Opinion

Gynecologic Oncology Consult: Update on Endometrial Cancer Treatment
Checkpoint inhibitors improve outcomes in women with advanced endometrial cancer and an immunotherapy and antivascular endothelial growth factor...
Opinion
Molecular Classification of Endometrial Carcinomas
When The Cancer Genome Atlas performed genomic, transcriptomic, and proteomic characterization of endometrial carcinomas, they identified four...
Opinion

Surgical management of borderline ovarian tumors, part 1
Ovarian-sparing procedures should be offered to patients in the setting of borderline ovarian tumors, with the understanding that they are...
Opinion

Update on secondary cytoreduction in recurrent ovarian cancer
Secondary debulking surgery has been studied since the 1980s with mixed results; these data have shown that the largest barrier to care has been...
Opinion

Update on high-grade vulvar interepithelial neoplasia
Treatment of high-grade vulvar intraepithelial neoplasia should be driven by the clinical characteristics of the vulvar lesions, patients’...
Opinion
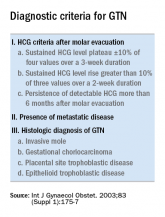
The role of repeat uterine curettage in postmolar gestational trophoblastic neoplasia
Second uterine evacuation for treatment of nonmetastatic, low-risk postmolar GTN is a reasonable treatment option and one that should be...
Opinion
Estrogen replacement therapy in endometrial cancer survivors
Given the data we have, ERT does not appear to significantly affect oncologic outcomes in low-risk, early-stage endometrial cancer survivors.
Opinion
The perils of CA-125 as a diagnostic tool in patients with adnexal masses
It is important to have conversations with patients before ordering a CA-125 (or other serum biomarkers) about potential results and their effect...