2 daily doses than with 3 or more daily doses.58-60 In fact, a recent market research study showed that patients perceive once-daily, short-course antibiotic treatment to be significantly more effective than longer courses. This may be due to faster improvement of infection-related symptoms.61 For example, Dunbar et al observed that significantly more patients treated with high-dose, short-course levofloxacin experienced subjective and objective resolution of fever by day 3 compared with those who received standard-dose, short-course levofloxacin.48
TABLE 4
Clinical trials of high-dose, short-course antibiotic therapy
| Drug regimen | N (ref) | Outcome |
|---|---|---|
| Amoxicillin 90 mg/kg/d x 5 d vs Amoxicillin 40 mg/kg/d x 10 d | 797 |
|
| (47) | ||
| Levofloxacin 750 mg/d x 5d vs Levofloxacin 500 mg/d x 10 d | 390 |
|
| (48) |
TABLE 5 Clinical trials of standard-dose, short-course antibiotic therapy
Summary
Essential questions that need to be answered for every patient who presents with a possible CARTI include : 1) Is antibacterial therapy necessary? 2) If so, what is the best antibiotic and at what dose and for how long should it be administered? Accumulating evidence indicates that some antibiotics when given in high doses for a short duration are as effective and safe as standard therapy for CARTIs. Short-course therapy also promotes patient compliance.
Disclosures:
The authors reported the following financial relationships: Dr Brunton: consultant to Abbott, Ortho-McNeil Pharmaceutical, Inc., and SanofiAventis. Dr Carmichael: consultant to Ortho-McNeil Pharmaceutical, Inc.; on the speakers’ bureaus for Bristol-Myers Squibb Company, Merck & Co., OrthoMcNeil Pharmaceutical, Inc., and Pfizer Inc. Dr Fitzgerald: on the speakers’ bureaus for Boehringer Ingelheim, GlaxoSmithKline, Ortho-McNeil Pharmaceutical, Inc., Pfizer Inc., Sepracor Inc., and 3M. Dr Liu: on the speakers’ bureaus for Aventis Pharmaceuticals, Bayer Pharmaceuticals Corporation, Bristol-Myers Squibb Company, Cobist, GlaxoSmithKline, Merck & Co., Ortho-McNeil Pharmaceutical, Inc., Pfizer Inc., Purdue Pharma, Oscient Pharmaceuticals Corporation, and Wyeth Pharmaceuticals. Dr Varon: on the speakers’ bureau for Ortho-McNeil Pharmaceutical, Inc. Dr. Weiland: consultant to Abbott Laboratories, Ortho-McNeil Pharmaceutical, Inc., and Pfizer Inc.
This supplement to The Journal of Family Practice is supported by a grant from Ortho-McNeil Pharmaceutical, Inc. It was adapted from a consensus conference coordinated by the Primary Care Education Consortium and Texas Academy of Family Physicians and was edited and peer-reviewed by The Journal of Family Practice. © 2005 Quadrant HealthCom Inc. and Primary Care Education Consortium.
1. Centers for Disease Control and Prevention. National Center for Health Statistics website. National Ambulatory Medical Care Survey: 2001 Summary. Available at: http://www.cdc.gov/nchs/data/ad/ad337.pdf. Accessed February 2, 2005.
2. World Health Organization.World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 4. Big guns of resistance. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
3. Metlay JP, Fine MJ. Testing strategies in the initial management of patients with community-acquired pneumonia. Ann Intern Med. 2003;138:109-118.
4. File TM. Community-acquired pneumonia. Lancet. 2003;362:1991-2001.
5. Mandell LA, Bartlett JG, Dowell SF, File TM, Jr, Musher DM, Whitney C. Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clin Infect Dis. 2003;37:1405-1433.
6. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336:243-250.
7. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106:196-204.
8. Balter MS, La Forge J, Low DE, Mandell L, Grossman RF. Canadian guidelines for the management of acute exacerbations of chronic bronchitis. Can Respir J. 2003;10(suppl B):3B-32B.
9. World Health Organization. World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 5. A call to action: A massive effort to provide proper treatment. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
10. Shlaes DM, Gerding DN, John JF, Jr, et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the Prevention of Antimicrobial Resistance: guidelines for the prevention of antimicrobial resistance in hospitals. Clin Infect Dis. 1997;25:584-599.
11. Scottish Intercollegiate Guidelines Network. National Guideline Clearinghouse website. Community management of lower respiratory tract infection in adults. A national clinical guideline. Available at: http://www.guideline.gov/summary/summary.aspx?ss=15& doc_id=3361&nbr=2587&string=respiratory%20AND%20tract%20AND% 20infection. Accessed December 17, 2004.
12. Bochud PY, Moser F, Erard P, et al. Community-acquired pneumonia. A prospective outpatient study. Medicine (Baltimore). 2001;80:75-87.
13. Falguera M, Sacristan O, Nogues A, et al. Nonsevere community-acquired pneumonia: correlation between cause and severity or comorbidity. Arch Intern Med. 2001;161:1866-1872.
14. Ruiz M, Ewig S, Marcos MA, et al. Etiology of community-acquired pneumonia: impact of age, comorbidity, and severity. Am J Respir Crit Care Med. 1999;160:397-405.
15. Sethi S. Infectious etiology of acute exacerbations of chronic bronchitis. Chest. 2000;117(5 Suppl 2):380S-385S.
16. Eller J, Ede A, Schaberg T, Niederman MS, Mauch H, Lode H. Infective exacerbations of chronic bronchitis: relation between bacteriologic etiology and lung function. Chest. 1998;113:1542-1548.
17. Anon JB, Jacobs MR, Poole MD, et al. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg. 2004;130(1 Suppl):1-45.
18. Albrich WC, Monnet DL, Harbarth S. Antibiotic selection pressure and resistance in Streptococcus pneumoniae. and Streptococcus pyogenes. Emerg Infect Dis. 2004;10:514-517.
19. Ball P, Baquero F, Cars O, et al. Antibiotic therapy of community respiratory tract infections: strategies for optimal outcomes and minimized resistance emergence. J Antimicrob Chemother. 2002;49:31-40.
20. Harbarth S, Albrich W, Brun-Buisson C. Outpatient antibiotic use and prevalence of antibiotic-resistant pneumococci in France and Germany: a sociocultural perspective. Emerg Infect Dis. 2002;8:1460-1467.
21. Lonks JR, Garau J, Medeiros AA. Implications of antimicrobial resistance in the empirical treatment of community-acquired respiratory tract infections: the case of macrolides. J Antimicrob Chemother. 2002;50(Suppl S2):87-92.
22. Lonks JR, Garau J, Gomez L, et al. Failure of macrolide antibiotic treatment in patients with bacteremia due to erythromycin-resistant Streptococcus pneumoniae. Clin Infect Dis. 2002;35:556-564.
23. Moellering RC, Jr, Craig W, Edmond M, et al. Clinical and public health implications of macrolide-resistant Streptococcus pneumoniae. J Chemother. 2002;14(suppl 3):42-56.
24. Davidson R, Cavalcanti R, Brunton JL, et al. Resistance to levofloxacin and failure of treatment of pneumococcal pneumonia. N Engl J Med. 2002;346:747-750.
25. Musher DM, Dowell ME, Shortridge VD, et al. Emergence of macrolide resistance during treatment of pneumococcal pneumonia. N Engl J Med. 2002;346:630-631.
26. Waterer GW, Buckingham SC, Kessler LA, Quasney MW, Wunderink RG. Decreasing β-lactam resistance in Pneumococci. from the Memphis region: analysis of 2,152 isolates From 1996 to 2001. Chest. 2003;124:519-525.
27. Nuermberger E, Bishai WR. The clinical significance of macrolide-resistant Streptococcus pneumoniae.: it’s all relative. Clin Infect Dis. 2004;38:99-103.
28. Yu VL, Chiou CC, Feldman C, et al. An international prospective study of pneumococcal bacteremia: correlation with in vitro resistance, antibiotics administered, and clinical outcome. Clin Infect Dis. 2003;37:230-237.
29. Metlay JP. Update on community-acquired pneumonia: impact of antibiotic resistance on clinical outcomes. Curr Opin Infect Dis. 2002;15:163-167.
30. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention web site. Drug-resistant Streptococcus pneumoniae disease. Available at: http://www.cdc.gov/ncidod/dbmd/diseaseinfo/drugresisstreppneum_t.htm. Accessed January 4, 2005.
31. World Health Organization World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 3. Factors contributing to resistance. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
32. Jacobs MR, Felmingham D, Appelbaum PC, Gruneberg RN. The Alexander Project 1998-2000: susceptibility of pathogens isolated from communityacquired respiratory tract infection to commonly used antimicrobial agents. J Antimicrob Chemother. 2003;52:229-246.
33. Thornsberry C, Sahm DF, Kelly LJ, et al. Regional trends in antimicrobial resistance among clinical isolates of Streptococcus pneumoniae., Haemophilus influenzae., and Moraxella catarrhalis. in the United States: results from the TRUST Surveillance Program, 1999-2000. Clin Infect Dis. 2002;34(suppl 1):S4-S16.
34. Karlowsky JA, Thornsberry C, Jones ME, Evangelista AT, Critchley IA, Sahm DF. Factors associated with relative rates of antimicrobial resistance among Streptococcus pneumoniae. in the United States: results from the TRUST Surveillance Program (1998-2002). Clin Infect Dis. 2003;36:963-970.
35. Karlowsky JA, Kelly LJ, Thornsberry C, et al. Susceptibility to fluoroquinolones among commonly isolated Gram-negative bacilli in 2000: TRUST and TSN data for the United States. Tracking Resistance in the United States Today. The Surveillance Network. Int J Antimicrob Agents. 2002;19:21-31.
36. Karlowsky JA, Thornsberry C, Critchley IA, et al. Susceptibilities to levofloxacin in Streptococcus pneumoniae., Haemophilus influenzae., and Moraxella catarrhalis. clinical isolates from children: results from 2000-2001 and 2001-2002 TRUST studies in the United States. Antimicrob Agents Chemother. 2003;47:1790-1797.
37. Quale J, Landman D, Ravishankar J, Flores C, Bratu S. Streptococcus pneumo.-niae., Brooklyn, New York: fluoroquinolone resistance at our doorstep. Emerg Infect Dis. 2002;8:594-597.
38. Williams JW, Jr, Aguilar C, Cornell J, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2004;2:CD000243.-
39. Guillemot D, Carbon C, Balkau B, et al. Low dosage and long treatment duration of β-lactam: risk factors for carriage of penicillin-resistant Streptococcus pneumoniae. JAMA. 1998;279:365-370.
40. Scheld WM. Maintaining fluoroquinolone class efficacy: review of influencing factors. Emerg Infect Dis. 2003;9:1-9.
41. Thomson KS. Minimizing quinolone resistance: are the new agents more or less likely to cause resistance? J Antimicrob Chemother. 2000;45:719-723.
42. World Health Organization. World Health Organization web site. WHO global strategy for containment of antimicrobial resistance. Available at: http://www.who.int/csr/resources/publications/drugresist/en/EGlobal_Strat.pdf. Accessed February 2, 2005.
43. Hepburn MJ, Dooley DP, Skidmore PJ, Ellis MW, Starnes WF, Hasewinkle WC. Comparison of short-course (5 days) and standard (10 days) treatment for uncomplicated cellulitis. Arch Intern Med. 2004;164:1669-1674.
44. Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588-2598.
45. Ellis-Pegler R, Galler L, Roberts S, Thomas M, Woodhouse A. Three days of intravenous benzyl penicillin treatment of meningococcal disease in adults. Clin Infect Dis. 2003;37:658-662.
46. Craig WA. Basic pharmacodynamics of antibacterials with clinical applications to the use of β-lactams, glycopeptides, and linezolid. Infect Dis Clin North Am. 2003;17:479-501.
47. Schrag SJ, Pena C, Fernandez J, et al. Effect of short-course, high-dose amoxicillin therapy on resistant pneumococcal carriage: a randomized trial. JAMA. 2001;286:49-56.
48. Dunbar LM, Wunderink RG, Habib MP, et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
49. Tellier G, Niederman MS, Nusrat R, Patel M, Lavin B. Clinical and bacteriological efficacy and safety of 5 and 7 day regimens of telithromycin once daily compared with a 10 day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515-523.
50. Zithromax [prescribing information] New York, NY: Pfizer Labs; 2004.
51. Wilson R, Langan C, Ball P, Bateman K, Pypstra R. Oral gemifloxacin once daily for 5 days compared with sequential therapy with i.v. ceftriaxone/oral cefuroxime (maximum of 10 days) in the treatment of hospitalized patients with acute exacerbations of chronic bronchitis. Respir Med. 2003;97:242-249.
52. Tennenberg A, Walker K, Khashab M, Zadelkis N. The safety and efficacy of short-course (3-5 days), 750 mg levofloxacin (LVX) for acute bacterial exacerbation of chronic bronchitis (ABECB). Presented at: American Thoracic Society 100th International Conference, May 21-26, 2004, Orlando, Fl.
53. Wilson R, Allegra L, Huchon G, et al. Short-term and long-term outcomes of moxifloxacin compared to standard antibiotic treatment in acute exacerbations of chronic bronchitis. Chest. 2004;125:953-964.
54. Aubier M, Aldons PM, Leak A, et al. Telithromycin is as effective as amoxicillin/clavulanate in acute exacerbations of chronic bronchitis. Respir Med. 2002;96:862-871.
55. Zervos MJ, Heyder AM, Leroy B. Oral telithromycin 800 mg once daily for 5 days versus cefuroxime axetil 500 mg twice daily for 10 days in adults with acute exacerbations of chronic bronchitis. J Int Med Res. 2003;31:157-169.
56. Ketek [prescribing information]. Kansas City, Mo: Aventis Pharmaceuticals Inc.; 2004.
57. Carbon C, Chatelin A, Bingen E, et al. A double-blind randomized trial comparing the efficacy and safety of a 5-day course of cefotiam hexetil with that of a 10-day course of penicillin V in adult patients with pharyngitis caused by group A β-haemolytic streptococci. J Antimicrob Chemother 1995;35:843-854.
58. Cockburn J, Gibberd RW, Reid AL, Sanson-Fisher RW. Determinants of noncompliance with short term antibiotic regimens. Br Med J (Clin Res Ed). 1987;295:814-818.
59. Greenberg RN. Overview of patient compliance with medication dosing: a literature review. Clin Ther. 1984;6:592-599.
60. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23:1296-1310.
61. Perez-Gorricho B, Ripoll M. Does short-course antibiotic therapy better meet patient expectations? Int J Antimicrob Agents. 2003;21:222-228.
- To minimize development and spread of antibiotic resistance, it is important to administer the correct antibacterial, by the best route, in the right amount, at optimum intervals, and for the appropriate duration.
- Streptococcus pneumoniae and Haemophilus influenzae are the 2 most common bacterial pathogens observed in community-acquired respiratory tract infections.
- Surveillance studies indicate increasing rates of in vitro resistance by S pneumoniae to many β-lactam and macrolide antibiotics.
- To minimize risk of resistance-associated recurrence or relapse, antibacterial agents should be prescribed in accordance with existing guidelines and local resistance patterns. Patient compliance with dosage and duration of therapy should be fostered.
- Preliminary data suggest that high-dose, short-course antibacterial therapy may be as effective as longer courses of low-dose therapy.
Community-acquired respiratory tract infections (CARTIs) are a reason for seeking medical attention. In 2001, there were 28.4 million office visits in the United States for an acute respiratory tract infection (excluding pharyngitis).1
Management of CARTIs poses several challenges. According to the World Health Organization (WHO), “for every 100 respiratory infections, only 20% require antibiotic treatment”2 —the remaining 80 infections most likely have a viral origin. Thus, antibacterial therapy should be avoided unless a bacterial cause has been confirmed or is deemed likely.
Once that determination has been made, clinicians need to separate patients who can be safely managed as outpatients from those who need to be hospitalized. Disease severity is, of course, an important consideration in this selection process.3-8
For management of patients who will not be hospitalized, the WHO and the Society for Healthcare Epidemiology of America/Infectious Diseases Society of America (SHEA/IDSA) offer the 3 Ds: administer the correct drug, at the right dose, and for the appropriate duration, to minimize development and spread of resistance.9,10 A recent consensus conference coordinated by the Primary Care Education Consortium and Texas Academy of Family Physicians elaborated on this mnemonic as it relates to outpatient management of 3 CARTIs: community-acquired pneumonia, acute bacterial exacerbations of chronic bronchitis, and acute bacterial rhinosinusitis. Its recommendations, which have been drawn largely from existing evidence-based guidelines, form the basis for this review.
Drug selection
Treatment with an antibacterial agent will not be medically warranted in the majority of patients with a CARTI. Many of these patients will, however, expect to go home with an antibiotic prescription. The primary care clinician can reduce such expectations and prevent unnecessary reconsultations by briefly addressing four issues: 1) the natural course of the viral illness, 2) the lack of effectiveness of antibiotics, 3) the problem of antibiotic resistance, and 4) the side effects of antibiotics.11
When selecting an antibacterial agent for patients with pneumonia, bronchitis, or rhinosinusitis for which a bacterial cause has been identified or deemed likely, several factors need to be taken into account, including the suspected or identified pathogens, local resistance patterns, previous therapy, patient allergies, and the patient’s ability to tolerate treatment failure. Many of these factors are considered by professional organizations that regularly develop guidelines for CARTIs based on the best available evidence. Perhaps most critical for decision-making in the primary care setting is an understanding of evolving microbiology and resistance patterns.
Common pathogens
There is considerable overlap among pathogens commonly found in CARTIs. Streptococcus pneumoniae and Haemophilus influenzae are most often observed in the outpatient setting.
Community-acquired pneumonia. In outpatients with mild illness, S pneumoniae, Mycoplasma pneumoniae, Chlamydia species (particularly Chlamydia pneumoniae, now called Chlamydophilia pneumoniae), and H influenzae are the most common pathogens.12,13 In patients younger than 50 years without significant comorbidity, Mycoplasma species are the most common pathogens. Older patients and those with significant comorbidity are more likely infected with S pneumoniae,13 a Gram-negative enteric bacillus, Pseudomonas aeruginosa, or Legionella.5,14
Bacterial bronchitis. In addition to S pneumoniae and H influenzae, Moraxella catarrhalis is a frequent pathogen in bacterial exacerbations of chronic bronchitis.15P aeruginosa and other Gram-negative bacilli are also seen, especially in patients with a severe acute exacerbation who have a forced expiratory volume in 1 second (FEV1) of 35% of predicted or less.16 Infection due to multiple pathogens occurs in a small percentage of all patients with chronic bronchitis, particularly those with severe exacerbations. Fewer than 10% of acute exacerbations are due to an atypical bacterium, usually C pneumoniae. M pneumoniae and Legionella pneumophila are implicated even less frequently.15
Bacterial rhinosinusitis.S pneumoniae and H influenzae also are frequent causes of acute bacterial rhinosinusitis. Other pathogens commonly seen in this condition include other Streptococcus species, M catarrhalis, oral anaerobes, Staphylococcus aureus in adults, and M catarrhalis, Streptococcus pyogenes, and anaerobes in children.17
Resistance
Antibiotic resistance is an important consideration in the management of CARTIs. There is little doubt that widespread use of antibiotics leads to in vitro bacterial resistance.18-20 However, because clinical success has been observed in the presence of pathogens with low-level resistance, there is some debate as to whether low-level antibiotic resistance has a significant effect on clinical outcomes.18,21-29 Even so, the US Centers for Disease Control and Prevention has determined that people who attend or work at child-care centers and those who recently used antimicrobial agents are at increased risk for infection with drug-resistant S pneumoniae.30 Moreover, the WHO has stated that infection with resistant pathogens prolongs illness and increases the probability of a fatal outcome.31
Several surveillance programs that monitor antibiotic resistance patterns—including the Alexander Project32 and Tracking Resistance in the United States Today (TRUST)33-36 —have confirmed widespread resistance to antibiotics commonly used to treat CARTIs in the United States. β-Lactam resistance due to penicillin-binding protein changes in S pneumoniae has increased significantly over the past decade. Generally, more than 30% of S pneumoniae are now resistant to penicillins and macrolides (including azithromycin and clarithromycin, the ‘advanced’ agents in this group). A smaller number (6%) are resistant to amoxicillin/clavulanate, although this appears to be a result of in vitro test parameters involving primarily strains with high-level β-lactam resistance. Some cephalosporins also show greater activity than penicillin against intermediately susceptible S pneumoniae, but are not effective against highly resistant strains. In contrast, fewer than 1% of all pneumococci are resistant to newer fluoroquinolones (the so-called respiratory fluoroquinolones, such as gatifloxacin, gemifloxacin, levofloxacin, moxifloxacin) and the ketolide telithromycin.
The prevalence of β-lactamase–producing strains of H influenzae appears to have leveled off. Approximately 30% of H influenzae strains are resistant to ampicillin, while fewer than 1% are resistant to amoxicillin/clavulanate, cefuroxime, macrolides, and newer fluoroquinolones.
More than 90% of M catarrhalis isolates produce β-lactamase, thereby conferring resistance to ampicillin and amoxicillin.
Significant geographical variation in resistance has been observed. The prevalence of penicillin-resistant S pneumoniae ranges from 8% in New England to 25% in the South Atlantic, while ampicillin-resistant H influenzae is seen most often in New England (35%) and least often in the Rocky Mountain region (24%).33,34,36 Significant differences within a community also have been observed.37 Thus, knowledge of local resistance patterns is necessary. This information generally is available from local hospitals, although such data may be more reflective of nosocomial pathogens, or state health departments.
Community-acquired pneumonia
The 2003 guidelines of the IDSA give advanced macrolides and respiratory fluoroquinolones a prominent role in the management of community-acquired pneumonia (TABLE 1).5 The IDSA reviewed data from more than 150 clinical trials conducted in adults over 15 years. The IDSA panel acknowledged the increasing in vitro resistance of S pneumoniae to the macrolides, but noted that reports of clinical failure have not paralleled this. The panel also pointed out the significantly lower rates of resistance to the respiratory fluoroquinolones and expressed concern that abuse of these agents could lead to increased resistance by S pneumoniae.
In a previously healthy person who has not taken an antibiotic in the last 3 months, the IDSA recommends a macrolide or doxycycline as first-line therapy, whereas a fluoroquinolone, high-dose amoxicillin/clavulanate, or a macrolide plus high-dose amoxicillin should be used if an antibiotic has been taken during the last 3 months. Patients with a significant comorbidity can be treated with a fluoroquinolone without regard to recent antibiotic use. Alternatively, a macrolide can be used alone in patients who have not taken an antibiotic in 3 months, but otherwise must be used in combination with high-dose amoxicillin. High-dose amoxicillin/clavulanate or cefpodoxime, cefprozil, or cefuroxime can be used in those with a significant comorbidity and recent antibiotic use.
TABLE 1
Initial empiric therapy in outpatients with community-acquired pneumonia
| Clinical characteristics | No recent antibiotic therapy | Antibiotics during past 3 months |
|---|---|---|
| Previously healthy |
|
|
| Comorbidities (chronic obstructive pulmonary disease, diabetes, renal failure, congestive heart failure, malignancy) |
|
|
| Suspected aspiration with infection |
| |
| Influenza with bacterial superinfection |
| |
| Adapted from Mandell et al.5 © 2003 Infectious Diseases Society of America. | ||
Bacterial bronchitis
A panel of primary care physicians and specialists convened by the Canadian Thoracic Society (CTS) reviewed nearly 400 published articles on acute bacterial exacerbations of chronic bronchitis, including evidence-based reviews such as the Cochrane Database. The 2003 CTS guidelines recommend that treatment be based on the risk for treatment failure (TABLE 2).8
Antibacterial treatment is not recommended for patients whose clinical history and symptoms suggest a viral infection (group 0) unless symptoms persist for more than 10 to 14 days. In those cases, bacterial superinfection with M pneumoniae, C pneumoniae, or Bordetella pertussis is possible. Patients with chronic bronchitis but without risk factors for treatment failure (group 1) may be treated with a variety of first-line agents, including azithromycin, clarithromycin, cefuroxime, cefprozil, cefixime, amoxicillin, doxycycline, or trimethoprim/sulfamethoxazole. For patients in group 1 who fail first-line therapy, and as first-line therapy for patients in group 2, a fluoroquinolone or amoxicillin/clavulanate is recommended. Patients in group 3 are more likely to be infected with a Gram-negative pathogen, such as Ps aeruginosa or Enterobacter species, and are least able to tolerate treatment failure. Hence, ciprofloxacin is appropriate in the outpatient setting.
TABLE 2
Initial empiric therapy in outpatients with acute bacterial exacerbations of chronic bronchitis
| Group | Clinical status | Symptoms/risk factors | Initial treatment | Alternative when 1st-line agent fails |
|---|---|---|---|---|
| 0 | Acute tracheobronchitis |
|
|
|
| 1 | Chronic bronchitis without risk factors |
|
|
|
| 2 | Chronic bronchitis with risk factors |
|
|
|
| 3 | Chronic suppurative bronchitis |
|
| |
| Adapted from Balter et al,8 with permission. The publisher of Can Respir J does not assume responsibility for errors or discrepancies that may have occurred. | ||||
Bacterial rhinosinusitis
The recommendations for management of acute bacterial rhinosinusitis issued by the Sinus and Allergy Health Partnership (SAHP), a not-for-profit organization created by the American Academy of Otolaryngic Allergy, the American Academy of Otolaryngology-Head and Neck Surgery, and the American Rhinologic Society, are based on a variety of factors. These include rate of spontaneous resolution, pathogen distribution, antibacterial resistance data, the importance of S pneumoniae in intracranial and extrasinus complications, and the ability of a patient to tolerate treatment failure (TABLE 3).17 The panel reviewed more than 150 published articles on management of children and adults with bacterial rhinosinusitis.
As in the pneumonia guidelines, recent antibiotic use is an important consideration when selecting an antibiotic since resistant pathogens are likely. β-Lactam agents play a major role as initial therapy in both children and adults. This recommendation is consistent with those of Williams et al who reviewed 49 clinical trials involving 13,660 patients. These investigators recommended 7 to 14 days of penicillin or amoxicillin for acute maxillary sinusitis confirmed radiographically or by aspiration.38
The SAHP recommended higher doses of amoxicillin (with or without clavulanate) in patients who have recently taken an antibiotic or who have moderate disease. Fluoroquinolones are recommended as alternatives in patients with mild disease who have not taken an antibiotic in the last 4 to 6 weeks. However, in patients with mild disease who have taken antibiotics recently or who have moderate disease, fluoroquinolones are recommended as first-line therapy. Macrolides are recommended only for patients with a β-lactam allergy since failure rates of 20% to 25% are possible. Lack of improvement or worsening symptoms after 72 hours should prompt reevaluation, may necessitate cultures and/or a CT scan, and should raise the possibility of causal organisms other than S pneumoniae, H influenzae, and M catarrhalis.
TABLE 3
Initial empiric therapy in outpatients with acute bacterial rhinosinusitis
| Initial therapy | Alternative agent if no improvement or worsening after 72 hours | |
|---|---|---|
| Mild disease, no antibiotic during past 4 to 6 weeks | ||
| Children |
|
|
| Children with β-lactam allergy |
|
|
| Adults |
|
|
| Adults with β-lactam allergy |
|
|
| Mild disease and antibiotic during past 4 to 6 weeks or moderate disease | ||
| Children |
|
|
| Children with β-lactam allergy |
|
|
| Adults |
|
|
| Adults with β-lactam allergy |
|
|
| Adapted from Anon et al17 © 2004, with permission from American Academy of Otolaryngology-Head and Neck Surgery Foundation, Inc. | ||
Dose and duration
While each of the three guidelines provides detailed recommendations regarding selection of an antibacterial agent, the dose and duration of therapy generally are not well defined. Fortunately, other sources provide guidance in these 2 areas.
First, an independent international panel of infectious diseases experts, whose goal was to identify ways to improve prescription of antibiotics for lower respiratory tract infections, stressed that an important purpose of therapy is to reduce bacterial load and, in fact, treat to bacteriologic cure.19 Antibiotic therapy that allows some bacteria to survive increases the risk of early recurrence or relapse and encourages resistance selection. Such therapy is, therefore, inappropriate. The panel concurred with the WHO and others that the likelihood of bacterial persistence increases when antibiotics are prescribed in low doses, especially if given over long periods.18,39-41 Prolonged low-dose antibiotic therapy, which has been common practice for many infections, is contrary to the WHO Global Strategy for Containment of Antimicrobial Resistance, which notes that single-agent therapy for a short duration is 1 of several actions that can be taken to minimize bacterial resistance.42 Shorter courses of antibiotic therapy also are consistent with SHEA/IDSA recommendations.10
The clinical appropriateness of this recommendation is reinforced by the changes that have occurred during the past decade in the management of selected urinary tract infections (UTIs). Some UTIs that previously had been treated with low-dose antibiotics for 10 to 14 days now are treated with only 1 or a few high doses of a single agent. Other infections for which clinical data support shorter courses of antibiotic therapy include uncomplicated cellulitis,43 ventilator-associated pneumonia,44 and meningococcal disease.45
Shorter-course antibacterial therapy for CARTIs increasingly has been the focus of clinical trials. The focus is not unreasonable. Many of the antibiotics used for CARTIs are very potent against the pathogens commonly encountered, penetrate infected tissues well, are available in oral formulations, and are generally well tolerated. However, to optimize an antibiotic’s bactericidal potential, it is necessary to base the dosing regimen on its pharmacodynamics. From a pharmacodynamic perspective, there are 2 groups of antibiotics, those with concentration-dependent killing and those with time-dependent killing. For agents with concentration-dependent killing, such as fluoroquinolones, ketolides, and aminoglycosides, the goal is to select a dose that achieves a higher peak concentration and/or a larger area under the plasma concentration curve, with acceptable tolerability. In contrast, antibiotics that rely on time-dependent killing, such as β-lactams, macrolides, azalides, tetracyclines, and some others, require extended durations of concentrations above the MIC90 of the bacterial pathogen(s). Consequently, multiple daily dosing may be preferable.46
Dose. A few studies have compared high-dose, short-course therapy with therapy using standard doses and durations (TABLE 4). To assess the impact of highdose, short-course therapy on post-treatment resistant pneumococcal carriage, Schrag compared amoxicillin given either as 90 mg/kg/day for 5 days (high-dose, short-course) or 40 mg/kg/day for 10 days (standard) in 797 children with a respiratory tract infection.47 At day 28, nasal carriage of penicillin-resistant S pneumoniae was detected in 24% of the high-dose, shortcourse group and in 32% of the standard group (relative risk, 0.77; P=0.03). Among the pneumococcal carriers, the risk of penicillin-resistant S pneumoniae was significantly lower in the high-dose, short-course group than in the standard therapy group (relative risk, 0.78; P=0.01)
Another study investigated high-dose, short-course therapy with levofloxacin in patients with mild to severe community-acquired pneumonia. Patients received levofloxacin 750 mg/d for 5 days or 500 mg/d for 10 days.48 The clinical success rates were 92.4% and 91.1%, respectively, while the bacteriologic eradication rates at 7 to 14 days post-therapy were 93.2% and 92.4%, respectively, thereby demonstrating that high-dose, shortcourse levofloxacin therapy is at least as effective as standard levofloxacin therapy.
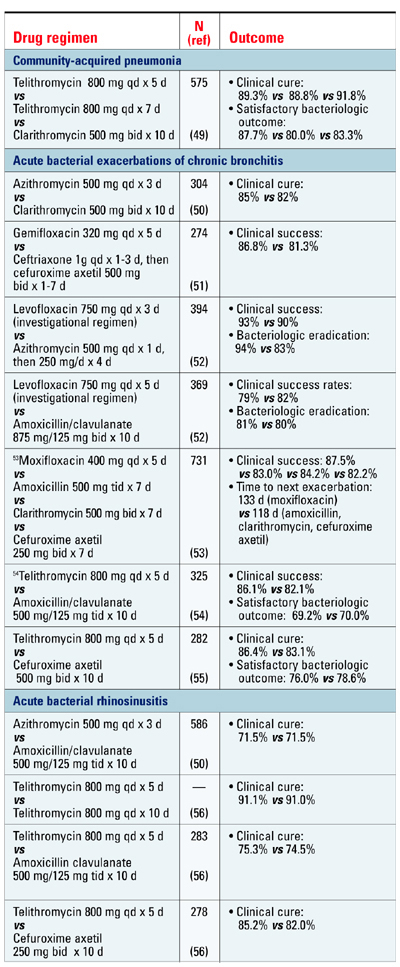
Duration. Short-course therapy using standard doses of azithromycin, gemifloxacin, levofloxacin, moxifloxacin, and telithromycin has been investigated in clinical trials of CARTIs (FIGURE). In patients with community-acquired pneumonia, 5 days of therapy with telithromycin was shown to be equivalent to a 7-day course (both using a single daily dose of 800 mg), as well as to clarithromycin 500 mg bid for 10 days.49
In studies of acute exacerbations of chronic bronchitis, a 3-day course of azithromycin was equivalent to clarithromycin for 10 days50 and gemifloxacin for 5 days was equivalent to a sequential combination of ceftriaxone and cefuroxime axetil for up to 10 days.51 Levofloxacin for 3 days and azithromycin for 5 days provided equivalent outcomes,52 as did levofloxacin for 5 days and amoxicillin/clavulanate for 10 days.52 Moxifloxacin for 5 days provided results equivalent to those of 7 days of amoxicillin, clarithromycin, or cefuroxime axetil.53 Five days of telithromycin was shown to be equivalent to 10 days of amoxicillin/clavu-lanate54 or cefuroxime axetil.55
Studies of acute bacterial rhinosinusitis have demonstrated equivalent results with azithromycin for 3 days and amoxicillin/clavulanate for 10 days.50 Similarly, telithromycin for 5 days was equivalent to 10 days of telithromycin, amoxicillin/clavulanate, or cefuroxime axetil.56
These clinical trials demonstrate that short-course therapy achieves clinical cure and/or bacteriologic eradication rates that are at least equivalent to those of standard therapy, with no significant difference in safety. Symptomatic improvement is faster and total antibiotic exposure is reduced with short-course therapy.
A significant advantage of short-course antibacterial therapy is improved patient adherence. Adherence is 10% to 20% better with 5-day courses than with 10-day courses,47,57 and is significantly better with 1 or 2 daily doses than with 3 or more daily doses.58-60 In fact, a recent market research study showed that patients perceive once-daily, short-course antibiotic treatment to be significantly more effective than longer courses. This may be due to faster improvement of infection-related symptoms.61 For example, Dunbar et al observed that significantly more patients treated with high-dose, short-course levofloxacin experienced subjective and objective resolution of fever by day 3 compared with those who received standard-dose, short-course levofloxacin.48
TABLE 4
Clinical trials of high-dose, short-course antibiotic therapy
| Drug regimen | N (ref) | Outcome |
|---|---|---|
| Amoxicillin 90 mg/kg/d x 5 d vs Amoxicillin 40 mg/kg/d x 10 d | 797 |
|
| (47) | ||
| Levofloxacin 750 mg/d x 5d vs Levofloxacin 500 mg/d x 10 d | 390 |
|
| (48) |
TABLE 5 Clinical trials of standard-dose, short-course antibiotic therapy
Summary
Essential questions that need to be answered for every patient who presents with a possible CARTI include : 1) Is antibacterial therapy necessary? 2) If so, what is the best antibiotic and at what dose and for how long should it be administered? Accumulating evidence indicates that some antibiotics when given in high doses for a short duration are as effective and safe as standard therapy for CARTIs. Short-course therapy also promotes patient compliance.
Disclosures:
The authors reported the following financial relationships: Dr Brunton: consultant to Abbott, Ortho-McNeil Pharmaceutical, Inc., and SanofiAventis. Dr Carmichael: consultant to Ortho-McNeil Pharmaceutical, Inc.; on the speakers’ bureaus for Bristol-Myers Squibb Company, Merck & Co., OrthoMcNeil Pharmaceutical, Inc., and Pfizer Inc. Dr Fitzgerald: on the speakers’ bureaus for Boehringer Ingelheim, GlaxoSmithKline, Ortho-McNeil Pharmaceutical, Inc., Pfizer Inc., Sepracor Inc., and 3M. Dr Liu: on the speakers’ bureaus for Aventis Pharmaceuticals, Bayer Pharmaceuticals Corporation, Bristol-Myers Squibb Company, Cobist, GlaxoSmithKline, Merck & Co., Ortho-McNeil Pharmaceutical, Inc., Pfizer Inc., Purdue Pharma, Oscient Pharmaceuticals Corporation, and Wyeth Pharmaceuticals. Dr Varon: on the speakers’ bureau for Ortho-McNeil Pharmaceutical, Inc. Dr. Weiland: consultant to Abbott Laboratories, Ortho-McNeil Pharmaceutical, Inc., and Pfizer Inc.
This supplement to The Journal of Family Practice is supported by a grant from Ortho-McNeil Pharmaceutical, Inc. It was adapted from a consensus conference coordinated by the Primary Care Education Consortium and Texas Academy of Family Physicians and was edited and peer-reviewed by The Journal of Family Practice. © 2005 Quadrant HealthCom Inc. and Primary Care Education Consortium.
- To minimize development and spread of antibiotic resistance, it is important to administer the correct antibacterial, by the best route, in the right amount, at optimum intervals, and for the appropriate duration.
- Streptococcus pneumoniae and Haemophilus influenzae are the 2 most common bacterial pathogens observed in community-acquired respiratory tract infections.
- Surveillance studies indicate increasing rates of in vitro resistance by S pneumoniae to many β-lactam and macrolide antibiotics.
- To minimize risk of resistance-associated recurrence or relapse, antibacterial agents should be prescribed in accordance with existing guidelines and local resistance patterns. Patient compliance with dosage and duration of therapy should be fostered.
- Preliminary data suggest that high-dose, short-course antibacterial therapy may be as effective as longer courses of low-dose therapy.
Community-acquired respiratory tract infections (CARTIs) are a reason for seeking medical attention. In 2001, there were 28.4 million office visits in the United States for an acute respiratory tract infection (excluding pharyngitis).1
Management of CARTIs poses several challenges. According to the World Health Organization (WHO), “for every 100 respiratory infections, only 20% require antibiotic treatment”2 —the remaining 80 infections most likely have a viral origin. Thus, antibacterial therapy should be avoided unless a bacterial cause has been confirmed or is deemed likely.
Once that determination has been made, clinicians need to separate patients who can be safely managed as outpatients from those who need to be hospitalized. Disease severity is, of course, an important consideration in this selection process.3-8
For management of patients who will not be hospitalized, the WHO and the Society for Healthcare Epidemiology of America/Infectious Diseases Society of America (SHEA/IDSA) offer the 3 Ds: administer the correct drug, at the right dose, and for the appropriate duration, to minimize development and spread of resistance.9,10 A recent consensus conference coordinated by the Primary Care Education Consortium and Texas Academy of Family Physicians elaborated on this mnemonic as it relates to outpatient management of 3 CARTIs: community-acquired pneumonia, acute bacterial exacerbations of chronic bronchitis, and acute bacterial rhinosinusitis. Its recommendations, which have been drawn largely from existing evidence-based guidelines, form the basis for this review.
Drug selection
Treatment with an antibacterial agent will not be medically warranted in the majority of patients with a CARTI. Many of these patients will, however, expect to go home with an antibiotic prescription. The primary care clinician can reduce such expectations and prevent unnecessary reconsultations by briefly addressing four issues: 1) the natural course of the viral illness, 2) the lack of effectiveness of antibiotics, 3) the problem of antibiotic resistance, and 4) the side effects of antibiotics.11
When selecting an antibacterial agent for patients with pneumonia, bronchitis, or rhinosinusitis for which a bacterial cause has been identified or deemed likely, several factors need to be taken into account, including the suspected or identified pathogens, local resistance patterns, previous therapy, patient allergies, and the patient’s ability to tolerate treatment failure. Many of these factors are considered by professional organizations that regularly develop guidelines for CARTIs based on the best available evidence. Perhaps most critical for decision-making in the primary care setting is an understanding of evolving microbiology and resistance patterns.
Common pathogens
There is considerable overlap among pathogens commonly found in CARTIs. Streptococcus pneumoniae and Haemophilus influenzae are most often observed in the outpatient setting.
Community-acquired pneumonia. In outpatients with mild illness, S pneumoniae, Mycoplasma pneumoniae, Chlamydia species (particularly Chlamydia pneumoniae, now called Chlamydophilia pneumoniae), and H influenzae are the most common pathogens.12,13 In patients younger than 50 years without significant comorbidity, Mycoplasma species are the most common pathogens. Older patients and those with significant comorbidity are more likely infected with S pneumoniae,13 a Gram-negative enteric bacillus, Pseudomonas aeruginosa, or Legionella.5,14
Bacterial bronchitis. In addition to S pneumoniae and H influenzae, Moraxella catarrhalis is a frequent pathogen in bacterial exacerbations of chronic bronchitis.15P aeruginosa and other Gram-negative bacilli are also seen, especially in patients with a severe acute exacerbation who have a forced expiratory volume in 1 second (FEV1) of 35% of predicted or less.16 Infection due to multiple pathogens occurs in a small percentage of all patients with chronic bronchitis, particularly those with severe exacerbations. Fewer than 10% of acute exacerbations are due to an atypical bacterium, usually C pneumoniae. M pneumoniae and Legionella pneumophila are implicated even less frequently.15
Bacterial rhinosinusitis.S pneumoniae and H influenzae also are frequent causes of acute bacterial rhinosinusitis. Other pathogens commonly seen in this condition include other Streptococcus species, M catarrhalis, oral anaerobes, Staphylococcus aureus in adults, and M catarrhalis, Streptococcus pyogenes, and anaerobes in children.17
Resistance
Antibiotic resistance is an important consideration in the management of CARTIs. There is little doubt that widespread use of antibiotics leads to in vitro bacterial resistance.18-20 However, because clinical success has been observed in the presence of pathogens with low-level resistance, there is some debate as to whether low-level antibiotic resistance has a significant effect on clinical outcomes.18,21-29 Even so, the US Centers for Disease Control and Prevention has determined that people who attend or work at child-care centers and those who recently used antimicrobial agents are at increased risk for infection with drug-resistant S pneumoniae.30 Moreover, the WHO has stated that infection with resistant pathogens prolongs illness and increases the probability of a fatal outcome.31
Several surveillance programs that monitor antibiotic resistance patterns—including the Alexander Project32 and Tracking Resistance in the United States Today (TRUST)33-36 —have confirmed widespread resistance to antibiotics commonly used to treat CARTIs in the United States. β-Lactam resistance due to penicillin-binding protein changes in S pneumoniae has increased significantly over the past decade. Generally, more than 30% of S pneumoniae are now resistant to penicillins and macrolides (including azithromycin and clarithromycin, the ‘advanced’ agents in this group). A smaller number (6%) are resistant to amoxicillin/clavulanate, although this appears to be a result of in vitro test parameters involving primarily strains with high-level β-lactam resistance. Some cephalosporins also show greater activity than penicillin against intermediately susceptible S pneumoniae, but are not effective against highly resistant strains. In contrast, fewer than 1% of all pneumococci are resistant to newer fluoroquinolones (the so-called respiratory fluoroquinolones, such as gatifloxacin, gemifloxacin, levofloxacin, moxifloxacin) and the ketolide telithromycin.
The prevalence of β-lactamase–producing strains of H influenzae appears to have leveled off. Approximately 30% of H influenzae strains are resistant to ampicillin, while fewer than 1% are resistant to amoxicillin/clavulanate, cefuroxime, macrolides, and newer fluoroquinolones.
More than 90% of M catarrhalis isolates produce β-lactamase, thereby conferring resistance to ampicillin and amoxicillin.
Significant geographical variation in resistance has been observed. The prevalence of penicillin-resistant S pneumoniae ranges from 8% in New England to 25% in the South Atlantic, while ampicillin-resistant H influenzae is seen most often in New England (35%) and least often in the Rocky Mountain region (24%).33,34,36 Significant differences within a community also have been observed.37 Thus, knowledge of local resistance patterns is necessary. This information generally is available from local hospitals, although such data may be more reflective of nosocomial pathogens, or state health departments.
Community-acquired pneumonia
The 2003 guidelines of the IDSA give advanced macrolides and respiratory fluoroquinolones a prominent role in the management of community-acquired pneumonia (TABLE 1).5 The IDSA reviewed data from more than 150 clinical trials conducted in adults over 15 years. The IDSA panel acknowledged the increasing in vitro resistance of S pneumoniae to the macrolides, but noted that reports of clinical failure have not paralleled this. The panel also pointed out the significantly lower rates of resistance to the respiratory fluoroquinolones and expressed concern that abuse of these agents could lead to increased resistance by S pneumoniae.
In a previously healthy person who has not taken an antibiotic in the last 3 months, the IDSA recommends a macrolide or doxycycline as first-line therapy, whereas a fluoroquinolone, high-dose amoxicillin/clavulanate, or a macrolide plus high-dose amoxicillin should be used if an antibiotic has been taken during the last 3 months. Patients with a significant comorbidity can be treated with a fluoroquinolone without regard to recent antibiotic use. Alternatively, a macrolide can be used alone in patients who have not taken an antibiotic in 3 months, but otherwise must be used in combination with high-dose amoxicillin. High-dose amoxicillin/clavulanate or cefpodoxime, cefprozil, or cefuroxime can be used in those with a significant comorbidity and recent antibiotic use.
TABLE 1
Initial empiric therapy in outpatients with community-acquired pneumonia
| Clinical characteristics | No recent antibiotic therapy | Antibiotics during past 3 months |
|---|---|---|
| Previously healthy |
|
|
| Comorbidities (chronic obstructive pulmonary disease, diabetes, renal failure, congestive heart failure, malignancy) |
|
|
| Suspected aspiration with infection |
| |
| Influenza with bacterial superinfection |
| |
| Adapted from Mandell et al.5 © 2003 Infectious Diseases Society of America. | ||
Bacterial bronchitis
A panel of primary care physicians and specialists convened by the Canadian Thoracic Society (CTS) reviewed nearly 400 published articles on acute bacterial exacerbations of chronic bronchitis, including evidence-based reviews such as the Cochrane Database. The 2003 CTS guidelines recommend that treatment be based on the risk for treatment failure (TABLE 2).8
Antibacterial treatment is not recommended for patients whose clinical history and symptoms suggest a viral infection (group 0) unless symptoms persist for more than 10 to 14 days. In those cases, bacterial superinfection with M pneumoniae, C pneumoniae, or Bordetella pertussis is possible. Patients with chronic bronchitis but without risk factors for treatment failure (group 1) may be treated with a variety of first-line agents, including azithromycin, clarithromycin, cefuroxime, cefprozil, cefixime, amoxicillin, doxycycline, or trimethoprim/sulfamethoxazole. For patients in group 1 who fail first-line therapy, and as first-line therapy for patients in group 2, a fluoroquinolone or amoxicillin/clavulanate is recommended. Patients in group 3 are more likely to be infected with a Gram-negative pathogen, such as Ps aeruginosa or Enterobacter species, and are least able to tolerate treatment failure. Hence, ciprofloxacin is appropriate in the outpatient setting.
TABLE 2
Initial empiric therapy in outpatients with acute bacterial exacerbations of chronic bronchitis
| Group | Clinical status | Symptoms/risk factors | Initial treatment | Alternative when 1st-line agent fails |
|---|---|---|---|---|
| 0 | Acute tracheobronchitis |
|
|
|
| 1 | Chronic bronchitis without risk factors |
|
|
|
| 2 | Chronic bronchitis with risk factors |
|
|
|
| 3 | Chronic suppurative bronchitis |
|
| |
| Adapted from Balter et al,8 with permission. The publisher of Can Respir J does not assume responsibility for errors or discrepancies that may have occurred. | ||||
Bacterial rhinosinusitis
The recommendations for management of acute bacterial rhinosinusitis issued by the Sinus and Allergy Health Partnership (SAHP), a not-for-profit organization created by the American Academy of Otolaryngic Allergy, the American Academy of Otolaryngology-Head and Neck Surgery, and the American Rhinologic Society, are based on a variety of factors. These include rate of spontaneous resolution, pathogen distribution, antibacterial resistance data, the importance of S pneumoniae in intracranial and extrasinus complications, and the ability of a patient to tolerate treatment failure (TABLE 3).17 The panel reviewed more than 150 published articles on management of children and adults with bacterial rhinosinusitis.
As in the pneumonia guidelines, recent antibiotic use is an important consideration when selecting an antibiotic since resistant pathogens are likely. β-Lactam agents play a major role as initial therapy in both children and adults. This recommendation is consistent with those of Williams et al who reviewed 49 clinical trials involving 13,660 patients. These investigators recommended 7 to 14 days of penicillin or amoxicillin for acute maxillary sinusitis confirmed radiographically or by aspiration.38
The SAHP recommended higher doses of amoxicillin (with or without clavulanate) in patients who have recently taken an antibiotic or who have moderate disease. Fluoroquinolones are recommended as alternatives in patients with mild disease who have not taken an antibiotic in the last 4 to 6 weeks. However, in patients with mild disease who have taken antibiotics recently or who have moderate disease, fluoroquinolones are recommended as first-line therapy. Macrolides are recommended only for patients with a β-lactam allergy since failure rates of 20% to 25% are possible. Lack of improvement or worsening symptoms after 72 hours should prompt reevaluation, may necessitate cultures and/or a CT scan, and should raise the possibility of causal organisms other than S pneumoniae, H influenzae, and M catarrhalis.
TABLE 3
Initial empiric therapy in outpatients with acute bacterial rhinosinusitis
| Initial therapy | Alternative agent if no improvement or worsening after 72 hours | |
|---|---|---|
| Mild disease, no antibiotic during past 4 to 6 weeks | ||
| Children |
|
|
| Children with β-lactam allergy |
|
|
| Adults |
|
|
| Adults with β-lactam allergy |
|
|
| Mild disease and antibiotic during past 4 to 6 weeks or moderate disease | ||
| Children |
|
|
| Children with β-lactam allergy |
|
|
| Adults |
|
|
| Adults with β-lactam allergy |
|
|
| Adapted from Anon et al17 © 2004, with permission from American Academy of Otolaryngology-Head and Neck Surgery Foundation, Inc. | ||
Dose and duration
While each of the three guidelines provides detailed recommendations regarding selection of an antibacterial agent, the dose and duration of therapy generally are not well defined. Fortunately, other sources provide guidance in these 2 areas.
First, an independent international panel of infectious diseases experts, whose goal was to identify ways to improve prescription of antibiotics for lower respiratory tract infections, stressed that an important purpose of therapy is to reduce bacterial load and, in fact, treat to bacteriologic cure.19 Antibiotic therapy that allows some bacteria to survive increases the risk of early recurrence or relapse and encourages resistance selection. Such therapy is, therefore, inappropriate. The panel concurred with the WHO and others that the likelihood of bacterial persistence increases when antibiotics are prescribed in low doses, especially if given over long periods.18,39-41 Prolonged low-dose antibiotic therapy, which has been common practice for many infections, is contrary to the WHO Global Strategy for Containment of Antimicrobial Resistance, which notes that single-agent therapy for a short duration is 1 of several actions that can be taken to minimize bacterial resistance.42 Shorter courses of antibiotic therapy also are consistent with SHEA/IDSA recommendations.10
The clinical appropriateness of this recommendation is reinforced by the changes that have occurred during the past decade in the management of selected urinary tract infections (UTIs). Some UTIs that previously had been treated with low-dose antibiotics for 10 to 14 days now are treated with only 1 or a few high doses of a single agent. Other infections for which clinical data support shorter courses of antibiotic therapy include uncomplicated cellulitis,43 ventilator-associated pneumonia,44 and meningococcal disease.45
Shorter-course antibacterial therapy for CARTIs increasingly has been the focus of clinical trials. The focus is not unreasonable. Many of the antibiotics used for CARTIs are very potent against the pathogens commonly encountered, penetrate infected tissues well, are available in oral formulations, and are generally well tolerated. However, to optimize an antibiotic’s bactericidal potential, it is necessary to base the dosing regimen on its pharmacodynamics. From a pharmacodynamic perspective, there are 2 groups of antibiotics, those with concentration-dependent killing and those with time-dependent killing. For agents with concentration-dependent killing, such as fluoroquinolones, ketolides, and aminoglycosides, the goal is to select a dose that achieves a higher peak concentration and/or a larger area under the plasma concentration curve, with acceptable tolerability. In contrast, antibiotics that rely on time-dependent killing, such as β-lactams, macrolides, azalides, tetracyclines, and some others, require extended durations of concentrations above the MIC90 of the bacterial pathogen(s). Consequently, multiple daily dosing may be preferable.46
Dose. A few studies have compared high-dose, short-course therapy with therapy using standard doses and durations (TABLE 4). To assess the impact of highdose, short-course therapy on post-treatment resistant pneumococcal carriage, Schrag compared amoxicillin given either as 90 mg/kg/day for 5 days (high-dose, short-course) or 40 mg/kg/day for 10 days (standard) in 797 children with a respiratory tract infection.47 At day 28, nasal carriage of penicillin-resistant S pneumoniae was detected in 24% of the high-dose, shortcourse group and in 32% of the standard group (relative risk, 0.77; P=0.03). Among the pneumococcal carriers, the risk of penicillin-resistant S pneumoniae was significantly lower in the high-dose, short-course group than in the standard therapy group (relative risk, 0.78; P=0.01)
Another study investigated high-dose, short-course therapy with levofloxacin in patients with mild to severe community-acquired pneumonia. Patients received levofloxacin 750 mg/d for 5 days or 500 mg/d for 10 days.48 The clinical success rates were 92.4% and 91.1%, respectively, while the bacteriologic eradication rates at 7 to 14 days post-therapy were 93.2% and 92.4%, respectively, thereby demonstrating that high-dose, shortcourse levofloxacin therapy is at least as effective as standard levofloxacin therapy.
Duration. Short-course therapy using standard doses of azithromycin, gemifloxacin, levofloxacin, moxifloxacin, and telithromycin has been investigated in clinical trials of CARTIs (FIGURE). In patients with community-acquired pneumonia, 5 days of therapy with telithromycin was shown to be equivalent to a 7-day course (both using a single daily dose of 800 mg), as well as to clarithromycin 500 mg bid for 10 days.49
In studies of acute exacerbations of chronic bronchitis, a 3-day course of azithromycin was equivalent to clarithromycin for 10 days50 and gemifloxacin for 5 days was equivalent to a sequential combination of ceftriaxone and cefuroxime axetil for up to 10 days.51 Levofloxacin for 3 days and azithromycin for 5 days provided equivalent outcomes,52 as did levofloxacin for 5 days and amoxicillin/clavulanate for 10 days.52 Moxifloxacin for 5 days provided results equivalent to those of 7 days of amoxicillin, clarithromycin, or cefuroxime axetil.53 Five days of telithromycin was shown to be equivalent to 10 days of amoxicillin/clavu-lanate54 or cefuroxime axetil.55
Studies of acute bacterial rhinosinusitis have demonstrated equivalent results with azithromycin for 3 days and amoxicillin/clavulanate for 10 days.50 Similarly, telithromycin for 5 days was equivalent to 10 days of telithromycin, amoxicillin/clavulanate, or cefuroxime axetil.56
These clinical trials demonstrate that short-course therapy achieves clinical cure and/or bacteriologic eradication rates that are at least equivalent to those of standard therapy, with no significant difference in safety. Symptomatic improvement is faster and total antibiotic exposure is reduced with short-course therapy.
A significant advantage of short-course antibacterial therapy is improved patient adherence. Adherence is 10% to 20% better with 5-day courses than with 10-day courses,47,57 and is significantly better with 1 or 2 daily doses than with 3 or more daily doses.58-60 In fact, a recent market research study showed that patients perceive once-daily, short-course antibiotic treatment to be significantly more effective than longer courses. This may be due to faster improvement of infection-related symptoms.61 For example, Dunbar et al observed that significantly more patients treated with high-dose, short-course levofloxacin experienced subjective and objective resolution of fever by day 3 compared with those who received standard-dose, short-course levofloxacin.48
TABLE 4
Clinical trials of high-dose, short-course antibiotic therapy
| Drug regimen | N (ref) | Outcome |
|---|---|---|
| Amoxicillin 90 mg/kg/d x 5 d vs Amoxicillin 40 mg/kg/d x 10 d | 797 |
|
| (47) | ||
| Levofloxacin 750 mg/d x 5d vs Levofloxacin 500 mg/d x 10 d | 390 |
|
| (48) |
TABLE 5 Clinical trials of standard-dose, short-course antibiotic therapy
Summary
Essential questions that need to be answered for every patient who presents with a possible CARTI include : 1) Is antibacterial therapy necessary? 2) If so, what is the best antibiotic and at what dose and for how long should it be administered? Accumulating evidence indicates that some antibiotics when given in high doses for a short duration are as effective and safe as standard therapy for CARTIs. Short-course therapy also promotes patient compliance.
Disclosures:
The authors reported the following financial relationships: Dr Brunton: consultant to Abbott, Ortho-McNeil Pharmaceutical, Inc., and SanofiAventis. Dr Carmichael: consultant to Ortho-McNeil Pharmaceutical, Inc.; on the speakers’ bureaus for Bristol-Myers Squibb Company, Merck & Co., OrthoMcNeil Pharmaceutical, Inc., and Pfizer Inc. Dr Fitzgerald: on the speakers’ bureaus for Boehringer Ingelheim, GlaxoSmithKline, Ortho-McNeil Pharmaceutical, Inc., Pfizer Inc., Sepracor Inc., and 3M. Dr Liu: on the speakers’ bureaus for Aventis Pharmaceuticals, Bayer Pharmaceuticals Corporation, Bristol-Myers Squibb Company, Cobist, GlaxoSmithKline, Merck & Co., Ortho-McNeil Pharmaceutical, Inc., Pfizer Inc., Purdue Pharma, Oscient Pharmaceuticals Corporation, and Wyeth Pharmaceuticals. Dr Varon: on the speakers’ bureau for Ortho-McNeil Pharmaceutical, Inc. Dr. Weiland: consultant to Abbott Laboratories, Ortho-McNeil Pharmaceutical, Inc., and Pfizer Inc.
This supplement to The Journal of Family Practice is supported by a grant from Ortho-McNeil Pharmaceutical, Inc. It was adapted from a consensus conference coordinated by the Primary Care Education Consortium and Texas Academy of Family Physicians and was edited and peer-reviewed by The Journal of Family Practice. © 2005 Quadrant HealthCom Inc. and Primary Care Education Consortium.
1. Centers for Disease Control and Prevention. National Center for Health Statistics website. National Ambulatory Medical Care Survey: 2001 Summary. Available at: http://www.cdc.gov/nchs/data/ad/ad337.pdf. Accessed February 2, 2005.
2. World Health Organization.World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 4. Big guns of resistance. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
3. Metlay JP, Fine MJ. Testing strategies in the initial management of patients with community-acquired pneumonia. Ann Intern Med. 2003;138:109-118.
4. File TM. Community-acquired pneumonia. Lancet. 2003;362:1991-2001.
5. Mandell LA, Bartlett JG, Dowell SF, File TM, Jr, Musher DM, Whitney C. Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clin Infect Dis. 2003;37:1405-1433.
6. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336:243-250.
7. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106:196-204.
8. Balter MS, La Forge J, Low DE, Mandell L, Grossman RF. Canadian guidelines for the management of acute exacerbations of chronic bronchitis. Can Respir J. 2003;10(suppl B):3B-32B.
9. World Health Organization. World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 5. A call to action: A massive effort to provide proper treatment. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
10. Shlaes DM, Gerding DN, John JF, Jr, et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the Prevention of Antimicrobial Resistance: guidelines for the prevention of antimicrobial resistance in hospitals. Clin Infect Dis. 1997;25:584-599.
11. Scottish Intercollegiate Guidelines Network. National Guideline Clearinghouse website. Community management of lower respiratory tract infection in adults. A national clinical guideline. Available at: http://www.guideline.gov/summary/summary.aspx?ss=15& doc_id=3361&nbr=2587&string=respiratory%20AND%20tract%20AND% 20infection. Accessed December 17, 2004.
12. Bochud PY, Moser F, Erard P, et al. Community-acquired pneumonia. A prospective outpatient study. Medicine (Baltimore). 2001;80:75-87.
13. Falguera M, Sacristan O, Nogues A, et al. Nonsevere community-acquired pneumonia: correlation between cause and severity or comorbidity. Arch Intern Med. 2001;161:1866-1872.
14. Ruiz M, Ewig S, Marcos MA, et al. Etiology of community-acquired pneumonia: impact of age, comorbidity, and severity. Am J Respir Crit Care Med. 1999;160:397-405.
15. Sethi S. Infectious etiology of acute exacerbations of chronic bronchitis. Chest. 2000;117(5 Suppl 2):380S-385S.
16. Eller J, Ede A, Schaberg T, Niederman MS, Mauch H, Lode H. Infective exacerbations of chronic bronchitis: relation between bacteriologic etiology and lung function. Chest. 1998;113:1542-1548.
17. Anon JB, Jacobs MR, Poole MD, et al. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg. 2004;130(1 Suppl):1-45.
18. Albrich WC, Monnet DL, Harbarth S. Antibiotic selection pressure and resistance in Streptococcus pneumoniae. and Streptococcus pyogenes. Emerg Infect Dis. 2004;10:514-517.
19. Ball P, Baquero F, Cars O, et al. Antibiotic therapy of community respiratory tract infections: strategies for optimal outcomes and minimized resistance emergence. J Antimicrob Chemother. 2002;49:31-40.
20. Harbarth S, Albrich W, Brun-Buisson C. Outpatient antibiotic use and prevalence of antibiotic-resistant pneumococci in France and Germany: a sociocultural perspective. Emerg Infect Dis. 2002;8:1460-1467.
21. Lonks JR, Garau J, Medeiros AA. Implications of antimicrobial resistance in the empirical treatment of community-acquired respiratory tract infections: the case of macrolides. J Antimicrob Chemother. 2002;50(Suppl S2):87-92.
22. Lonks JR, Garau J, Gomez L, et al. Failure of macrolide antibiotic treatment in patients with bacteremia due to erythromycin-resistant Streptococcus pneumoniae. Clin Infect Dis. 2002;35:556-564.
23. Moellering RC, Jr, Craig W, Edmond M, et al. Clinical and public health implications of macrolide-resistant Streptococcus pneumoniae. J Chemother. 2002;14(suppl 3):42-56.
24. Davidson R, Cavalcanti R, Brunton JL, et al. Resistance to levofloxacin and failure of treatment of pneumococcal pneumonia. N Engl J Med. 2002;346:747-750.
25. Musher DM, Dowell ME, Shortridge VD, et al. Emergence of macrolide resistance during treatment of pneumococcal pneumonia. N Engl J Med. 2002;346:630-631.
26. Waterer GW, Buckingham SC, Kessler LA, Quasney MW, Wunderink RG. Decreasing β-lactam resistance in Pneumococci. from the Memphis region: analysis of 2,152 isolates From 1996 to 2001. Chest. 2003;124:519-525.
27. Nuermberger E, Bishai WR. The clinical significance of macrolide-resistant Streptococcus pneumoniae.: it’s all relative. Clin Infect Dis. 2004;38:99-103.
28. Yu VL, Chiou CC, Feldman C, et al. An international prospective study of pneumococcal bacteremia: correlation with in vitro resistance, antibiotics administered, and clinical outcome. Clin Infect Dis. 2003;37:230-237.
29. Metlay JP. Update on community-acquired pneumonia: impact of antibiotic resistance on clinical outcomes. Curr Opin Infect Dis. 2002;15:163-167.
30. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention web site. Drug-resistant Streptococcus pneumoniae disease. Available at: http://www.cdc.gov/ncidod/dbmd/diseaseinfo/drugresisstreppneum_t.htm. Accessed January 4, 2005.
31. World Health Organization World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 3. Factors contributing to resistance. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
32. Jacobs MR, Felmingham D, Appelbaum PC, Gruneberg RN. The Alexander Project 1998-2000: susceptibility of pathogens isolated from communityacquired respiratory tract infection to commonly used antimicrobial agents. J Antimicrob Chemother. 2003;52:229-246.
33. Thornsberry C, Sahm DF, Kelly LJ, et al. Regional trends in antimicrobial resistance among clinical isolates of Streptococcus pneumoniae., Haemophilus influenzae., and Moraxella catarrhalis. in the United States: results from the TRUST Surveillance Program, 1999-2000. Clin Infect Dis. 2002;34(suppl 1):S4-S16.
34. Karlowsky JA, Thornsberry C, Jones ME, Evangelista AT, Critchley IA, Sahm DF. Factors associated with relative rates of antimicrobial resistance among Streptococcus pneumoniae. in the United States: results from the TRUST Surveillance Program (1998-2002). Clin Infect Dis. 2003;36:963-970.
35. Karlowsky JA, Kelly LJ, Thornsberry C, et al. Susceptibility to fluoroquinolones among commonly isolated Gram-negative bacilli in 2000: TRUST and TSN data for the United States. Tracking Resistance in the United States Today. The Surveillance Network. Int J Antimicrob Agents. 2002;19:21-31.
36. Karlowsky JA, Thornsberry C, Critchley IA, et al. Susceptibilities to levofloxacin in Streptococcus pneumoniae., Haemophilus influenzae., and Moraxella catarrhalis. clinical isolates from children: results from 2000-2001 and 2001-2002 TRUST studies in the United States. Antimicrob Agents Chemother. 2003;47:1790-1797.
37. Quale J, Landman D, Ravishankar J, Flores C, Bratu S. Streptococcus pneumo.-niae., Brooklyn, New York: fluoroquinolone resistance at our doorstep. Emerg Infect Dis. 2002;8:594-597.
38. Williams JW, Jr, Aguilar C, Cornell J, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2004;2:CD000243.-
39. Guillemot D, Carbon C, Balkau B, et al. Low dosage and long treatment duration of β-lactam: risk factors for carriage of penicillin-resistant Streptococcus pneumoniae. JAMA. 1998;279:365-370.
40. Scheld WM. Maintaining fluoroquinolone class efficacy: review of influencing factors. Emerg Infect Dis. 2003;9:1-9.
41. Thomson KS. Minimizing quinolone resistance: are the new agents more or less likely to cause resistance? J Antimicrob Chemother. 2000;45:719-723.
42. World Health Organization. World Health Organization web site. WHO global strategy for containment of antimicrobial resistance. Available at: http://www.who.int/csr/resources/publications/drugresist/en/EGlobal_Strat.pdf. Accessed February 2, 2005.
43. Hepburn MJ, Dooley DP, Skidmore PJ, Ellis MW, Starnes WF, Hasewinkle WC. Comparison of short-course (5 days) and standard (10 days) treatment for uncomplicated cellulitis. Arch Intern Med. 2004;164:1669-1674.
44. Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588-2598.
45. Ellis-Pegler R, Galler L, Roberts S, Thomas M, Woodhouse A. Three days of intravenous benzyl penicillin treatment of meningococcal disease in adults. Clin Infect Dis. 2003;37:658-662.
46. Craig WA. Basic pharmacodynamics of antibacterials with clinical applications to the use of β-lactams, glycopeptides, and linezolid. Infect Dis Clin North Am. 2003;17:479-501.
47. Schrag SJ, Pena C, Fernandez J, et al. Effect of short-course, high-dose amoxicillin therapy on resistant pneumococcal carriage: a randomized trial. JAMA. 2001;286:49-56.
48. Dunbar LM, Wunderink RG, Habib MP, et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
49. Tellier G, Niederman MS, Nusrat R, Patel M, Lavin B. Clinical and bacteriological efficacy and safety of 5 and 7 day regimens of telithromycin once daily compared with a 10 day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515-523.
50. Zithromax [prescribing information] New York, NY: Pfizer Labs; 2004.
51. Wilson R, Langan C, Ball P, Bateman K, Pypstra R. Oral gemifloxacin once daily for 5 days compared with sequential therapy with i.v. ceftriaxone/oral cefuroxime (maximum of 10 days) in the treatment of hospitalized patients with acute exacerbations of chronic bronchitis. Respir Med. 2003;97:242-249.
52. Tennenberg A, Walker K, Khashab M, Zadelkis N. The safety and efficacy of short-course (3-5 days), 750 mg levofloxacin (LVX) for acute bacterial exacerbation of chronic bronchitis (ABECB). Presented at: American Thoracic Society 100th International Conference, May 21-26, 2004, Orlando, Fl.
53. Wilson R, Allegra L, Huchon G, et al. Short-term and long-term outcomes of moxifloxacin compared to standard antibiotic treatment in acute exacerbations of chronic bronchitis. Chest. 2004;125:953-964.
54. Aubier M, Aldons PM, Leak A, et al. Telithromycin is as effective as amoxicillin/clavulanate in acute exacerbations of chronic bronchitis. Respir Med. 2002;96:862-871.
55. Zervos MJ, Heyder AM, Leroy B. Oral telithromycin 800 mg once daily for 5 days versus cefuroxime axetil 500 mg twice daily for 10 days in adults with acute exacerbations of chronic bronchitis. J Int Med Res. 2003;31:157-169.
56. Ketek [prescribing information]. Kansas City, Mo: Aventis Pharmaceuticals Inc.; 2004.
57. Carbon C, Chatelin A, Bingen E, et al. A double-blind randomized trial comparing the efficacy and safety of a 5-day course of cefotiam hexetil with that of a 10-day course of penicillin V in adult patients with pharyngitis caused by group A β-haemolytic streptococci. J Antimicrob Chemother 1995;35:843-854.
58. Cockburn J, Gibberd RW, Reid AL, Sanson-Fisher RW. Determinants of noncompliance with short term antibiotic regimens. Br Med J (Clin Res Ed). 1987;295:814-818.
59. Greenberg RN. Overview of patient compliance with medication dosing: a literature review. Clin Ther. 1984;6:592-599.
60. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23:1296-1310.
61. Perez-Gorricho B, Ripoll M. Does short-course antibiotic therapy better meet patient expectations? Int J Antimicrob Agents. 2003;21:222-228.
1. Centers for Disease Control and Prevention. National Center for Health Statistics website. National Ambulatory Medical Care Survey: 2001 Summary. Available at: http://www.cdc.gov/nchs/data/ad/ad337.pdf. Accessed February 2, 2005.
2. World Health Organization.World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 4. Big guns of resistance. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
3. Metlay JP, Fine MJ. Testing strategies in the initial management of patients with community-acquired pneumonia. Ann Intern Med. 2003;138:109-118.
4. File TM. Community-acquired pneumonia. Lancet. 2003;362:1991-2001.
5. Mandell LA, Bartlett JG, Dowell SF, File TM, Jr, Musher DM, Whitney C. Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clin Infect Dis. 2003;37:1405-1433.
6. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336:243-250.
7. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106:196-204.
8. Balter MS, La Forge J, Low DE, Mandell L, Grossman RF. Canadian guidelines for the management of acute exacerbations of chronic bronchitis. Can Respir J. 2003;10(suppl B):3B-32B.
9. World Health Organization. World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 5. A call to action: A massive effort to provide proper treatment. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
10. Shlaes DM, Gerding DN, John JF, Jr, et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the Prevention of Antimicrobial Resistance: guidelines for the prevention of antimicrobial resistance in hospitals. Clin Infect Dis. 1997;25:584-599.
11. Scottish Intercollegiate Guidelines Network. National Guideline Clearinghouse website. Community management of lower respiratory tract infection in adults. A national clinical guideline. Available at: http://www.guideline.gov/summary/summary.aspx?ss=15& doc_id=3361&nbr=2587&string=respiratory%20AND%20tract%20AND% 20infection. Accessed December 17, 2004.
12. Bochud PY, Moser F, Erard P, et al. Community-acquired pneumonia. A prospective outpatient study. Medicine (Baltimore). 2001;80:75-87.
13. Falguera M, Sacristan O, Nogues A, et al. Nonsevere community-acquired pneumonia: correlation between cause and severity or comorbidity. Arch Intern Med. 2001;161:1866-1872.
14. Ruiz M, Ewig S, Marcos MA, et al. Etiology of community-acquired pneumonia: impact of age, comorbidity, and severity. Am J Respir Crit Care Med. 1999;160:397-405.
15. Sethi S. Infectious etiology of acute exacerbations of chronic bronchitis. Chest. 2000;117(5 Suppl 2):380S-385S.
16. Eller J, Ede A, Schaberg T, Niederman MS, Mauch H, Lode H. Infective exacerbations of chronic bronchitis: relation between bacteriologic etiology and lung function. Chest. 1998;113:1542-1548.
17. Anon JB, Jacobs MR, Poole MD, et al. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg. 2004;130(1 Suppl):1-45.
18. Albrich WC, Monnet DL, Harbarth S. Antibiotic selection pressure and resistance in Streptococcus pneumoniae. and Streptococcus pyogenes. Emerg Infect Dis. 2004;10:514-517.
19. Ball P, Baquero F, Cars O, et al. Antibiotic therapy of community respiratory tract infections: strategies for optimal outcomes and minimized resistance emergence. J Antimicrob Chemother. 2002;49:31-40.
20. Harbarth S, Albrich W, Brun-Buisson C. Outpatient antibiotic use and prevalence of antibiotic-resistant pneumococci in France and Germany: a sociocultural perspective. Emerg Infect Dis. 2002;8:1460-1467.
21. Lonks JR, Garau J, Medeiros AA. Implications of antimicrobial resistance in the empirical treatment of community-acquired respiratory tract infections: the case of macrolides. J Antimicrob Chemother. 2002;50(Suppl S2):87-92.
22. Lonks JR, Garau J, Gomez L, et al. Failure of macrolide antibiotic treatment in patients with bacteremia due to erythromycin-resistant Streptococcus pneumoniae. Clin Infect Dis. 2002;35:556-564.
23. Moellering RC, Jr, Craig W, Edmond M, et al. Clinical and public health implications of macrolide-resistant Streptococcus pneumoniae. J Chemother. 2002;14(suppl 3):42-56.
24. Davidson R, Cavalcanti R, Brunton JL, et al. Resistance to levofloxacin and failure of treatment of pneumococcal pneumonia. N Engl J Med. 2002;346:747-750.
25. Musher DM, Dowell ME, Shortridge VD, et al. Emergence of macrolide resistance during treatment of pneumococcal pneumonia. N Engl J Med. 2002;346:630-631.
26. Waterer GW, Buckingham SC, Kessler LA, Quasney MW, Wunderink RG. Decreasing β-lactam resistance in Pneumococci. from the Memphis region: analysis of 2,152 isolates From 1996 to 2001. Chest. 2003;124:519-525.
27. Nuermberger E, Bishai WR. The clinical significance of macrolide-resistant Streptococcus pneumoniae.: it’s all relative. Clin Infect Dis. 2004;38:99-103.
28. Yu VL, Chiou CC, Feldman C, et al. An international prospective study of pneumococcal bacteremia: correlation with in vitro resistance, antibiotics administered, and clinical outcome. Clin Infect Dis. 2003;37:230-237.
29. Metlay JP. Update on community-acquired pneumonia: impact of antibiotic resistance on clinical outcomes. Curr Opin Infect Dis. 2002;15:163-167.
30. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention web site. Drug-resistant Streptococcus pneumoniae disease. Available at: http://www.cdc.gov/ncidod/dbmd/diseaseinfo/drugresisstreppneum_t.htm. Accessed January 4, 2005.
31. World Health Organization World Health Organization web site. World Health Organization Report on Infectious Diseases 2000. Overcoming antimicrobial resistance. Chapter 3. Factors contributing to resistance. Available at: http://www.who.int/infectious-disease-report/2000/. Accessed February 2, 2005.
32. Jacobs MR, Felmingham D, Appelbaum PC, Gruneberg RN. The Alexander Project 1998-2000: susceptibility of pathogens isolated from communityacquired respiratory tract infection to commonly used antimicrobial agents. J Antimicrob Chemother. 2003;52:229-246.
33. Thornsberry C, Sahm DF, Kelly LJ, et al. Regional trends in antimicrobial resistance among clinical isolates of Streptococcus pneumoniae., Haemophilus influenzae., and Moraxella catarrhalis. in the United States: results from the TRUST Surveillance Program, 1999-2000. Clin Infect Dis. 2002;34(suppl 1):S4-S16.
34. Karlowsky JA, Thornsberry C, Jones ME, Evangelista AT, Critchley IA, Sahm DF. Factors associated with relative rates of antimicrobial resistance among Streptococcus pneumoniae. in the United States: results from the TRUST Surveillance Program (1998-2002). Clin Infect Dis. 2003;36:963-970.
35. Karlowsky JA, Kelly LJ, Thornsberry C, et al. Susceptibility to fluoroquinolones among commonly isolated Gram-negative bacilli in 2000: TRUST and TSN data for the United States. Tracking Resistance in the United States Today. The Surveillance Network. Int J Antimicrob Agents. 2002;19:21-31.
36. Karlowsky JA, Thornsberry C, Critchley IA, et al. Susceptibilities to levofloxacin in Streptococcus pneumoniae., Haemophilus influenzae., and Moraxella catarrhalis. clinical isolates from children: results from 2000-2001 and 2001-2002 TRUST studies in the United States. Antimicrob Agents Chemother. 2003;47:1790-1797.
37. Quale J, Landman D, Ravishankar J, Flores C, Bratu S. Streptococcus pneumo.-niae., Brooklyn, New York: fluoroquinolone resistance at our doorstep. Emerg Infect Dis. 2002;8:594-597.
38. Williams JW, Jr, Aguilar C, Cornell J, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2004;2:CD000243.-
39. Guillemot D, Carbon C, Balkau B, et al. Low dosage and long treatment duration of β-lactam: risk factors for carriage of penicillin-resistant Streptococcus pneumoniae. JAMA. 1998;279:365-370.
40. Scheld WM. Maintaining fluoroquinolone class efficacy: review of influencing factors. Emerg Infect Dis. 2003;9:1-9.
41. Thomson KS. Minimizing quinolone resistance: are the new agents more or less likely to cause resistance? J Antimicrob Chemother. 2000;45:719-723.
42. World Health Organization. World Health Organization web site. WHO global strategy for containment of antimicrobial resistance. Available at: http://www.who.int/csr/resources/publications/drugresist/en/EGlobal_Strat.pdf. Accessed February 2, 2005.
43. Hepburn MJ, Dooley DP, Skidmore PJ, Ellis MW, Starnes WF, Hasewinkle WC. Comparison of short-course (5 days) and standard (10 days) treatment for uncomplicated cellulitis. Arch Intern Med. 2004;164:1669-1674.
44. Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588-2598.
45. Ellis-Pegler R, Galler L, Roberts S, Thomas M, Woodhouse A. Three days of intravenous benzyl penicillin treatment of meningococcal disease in adults. Clin Infect Dis. 2003;37:658-662.
46. Craig WA. Basic pharmacodynamics of antibacterials with clinical applications to the use of β-lactams, glycopeptides, and linezolid. Infect Dis Clin North Am. 2003;17:479-501.
47. Schrag SJ, Pena C, Fernandez J, et al. Effect of short-course, high-dose amoxicillin therapy on resistant pneumococcal carriage: a randomized trial. JAMA. 2001;286:49-56.
48. Dunbar LM, Wunderink RG, Habib MP, et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
49. Tellier G, Niederman MS, Nusrat R, Patel M, Lavin B. Clinical and bacteriological efficacy and safety of 5 and 7 day regimens of telithromycin once daily compared with a 10 day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515-523.
50. Zithromax [prescribing information] New York, NY: Pfizer Labs; 2004.
51. Wilson R, Langan C, Ball P, Bateman K, Pypstra R. Oral gemifloxacin once daily for 5 days compared with sequential therapy with i.v. ceftriaxone/oral cefuroxime (maximum of 10 days) in the treatment of hospitalized patients with acute exacerbations of chronic bronchitis. Respir Med. 2003;97:242-249.
52. Tennenberg A, Walker K, Khashab M, Zadelkis N. The safety and efficacy of short-course (3-5 days), 750 mg levofloxacin (LVX) for acute bacterial exacerbation of chronic bronchitis (ABECB). Presented at: American Thoracic Society 100th International Conference, May 21-26, 2004, Orlando, Fl.
53. Wilson R, Allegra L, Huchon G, et al. Short-term and long-term outcomes of moxifloxacin compared to standard antibiotic treatment in acute exacerbations of chronic bronchitis. Chest. 2004;125:953-964.
54. Aubier M, Aldons PM, Leak A, et al. Telithromycin is as effective as amoxicillin/clavulanate in acute exacerbations of chronic bronchitis. Respir Med. 2002;96:862-871.
55. Zervos MJ, Heyder AM, Leroy B. Oral telithromycin 800 mg once daily for 5 days versus cefuroxime axetil 500 mg twice daily for 10 days in adults with acute exacerbations of chronic bronchitis. J Int Med Res. 2003;31:157-169.
56. Ketek [prescribing information]. Kansas City, Mo: Aventis Pharmaceuticals Inc.; 2004.
57. Carbon C, Chatelin A, Bingen E, et al. A double-blind randomized trial comparing the efficacy and safety of a 5-day course of cefotiam hexetil with that of a 10-day course of penicillin V in adult patients with pharyngitis caused by group A β-haemolytic streptococci. J Antimicrob Chemother 1995;35:843-854.
58. Cockburn J, Gibberd RW, Reid AL, Sanson-Fisher RW. Determinants of noncompliance with short term antibiotic regimens. Br Med J (Clin Res Ed). 1987;295:814-818.
59. Greenberg RN. Overview of patient compliance with medication dosing: a literature review. Clin Ther. 1984;6:592-599.
60. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23:1296-1310.
61. Perez-Gorricho B, Ripoll M. Does short-course antibiotic therapy better meet patient expectations? Int J Antimicrob Agents. 2003;21:222-228.