User login
Primary Care Physicians Underutilize Nonantibiotic Prophylaxis for Recurrent UTIs
While primary care physicians are generally comfortable prescribing vaginal estrogen therapy for recurrent urinary tract infections (UTIs), other nonantibiotic prophylactic options remain significantly underutilized, according to new research that highlights a crucial gap in antibiotic stewardship practices among primary care physicians.
UTIs are the most common bacterial infection in women of all ages, and an estimated 30%-40% of women will experience reinfection within 6 months. Recurrent UTI is typically defined as two or more infections within 6 months or a greater number of infections within a year, according to the American Academy of Family Physicians.
Antibiotics are the first line of defense in preventing and treating recurrent UTIs, but repeated and prolonged use could lead to antibiotic resistance.
Researchers at the University of North Carolina surveyed 40 primary care physicians at one academic medical center and found that 96% of primary care physicians prescribe vaginal estrogen therapy for recurrent UTI prevention, with 58% doing so “often.” Estrogen deficiency and urinary retention are strong contributors to infection.
However, 78% of physicians surveyed said they had never prescribed methenamine hippurate, and 85% said they had never prescribed D-mannose.
Physicians with specialized training in menopausal care felt more at ease prescribing vaginal estrogen therapy to patients with complex medical histories, such as those with a family history of breast cancer or endometrial cancer. This suggests that enhanced education could play a vital role in increasing comfort levels among general practitioners, said Lauren Tholemeier, MD, a urogynecology fellow at the University of North Carolina at Chapel Hill.
“Primary care physicians are the front line of managing patients with recurrent UTI,” said Tholemeier.
“There’s an opportunity for further education on, and even awareness of, methenamine hippurate and D-mannose as an option that has data behind it and can be included as a tool” for patient care, she said.
Indeed, physicians who saw six or more recurrent patients with UTI each month were more likely to prescribe methenamine hippurate, the study found, suggesting that familiarity with recurrent UTI cases can lead to greater confidence in employing alternative prophylactic strategies.
Tholemeier presented her research at the American Urogynecologic Society’s PFD Week in Washington, DC.
Expanding physician knowledge and utilization of all available nonantibiotic therapies can help them better care for patients who don’t necessarily have access to a subspecialist, Tholemeier said.
According to the American Urogynecologic Society’s best practice guidelines, there is limited evidence supporting routine use of D-mannose to prevent recurrent UTI. Methenamine hippurate, however, may be effective for short-term UTI prevention, according to the group.
By broadening the use of vaginal estrogen therapy, methenamine hippurate, and D-mannose, primary care physicians can help reduce reliance on antibiotics for recurrent UTI prevention — a practice that may contribute to growing antibiotic resistance, said Tholemeier.
“The end goal isn’t going to be to say that we should never prescribe antibiotics for UTI infection,” said Tholemeier, adding that, in some cases, physicians can consider using these other medications in conjunction with antibiotics.
“But it’s knowing they [clinicians] have some other options in their toolbox,” she said.
A version of this article first appeared on Medscape.com.
While primary care physicians are generally comfortable prescribing vaginal estrogen therapy for recurrent urinary tract infections (UTIs), other nonantibiotic prophylactic options remain significantly underutilized, according to new research that highlights a crucial gap in antibiotic stewardship practices among primary care physicians.
UTIs are the most common bacterial infection in women of all ages, and an estimated 30%-40% of women will experience reinfection within 6 months. Recurrent UTI is typically defined as two or more infections within 6 months or a greater number of infections within a year, according to the American Academy of Family Physicians.
Antibiotics are the first line of defense in preventing and treating recurrent UTIs, but repeated and prolonged use could lead to antibiotic resistance.
Researchers at the University of North Carolina surveyed 40 primary care physicians at one academic medical center and found that 96% of primary care physicians prescribe vaginal estrogen therapy for recurrent UTI prevention, with 58% doing so “often.” Estrogen deficiency and urinary retention are strong contributors to infection.
However, 78% of physicians surveyed said they had never prescribed methenamine hippurate, and 85% said they had never prescribed D-mannose.
Physicians with specialized training in menopausal care felt more at ease prescribing vaginal estrogen therapy to patients with complex medical histories, such as those with a family history of breast cancer or endometrial cancer. This suggests that enhanced education could play a vital role in increasing comfort levels among general practitioners, said Lauren Tholemeier, MD, a urogynecology fellow at the University of North Carolina at Chapel Hill.
“Primary care physicians are the front line of managing patients with recurrent UTI,” said Tholemeier.
“There’s an opportunity for further education on, and even awareness of, methenamine hippurate and D-mannose as an option that has data behind it and can be included as a tool” for patient care, she said.
Indeed, physicians who saw six or more recurrent patients with UTI each month were more likely to prescribe methenamine hippurate, the study found, suggesting that familiarity with recurrent UTI cases can lead to greater confidence in employing alternative prophylactic strategies.
Tholemeier presented her research at the American Urogynecologic Society’s PFD Week in Washington, DC.
Expanding physician knowledge and utilization of all available nonantibiotic therapies can help them better care for patients who don’t necessarily have access to a subspecialist, Tholemeier said.
According to the American Urogynecologic Society’s best practice guidelines, there is limited evidence supporting routine use of D-mannose to prevent recurrent UTI. Methenamine hippurate, however, may be effective for short-term UTI prevention, according to the group.
By broadening the use of vaginal estrogen therapy, methenamine hippurate, and D-mannose, primary care physicians can help reduce reliance on antibiotics for recurrent UTI prevention — a practice that may contribute to growing antibiotic resistance, said Tholemeier.
“The end goal isn’t going to be to say that we should never prescribe antibiotics for UTI infection,” said Tholemeier, adding that, in some cases, physicians can consider using these other medications in conjunction with antibiotics.
“But it’s knowing they [clinicians] have some other options in their toolbox,” she said.
A version of this article first appeared on Medscape.com.
While primary care physicians are generally comfortable prescribing vaginal estrogen therapy for recurrent urinary tract infections (UTIs), other nonantibiotic prophylactic options remain significantly underutilized, according to new research that highlights a crucial gap in antibiotic stewardship practices among primary care physicians.
UTIs are the most common bacterial infection in women of all ages, and an estimated 30%-40% of women will experience reinfection within 6 months. Recurrent UTI is typically defined as two or more infections within 6 months or a greater number of infections within a year, according to the American Academy of Family Physicians.
Antibiotics are the first line of defense in preventing and treating recurrent UTIs, but repeated and prolonged use could lead to antibiotic resistance.
Researchers at the University of North Carolina surveyed 40 primary care physicians at one academic medical center and found that 96% of primary care physicians prescribe vaginal estrogen therapy for recurrent UTI prevention, with 58% doing so “often.” Estrogen deficiency and urinary retention are strong contributors to infection.
However, 78% of physicians surveyed said they had never prescribed methenamine hippurate, and 85% said they had never prescribed D-mannose.
Physicians with specialized training in menopausal care felt more at ease prescribing vaginal estrogen therapy to patients with complex medical histories, such as those with a family history of breast cancer or endometrial cancer. This suggests that enhanced education could play a vital role in increasing comfort levels among general practitioners, said Lauren Tholemeier, MD, a urogynecology fellow at the University of North Carolina at Chapel Hill.
“Primary care physicians are the front line of managing patients with recurrent UTI,” said Tholemeier.
“There’s an opportunity for further education on, and even awareness of, methenamine hippurate and D-mannose as an option that has data behind it and can be included as a tool” for patient care, she said.
Indeed, physicians who saw six or more recurrent patients with UTI each month were more likely to prescribe methenamine hippurate, the study found, suggesting that familiarity with recurrent UTI cases can lead to greater confidence in employing alternative prophylactic strategies.
Tholemeier presented her research at the American Urogynecologic Society’s PFD Week in Washington, DC.
Expanding physician knowledge and utilization of all available nonantibiotic therapies can help them better care for patients who don’t necessarily have access to a subspecialist, Tholemeier said.
According to the American Urogynecologic Society’s best practice guidelines, there is limited evidence supporting routine use of D-mannose to prevent recurrent UTI. Methenamine hippurate, however, may be effective for short-term UTI prevention, according to the group.
By broadening the use of vaginal estrogen therapy, methenamine hippurate, and D-mannose, primary care physicians can help reduce reliance on antibiotics for recurrent UTI prevention — a practice that may contribute to growing antibiotic resistance, said Tholemeier.
“The end goal isn’t going to be to say that we should never prescribe antibiotics for UTI infection,” said Tholemeier, adding that, in some cases, physicians can consider using these other medications in conjunction with antibiotics.
“But it’s knowing they [clinicians] have some other options in their toolbox,” she said.
A version of this article first appeared on Medscape.com.
FROM PFD WEEK 2024
Over-the-Counter UTI Products: What Primary Care Clinicians Need to Know
When it comes to managing urinary tract infections (UTIs), patients often turn to over-the-counter (OTC) products in search of quick relief. However, recent research suggests some products promise more than they can deliver and can vary widely in price and ingredients. For primary care clinicians, understanding these differences could make all the difference in offering effective, cost-conscious advice to patients.
Researchers from the University of Wisconsin analyzed OTC products marketed for urinary tract health in three major US drugstores and found significant price variations and a wide array of active ingredients.
Their study, presented at the American Urogynecologic Society’s PFD Week conference, found that the price of OTC products fluctuates dramatically. Phenazopyridine hydrochloride, commonly used for UTI symptom relief, ranged from $0.17 to $0.83 per tablet, the study found. Methenamine/sodium salicylate combinations, which are marketed for UTI prevention, varied from $0.13 to $0.33 per tablet. Cranberry supplements — often touted for their preventive benefits — showed the most extreme price range, from as low as $0.07 to as high as $1.00 per serving.
The study also looked into the ingredients, which were categorized into five main groups: Phenazopyridine hydrochloride, methenamine/sodium salicylate, cranberry supplements, D-mannose, and cranberry/D-mannose combinations.
These ingredients vary not only in price but also in the strength of scientific evidence supporting their use.
The researchers concluded:
- Phenazopyridine hydrochloride offers effective symptom relief but is not a UTI treatment.
- Methenamine/sodium salicylate shows potential for preventing recurrent UTIs in certain patients.
- Cranberry supplements have limited evidence for preventing UTIs, with no proof they treat infections.
- D-mannose has shown promise for short-term use in preventing recurrent UTIs, though more research is needed to weigh its effectiveness in the long run.
“No OTC product within its respective category is superior to another,” said Ushma J. Patel, MD, a fellow in Urogynecology and Reconstructive Pelvic Surgery at the University of Wisconsin School of Medicine and Public Health, Madison, and lead author of the study.
Patel and her coresearcher also found that many products are falsely marketed as treatments for UTI.
“The products in each type of category are for symptom relief or UTI prevention — not treatment,” said Patel. “These products within the categories described are interchangeable, and consumers should make cost-effective choices as no product is superior to another within its respective category.”
This presents the opportunity for clinicians to guide individuals to pick the right products while explaining that symptom relief doesn’t necessarily mean an infection is being treated, Patel said.
Indeed, Patel proposed that clinicians utilize a summary table created from their findings to offer patients vetted information about OTC UTI products.
And, while OTC products can provide benefits, they should not replace proper medical evaluation and treatment of UTIs.
“If patients are experiencing ongoing symptoms or develop new-onset symptoms despite trialing an over-the-counter product, they should contact a healthcare provider,” said Patel. “OTC products can provide symptom relief until patients are able to see a healthcare provider.”
The researchers reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
When it comes to managing urinary tract infections (UTIs), patients often turn to over-the-counter (OTC) products in search of quick relief. However, recent research suggests some products promise more than they can deliver and can vary widely in price and ingredients. For primary care clinicians, understanding these differences could make all the difference in offering effective, cost-conscious advice to patients.
Researchers from the University of Wisconsin analyzed OTC products marketed for urinary tract health in three major US drugstores and found significant price variations and a wide array of active ingredients.
Their study, presented at the American Urogynecologic Society’s PFD Week conference, found that the price of OTC products fluctuates dramatically. Phenazopyridine hydrochloride, commonly used for UTI symptom relief, ranged from $0.17 to $0.83 per tablet, the study found. Methenamine/sodium salicylate combinations, which are marketed for UTI prevention, varied from $0.13 to $0.33 per tablet. Cranberry supplements — often touted for their preventive benefits — showed the most extreme price range, from as low as $0.07 to as high as $1.00 per serving.
The study also looked into the ingredients, which were categorized into five main groups: Phenazopyridine hydrochloride, methenamine/sodium salicylate, cranberry supplements, D-mannose, and cranberry/D-mannose combinations.
These ingredients vary not only in price but also in the strength of scientific evidence supporting their use.
The researchers concluded:
- Phenazopyridine hydrochloride offers effective symptom relief but is not a UTI treatment.
- Methenamine/sodium salicylate shows potential for preventing recurrent UTIs in certain patients.
- Cranberry supplements have limited evidence for preventing UTIs, with no proof they treat infections.
- D-mannose has shown promise for short-term use in preventing recurrent UTIs, though more research is needed to weigh its effectiveness in the long run.
“No OTC product within its respective category is superior to another,” said Ushma J. Patel, MD, a fellow in Urogynecology and Reconstructive Pelvic Surgery at the University of Wisconsin School of Medicine and Public Health, Madison, and lead author of the study.
Patel and her coresearcher also found that many products are falsely marketed as treatments for UTI.
“The products in each type of category are for symptom relief or UTI prevention — not treatment,” said Patel. “These products within the categories described are interchangeable, and consumers should make cost-effective choices as no product is superior to another within its respective category.”
This presents the opportunity for clinicians to guide individuals to pick the right products while explaining that symptom relief doesn’t necessarily mean an infection is being treated, Patel said.
Indeed, Patel proposed that clinicians utilize a summary table created from their findings to offer patients vetted information about OTC UTI products.
And, while OTC products can provide benefits, they should not replace proper medical evaluation and treatment of UTIs.
“If patients are experiencing ongoing symptoms or develop new-onset symptoms despite trialing an over-the-counter product, they should contact a healthcare provider,” said Patel. “OTC products can provide symptom relief until patients are able to see a healthcare provider.”
The researchers reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
When it comes to managing urinary tract infections (UTIs), patients often turn to over-the-counter (OTC) products in search of quick relief. However, recent research suggests some products promise more than they can deliver and can vary widely in price and ingredients. For primary care clinicians, understanding these differences could make all the difference in offering effective, cost-conscious advice to patients.
Researchers from the University of Wisconsin analyzed OTC products marketed for urinary tract health in three major US drugstores and found significant price variations and a wide array of active ingredients.
Their study, presented at the American Urogynecologic Society’s PFD Week conference, found that the price of OTC products fluctuates dramatically. Phenazopyridine hydrochloride, commonly used for UTI symptom relief, ranged from $0.17 to $0.83 per tablet, the study found. Methenamine/sodium salicylate combinations, which are marketed for UTI prevention, varied from $0.13 to $0.33 per tablet. Cranberry supplements — often touted for their preventive benefits — showed the most extreme price range, from as low as $0.07 to as high as $1.00 per serving.
The study also looked into the ingredients, which were categorized into five main groups: Phenazopyridine hydrochloride, methenamine/sodium salicylate, cranberry supplements, D-mannose, and cranberry/D-mannose combinations.
These ingredients vary not only in price but also in the strength of scientific evidence supporting their use.
The researchers concluded:
- Phenazopyridine hydrochloride offers effective symptom relief but is not a UTI treatment.
- Methenamine/sodium salicylate shows potential for preventing recurrent UTIs in certain patients.
- Cranberry supplements have limited evidence for preventing UTIs, with no proof they treat infections.
- D-mannose has shown promise for short-term use in preventing recurrent UTIs, though more research is needed to weigh its effectiveness in the long run.
“No OTC product within its respective category is superior to another,” said Ushma J. Patel, MD, a fellow in Urogynecology and Reconstructive Pelvic Surgery at the University of Wisconsin School of Medicine and Public Health, Madison, and lead author of the study.
Patel and her coresearcher also found that many products are falsely marketed as treatments for UTI.
“The products in each type of category are for symptom relief or UTI prevention — not treatment,” said Patel. “These products within the categories described are interchangeable, and consumers should make cost-effective choices as no product is superior to another within its respective category.”
This presents the opportunity for clinicians to guide individuals to pick the right products while explaining that symptom relief doesn’t necessarily mean an infection is being treated, Patel said.
Indeed, Patel proposed that clinicians utilize a summary table created from their findings to offer patients vetted information about OTC UTI products.
And, while OTC products can provide benefits, they should not replace proper medical evaluation and treatment of UTIs.
“If patients are experiencing ongoing symptoms or develop new-onset symptoms despite trialing an over-the-counter product, they should contact a healthcare provider,” said Patel. “OTC products can provide symptom relief until patients are able to see a healthcare provider.”
The researchers reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM PFD WEEK 2024
Innovative Biomaterial May Treat Common Vaginal Changes and Discomfort in Menopausal Women
A novel biomaterial developed by researchers at the University of California, San Diego, may help treat commonly overlooked menopausal vaginal changes and discomfort experienced by many women.
As many as 84% of menopausal women experience genitourinary syndrome of menopause, a condition that can cause vaginal dryness, irritation, and pain during intercourse and significantly affect quality of life. Current treatments, mainly estrogen creams, help with surface issues but don’t address deeper tissue problems.
Marianna Alperin, MD, and researchers at her lab created a gel-like material derived from pig vaginal tissue designed to mimic the natural environment of the vagina and stimulate the body’s own healing processes.
“We used porcine vaginal tissue that was minced, decellularized by detergent, lyophilized, milled into powder, and enzymatically digested,” said Alperin, professor and vice chair for translational research in the Department of Obstetrics, Gynecology, and Reproductive Sciences and professor of urology at the University of California, San Diego.
Using the vaginal extracellular matrix biomaterial on rats — which have vaginal tissue similar to that of humans — improved vaginal epithelial thickness and health of the vaginal lining.
Three days after administering the biomaterial, the treatment group exhibited a mean epithelial thickness of 32.37 ± 6.29 µm, compared with 19.00 ± 1.59 µm in the saline control group (P < .0001). Rats treated with vaginal extracellular matrix biomaterial also showed a mean smooth muscle layer thickness of 54.02 ± 10.56 µm, significantly thicker than the saline group’s 35.07 ± 7.80 µm (P < .05), the study found.
“While [the biomaterial] did not restore the epithelial thickness all the way to the level of the healthy, unperturbed animals, it certainly was superior to the other groups, especially at the higher dose,” she said.
It also enhanced the underlying muscle layer, something current treatments don’t typically achieve, the researchers noted.
Alperin’s research was awarded best overall paper at the American Urogynecologic Society’s PFD Week conference in Washington, DC.
The material seems to work by interacting with immune cells to carry the healing material deeper into the vaginal tissues, potentially explaining its widespread effects.
“It looked like the cells are trafficking the biomaterial into the deeper tissues, which is very exciting,” said Alperin, adding that unlike existing treatments, this new approach may improve both the surface layer and deeper tissues of the vagina.
Also, the benefits appeared to increase with higher doses of the material, they found.
While the study shows promise, Alperin acknowledged that further research is needed, particularly in comparing their treatment with topical estrogen.
“We are repeating the experiment with the dose adjusted to the volume of the rat vagina,” Alperin said.
A version of this article appeared on Medscape.com.
A novel biomaterial developed by researchers at the University of California, San Diego, may help treat commonly overlooked menopausal vaginal changes and discomfort experienced by many women.
As many as 84% of menopausal women experience genitourinary syndrome of menopause, a condition that can cause vaginal dryness, irritation, and pain during intercourse and significantly affect quality of life. Current treatments, mainly estrogen creams, help with surface issues but don’t address deeper tissue problems.
Marianna Alperin, MD, and researchers at her lab created a gel-like material derived from pig vaginal tissue designed to mimic the natural environment of the vagina and stimulate the body’s own healing processes.
“We used porcine vaginal tissue that was minced, decellularized by detergent, lyophilized, milled into powder, and enzymatically digested,” said Alperin, professor and vice chair for translational research in the Department of Obstetrics, Gynecology, and Reproductive Sciences and professor of urology at the University of California, San Diego.
Using the vaginal extracellular matrix biomaterial on rats — which have vaginal tissue similar to that of humans — improved vaginal epithelial thickness and health of the vaginal lining.
Three days after administering the biomaterial, the treatment group exhibited a mean epithelial thickness of 32.37 ± 6.29 µm, compared with 19.00 ± 1.59 µm in the saline control group (P < .0001). Rats treated with vaginal extracellular matrix biomaterial also showed a mean smooth muscle layer thickness of 54.02 ± 10.56 µm, significantly thicker than the saline group’s 35.07 ± 7.80 µm (P < .05), the study found.
“While [the biomaterial] did not restore the epithelial thickness all the way to the level of the healthy, unperturbed animals, it certainly was superior to the other groups, especially at the higher dose,” she said.
It also enhanced the underlying muscle layer, something current treatments don’t typically achieve, the researchers noted.
Alperin’s research was awarded best overall paper at the American Urogynecologic Society’s PFD Week conference in Washington, DC.
The material seems to work by interacting with immune cells to carry the healing material deeper into the vaginal tissues, potentially explaining its widespread effects.
“It looked like the cells are trafficking the biomaterial into the deeper tissues, which is very exciting,” said Alperin, adding that unlike existing treatments, this new approach may improve both the surface layer and deeper tissues of the vagina.
Also, the benefits appeared to increase with higher doses of the material, they found.
While the study shows promise, Alperin acknowledged that further research is needed, particularly in comparing their treatment with topical estrogen.
“We are repeating the experiment with the dose adjusted to the volume of the rat vagina,” Alperin said.
A version of this article appeared on Medscape.com.
A novel biomaterial developed by researchers at the University of California, San Diego, may help treat commonly overlooked menopausal vaginal changes and discomfort experienced by many women.
As many as 84% of menopausal women experience genitourinary syndrome of menopause, a condition that can cause vaginal dryness, irritation, and pain during intercourse and significantly affect quality of life. Current treatments, mainly estrogen creams, help with surface issues but don’t address deeper tissue problems.
Marianna Alperin, MD, and researchers at her lab created a gel-like material derived from pig vaginal tissue designed to mimic the natural environment of the vagina and stimulate the body’s own healing processes.
“We used porcine vaginal tissue that was minced, decellularized by detergent, lyophilized, milled into powder, and enzymatically digested,” said Alperin, professor and vice chair for translational research in the Department of Obstetrics, Gynecology, and Reproductive Sciences and professor of urology at the University of California, San Diego.
Using the vaginal extracellular matrix biomaterial on rats — which have vaginal tissue similar to that of humans — improved vaginal epithelial thickness and health of the vaginal lining.
Three days after administering the biomaterial, the treatment group exhibited a mean epithelial thickness of 32.37 ± 6.29 µm, compared with 19.00 ± 1.59 µm in the saline control group (P < .0001). Rats treated with vaginal extracellular matrix biomaterial also showed a mean smooth muscle layer thickness of 54.02 ± 10.56 µm, significantly thicker than the saline group’s 35.07 ± 7.80 µm (P < .05), the study found.
“While [the biomaterial] did not restore the epithelial thickness all the way to the level of the healthy, unperturbed animals, it certainly was superior to the other groups, especially at the higher dose,” she said.
It also enhanced the underlying muscle layer, something current treatments don’t typically achieve, the researchers noted.
Alperin’s research was awarded best overall paper at the American Urogynecologic Society’s PFD Week conference in Washington, DC.
The material seems to work by interacting with immune cells to carry the healing material deeper into the vaginal tissues, potentially explaining its widespread effects.
“It looked like the cells are trafficking the biomaterial into the deeper tissues, which is very exciting,” said Alperin, adding that unlike existing treatments, this new approach may improve both the surface layer and deeper tissues of the vagina.
Also, the benefits appeared to increase with higher doses of the material, they found.
While the study shows promise, Alperin acknowledged that further research is needed, particularly in comparing their treatment with topical estrogen.
“We are repeating the experiment with the dose adjusted to the volume of the rat vagina,” Alperin said.
A version of this article appeared on Medscape.com.
Considering Eating Disorder Potential When Prescribing Weight Loss Drugs to Teens
Now, with the rising popularity of medications like Ozempic for weight loss, she fears she will care for more teens with eating disorders who are seeking glucagon-like peptide 1 (GLP-1) agonists or who have developed a disorder while taking them.
“We haven’t seen patients yet, but I’m sure they are on their way,” said Dr. Dennis, a clinical assistant professor in the Department of Psychiatry at the University of Illinois College of Medicine in Chicago. She is also the cofounder and chief medical officer of SunCloud Health, an outpatient eating disorder treatment center in Illinois.
Dr. Dennis’ concerns reflect a growing unease among eating disorder specialists as obesity medications gain traction for adolescent use. A recent study published in JAMA Pediatrics showed nearly 80% of teens in treatment for obesity reported symptoms of disordered eating at the outset of an intervention. These included signs of binge eating and loss of control.
The randomized clinical trial, conducted from 2018 to 2023, examined 141 adolescents with obesity undergoing interventions like low-energy diets or intermittent energy restriction. Almost half scored as having risk for an undiagnosed eating disorder, as defined by the Eating Disorder Examination Questionnaire (EDE-Q).
At the end of the intervention, many teens continued to have symptoms of disordered eating, while a smaller group was newly scored as having a risk for an eating disorder.
Weight Loss and Eating Disorders: A Balancing Act
The findings illuminate a significant challenge for pediatricians and primary care clinicians: Balancing effective weight management with the risk of exacerbating or triggering eating disorders, said Hiba Jebeile, PhD, a research dietitian at The Children’s Hospital at Westmead in Australia, and the study’s lead author. Adding weight loss medication on top of the equation can further complicate care.
“It is helpful for obesity and eating disorder services to work together, with clear referral pathways, to manage these adolescents,” Dr. Jebeile said.
The US Food and Drug Administration approved semaglutide for weight loss in adolescents aged 12-17 years in December 2020. One study found that the number of adolescents prescribed GLP-1 receptor agonists (GLP-1 RAs) for type 2 diabetes and weight management rose from 8722 to 60,567 between 2020 and 2023 — a nearly sevenfold increase.
“The number of adolescents taking these medications is going up because they work,” said Suzanne Cuda, MD, medical director of Alamo City Healthy Kids and Families, a medical weight management clinic in San Antonio. The medications have been shown to treat type 2 diabetes, lower blood pressure, and reduce the risk for cardiovascular diseases.
“The younger you are, the better the outcome,” Dr. Cuda said.
How GLP-1 agonists may affect adolescents in the long run is not yet clear. Existing studies on GLP-1 medications in patients with eating disorders have shown mixed results. Some studies indicate that the drugs decrease binge episodes for those with binge eating disorder or bulimia nervosa. However, these studies had small sample sizes and measured only short-term effects, leaving long-term outcomes and risks unknown.
Traditional treatments for eating disorders emphasize regular eating patterns, body acceptance, addressing weight stigma, and improving attunement to hunger and fullness cues — approaches that may conflict with the effects of GLP-1 agonists. These drugs suppress appetite, alter metabolic signals, and may unintentionally reinforce weight loss as a primary goal, creating a potential disconnect between the aims of recovery from eating disorders and the biologic effects of the medication, experts said.
Dr. Cuda said she has cared for adolescents with diagnosed eating disorders in her practice who are seeking GLP-1 agonists. She said she first works with patients to treat the underlying disorder before prescribing medication.
“One of the concerns is the extreme reductions in calories that could be induced by GLP-1 RA in children and adolescents,” she said. Unlike adults, adolescents use caloric energy not just for physical activity but also for growing and developing, she said.
“They can’t catch up on that growth and development,” she added.
Advice for Screening and Monitoring
The National Eating Disorders Association raised concerns about the potential misuse of these medications and their potential to exacerbate eating disorder behaviors in people who are already at a higher risk of developing one of the conditions, including those with existing mental health disorders, stress, who have already dieted, and who have experienced weight-centric bullying.
Clinicians should be on the lookout for patients seeking GLP-1s who present with symptoms of an eating disorder that may be less apparent, such as picky eating, insomnia or difficulty sleeping, or, for girls, irregular menstrual periods, Dr. Dennis said. These patients may be more likely to go undiagnosed or misdiagnosed. Research also suggests that people of color are less likely to be diagnosed or receive specialty care for eating disorders.
Discussions between patients and clinicians about obesity treatment prior to prescribing provide a crucial opportunity to screen and monitor for disordered eating, which Dr. Dennis said does not universally occur currently.
Dr. Dennis recommended initial assessments using validated screening tools like the EDE-Q and the Center for Epidemiologic Studies Depression Scale Revised, 10-Item Version.
Ongoing monitoring throughout treatment is essential, with initial monthly check-ins that include dietary counseling to detect subtle changes in eating behaviors or attitudes toward food and body image, Dr. Cuda said.
The Obesity Medicine Association (OMA) has stressed the importance of a collaborative approach involving connections with mental health professionals specializing in eating disorders and dietitians.
“If you have a chance to send them to an obesity medicine specialist, you should do that,” said Dr. Cuda, who coauthored the OMA statement. “It’s impractical to expect a primary care physician to do everything: Screen for dietary disorders, do a full dietary counseling, follow up on their activity.”
For patients showing signs of disordered eating, clinicians should avoid recommending restrictive dietary approaches, like cutting out food groups such as carbohydrates or a restricted calorie goal. Instead, they can suggest focusing on healthier lifestyle habits and referring to a psychotherapist, the experts said. Clinicians also should be prepared to adjust or pause GLP-1 agonists if disordered eating disorder symptoms worsen.
“I think a weight-agnostic approach where the focus of care is not weight loss but increase in health protective behaviors and nutritional intake is safest for all kids, especially those with eating disorders or eating disorder risk factors,” Dr. Dennis said.
Various authors of the eating disorder study reported receiving grants, advisory board fees, and speaker fees from entities including the National Health and Medical Research Council of Australia, Eli Lilly, Novo Nordisk, Nu-Mega Ingredients, and the National Institutes of Health, among others.
A version of this article appeared on Medscape.com.
Now, with the rising popularity of medications like Ozempic for weight loss, she fears she will care for more teens with eating disorders who are seeking glucagon-like peptide 1 (GLP-1) agonists or who have developed a disorder while taking them.
“We haven’t seen patients yet, but I’m sure they are on their way,” said Dr. Dennis, a clinical assistant professor in the Department of Psychiatry at the University of Illinois College of Medicine in Chicago. She is also the cofounder and chief medical officer of SunCloud Health, an outpatient eating disorder treatment center in Illinois.
Dr. Dennis’ concerns reflect a growing unease among eating disorder specialists as obesity medications gain traction for adolescent use. A recent study published in JAMA Pediatrics showed nearly 80% of teens in treatment for obesity reported symptoms of disordered eating at the outset of an intervention. These included signs of binge eating and loss of control.
The randomized clinical trial, conducted from 2018 to 2023, examined 141 adolescents with obesity undergoing interventions like low-energy diets or intermittent energy restriction. Almost half scored as having risk for an undiagnosed eating disorder, as defined by the Eating Disorder Examination Questionnaire (EDE-Q).
At the end of the intervention, many teens continued to have symptoms of disordered eating, while a smaller group was newly scored as having a risk for an eating disorder.
Weight Loss and Eating Disorders: A Balancing Act
The findings illuminate a significant challenge for pediatricians and primary care clinicians: Balancing effective weight management with the risk of exacerbating or triggering eating disorders, said Hiba Jebeile, PhD, a research dietitian at The Children’s Hospital at Westmead in Australia, and the study’s lead author. Adding weight loss medication on top of the equation can further complicate care.
“It is helpful for obesity and eating disorder services to work together, with clear referral pathways, to manage these adolescents,” Dr. Jebeile said.
The US Food and Drug Administration approved semaglutide for weight loss in adolescents aged 12-17 years in December 2020. One study found that the number of adolescents prescribed GLP-1 receptor agonists (GLP-1 RAs) for type 2 diabetes and weight management rose from 8722 to 60,567 between 2020 and 2023 — a nearly sevenfold increase.
“The number of adolescents taking these medications is going up because they work,” said Suzanne Cuda, MD, medical director of Alamo City Healthy Kids and Families, a medical weight management clinic in San Antonio. The medications have been shown to treat type 2 diabetes, lower blood pressure, and reduce the risk for cardiovascular diseases.
“The younger you are, the better the outcome,” Dr. Cuda said.
How GLP-1 agonists may affect adolescents in the long run is not yet clear. Existing studies on GLP-1 medications in patients with eating disorders have shown mixed results. Some studies indicate that the drugs decrease binge episodes for those with binge eating disorder or bulimia nervosa. However, these studies had small sample sizes and measured only short-term effects, leaving long-term outcomes and risks unknown.
Traditional treatments for eating disorders emphasize regular eating patterns, body acceptance, addressing weight stigma, and improving attunement to hunger and fullness cues — approaches that may conflict with the effects of GLP-1 agonists. These drugs suppress appetite, alter metabolic signals, and may unintentionally reinforce weight loss as a primary goal, creating a potential disconnect between the aims of recovery from eating disorders and the biologic effects of the medication, experts said.
Dr. Cuda said she has cared for adolescents with diagnosed eating disorders in her practice who are seeking GLP-1 agonists. She said she first works with patients to treat the underlying disorder before prescribing medication.
“One of the concerns is the extreme reductions in calories that could be induced by GLP-1 RA in children and adolescents,” she said. Unlike adults, adolescents use caloric energy not just for physical activity but also for growing and developing, she said.
“They can’t catch up on that growth and development,” she added.
Advice for Screening and Monitoring
The National Eating Disorders Association raised concerns about the potential misuse of these medications and their potential to exacerbate eating disorder behaviors in people who are already at a higher risk of developing one of the conditions, including those with existing mental health disorders, stress, who have already dieted, and who have experienced weight-centric bullying.
Clinicians should be on the lookout for patients seeking GLP-1s who present with symptoms of an eating disorder that may be less apparent, such as picky eating, insomnia or difficulty sleeping, or, for girls, irregular menstrual periods, Dr. Dennis said. These patients may be more likely to go undiagnosed or misdiagnosed. Research also suggests that people of color are less likely to be diagnosed or receive specialty care for eating disorders.
Discussions between patients and clinicians about obesity treatment prior to prescribing provide a crucial opportunity to screen and monitor for disordered eating, which Dr. Dennis said does not universally occur currently.
Dr. Dennis recommended initial assessments using validated screening tools like the EDE-Q and the Center for Epidemiologic Studies Depression Scale Revised, 10-Item Version.
Ongoing monitoring throughout treatment is essential, with initial monthly check-ins that include dietary counseling to detect subtle changes in eating behaviors or attitudes toward food and body image, Dr. Cuda said.
The Obesity Medicine Association (OMA) has stressed the importance of a collaborative approach involving connections with mental health professionals specializing in eating disorders and dietitians.
“If you have a chance to send them to an obesity medicine specialist, you should do that,” said Dr. Cuda, who coauthored the OMA statement. “It’s impractical to expect a primary care physician to do everything: Screen for dietary disorders, do a full dietary counseling, follow up on their activity.”
For patients showing signs of disordered eating, clinicians should avoid recommending restrictive dietary approaches, like cutting out food groups such as carbohydrates or a restricted calorie goal. Instead, they can suggest focusing on healthier lifestyle habits and referring to a psychotherapist, the experts said. Clinicians also should be prepared to adjust or pause GLP-1 agonists if disordered eating disorder symptoms worsen.
“I think a weight-agnostic approach where the focus of care is not weight loss but increase in health protective behaviors and nutritional intake is safest for all kids, especially those with eating disorders or eating disorder risk factors,” Dr. Dennis said.
Various authors of the eating disorder study reported receiving grants, advisory board fees, and speaker fees from entities including the National Health and Medical Research Council of Australia, Eli Lilly, Novo Nordisk, Nu-Mega Ingredients, and the National Institutes of Health, among others.
A version of this article appeared on Medscape.com.
Now, with the rising popularity of medications like Ozempic for weight loss, she fears she will care for more teens with eating disorders who are seeking glucagon-like peptide 1 (GLP-1) agonists or who have developed a disorder while taking them.
“We haven’t seen patients yet, but I’m sure they are on their way,” said Dr. Dennis, a clinical assistant professor in the Department of Psychiatry at the University of Illinois College of Medicine in Chicago. She is also the cofounder and chief medical officer of SunCloud Health, an outpatient eating disorder treatment center in Illinois.
Dr. Dennis’ concerns reflect a growing unease among eating disorder specialists as obesity medications gain traction for adolescent use. A recent study published in JAMA Pediatrics showed nearly 80% of teens in treatment for obesity reported symptoms of disordered eating at the outset of an intervention. These included signs of binge eating and loss of control.
The randomized clinical trial, conducted from 2018 to 2023, examined 141 adolescents with obesity undergoing interventions like low-energy diets or intermittent energy restriction. Almost half scored as having risk for an undiagnosed eating disorder, as defined by the Eating Disorder Examination Questionnaire (EDE-Q).
At the end of the intervention, many teens continued to have symptoms of disordered eating, while a smaller group was newly scored as having a risk for an eating disorder.
Weight Loss and Eating Disorders: A Balancing Act
The findings illuminate a significant challenge for pediatricians and primary care clinicians: Balancing effective weight management with the risk of exacerbating or triggering eating disorders, said Hiba Jebeile, PhD, a research dietitian at The Children’s Hospital at Westmead in Australia, and the study’s lead author. Adding weight loss medication on top of the equation can further complicate care.
“It is helpful for obesity and eating disorder services to work together, with clear referral pathways, to manage these adolescents,” Dr. Jebeile said.
The US Food and Drug Administration approved semaglutide for weight loss in adolescents aged 12-17 years in December 2020. One study found that the number of adolescents prescribed GLP-1 receptor agonists (GLP-1 RAs) for type 2 diabetes and weight management rose from 8722 to 60,567 between 2020 and 2023 — a nearly sevenfold increase.
“The number of adolescents taking these medications is going up because they work,” said Suzanne Cuda, MD, medical director of Alamo City Healthy Kids and Families, a medical weight management clinic in San Antonio. The medications have been shown to treat type 2 diabetes, lower blood pressure, and reduce the risk for cardiovascular diseases.
“The younger you are, the better the outcome,” Dr. Cuda said.
How GLP-1 agonists may affect adolescents in the long run is not yet clear. Existing studies on GLP-1 medications in patients with eating disorders have shown mixed results. Some studies indicate that the drugs decrease binge episodes for those with binge eating disorder or bulimia nervosa. However, these studies had small sample sizes and measured only short-term effects, leaving long-term outcomes and risks unknown.
Traditional treatments for eating disorders emphasize regular eating patterns, body acceptance, addressing weight stigma, and improving attunement to hunger and fullness cues — approaches that may conflict with the effects of GLP-1 agonists. These drugs suppress appetite, alter metabolic signals, and may unintentionally reinforce weight loss as a primary goal, creating a potential disconnect between the aims of recovery from eating disorders and the biologic effects of the medication, experts said.
Dr. Cuda said she has cared for adolescents with diagnosed eating disorders in her practice who are seeking GLP-1 agonists. She said she first works with patients to treat the underlying disorder before prescribing medication.
“One of the concerns is the extreme reductions in calories that could be induced by GLP-1 RA in children and adolescents,” she said. Unlike adults, adolescents use caloric energy not just for physical activity but also for growing and developing, she said.
“They can’t catch up on that growth and development,” she added.
Advice for Screening and Monitoring
The National Eating Disorders Association raised concerns about the potential misuse of these medications and their potential to exacerbate eating disorder behaviors in people who are already at a higher risk of developing one of the conditions, including those with existing mental health disorders, stress, who have already dieted, and who have experienced weight-centric bullying.
Clinicians should be on the lookout for patients seeking GLP-1s who present with symptoms of an eating disorder that may be less apparent, such as picky eating, insomnia or difficulty sleeping, or, for girls, irregular menstrual periods, Dr. Dennis said. These patients may be more likely to go undiagnosed or misdiagnosed. Research also suggests that people of color are less likely to be diagnosed or receive specialty care for eating disorders.
Discussions between patients and clinicians about obesity treatment prior to prescribing provide a crucial opportunity to screen and monitor for disordered eating, which Dr. Dennis said does not universally occur currently.
Dr. Dennis recommended initial assessments using validated screening tools like the EDE-Q and the Center for Epidemiologic Studies Depression Scale Revised, 10-Item Version.
Ongoing monitoring throughout treatment is essential, with initial monthly check-ins that include dietary counseling to detect subtle changes in eating behaviors or attitudes toward food and body image, Dr. Cuda said.
The Obesity Medicine Association (OMA) has stressed the importance of a collaborative approach involving connections with mental health professionals specializing in eating disorders and dietitians.
“If you have a chance to send them to an obesity medicine specialist, you should do that,” said Dr. Cuda, who coauthored the OMA statement. “It’s impractical to expect a primary care physician to do everything: Screen for dietary disorders, do a full dietary counseling, follow up on their activity.”
For patients showing signs of disordered eating, clinicians should avoid recommending restrictive dietary approaches, like cutting out food groups such as carbohydrates or a restricted calorie goal. Instead, they can suggest focusing on healthier lifestyle habits and referring to a psychotherapist, the experts said. Clinicians also should be prepared to adjust or pause GLP-1 agonists if disordered eating disorder symptoms worsen.
“I think a weight-agnostic approach where the focus of care is not weight loss but increase in health protective behaviors and nutritional intake is safest for all kids, especially those with eating disorders or eating disorder risk factors,” Dr. Dennis said.
Various authors of the eating disorder study reported receiving grants, advisory board fees, and speaker fees from entities including the National Health and Medical Research Council of Australia, Eli Lilly, Novo Nordisk, Nu-Mega Ingredients, and the National Institutes of Health, among others.
A version of this article appeared on Medscape.com.
FROM JAMA PEDIATRICS
Introducing: A New Way to Get Teens Mental Health Care
Lauren Opladen remembers the agonizing wait all too well.
At age 17, struggling with paralyzing depression after losing her brother to suicide and her father to amyotrophic lateral sclerosis, her teacher suggested she seek help.
So, she did. But she had to spend 3 days inside an emergency department at the University of Rochester Medical Center in Rochester, New York, where the Comprehensive Psychiatric Emergency Program (CPEP) provides immediate care for youth and adults experiencing psychiatric emergencies.
“We were sleeping on a couch just waiting for all these services, when that’s precious time wasted,” Ms. Opladen said.
Ms. Opladen made it through that dark period, and 5 years later, she is a registered nurse at the same hospital. Every day she walks past a new facility she wishes had existed during her troubled teenage years: An urgent care center for children and adolescents experiencing mental health crises.
Brighter Days Pediatric Mental Health Urgent Care Center, Rochester, New York, opened in July as a walk-in clinic offering rapid assessment, crisis intervention, and short-term stabilization, provides referrals to counseling or psychiatric care. Children and adolescents at immediate risk of harming themselves or others, or who need inpatient care, are sent to CPEP or another emergency department in the area.
Similar walk-in facilities linking youth to longer-term services are popping up in nearly a dozen states, including New York, Ohio, Massachusetts, and Wisconsin. The emerging model of care may offer a crucial bridge between traditional outpatient services and emergency room (ER) visits for some young people experiencing mental health crises.
“We’ve seen a significant increase in the number of children and adolescents presenting to emergency departments with mental health concerns,” said Michael A. Scharf, MD, chief of the Division of Child and Adolescent Psychiatry at the University of Rochester Medical Center, who oversees operations at Brighter Days. “These urgent care centers provide a more appropriate setting for many of these cases, offering specialized care without the often overwhelming environment of an ER.”
The urgency of addressing youth behavioral health has become increasingly apparent. The most recent data from the US Centers for Disease Control and Prevention showed that over a 6-month period in 2020, during the early months of the COVID-19 pandemic, visits to the emergency department for mental health problems spiked 24% among children aged 5-11 years and 31% among 12-17-year-olds compared with the same period in 2019. Between March 2021 and February 2022, such emergency visits rose by 22% for teen girls, while falling by 15% for boys ages 5-12 years and 9% for older boys. Most visits occur during the school year.
But staffing shortages and limited physical space are taxing the capacity of the healthcare system to screen, diagnose, and manage these patients, according to a 2023 report published in Pediatrics.
Urgent Care: A Misnomer?
Some in the mental health community said the label “urgent” in these centers’ titles is misleading. Brighter Days and similar facilities do not conduct involuntary holds, administer medication, or handle serious cases like psychotic episodes.
David Mathison, MD, senior vice president of clinic operations at PM Pediatrics, a chain of pediatric urgent care clinics in Maryland, said patients and their families may mistakenly believe the centers will address mental health problems quickly.
“It’s really not urgent behavioral health. It’s really just another access point to get behavioral health,” Dr. Mathison said. “Crises in pediatrics are so much more complex” than physical injuries or acute infections, which are the bread and butter of urgent care centers.
“An urgent care center almost implies you’re going to come in for a solution to a simple problem, and it’s going to be done relatively quickly on demand, and it’s just not what the behavioral health centers do,” he said.
Dr. Mathison, who also serves on the executive committee for the section on urgent care at the American Academy of Pediatrics, likened the centers to in-person versions of crisis center hotlines, which offer virtual counseling and talk therapy and may refer individuals to specialists who can provide clinical care over the long term.
Instead, Brighter Days and other centers provide crisis de-escalation for individuals experiencing an exacerbation of a diagnosed mental illness, such a manic episode from bipolar disorder.
“Most places aren’t just going to change their therapy without either contacting their psychiatrist or having psychiatrists on staff,” Dr. Mathison said.
Other challenges at Brighter Days and similar centers include staffing with appropriately trained mental health professionals, given the nationwide shortage of child and adolescent psychiatrists, Dr. Scharf said.
The number of child and adolescent psychiatrists per 100,000 children varies significantly across states. Nationally, the average stands at 14 psychiatrists per 100,000 children, but ranges from as low as 4 to 65, according to the American Academy of Child & Adolescent Psychiatry.
For now, Dr. Scharf said, patients who visit Brighter Days are billed as if they are having a routine pediatric office visit as opposed to a pricier trip to the emergency department. And the center accepts all individuals, regardless of their insurance status.
Ms. Opladen said the urgent care center represents a significant improvement over her experience at the emergency department’s psychiatric triage.
“I saw how awful it was and just the environment,” she said. “The first thing I thought was, what do I need to do to get out of here?”
She said the pediatric mental health urgent care centers are “the complete opposite.” Like Brighter Days, these centers are designed to look more like a pediatrician’s office, with bright welcoming colors and games and toys.
“It’s separated from everything else. There’s a welcome, relaxed space,” she said. “The welcoming feel is just a whole different environment, and that’s really how it should be.”
A version of this article first appeared on Medscape.com.
Lauren Opladen remembers the agonizing wait all too well.
At age 17, struggling with paralyzing depression after losing her brother to suicide and her father to amyotrophic lateral sclerosis, her teacher suggested she seek help.
So, she did. But she had to spend 3 days inside an emergency department at the University of Rochester Medical Center in Rochester, New York, where the Comprehensive Psychiatric Emergency Program (CPEP) provides immediate care for youth and adults experiencing psychiatric emergencies.
“We were sleeping on a couch just waiting for all these services, when that’s precious time wasted,” Ms. Opladen said.
Ms. Opladen made it through that dark period, and 5 years later, she is a registered nurse at the same hospital. Every day she walks past a new facility she wishes had existed during her troubled teenage years: An urgent care center for children and adolescents experiencing mental health crises.
Brighter Days Pediatric Mental Health Urgent Care Center, Rochester, New York, opened in July as a walk-in clinic offering rapid assessment, crisis intervention, and short-term stabilization, provides referrals to counseling or psychiatric care. Children and adolescents at immediate risk of harming themselves or others, or who need inpatient care, are sent to CPEP or another emergency department in the area.
Similar walk-in facilities linking youth to longer-term services are popping up in nearly a dozen states, including New York, Ohio, Massachusetts, and Wisconsin. The emerging model of care may offer a crucial bridge between traditional outpatient services and emergency room (ER) visits for some young people experiencing mental health crises.
“We’ve seen a significant increase in the number of children and adolescents presenting to emergency departments with mental health concerns,” said Michael A. Scharf, MD, chief of the Division of Child and Adolescent Psychiatry at the University of Rochester Medical Center, who oversees operations at Brighter Days. “These urgent care centers provide a more appropriate setting for many of these cases, offering specialized care without the often overwhelming environment of an ER.”
The urgency of addressing youth behavioral health has become increasingly apparent. The most recent data from the US Centers for Disease Control and Prevention showed that over a 6-month period in 2020, during the early months of the COVID-19 pandemic, visits to the emergency department for mental health problems spiked 24% among children aged 5-11 years and 31% among 12-17-year-olds compared with the same period in 2019. Between March 2021 and February 2022, such emergency visits rose by 22% for teen girls, while falling by 15% for boys ages 5-12 years and 9% for older boys. Most visits occur during the school year.
But staffing shortages and limited physical space are taxing the capacity of the healthcare system to screen, diagnose, and manage these patients, according to a 2023 report published in Pediatrics.
Urgent Care: A Misnomer?
Some in the mental health community said the label “urgent” in these centers’ titles is misleading. Brighter Days and similar facilities do not conduct involuntary holds, administer medication, or handle serious cases like psychotic episodes.
David Mathison, MD, senior vice president of clinic operations at PM Pediatrics, a chain of pediatric urgent care clinics in Maryland, said patients and their families may mistakenly believe the centers will address mental health problems quickly.
“It’s really not urgent behavioral health. It’s really just another access point to get behavioral health,” Dr. Mathison said. “Crises in pediatrics are so much more complex” than physical injuries or acute infections, which are the bread and butter of urgent care centers.
“An urgent care center almost implies you’re going to come in for a solution to a simple problem, and it’s going to be done relatively quickly on demand, and it’s just not what the behavioral health centers do,” he said.
Dr. Mathison, who also serves on the executive committee for the section on urgent care at the American Academy of Pediatrics, likened the centers to in-person versions of crisis center hotlines, which offer virtual counseling and talk therapy and may refer individuals to specialists who can provide clinical care over the long term.
Instead, Brighter Days and other centers provide crisis de-escalation for individuals experiencing an exacerbation of a diagnosed mental illness, such a manic episode from bipolar disorder.
“Most places aren’t just going to change their therapy without either contacting their psychiatrist or having psychiatrists on staff,” Dr. Mathison said.
Other challenges at Brighter Days and similar centers include staffing with appropriately trained mental health professionals, given the nationwide shortage of child and adolescent psychiatrists, Dr. Scharf said.
The number of child and adolescent psychiatrists per 100,000 children varies significantly across states. Nationally, the average stands at 14 psychiatrists per 100,000 children, but ranges from as low as 4 to 65, according to the American Academy of Child & Adolescent Psychiatry.
For now, Dr. Scharf said, patients who visit Brighter Days are billed as if they are having a routine pediatric office visit as opposed to a pricier trip to the emergency department. And the center accepts all individuals, regardless of their insurance status.
Ms. Opladen said the urgent care center represents a significant improvement over her experience at the emergency department’s psychiatric triage.
“I saw how awful it was and just the environment,” she said. “The first thing I thought was, what do I need to do to get out of here?”
She said the pediatric mental health urgent care centers are “the complete opposite.” Like Brighter Days, these centers are designed to look more like a pediatrician’s office, with bright welcoming colors and games and toys.
“It’s separated from everything else. There’s a welcome, relaxed space,” she said. “The welcoming feel is just a whole different environment, and that’s really how it should be.”
A version of this article first appeared on Medscape.com.
Lauren Opladen remembers the agonizing wait all too well.
At age 17, struggling with paralyzing depression after losing her brother to suicide and her father to amyotrophic lateral sclerosis, her teacher suggested she seek help.
So, she did. But she had to spend 3 days inside an emergency department at the University of Rochester Medical Center in Rochester, New York, where the Comprehensive Psychiatric Emergency Program (CPEP) provides immediate care for youth and adults experiencing psychiatric emergencies.
“We were sleeping on a couch just waiting for all these services, when that’s precious time wasted,” Ms. Opladen said.
Ms. Opladen made it through that dark period, and 5 years later, she is a registered nurse at the same hospital. Every day she walks past a new facility she wishes had existed during her troubled teenage years: An urgent care center for children and adolescents experiencing mental health crises.
Brighter Days Pediatric Mental Health Urgent Care Center, Rochester, New York, opened in July as a walk-in clinic offering rapid assessment, crisis intervention, and short-term stabilization, provides referrals to counseling or psychiatric care. Children and adolescents at immediate risk of harming themselves or others, or who need inpatient care, are sent to CPEP or another emergency department in the area.
Similar walk-in facilities linking youth to longer-term services are popping up in nearly a dozen states, including New York, Ohio, Massachusetts, and Wisconsin. The emerging model of care may offer a crucial bridge between traditional outpatient services and emergency room (ER) visits for some young people experiencing mental health crises.
“We’ve seen a significant increase in the number of children and adolescents presenting to emergency departments with mental health concerns,” said Michael A. Scharf, MD, chief of the Division of Child and Adolescent Psychiatry at the University of Rochester Medical Center, who oversees operations at Brighter Days. “These urgent care centers provide a more appropriate setting for many of these cases, offering specialized care without the often overwhelming environment of an ER.”
The urgency of addressing youth behavioral health has become increasingly apparent. The most recent data from the US Centers for Disease Control and Prevention showed that over a 6-month period in 2020, during the early months of the COVID-19 pandemic, visits to the emergency department for mental health problems spiked 24% among children aged 5-11 years and 31% among 12-17-year-olds compared with the same period in 2019. Between March 2021 and February 2022, such emergency visits rose by 22% for teen girls, while falling by 15% for boys ages 5-12 years and 9% for older boys. Most visits occur during the school year.
But staffing shortages and limited physical space are taxing the capacity of the healthcare system to screen, diagnose, and manage these patients, according to a 2023 report published in Pediatrics.
Urgent Care: A Misnomer?
Some in the mental health community said the label “urgent” in these centers’ titles is misleading. Brighter Days and similar facilities do not conduct involuntary holds, administer medication, or handle serious cases like psychotic episodes.
David Mathison, MD, senior vice president of clinic operations at PM Pediatrics, a chain of pediatric urgent care clinics in Maryland, said patients and their families may mistakenly believe the centers will address mental health problems quickly.
“It’s really not urgent behavioral health. It’s really just another access point to get behavioral health,” Dr. Mathison said. “Crises in pediatrics are so much more complex” than physical injuries or acute infections, which are the bread and butter of urgent care centers.
“An urgent care center almost implies you’re going to come in for a solution to a simple problem, and it’s going to be done relatively quickly on demand, and it’s just not what the behavioral health centers do,” he said.
Dr. Mathison, who also serves on the executive committee for the section on urgent care at the American Academy of Pediatrics, likened the centers to in-person versions of crisis center hotlines, which offer virtual counseling and talk therapy and may refer individuals to specialists who can provide clinical care over the long term.
Instead, Brighter Days and other centers provide crisis de-escalation for individuals experiencing an exacerbation of a diagnosed mental illness, such a manic episode from bipolar disorder.
“Most places aren’t just going to change their therapy without either contacting their psychiatrist or having psychiatrists on staff,” Dr. Mathison said.
Other challenges at Brighter Days and similar centers include staffing with appropriately trained mental health professionals, given the nationwide shortage of child and adolescent psychiatrists, Dr. Scharf said.
The number of child and adolescent psychiatrists per 100,000 children varies significantly across states. Nationally, the average stands at 14 psychiatrists per 100,000 children, but ranges from as low as 4 to 65, according to the American Academy of Child & Adolescent Psychiatry.
For now, Dr. Scharf said, patients who visit Brighter Days are billed as if they are having a routine pediatric office visit as opposed to a pricier trip to the emergency department. And the center accepts all individuals, regardless of their insurance status.
Ms. Opladen said the urgent care center represents a significant improvement over her experience at the emergency department’s psychiatric triage.
“I saw how awful it was and just the environment,” she said. “The first thing I thought was, what do I need to do to get out of here?”
She said the pediatric mental health urgent care centers are “the complete opposite.” Like Brighter Days, these centers are designed to look more like a pediatrician’s office, with bright welcoming colors and games and toys.
“It’s separated from everything else. There’s a welcome, relaxed space,” she said. “The welcoming feel is just a whole different environment, and that’s really how it should be.”
A version of this article first appeared on Medscape.com.
Clinicians Face Hurdles in Caring for the Growing Number of Cancer Survivors
BOSTON — Primary care clinicians face challenges in knowledge and care coordination as they care for a rising number of cancer survivors in the United States, according to panelists who spoke during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
By the year 2040, an estimated 26 million people will have lived ≥ 5 years after their initial cancer diagnosis, an increase of eight million from 2022, according to the National Cancer Institute. Primary care clinicians must help patients with new health problems that emerge as the result of previous cancer treatments and with side effects that can last for decades.
“It’s a good thing that more people are living longer and living better after cancer, but now that means we have to train an army of primary care doctors to feel empowered to take care of these patients in a general setting,” said Ilana Yurkiewicz, MD, an oncologist, internal medicine physician, and clinical assistant professor at Stanford University, Stanford, California, who co-moderated the workshop.
Dr. Yurkiewicz and her fellow panelists emphasized the high likelihood that every primary care clinician is currently caring for a survivor of cancer.
One of the greatest barriers these clinicians face in caring for survivors is the difficulty in getting screening tests paid for by insurers, according to Regina Jacob, MD, associate professor at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, who co-moderated the session.
“We have a tough time getting surveillance tests [for cancer] covered through insurance” because in some cases physician groups do not provide consensus on which surveillance tools to use or how often people should be screened, Dr. Jacob said.
For instance, the American Gastroenterological Association and the US Preventive Services Task Force — which many insurers use as basis for coverage determinations — offer differing recommendations.
Primary care physicians also face challenges in understanding the complexity of conditions patients may face during and after cancer treatment since conditions that emerge from cancer or treatment may vary among patients.
“Cancer survivorship starts the day of the diagnosis,” said Dr. Yurkiewicz. “It doesn’t necessarily mean someone who has completed cancer treatment.”
During the workshop, participants offered their own recommendations for care based on case studies, which included issues such as long-term effects of cancer and its therapies, which may arise immediately after or even years or decades after treatment.
A common situation for cancer survivors involves new health issues that occur after treatment has ended.
“Who do they turn to in cases where they don’t know if it’s related to the cancer or the cancer treatment or are separate issues? Do they turn to their oncologist? Do they turn to their primary care doctor?” Dr. Yurkiewicz said. “How should I, the primary care doctor, be thinking about the issue?”
She proposed that primary care clinicians give patients a 2-week waiting period at the onset of a symptom before intervening.
Participants also suggested establishing rapport with the treating oncologist and other specialists so that if a question arises, the primary care clinician can ask for advice.
The method physicians choose to communicate and coordinate care should be tailored to the health system in which they work, participants suggested.
“Some people have the luxury of having a unified electronic health record; some people don’t have that luxury,” said Dr. Jacob. “Recognize the institution in which you work, recognize the context in which you work, and develop a communication strategy that closes the gap.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Primary care clinicians face challenges in knowledge and care coordination as they care for a rising number of cancer survivors in the United States, according to panelists who spoke during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
By the year 2040, an estimated 26 million people will have lived ≥ 5 years after their initial cancer diagnosis, an increase of eight million from 2022, according to the National Cancer Institute. Primary care clinicians must help patients with new health problems that emerge as the result of previous cancer treatments and with side effects that can last for decades.
“It’s a good thing that more people are living longer and living better after cancer, but now that means we have to train an army of primary care doctors to feel empowered to take care of these patients in a general setting,” said Ilana Yurkiewicz, MD, an oncologist, internal medicine physician, and clinical assistant professor at Stanford University, Stanford, California, who co-moderated the workshop.
Dr. Yurkiewicz and her fellow panelists emphasized the high likelihood that every primary care clinician is currently caring for a survivor of cancer.
One of the greatest barriers these clinicians face in caring for survivors is the difficulty in getting screening tests paid for by insurers, according to Regina Jacob, MD, associate professor at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, who co-moderated the session.
“We have a tough time getting surveillance tests [for cancer] covered through insurance” because in some cases physician groups do not provide consensus on which surveillance tools to use or how often people should be screened, Dr. Jacob said.
For instance, the American Gastroenterological Association and the US Preventive Services Task Force — which many insurers use as basis for coverage determinations — offer differing recommendations.
Primary care physicians also face challenges in understanding the complexity of conditions patients may face during and after cancer treatment since conditions that emerge from cancer or treatment may vary among patients.
“Cancer survivorship starts the day of the diagnosis,” said Dr. Yurkiewicz. “It doesn’t necessarily mean someone who has completed cancer treatment.”
During the workshop, participants offered their own recommendations for care based on case studies, which included issues such as long-term effects of cancer and its therapies, which may arise immediately after or even years or decades after treatment.
A common situation for cancer survivors involves new health issues that occur after treatment has ended.
“Who do they turn to in cases where they don’t know if it’s related to the cancer or the cancer treatment or are separate issues? Do they turn to their oncologist? Do they turn to their primary care doctor?” Dr. Yurkiewicz said. “How should I, the primary care doctor, be thinking about the issue?”
She proposed that primary care clinicians give patients a 2-week waiting period at the onset of a symptom before intervening.
Participants also suggested establishing rapport with the treating oncologist and other specialists so that if a question arises, the primary care clinician can ask for advice.
The method physicians choose to communicate and coordinate care should be tailored to the health system in which they work, participants suggested.
“Some people have the luxury of having a unified electronic health record; some people don’t have that luxury,” said Dr. Jacob. “Recognize the institution in which you work, recognize the context in which you work, and develop a communication strategy that closes the gap.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Primary care clinicians face challenges in knowledge and care coordination as they care for a rising number of cancer survivors in the United States, according to panelists who spoke during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
By the year 2040, an estimated 26 million people will have lived ≥ 5 years after their initial cancer diagnosis, an increase of eight million from 2022, according to the National Cancer Institute. Primary care clinicians must help patients with new health problems that emerge as the result of previous cancer treatments and with side effects that can last for decades.
“It’s a good thing that more people are living longer and living better after cancer, but now that means we have to train an army of primary care doctors to feel empowered to take care of these patients in a general setting,” said Ilana Yurkiewicz, MD, an oncologist, internal medicine physician, and clinical assistant professor at Stanford University, Stanford, California, who co-moderated the workshop.
Dr. Yurkiewicz and her fellow panelists emphasized the high likelihood that every primary care clinician is currently caring for a survivor of cancer.
One of the greatest barriers these clinicians face in caring for survivors is the difficulty in getting screening tests paid for by insurers, according to Regina Jacob, MD, associate professor at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, who co-moderated the session.
“We have a tough time getting surveillance tests [for cancer] covered through insurance” because in some cases physician groups do not provide consensus on which surveillance tools to use or how often people should be screened, Dr. Jacob said.
For instance, the American Gastroenterological Association and the US Preventive Services Task Force — which many insurers use as basis for coverage determinations — offer differing recommendations.
Primary care physicians also face challenges in understanding the complexity of conditions patients may face during and after cancer treatment since conditions that emerge from cancer or treatment may vary among patients.
“Cancer survivorship starts the day of the diagnosis,” said Dr. Yurkiewicz. “It doesn’t necessarily mean someone who has completed cancer treatment.”
During the workshop, participants offered their own recommendations for care based on case studies, which included issues such as long-term effects of cancer and its therapies, which may arise immediately after or even years or decades after treatment.
A common situation for cancer survivors involves new health issues that occur after treatment has ended.
“Who do they turn to in cases where they don’t know if it’s related to the cancer or the cancer treatment or are separate issues? Do they turn to their oncologist? Do they turn to their primary care doctor?” Dr. Yurkiewicz said. “How should I, the primary care doctor, be thinking about the issue?”
She proposed that primary care clinicians give patients a 2-week waiting period at the onset of a symptom before intervening.
Participants also suggested establishing rapport with the treating oncologist and other specialists so that if a question arises, the primary care clinician can ask for advice.
The method physicians choose to communicate and coordinate care should be tailored to the health system in which they work, participants suggested.
“Some people have the luxury of having a unified electronic health record; some people don’t have that luxury,” said Dr. Jacob. “Recognize the institution in which you work, recognize the context in which you work, and develop a communication strategy that closes the gap.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SGIM 2024
Helping Patients With Intellectual Disabilities Make Informed Decisions
BOSTON — Primary care clinicians caring for patients with intellectual and developmental disabilities often recommend guardianship, a responsibility with life-altering implications.
But only approximately 30% of primary care residency programs in the United States provide training on how to assess the ability of patients with disabilities to make decisions for themselves, and much of this training is optional, according to a recent study cited during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
Assessing the capacity of patients with disabilities involves navigating a maze of legal, ethical, and clinical considerations, according to Mary Thomas, MD, MPH, a clinical fellow in geriatrics at Yale University School of Medicine in New Haven, Connecticut, who co-moderated the workshop.
Guardianship, while sometimes necessary, can be overly restrictive and diminish patient autonomy, she said. The legal process — ultimately decided through the courts — gives a guardian permission to manage medical care and make decisions for someone who cannot make or communicate those decisions themselves.
Clinicians can assess patients through an evaluation of functional capacity, which allows them to observe a patient’s demeanor and administer a cognition test. Alternatives such as supported decision-making may be less restrictive and can better serve patients, she said. Supported decision-making allows for a person with disabilities to receive assistance from a supporter who can help a patient process medical conditions and treatment needs. The supporter helps empower capable patients to decide on their own.
Some states have introduced legislation that would legally recognize supported decision-making as a less restrictive alternative to guardianship or conservatorship, in which a court-appointed individual manages all aspects of a person’s life.
Sara Mixter, MD, MPH, an assistant professor of medicine and pediatrics at the Johns Hopkins University School of Medicine in Baltimore and a co-moderator of the workshop, called the use of inclusive language in patient communication the “first step toward fostering an environment where patients feel respected and understood.”
Inclusive conversations can include person-first language and using words such as “caregiver” rather than “caretaker.”
Dr. Thomas and Dr. Mixter also called for the directors of residency programs to provide more training on disabilities. They cited a 2023 survey of directors, many of whom said that educational boards do not require training in disability-specific care and that experts in the care of people with disabilities are few and far between.
“Education and awareness are key to overcoming the challenges we face,” Dr. Thomas said. “Improving our training programs means we can ensure that all patients receive the care and respect they deserve.”
Dr. Thomas and Dr. Mixter report no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Primary care clinicians caring for patients with intellectual and developmental disabilities often recommend guardianship, a responsibility with life-altering implications.
But only approximately 30% of primary care residency programs in the United States provide training on how to assess the ability of patients with disabilities to make decisions for themselves, and much of this training is optional, according to a recent study cited during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
Assessing the capacity of patients with disabilities involves navigating a maze of legal, ethical, and clinical considerations, according to Mary Thomas, MD, MPH, a clinical fellow in geriatrics at Yale University School of Medicine in New Haven, Connecticut, who co-moderated the workshop.
Guardianship, while sometimes necessary, can be overly restrictive and diminish patient autonomy, she said. The legal process — ultimately decided through the courts — gives a guardian permission to manage medical care and make decisions for someone who cannot make or communicate those decisions themselves.
Clinicians can assess patients through an evaluation of functional capacity, which allows them to observe a patient’s demeanor and administer a cognition test. Alternatives such as supported decision-making may be less restrictive and can better serve patients, she said. Supported decision-making allows for a person with disabilities to receive assistance from a supporter who can help a patient process medical conditions and treatment needs. The supporter helps empower capable patients to decide on their own.
Some states have introduced legislation that would legally recognize supported decision-making as a less restrictive alternative to guardianship or conservatorship, in which a court-appointed individual manages all aspects of a person’s life.
Sara Mixter, MD, MPH, an assistant professor of medicine and pediatrics at the Johns Hopkins University School of Medicine in Baltimore and a co-moderator of the workshop, called the use of inclusive language in patient communication the “first step toward fostering an environment where patients feel respected and understood.”
Inclusive conversations can include person-first language and using words such as “caregiver” rather than “caretaker.”
Dr. Thomas and Dr. Mixter also called for the directors of residency programs to provide more training on disabilities. They cited a 2023 survey of directors, many of whom said that educational boards do not require training in disability-specific care and that experts in the care of people with disabilities are few and far between.
“Education and awareness are key to overcoming the challenges we face,” Dr. Thomas said. “Improving our training programs means we can ensure that all patients receive the care and respect they deserve.”
Dr. Thomas and Dr. Mixter report no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Primary care clinicians caring for patients with intellectual and developmental disabilities often recommend guardianship, a responsibility with life-altering implications.
But only approximately 30% of primary care residency programs in the United States provide training on how to assess the ability of patients with disabilities to make decisions for themselves, and much of this training is optional, according to a recent study cited during a workshop at the 2024 annual meeting of the Society of General Internal Medicine.
Assessing the capacity of patients with disabilities involves navigating a maze of legal, ethical, and clinical considerations, according to Mary Thomas, MD, MPH, a clinical fellow in geriatrics at Yale University School of Medicine in New Haven, Connecticut, who co-moderated the workshop.
Guardianship, while sometimes necessary, can be overly restrictive and diminish patient autonomy, she said. The legal process — ultimately decided through the courts — gives a guardian permission to manage medical care and make decisions for someone who cannot make or communicate those decisions themselves.
Clinicians can assess patients through an evaluation of functional capacity, which allows them to observe a patient’s demeanor and administer a cognition test. Alternatives such as supported decision-making may be less restrictive and can better serve patients, she said. Supported decision-making allows for a person with disabilities to receive assistance from a supporter who can help a patient process medical conditions and treatment needs. The supporter helps empower capable patients to decide on their own.
Some states have introduced legislation that would legally recognize supported decision-making as a less restrictive alternative to guardianship or conservatorship, in which a court-appointed individual manages all aspects of a person’s life.
Sara Mixter, MD, MPH, an assistant professor of medicine and pediatrics at the Johns Hopkins University School of Medicine in Baltimore and a co-moderator of the workshop, called the use of inclusive language in patient communication the “first step toward fostering an environment where patients feel respected and understood.”
Inclusive conversations can include person-first language and using words such as “caregiver” rather than “caretaker.”
Dr. Thomas and Dr. Mixter also called for the directors of residency programs to provide more training on disabilities. They cited a 2023 survey of directors, many of whom said that educational boards do not require training in disability-specific care and that experts in the care of people with disabilities are few and far between.
“Education and awareness are key to overcoming the challenges we face,” Dr. Thomas said. “Improving our training programs means we can ensure that all patients receive the care and respect they deserve.”
Dr. Thomas and Dr. Mixter report no relevant disclosures.
A version of this article first appeared on Medscape.com.
Asynchronous Primary Care Offers Challenges, Opportunities
BOSTON — Online patient portals have shifted patient expectations of how quickly clinicians respond and provide timely care, which can lead to burnout. But asynchronous care can, in some cases, be compensated and increase physician productivity and enhance patient care, according to experts who led a workshop at the Society of General Internal Medicine (SGIM) 2024 Annual Meeting.
Patient portal visits have increased in popularity and use since the COVID-19 pandemic. For primary care clinicians especially, the amount of time spent and the span of requests, from messages with new health concerns to requests for prescription refills, can be daunting.
“Understanding the nuances of these relationships is pivotal in navigating the evolution toward asynchronous care,” said Jennifer Schmidt, MD, an assistant professor of medicine at the Washington University School of Medicine in St. Louis, who co-moderated the workshop.
But patient portals can give clinicians another tool to deliver care beyond conventional office visits or telemedicine appointments, Dr. Schmidt said.
Clinicians can bill insurance if their response to a patient question takes longer than 5 minutes to compose. Responses to messages related to scheduling appointments, refilling prescriptions, or visit follow-ups are not billable.
Some participants at the session said their employers do not have policies that allow compensation for their work in patient portals. Others said their health systems have reported that patients who use portals more frequently have higher satisfaction scores.
Asynchronous care holds promise for extending care beyond traditional constraints, according to Stephen Fuest, MD, an assistant professor of internal medicine at the University of Colorado Anschutz Medical Campus in Aurora, Colorado, and a co-moderator of the workshop.
“By capitalizing on our experiences in designing and implementing systems for portal communication, we can find ways to optimize productivity and alleviate burnout,” Dr. Fuest said.
Dr. Fuest noted that while compensation rates for virtual care are lower than those for in-person, the lack of geographical barriers and time constraints allow clinicians to care for more patients. Asynchronous care also can limit losing patients to follow-up.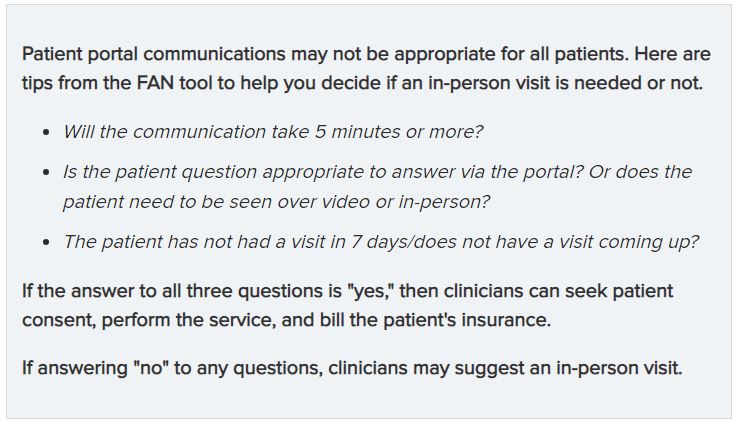
One participant noted that the use of the patient portal may increase disparities in care among non-English speaking patients who are unable to interpret communications or clinician notes.
Still, Dr. Schmidt said that asynchronous care is only as successful as the trust and rapport built between the clinician and the patient.
“Asynchronous care isn’t just a technological advancement, it’s a testament to the commitment to patient-centric care,” she said. “By embracing innovation responsibly, we’re ushering healthcare delivery characterized by efficiency, empathy, and empowerment.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Online patient portals have shifted patient expectations of how quickly clinicians respond and provide timely care, which can lead to burnout. But asynchronous care can, in some cases, be compensated and increase physician productivity and enhance patient care, according to experts who led a workshop at the Society of General Internal Medicine (SGIM) 2024 Annual Meeting.
Patient portal visits have increased in popularity and use since the COVID-19 pandemic. For primary care clinicians especially, the amount of time spent and the span of requests, from messages with new health concerns to requests for prescription refills, can be daunting.
“Understanding the nuances of these relationships is pivotal in navigating the evolution toward asynchronous care,” said Jennifer Schmidt, MD, an assistant professor of medicine at the Washington University School of Medicine in St. Louis, who co-moderated the workshop.
But patient portals can give clinicians another tool to deliver care beyond conventional office visits or telemedicine appointments, Dr. Schmidt said.
Clinicians can bill insurance if their response to a patient question takes longer than 5 minutes to compose. Responses to messages related to scheduling appointments, refilling prescriptions, or visit follow-ups are not billable.
Some participants at the session said their employers do not have policies that allow compensation for their work in patient portals. Others said their health systems have reported that patients who use portals more frequently have higher satisfaction scores.
Asynchronous care holds promise for extending care beyond traditional constraints, according to Stephen Fuest, MD, an assistant professor of internal medicine at the University of Colorado Anschutz Medical Campus in Aurora, Colorado, and a co-moderator of the workshop.
“By capitalizing on our experiences in designing and implementing systems for portal communication, we can find ways to optimize productivity and alleviate burnout,” Dr. Fuest said.
Dr. Fuest noted that while compensation rates for virtual care are lower than those for in-person, the lack of geographical barriers and time constraints allow clinicians to care for more patients. Asynchronous care also can limit losing patients to follow-up.
One participant noted that the use of the patient portal may increase disparities in care among non-English speaking patients who are unable to interpret communications or clinician notes.
Still, Dr. Schmidt said that asynchronous care is only as successful as the trust and rapport built between the clinician and the patient.
“Asynchronous care isn’t just a technological advancement, it’s a testament to the commitment to patient-centric care,” she said. “By embracing innovation responsibly, we’re ushering healthcare delivery characterized by efficiency, empathy, and empowerment.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Online patient portals have shifted patient expectations of how quickly clinicians respond and provide timely care, which can lead to burnout. But asynchronous care can, in some cases, be compensated and increase physician productivity and enhance patient care, according to experts who led a workshop at the Society of General Internal Medicine (SGIM) 2024 Annual Meeting.
Patient portal visits have increased in popularity and use since the COVID-19 pandemic. For primary care clinicians especially, the amount of time spent and the span of requests, from messages with new health concerns to requests for prescription refills, can be daunting.
“Understanding the nuances of these relationships is pivotal in navigating the evolution toward asynchronous care,” said Jennifer Schmidt, MD, an assistant professor of medicine at the Washington University School of Medicine in St. Louis, who co-moderated the workshop.
But patient portals can give clinicians another tool to deliver care beyond conventional office visits or telemedicine appointments, Dr. Schmidt said.
Clinicians can bill insurance if their response to a patient question takes longer than 5 minutes to compose. Responses to messages related to scheduling appointments, refilling prescriptions, or visit follow-ups are not billable.
Some participants at the session said their employers do not have policies that allow compensation for their work in patient portals. Others said their health systems have reported that patients who use portals more frequently have higher satisfaction scores.
Asynchronous care holds promise for extending care beyond traditional constraints, according to Stephen Fuest, MD, an assistant professor of internal medicine at the University of Colorado Anschutz Medical Campus in Aurora, Colorado, and a co-moderator of the workshop.
“By capitalizing on our experiences in designing and implementing systems for portal communication, we can find ways to optimize productivity and alleviate burnout,” Dr. Fuest said.
Dr. Fuest noted that while compensation rates for virtual care are lower than those for in-person, the lack of geographical barriers and time constraints allow clinicians to care for more patients. Asynchronous care also can limit losing patients to follow-up.
One participant noted that the use of the patient portal may increase disparities in care among non-English speaking patients who are unable to interpret communications or clinician notes.
Still, Dr. Schmidt said that asynchronous care is only as successful as the trust and rapport built between the clinician and the patient.
“Asynchronous care isn’t just a technological advancement, it’s a testament to the commitment to patient-centric care,” she said. “By embracing innovation responsibly, we’re ushering healthcare delivery characterized by efficiency, empathy, and empowerment.”
The moderators reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
More Cases of Acute Diverticulitis Treated Outside Hospital
BOSTON — Patients with acute colonic diverticulitis are more likely to be seen by primary care providers than by emergency physicians, representing a shift in the way clinicians detect and treat the condition.
Acute colonic diverticulitis affects roughly 180 per 100,000 people per year in the United States.
CT of the abdomen and pelvis may not be a first-line method to detect diverticulitis in the primary care setting as it has been in emergent care, according to Kaveh Sharzehi, MD, MS, associate professor of medicine in the Division of Gastroenterology and Hepatology at Oregon Health & Science University in Portland.
Indeed, clinical guidelines by multiple physician groups recommend that providers use a more individualized approach to detecting and treating the condition.
“There is still great value in proper and thorough physical history and some adjunct testing,” Dr. Sharzehi told attendees during a presentation on April 20 at the American College of Physicians Internal Medicine Meeting 2024. These two methods can detect the disease up to 65% of the time, Dr. Sharzehi added.
An initial evaluation of a patient with suspected acute diverticulitis should first assess the patient’s history of abdominal pain, fever, and leukocytosis, Dr. Sharzehi said.
A C-reactive protein level > 50 mg/L “almost doubles the odds of having diverticulitis,” Dr. Sharzehi said. Studies also suggest increased levels of procalcitonin and fecal calprotectin can indicate the presence of the condition.
The American Gastroenterological Association (AGA) and the American College of Physicians recommend abdominal CT if clinicians are uncertain of the diagnosis, and to evaluate potential complications in severe cases. Ultrasound and MRI can be useful alternatives, according to guidelines from the American Society of Colon and Rectal Surgeons.
The chances of developing diverticulitis increase with age. More than 60% of Americans aged 60 years or older have diverticulosis, a condition characterized by small pouches in the colon lining that can weaken the colon wall. Less than 5% of people with diverticulosis go on to develop diverticulitis.
“Aspirin and opioid use are also risk factors, likely from their effect on the colonic transit time and causing constipation that might contribute to diverticulitis, but that›s not very well understood,” Dr. Sharzehi said.
Medical management has shifted from predominantly inpatient to predominantly outpatient care, Dr. Sharzehi told attendees
“Unfortunately, there are not that many supportive guidelines for what diet a patient should have in the acute setting of diverticulitis,” he said.
Patients with a mild case may benefit from a clear liquid diet; for some patients, high-fiber diets, regular physical activity, and statins may protect against recurrence.
Current guidelines recommend against prescribing antibiotics for most cases because evidence suggests that diverticulitis is primarily an inflammatory process that can result in small tears in the diverticulum, rather than the disease being a complication of existing tears.
Patients should also not be treated with probiotics or 5-aminosalicylic acid agents, Dr. Sharzehi said.
“My practice is in the Pacific Northwest, where there’s a lot of belief in naturopathic remedies, so we get a lot of questions about supplements and probiotics in preventing diverticulitis,” he said. “We don’t think it does help, and this is unanimous among all the main [physician] societies.”
The AGA recommends referring patients for a colonoscopy within a year after diverticulitis symptoms have resided.
Severe or unresolved cases could require inpatient procedures such as percutaneous drainage or surgery. An estimated 15%-30% of patients admitted to hospital with acute diverticulitis require surgery, Dr. Sharzehi said.
Surgery may become an option for patients who have recurrent cases of the disease, even if not severe, Dr. Sharzehi said.
Dr. Sharzehi reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Patients with acute colonic diverticulitis are more likely to be seen by primary care providers than by emergency physicians, representing a shift in the way clinicians detect and treat the condition.
Acute colonic diverticulitis affects roughly 180 per 100,000 people per year in the United States.
CT of the abdomen and pelvis may not be a first-line method to detect diverticulitis in the primary care setting as it has been in emergent care, according to Kaveh Sharzehi, MD, MS, associate professor of medicine in the Division of Gastroenterology and Hepatology at Oregon Health & Science University in Portland.
Indeed, clinical guidelines by multiple physician groups recommend that providers use a more individualized approach to detecting and treating the condition.
“There is still great value in proper and thorough physical history and some adjunct testing,” Dr. Sharzehi told attendees during a presentation on April 20 at the American College of Physicians Internal Medicine Meeting 2024. These two methods can detect the disease up to 65% of the time, Dr. Sharzehi added.
An initial evaluation of a patient with suspected acute diverticulitis should first assess the patient’s history of abdominal pain, fever, and leukocytosis, Dr. Sharzehi said.
A C-reactive protein level > 50 mg/L “almost doubles the odds of having diverticulitis,” Dr. Sharzehi said. Studies also suggest increased levels of procalcitonin and fecal calprotectin can indicate the presence of the condition.
The American Gastroenterological Association (AGA) and the American College of Physicians recommend abdominal CT if clinicians are uncertain of the diagnosis, and to evaluate potential complications in severe cases. Ultrasound and MRI can be useful alternatives, according to guidelines from the American Society of Colon and Rectal Surgeons.
The chances of developing diverticulitis increase with age. More than 60% of Americans aged 60 years or older have diverticulosis, a condition characterized by small pouches in the colon lining that can weaken the colon wall. Less than 5% of people with diverticulosis go on to develop diverticulitis.
“Aspirin and opioid use are also risk factors, likely from their effect on the colonic transit time and causing constipation that might contribute to diverticulitis, but that›s not very well understood,” Dr. Sharzehi said.
Medical management has shifted from predominantly inpatient to predominantly outpatient care, Dr. Sharzehi told attendees
“Unfortunately, there are not that many supportive guidelines for what diet a patient should have in the acute setting of diverticulitis,” he said.
Patients with a mild case may benefit from a clear liquid diet; for some patients, high-fiber diets, regular physical activity, and statins may protect against recurrence.
Current guidelines recommend against prescribing antibiotics for most cases because evidence suggests that diverticulitis is primarily an inflammatory process that can result in small tears in the diverticulum, rather than the disease being a complication of existing tears.
Patients should also not be treated with probiotics or 5-aminosalicylic acid agents, Dr. Sharzehi said.
“My practice is in the Pacific Northwest, where there’s a lot of belief in naturopathic remedies, so we get a lot of questions about supplements and probiotics in preventing diverticulitis,” he said. “We don’t think it does help, and this is unanimous among all the main [physician] societies.”
The AGA recommends referring patients for a colonoscopy within a year after diverticulitis symptoms have resided.
Severe or unresolved cases could require inpatient procedures such as percutaneous drainage or surgery. An estimated 15%-30% of patients admitted to hospital with acute diverticulitis require surgery, Dr. Sharzehi said.
Surgery may become an option for patients who have recurrent cases of the disease, even if not severe, Dr. Sharzehi said.
Dr. Sharzehi reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
BOSTON — Patients with acute colonic diverticulitis are more likely to be seen by primary care providers than by emergency physicians, representing a shift in the way clinicians detect and treat the condition.
Acute colonic diverticulitis affects roughly 180 per 100,000 people per year in the United States.
CT of the abdomen and pelvis may not be a first-line method to detect diverticulitis in the primary care setting as it has been in emergent care, according to Kaveh Sharzehi, MD, MS, associate professor of medicine in the Division of Gastroenterology and Hepatology at Oregon Health & Science University in Portland.
Indeed, clinical guidelines by multiple physician groups recommend that providers use a more individualized approach to detecting and treating the condition.
“There is still great value in proper and thorough physical history and some adjunct testing,” Dr. Sharzehi told attendees during a presentation on April 20 at the American College of Physicians Internal Medicine Meeting 2024. These two methods can detect the disease up to 65% of the time, Dr. Sharzehi added.
An initial evaluation of a patient with suspected acute diverticulitis should first assess the patient’s history of abdominal pain, fever, and leukocytosis, Dr. Sharzehi said.
A C-reactive protein level > 50 mg/L “almost doubles the odds of having diverticulitis,” Dr. Sharzehi said. Studies also suggest increased levels of procalcitonin and fecal calprotectin can indicate the presence of the condition.
The American Gastroenterological Association (AGA) and the American College of Physicians recommend abdominal CT if clinicians are uncertain of the diagnosis, and to evaluate potential complications in severe cases. Ultrasound and MRI can be useful alternatives, according to guidelines from the American Society of Colon and Rectal Surgeons.
The chances of developing diverticulitis increase with age. More than 60% of Americans aged 60 years or older have diverticulosis, a condition characterized by small pouches in the colon lining that can weaken the colon wall. Less than 5% of people with diverticulosis go on to develop diverticulitis.
“Aspirin and opioid use are also risk factors, likely from their effect on the colonic transit time and causing constipation that might contribute to diverticulitis, but that›s not very well understood,” Dr. Sharzehi said.
Medical management has shifted from predominantly inpatient to predominantly outpatient care, Dr. Sharzehi told attendees
“Unfortunately, there are not that many supportive guidelines for what diet a patient should have in the acute setting of diverticulitis,” he said.
Patients with a mild case may benefit from a clear liquid diet; for some patients, high-fiber diets, regular physical activity, and statins may protect against recurrence.
Current guidelines recommend against prescribing antibiotics for most cases because evidence suggests that diverticulitis is primarily an inflammatory process that can result in small tears in the diverticulum, rather than the disease being a complication of existing tears.
Patients should also not be treated with probiotics or 5-aminosalicylic acid agents, Dr. Sharzehi said.
“My practice is in the Pacific Northwest, where there’s a lot of belief in naturopathic remedies, so we get a lot of questions about supplements and probiotics in preventing diverticulitis,” he said. “We don’t think it does help, and this is unanimous among all the main [physician] societies.”
The AGA recommends referring patients for a colonoscopy within a year after diverticulitis symptoms have resided.
Severe or unresolved cases could require inpatient procedures such as percutaneous drainage or surgery. An estimated 15%-30% of patients admitted to hospital with acute diverticulitis require surgery, Dr. Sharzehi said.
Surgery may become an option for patients who have recurrent cases of the disease, even if not severe, Dr. Sharzehi said.
Dr. Sharzehi reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
Menopause, RSV, and More: 4 New Meds to Know
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.