User login
SHM Opposes Bill Eliminating Key Federal Agency
SHM recently joined more than 135 organizations in opposing legislation that would eliminate funding for the Agency for Health Care Research and Quality (AHRQ), according to a July 30 letter. Language terminating the agency was part of a fiscal-year 2013 spending bill approved July 18 by the Republican-controlled Senate Subcommittee on Labor, Health and Human Services, Education, and Related Agencies.
Organized by the Friends of AHRQ Coalition, the letter calls on members of Congress to oppose any bill that terminates the agency and its important research.
“To ‘terminate’ AHRQ in the current fiscal environment is penny-wise and pound-foolish,” the letter states. “AHRQ-funded research is being used in hospitals, private practices, health departments, and communities across the nation to fuel innovation and improve quality, identify waste, and enhance efficiency of the healthcare system. … This research helps Americans get their money’s worth when it comes to healthcare. We need more of it, not less.”
A longtime supporter of AHRQ and its efforts to improve quality and patient safety, SHM is deeply concerned about efforts to eliminate this important agency and will fight to preserve its funding. A markup by the full committee has been postponed indefinitely.
The spending bill approved by the subcommittee also prohibits any patient-centered-outcomes research and all economic research within the National Institutes of Health (NIH). It freezes funding for NIH and rescinds the $1 billion available in 2013 under the Prevention and Public Health Fund. It also rescinds $1.6 billion for the Center for Medicare & Medicaid Innovation (CMMI) and blocks other funding for and implementation of the Affordable Care Act.
Laura Allendorf, SHM senior advisor, advocacy and government affairs
SHM recently joined more than 135 organizations in opposing legislation that would eliminate funding for the Agency for Health Care Research and Quality (AHRQ), according to a July 30 letter. Language terminating the agency was part of a fiscal-year 2013 spending bill approved July 18 by the Republican-controlled Senate Subcommittee on Labor, Health and Human Services, Education, and Related Agencies.
Organized by the Friends of AHRQ Coalition, the letter calls on members of Congress to oppose any bill that terminates the agency and its important research.
“To ‘terminate’ AHRQ in the current fiscal environment is penny-wise and pound-foolish,” the letter states. “AHRQ-funded research is being used in hospitals, private practices, health departments, and communities across the nation to fuel innovation and improve quality, identify waste, and enhance efficiency of the healthcare system. … This research helps Americans get their money’s worth when it comes to healthcare. We need more of it, not less.”
A longtime supporter of AHRQ and its efforts to improve quality and patient safety, SHM is deeply concerned about efforts to eliminate this important agency and will fight to preserve its funding. A markup by the full committee has been postponed indefinitely.
The spending bill approved by the subcommittee also prohibits any patient-centered-outcomes research and all economic research within the National Institutes of Health (NIH). It freezes funding for NIH and rescinds the $1 billion available in 2013 under the Prevention and Public Health Fund. It also rescinds $1.6 billion for the Center for Medicare & Medicaid Innovation (CMMI) and blocks other funding for and implementation of the Affordable Care Act.
Laura Allendorf, SHM senior advisor, advocacy and government affairs
SHM recently joined more than 135 organizations in opposing legislation that would eliminate funding for the Agency for Health Care Research and Quality (AHRQ), according to a July 30 letter. Language terminating the agency was part of a fiscal-year 2013 spending bill approved July 18 by the Republican-controlled Senate Subcommittee on Labor, Health and Human Services, Education, and Related Agencies.
Organized by the Friends of AHRQ Coalition, the letter calls on members of Congress to oppose any bill that terminates the agency and its important research.
“To ‘terminate’ AHRQ in the current fiscal environment is penny-wise and pound-foolish,” the letter states. “AHRQ-funded research is being used in hospitals, private practices, health departments, and communities across the nation to fuel innovation and improve quality, identify waste, and enhance efficiency of the healthcare system. … This research helps Americans get their money’s worth when it comes to healthcare. We need more of it, not less.”
A longtime supporter of AHRQ and its efforts to improve quality and patient safety, SHM is deeply concerned about efforts to eliminate this important agency and will fight to preserve its funding. A markup by the full committee has been postponed indefinitely.
The spending bill approved by the subcommittee also prohibits any patient-centered-outcomes research and all economic research within the National Institutes of Health (NIH). It freezes funding for NIH and rescinds the $1 billion available in 2013 under the Prevention and Public Health Fund. It also rescinds $1.6 billion for the Center for Medicare & Medicaid Innovation (CMMI) and blocks other funding for and implementation of the Affordable Care Act.
Laura Allendorf, SHM senior advisor, advocacy and government affairs
At Work in Washington

SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at lallendorf@hospitalmedicine.org.
SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at lallendorf@hospitalmedicine.org.
SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at lallendorf@hospitalmedicine.org.
Mission in D.C.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana

Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana
Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana
Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
Physician Payment Reform, P4P, AHRQ
SHM’s Public Policy Committee (PPC) monitors federal legislation and regulations affecting hospital medicine and recommending appropriate action by SHM. SHM works independently and through coalitions with like-minded organizations in pursuit of its policy objectives. This month, I’ll update you on PPC’s major activities in the past six months.
Physician Payment Reform
Late last year, as Congress debated whether to address pending reductions in 2007 Medicare payments to physicians before adjourning, PPC spearheaded a number of activities to influence debate on the issue. These efforts included:
- Sending a letter from then-SHM President Mary Jo Gorman, MD, MBA, to members of the key health committees, urging lawmakers to take action to avert the scheduled 5% cut in Medicare physician fees and enact a positive payment update that accurately reflects increases in practice costs;
- Launching a new advocacy tool that allows SHM members to quickly e-mail their members of Congress in opposition to the pending fee cut. In less than two weeks, 130 members sent nearly 390 messages to the U.S. House of Representatives and the Senate; and
- Lobbying Congress to ensure that any pay-for-reporting program for physicians be voluntary and based on valid measures developed by the medical profession.
The legislation approved by Congress (H.R. 6111) averted the 5% cut, as advocated by SHM, freezing rates at 2006 levels. Continuation of the current payment rates, combined with increases in evaluation and management services proposed by CMS and supported by SHM as part of the five-year review, translated into an average gain per hospitalist of approximately 8.8% on their Medicare billings.
A scheduled 10% cut in 2008 Medicare payments to physicians will dominate this year’s legislative agenda. The PPC will continue to oppose cuts in the physician update and advocate for a more permanent solution to the annual payment reductions caused by the flawed sustainable growth rate.
Pay for Performance
Together with SHM’s Performance and Standards Task Force (PSTF), the PPC has spent countless hours working to position SHM to influence the debate over pay for performance on Capitol Hill and with CMS. This has involved Hill visits by PPC members and staff in addition to conference calls, meetings, and communications with CMS officials. Part of the committee’s role is also to educate SHM members on how their practices will be affected by legislative and regulatory action in this area.
Under the new Physician Quality Reporting Initiative (PQRI) mandated under H.R. 6111, SHM members and other eligible professionals who successfully report quality measures on claims for dates of service from July 1 to Dec. 31 may earn a bonus payment, subject to a cap, of 1.5% of total allowed charges for covered Medicare physician fee schedule services.
Because measures were not originally developed for hospital medicine, PPC, PSTF, and staff actively lobbied CMS and the AMA’s Physician Consortium for Performance Improvement (PCPI) for changes to the measures that would allow wider reporting by SHM members. Significantly, PCPI accepted SHM’s recommendations, paving the way for hospitalist participation in this voluntary program. Had SHM not been at the table, hospitalists would have had only a limited opportunity to qualify for a 1.5% increase in their Medicare payments through participation in the PQRI program. SHM will also take the lead in developing measures on care transitions through the PCPI for 2009, which will position hospital medicine as the premier advocate for this important issue.
Funding for AHRQ
One of SHM’s legislative priorities is to advocate for increased funding for the Agency for Healthcare Research and Quality (AHRQ), whose mission is to improve the quality, safety, efficiency, and effectiveness of healthcare for all Americans. As part of this effort, we participate in the Friends of AHRQ, a voluntary coalition of more than 130 organizations that supports the AHRQ by sending joint letters to key members of Congress, making joint visits to members of Congress and their staff, and holding briefings to demonstrate the importance of AHRQ research.
In March, SHM and 50 other members of the coalition sent a letter to the chairs and ranking members of the House and Senate Appropriations committees recommending that AHRQ receive $350 million in FY 2008, an increase of $31 million over FY 2007. The groups pointed out that while AHRQ is charged with supporting research to improve healthcare quality, reduce costs, advance patient safety, decrease medical errors, eliminate healthcare disparities, and broaden access to essential services, “precarious funding levels threaten the agency’s ability to achieve this important mission, at a time when healthcare costs are at an all-time high.”
Funding for NIH and Other Agencies
SHM also routinely joins with other organizations in urging Congress to increase funding for the National Institutes of Health (NIH) and other public health programs.
A Feb. 26 letter, signed by SHM and 405 other health organizations, urged Congress to increase FY 2008 funding for public health programs by an additional $4 billion, or 7.8%, above the FY 2007 level. The letter states that this increase in the FY 2008 budget for Function 550 discretionary health programs such as NIH, AHRQ, and CDC will “reverse the erosion of support for the continuum of biomedical, behavioral and health services research, community-based disease prevention and health promotion, basic and targeted services for the medically uninsured and those with disabilities, health professions education, and robust regulation of the nation’s food and drug supply.”
Access to Care
Recognizing SHM member interest—and that of the 110th Congress—in initiatives to expand healthcare coverage to the nation’s 47 million uninsured, the PPC is reviewing legislative proposals being considered in this area.
At the committee’s recommendation, SHM sent a letter of support for the Health Partnership Act (S. 325/H.R. 506), which would establish a grant program to promote the development of innovative health coverage initiatives at the state level. In the letter, then-SHM President Mary Jo Gorman, MD, MBA, commended the sponsors for “giving state and local governments the flexibility to test a variety of options for improving access so they can address the unique needs of their uninsured populations.”
She noted that many hospitalist programs exist to manage the burgeoning population of uninsured and underinsured patients who require hospitalization, and offered SHM’s help in moving the bill through Congress.
Grass-roots Advocacy
Politically active members are an organization’s best resource when it comes to influencing healthcare policy on Capitol Hill. Building on the relationships established during SHM’s first Advocacy Day held during the 2006 annual meeting, PPC members traveled to Washington D.C., in February to brief members of Congress and their staffs on SHM’s 2007 legislative priorities, including support for initiatives designed to improve the quality, safety, and cost effectiveness of inpatient medical care.
More than 30 appointments were scheduled with lawmakers and their staffs, many of whom sit on the key congressional committees with jurisdiction over the Medicare and Medicaid programs. Each PPC member had from five to eight visits. They continued the process of educating Congress about the specialty of hospital medicine that began during Advocacy Day and the role of hospitalists in improving the quality of care provided in our nation’s hospitals. It was time well spent. Lawmakers and their staffs were eager to learn about hospital medicine and our support for increased funding for AHRQ, pay-for-reporting, and legislation like the Health Partnership Act.
Allendorf is senior adviser, advocacy and government relations, for SHM.
New Task Force, New Chair, Improved Patient Care
SHM’s HQPS Committee makes tremendous progress
By Shannon Roach
The past year has been successful and productive for the SHM Health Quality and Patient Safety (HQPS) Committee. Under the leadership of Lakshmi Halasyamani, MD, HQPS has strengthened its national leadership role in inpatient quality improvement efforts, most notably in the areas of reducing DVTs, improving glycemic control and management of patients with heart failure. Additionally, HQPS has strengthened relationships with partner organizations and created new alliances. HQPS has participated in the development of training activities and clinical support tools for quality improvement efforts.
Hand-Off Standards
The Hand-Off Standards and Communication Task Force was formed to create a formally recognized set of standards for ensuring optimum communication and continuity of care at the end of a medical professional’s shift or a patient’s change in service. The standards ensure that care is coordinated and that important clinical care issues are effectively managed. The development methodology mirrors that of the Discharge Planning Checklist and includes a literature review, panel of experts, presentation to and input from membership. Vineet Arora, MD, has led this development in collaboration with Sunil Kripalani, MD, Efren Manjarrez, MD, Dan Dressler, MD, Preetha Basaviah, MD, and Lakshmi Halasyamani, MD.
The Hand-Off Standards checklist was unveiled at the 2007 Annual Meeting from May 23-25 in Dallas, where attendees reviewed and voted on the standards in order to provide the Task Force with a final draft to present to the Expert Panel for a final review. Effective hand-offs require program policy, verbal exchange, and content exchange. A research agenda was also proposed to evaluate these standards rigorously, put emphasis on controlled interventions, and to encourage SHM and other organizations to fund research and innovations in this area.
Medication Reconciliation
The Medication Reconciliation Task Force is charged with understanding the state of and leading work related to Medication Reconciliation. In support of that, the Task Force submitted a grant proposal to AHRQ to provide funding for a multidisciplinary conference to identify barriers and develop strategies for Quality Improvement in this area.
Heart Failure
Dr. Halasyamani, former HQPS chair, was a key participant in the development of the Heart Failure Resource Room, which launched in February 2006. As part of the Heart Failure Education and Quality Improvement Initiative, there have been both clinical tools and CME/CE additions to this Web-based resource (visit www.hospitalmedicine.org and click “Quality & Safety” then click “Quality Improvement Resource Rooms”). The Quality Improvement Workbook, the Palliative Care CME Module, and Didactic Slide Sets are all housed in the Resource Room along with the recently developed Clinical Tools focusing on Team Communication, Discharge Planning and Polypharmacy.
The Tools include an Inpatient Goal Sheet, a Hospitalist Admission and Daily Rounding Checklist, a Conceptual Model for Teamwork, two reference guides: Patient Education and High Risk Medications for the Heart Failure Patient, and Heart Failure, specific elements of which were integrated into the SHM Discharge Planning Checklist.
Additional CME/CE modules have also been integrated into the Heart Failure Resource Room: Palliative Care for Patients with Heart Failure and Optimizing the Heart Failure Discharge Transition.
A CD-ROM including all these new resources was given to attendees of the Annual Meeting.
Building Partnerships
HQPS has been strengthening partnerships with other professional, regulatory and advocacy groups. These partnerships are intended to improve safety and take a leadership role in setting the national agenda for key quality improvement areas. We now have official liaisons with Academy of Health-System Pharmacists (AHSP), National Transitions of Care Coalition (NTOCC), Institute for Healthcare Improvement (IHI), and Transforming Care at the Bedside (TCAB).
HQPS members also serve as leaders in national efforts to define and improve care transitions including the American Board of Internal Medicine’s Stepping up to the Plate program, and Hartford’s Safe Steps.
SHM’s Public Policy Committee (PPC) monitors federal legislation and regulations affecting hospital medicine and recommending appropriate action by SHM. SHM works independently and through coalitions with like-minded organizations in pursuit of its policy objectives. This month, I’ll update you on PPC’s major activities in the past six months.
Physician Payment Reform
Late last year, as Congress debated whether to address pending reductions in 2007 Medicare payments to physicians before adjourning, PPC spearheaded a number of activities to influence debate on the issue. These efforts included:
- Sending a letter from then-SHM President Mary Jo Gorman, MD, MBA, to members of the key health committees, urging lawmakers to take action to avert the scheduled 5% cut in Medicare physician fees and enact a positive payment update that accurately reflects increases in practice costs;
- Launching a new advocacy tool that allows SHM members to quickly e-mail their members of Congress in opposition to the pending fee cut. In less than two weeks, 130 members sent nearly 390 messages to the U.S. House of Representatives and the Senate; and
- Lobbying Congress to ensure that any pay-for-reporting program for physicians be voluntary and based on valid measures developed by the medical profession.
The legislation approved by Congress (H.R. 6111) averted the 5% cut, as advocated by SHM, freezing rates at 2006 levels. Continuation of the current payment rates, combined with increases in evaluation and management services proposed by CMS and supported by SHM as part of the five-year review, translated into an average gain per hospitalist of approximately 8.8% on their Medicare billings.
A scheduled 10% cut in 2008 Medicare payments to physicians will dominate this year’s legislative agenda. The PPC will continue to oppose cuts in the physician update and advocate for a more permanent solution to the annual payment reductions caused by the flawed sustainable growth rate.
Pay for Performance
Together with SHM’s Performance and Standards Task Force (PSTF), the PPC has spent countless hours working to position SHM to influence the debate over pay for performance on Capitol Hill and with CMS. This has involved Hill visits by PPC members and staff in addition to conference calls, meetings, and communications with CMS officials. Part of the committee’s role is also to educate SHM members on how their practices will be affected by legislative and regulatory action in this area.
Under the new Physician Quality Reporting Initiative (PQRI) mandated under H.R. 6111, SHM members and other eligible professionals who successfully report quality measures on claims for dates of service from July 1 to Dec. 31 may earn a bonus payment, subject to a cap, of 1.5% of total allowed charges for covered Medicare physician fee schedule services.
Because measures were not originally developed for hospital medicine, PPC, PSTF, and staff actively lobbied CMS and the AMA’s Physician Consortium for Performance Improvement (PCPI) for changes to the measures that would allow wider reporting by SHM members. Significantly, PCPI accepted SHM’s recommendations, paving the way for hospitalist participation in this voluntary program. Had SHM not been at the table, hospitalists would have had only a limited opportunity to qualify for a 1.5% increase in their Medicare payments through participation in the PQRI program. SHM will also take the lead in developing measures on care transitions through the PCPI for 2009, which will position hospital medicine as the premier advocate for this important issue.
Funding for AHRQ
One of SHM’s legislative priorities is to advocate for increased funding for the Agency for Healthcare Research and Quality (AHRQ), whose mission is to improve the quality, safety, efficiency, and effectiveness of healthcare for all Americans. As part of this effort, we participate in the Friends of AHRQ, a voluntary coalition of more than 130 organizations that supports the AHRQ by sending joint letters to key members of Congress, making joint visits to members of Congress and their staff, and holding briefings to demonstrate the importance of AHRQ research.
In March, SHM and 50 other members of the coalition sent a letter to the chairs and ranking members of the House and Senate Appropriations committees recommending that AHRQ receive $350 million in FY 2008, an increase of $31 million over FY 2007. The groups pointed out that while AHRQ is charged with supporting research to improve healthcare quality, reduce costs, advance patient safety, decrease medical errors, eliminate healthcare disparities, and broaden access to essential services, “precarious funding levels threaten the agency’s ability to achieve this important mission, at a time when healthcare costs are at an all-time high.”
Funding for NIH and Other Agencies
SHM also routinely joins with other organizations in urging Congress to increase funding for the National Institutes of Health (NIH) and other public health programs.
A Feb. 26 letter, signed by SHM and 405 other health organizations, urged Congress to increase FY 2008 funding for public health programs by an additional $4 billion, or 7.8%, above the FY 2007 level. The letter states that this increase in the FY 2008 budget for Function 550 discretionary health programs such as NIH, AHRQ, and CDC will “reverse the erosion of support for the continuum of biomedical, behavioral and health services research, community-based disease prevention and health promotion, basic and targeted services for the medically uninsured and those with disabilities, health professions education, and robust regulation of the nation’s food and drug supply.”
Access to Care
Recognizing SHM member interest—and that of the 110th Congress—in initiatives to expand healthcare coverage to the nation’s 47 million uninsured, the PPC is reviewing legislative proposals being considered in this area.
At the committee’s recommendation, SHM sent a letter of support for the Health Partnership Act (S. 325/H.R. 506), which would establish a grant program to promote the development of innovative health coverage initiatives at the state level. In the letter, then-SHM President Mary Jo Gorman, MD, MBA, commended the sponsors for “giving state and local governments the flexibility to test a variety of options for improving access so they can address the unique needs of their uninsured populations.”
She noted that many hospitalist programs exist to manage the burgeoning population of uninsured and underinsured patients who require hospitalization, and offered SHM’s help in moving the bill through Congress.
Grass-roots Advocacy
Politically active members are an organization’s best resource when it comes to influencing healthcare policy on Capitol Hill. Building on the relationships established during SHM’s first Advocacy Day held during the 2006 annual meeting, PPC members traveled to Washington D.C., in February to brief members of Congress and their staffs on SHM’s 2007 legislative priorities, including support for initiatives designed to improve the quality, safety, and cost effectiveness of inpatient medical care.
More than 30 appointments were scheduled with lawmakers and their staffs, many of whom sit on the key congressional committees with jurisdiction over the Medicare and Medicaid programs. Each PPC member had from five to eight visits. They continued the process of educating Congress about the specialty of hospital medicine that began during Advocacy Day and the role of hospitalists in improving the quality of care provided in our nation’s hospitals. It was time well spent. Lawmakers and their staffs were eager to learn about hospital medicine and our support for increased funding for AHRQ, pay-for-reporting, and legislation like the Health Partnership Act.
Allendorf is senior adviser, advocacy and government relations, for SHM.
New Task Force, New Chair, Improved Patient Care
SHM’s HQPS Committee makes tremendous progress
By Shannon Roach
The past year has been successful and productive for the SHM Health Quality and Patient Safety (HQPS) Committee. Under the leadership of Lakshmi Halasyamani, MD, HQPS has strengthened its national leadership role in inpatient quality improvement efforts, most notably in the areas of reducing DVTs, improving glycemic control and management of patients with heart failure. Additionally, HQPS has strengthened relationships with partner organizations and created new alliances. HQPS has participated in the development of training activities and clinical support tools for quality improvement efforts.
Hand-Off Standards
The Hand-Off Standards and Communication Task Force was formed to create a formally recognized set of standards for ensuring optimum communication and continuity of care at the end of a medical professional’s shift or a patient’s change in service. The standards ensure that care is coordinated and that important clinical care issues are effectively managed. The development methodology mirrors that of the Discharge Planning Checklist and includes a literature review, panel of experts, presentation to and input from membership. Vineet Arora, MD, has led this development in collaboration with Sunil Kripalani, MD, Efren Manjarrez, MD, Dan Dressler, MD, Preetha Basaviah, MD, and Lakshmi Halasyamani, MD.
The Hand-Off Standards checklist was unveiled at the 2007 Annual Meeting from May 23-25 in Dallas, where attendees reviewed and voted on the standards in order to provide the Task Force with a final draft to present to the Expert Panel for a final review. Effective hand-offs require program policy, verbal exchange, and content exchange. A research agenda was also proposed to evaluate these standards rigorously, put emphasis on controlled interventions, and to encourage SHM and other organizations to fund research and innovations in this area.
Medication Reconciliation
The Medication Reconciliation Task Force is charged with understanding the state of and leading work related to Medication Reconciliation. In support of that, the Task Force submitted a grant proposal to AHRQ to provide funding for a multidisciplinary conference to identify barriers and develop strategies for Quality Improvement in this area.
Heart Failure
Dr. Halasyamani, former HQPS chair, was a key participant in the development of the Heart Failure Resource Room, which launched in February 2006. As part of the Heart Failure Education and Quality Improvement Initiative, there have been both clinical tools and CME/CE additions to this Web-based resource (visit www.hospitalmedicine.org and click “Quality & Safety” then click “Quality Improvement Resource Rooms”). The Quality Improvement Workbook, the Palliative Care CME Module, and Didactic Slide Sets are all housed in the Resource Room along with the recently developed Clinical Tools focusing on Team Communication, Discharge Planning and Polypharmacy.
The Tools include an Inpatient Goal Sheet, a Hospitalist Admission and Daily Rounding Checklist, a Conceptual Model for Teamwork, two reference guides: Patient Education and High Risk Medications for the Heart Failure Patient, and Heart Failure, specific elements of which were integrated into the SHM Discharge Planning Checklist.
Additional CME/CE modules have also been integrated into the Heart Failure Resource Room: Palliative Care for Patients with Heart Failure and Optimizing the Heart Failure Discharge Transition.
A CD-ROM including all these new resources was given to attendees of the Annual Meeting.
Building Partnerships
HQPS has been strengthening partnerships with other professional, regulatory and advocacy groups. These partnerships are intended to improve safety and take a leadership role in setting the national agenda for key quality improvement areas. We now have official liaisons with Academy of Health-System Pharmacists (AHSP), National Transitions of Care Coalition (NTOCC), Institute for Healthcare Improvement (IHI), and Transforming Care at the Bedside (TCAB).
HQPS members also serve as leaders in national efforts to define and improve care transitions including the American Board of Internal Medicine’s Stepping up to the Plate program, and Hartford’s Safe Steps.
SHM’s Public Policy Committee (PPC) monitors federal legislation and regulations affecting hospital medicine and recommending appropriate action by SHM. SHM works independently and through coalitions with like-minded organizations in pursuit of its policy objectives. This month, I’ll update you on PPC’s major activities in the past six months.
Physician Payment Reform
Late last year, as Congress debated whether to address pending reductions in 2007 Medicare payments to physicians before adjourning, PPC spearheaded a number of activities to influence debate on the issue. These efforts included:
- Sending a letter from then-SHM President Mary Jo Gorman, MD, MBA, to members of the key health committees, urging lawmakers to take action to avert the scheduled 5% cut in Medicare physician fees and enact a positive payment update that accurately reflects increases in practice costs;
- Launching a new advocacy tool that allows SHM members to quickly e-mail their members of Congress in opposition to the pending fee cut. In less than two weeks, 130 members sent nearly 390 messages to the U.S. House of Representatives and the Senate; and
- Lobbying Congress to ensure that any pay-for-reporting program for physicians be voluntary and based on valid measures developed by the medical profession.
The legislation approved by Congress (H.R. 6111) averted the 5% cut, as advocated by SHM, freezing rates at 2006 levels. Continuation of the current payment rates, combined with increases in evaluation and management services proposed by CMS and supported by SHM as part of the five-year review, translated into an average gain per hospitalist of approximately 8.8% on their Medicare billings.
A scheduled 10% cut in 2008 Medicare payments to physicians will dominate this year’s legislative agenda. The PPC will continue to oppose cuts in the physician update and advocate for a more permanent solution to the annual payment reductions caused by the flawed sustainable growth rate.
Pay for Performance
Together with SHM’s Performance and Standards Task Force (PSTF), the PPC has spent countless hours working to position SHM to influence the debate over pay for performance on Capitol Hill and with CMS. This has involved Hill visits by PPC members and staff in addition to conference calls, meetings, and communications with CMS officials. Part of the committee’s role is also to educate SHM members on how their practices will be affected by legislative and regulatory action in this area.
Under the new Physician Quality Reporting Initiative (PQRI) mandated under H.R. 6111, SHM members and other eligible professionals who successfully report quality measures on claims for dates of service from July 1 to Dec. 31 may earn a bonus payment, subject to a cap, of 1.5% of total allowed charges for covered Medicare physician fee schedule services.
Because measures were not originally developed for hospital medicine, PPC, PSTF, and staff actively lobbied CMS and the AMA’s Physician Consortium for Performance Improvement (PCPI) for changes to the measures that would allow wider reporting by SHM members. Significantly, PCPI accepted SHM’s recommendations, paving the way for hospitalist participation in this voluntary program. Had SHM not been at the table, hospitalists would have had only a limited opportunity to qualify for a 1.5% increase in their Medicare payments through participation in the PQRI program. SHM will also take the lead in developing measures on care transitions through the PCPI for 2009, which will position hospital medicine as the premier advocate for this important issue.
Funding for AHRQ
One of SHM’s legislative priorities is to advocate for increased funding for the Agency for Healthcare Research and Quality (AHRQ), whose mission is to improve the quality, safety, efficiency, and effectiveness of healthcare for all Americans. As part of this effort, we participate in the Friends of AHRQ, a voluntary coalition of more than 130 organizations that supports the AHRQ by sending joint letters to key members of Congress, making joint visits to members of Congress and their staff, and holding briefings to demonstrate the importance of AHRQ research.
In March, SHM and 50 other members of the coalition sent a letter to the chairs and ranking members of the House and Senate Appropriations committees recommending that AHRQ receive $350 million in FY 2008, an increase of $31 million over FY 2007. The groups pointed out that while AHRQ is charged with supporting research to improve healthcare quality, reduce costs, advance patient safety, decrease medical errors, eliminate healthcare disparities, and broaden access to essential services, “precarious funding levels threaten the agency’s ability to achieve this important mission, at a time when healthcare costs are at an all-time high.”
Funding for NIH and Other Agencies
SHM also routinely joins with other organizations in urging Congress to increase funding for the National Institutes of Health (NIH) and other public health programs.
A Feb. 26 letter, signed by SHM and 405 other health organizations, urged Congress to increase FY 2008 funding for public health programs by an additional $4 billion, or 7.8%, above the FY 2007 level. The letter states that this increase in the FY 2008 budget for Function 550 discretionary health programs such as NIH, AHRQ, and CDC will “reverse the erosion of support for the continuum of biomedical, behavioral and health services research, community-based disease prevention and health promotion, basic and targeted services for the medically uninsured and those with disabilities, health professions education, and robust regulation of the nation’s food and drug supply.”
Access to Care
Recognizing SHM member interest—and that of the 110th Congress—in initiatives to expand healthcare coverage to the nation’s 47 million uninsured, the PPC is reviewing legislative proposals being considered in this area.
At the committee’s recommendation, SHM sent a letter of support for the Health Partnership Act (S. 325/H.R. 506), which would establish a grant program to promote the development of innovative health coverage initiatives at the state level. In the letter, then-SHM President Mary Jo Gorman, MD, MBA, commended the sponsors for “giving state and local governments the flexibility to test a variety of options for improving access so they can address the unique needs of their uninsured populations.”
She noted that many hospitalist programs exist to manage the burgeoning population of uninsured and underinsured patients who require hospitalization, and offered SHM’s help in moving the bill through Congress.
Grass-roots Advocacy
Politically active members are an organization’s best resource when it comes to influencing healthcare policy on Capitol Hill. Building on the relationships established during SHM’s first Advocacy Day held during the 2006 annual meeting, PPC members traveled to Washington D.C., in February to brief members of Congress and their staffs on SHM’s 2007 legislative priorities, including support for initiatives designed to improve the quality, safety, and cost effectiveness of inpatient medical care.
More than 30 appointments were scheduled with lawmakers and their staffs, many of whom sit on the key congressional committees with jurisdiction over the Medicare and Medicaid programs. Each PPC member had from five to eight visits. They continued the process of educating Congress about the specialty of hospital medicine that began during Advocacy Day and the role of hospitalists in improving the quality of care provided in our nation’s hospitals. It was time well spent. Lawmakers and their staffs were eager to learn about hospital medicine and our support for increased funding for AHRQ, pay-for-reporting, and legislation like the Health Partnership Act.
Allendorf is senior adviser, advocacy and government relations, for SHM.
New Task Force, New Chair, Improved Patient Care
SHM’s HQPS Committee makes tremendous progress
By Shannon Roach
The past year has been successful and productive for the SHM Health Quality and Patient Safety (HQPS) Committee. Under the leadership of Lakshmi Halasyamani, MD, HQPS has strengthened its national leadership role in inpatient quality improvement efforts, most notably in the areas of reducing DVTs, improving glycemic control and management of patients with heart failure. Additionally, HQPS has strengthened relationships with partner organizations and created new alliances. HQPS has participated in the development of training activities and clinical support tools for quality improvement efforts.
Hand-Off Standards
The Hand-Off Standards and Communication Task Force was formed to create a formally recognized set of standards for ensuring optimum communication and continuity of care at the end of a medical professional’s shift or a patient’s change in service. The standards ensure that care is coordinated and that important clinical care issues are effectively managed. The development methodology mirrors that of the Discharge Planning Checklist and includes a literature review, panel of experts, presentation to and input from membership. Vineet Arora, MD, has led this development in collaboration with Sunil Kripalani, MD, Efren Manjarrez, MD, Dan Dressler, MD, Preetha Basaviah, MD, and Lakshmi Halasyamani, MD.
The Hand-Off Standards checklist was unveiled at the 2007 Annual Meeting from May 23-25 in Dallas, where attendees reviewed and voted on the standards in order to provide the Task Force with a final draft to present to the Expert Panel for a final review. Effective hand-offs require program policy, verbal exchange, and content exchange. A research agenda was also proposed to evaluate these standards rigorously, put emphasis on controlled interventions, and to encourage SHM and other organizations to fund research and innovations in this area.
Medication Reconciliation
The Medication Reconciliation Task Force is charged with understanding the state of and leading work related to Medication Reconciliation. In support of that, the Task Force submitted a grant proposal to AHRQ to provide funding for a multidisciplinary conference to identify barriers and develop strategies for Quality Improvement in this area.
Heart Failure
Dr. Halasyamani, former HQPS chair, was a key participant in the development of the Heart Failure Resource Room, which launched in February 2006. As part of the Heart Failure Education and Quality Improvement Initiative, there have been both clinical tools and CME/CE additions to this Web-based resource (visit www.hospitalmedicine.org and click “Quality & Safety” then click “Quality Improvement Resource Rooms”). The Quality Improvement Workbook, the Palliative Care CME Module, and Didactic Slide Sets are all housed in the Resource Room along with the recently developed Clinical Tools focusing on Team Communication, Discharge Planning and Polypharmacy.
The Tools include an Inpatient Goal Sheet, a Hospitalist Admission and Daily Rounding Checklist, a Conceptual Model for Teamwork, two reference guides: Patient Education and High Risk Medications for the Heart Failure Patient, and Heart Failure, specific elements of which were integrated into the SHM Discharge Planning Checklist.
Additional CME/CE modules have also been integrated into the Heart Failure Resource Room: Palliative Care for Patients with Heart Failure and Optimizing the Heart Failure Discharge Transition.
A CD-ROM including all these new resources was given to attendees of the Annual Meeting.
Building Partnerships
HQPS has been strengthening partnerships with other professional, regulatory and advocacy groups. These partnerships are intended to improve safety and take a leadership role in setting the national agenda for key quality improvement areas. We now have official liaisons with Academy of Health-System Pharmacists (AHSP), National Transitions of Care Coalition (NTOCC), Institute for Healthcare Improvement (IHI), and Transforming Care at the Bedside (TCAB).
HQPS members also serve as leaders in national efforts to define and improve care transitions including the American Board of Internal Medicine’s Stepping up to the Plate program, and Hartford’s Safe Steps.
Advocacy Efforts Continue in Support of Proposed E&M Increases
SHM intensified its advocacy efforts over the past several months in support of proposed changes to the Medicare physician fee schedule that would significantly increase payments to hospitalists for many services next year, if adopted by the Centers for Medicare and Medicaid Services (CMS). In June, CMS proposed to make the largest increase in the work relative value units (RVUs) assigned to evaluation and management (E/M) services since Medicare implemented the physician fee schedule in 1992. E/M codes, which represent the time and effort that physicians spend to evaluate patient conditions, have long been viewed as undervalued. Since the release of the proposed rule, SHM has voiced its strong support for CMS’ proposed changes. (See “Calculating the Future of Medicare Payments,” Oct., p. 1).
In an August 18 letter, SHM joined the American College of Physicians (ACP) and 12 other physician groups in urging CMS Administrator Mark McClellan, MD, to include in the final rule the proposed increases in the RVUs assigned to office and hospital visits, and consultations. The groups applauded CMS’ decision to accept the recommendations made by the AMA Relative Value Scale Update Committee (RUC) regarding the evaluation and management codes under the five-year review. “We support the decision to include them in this proposed rule and we strongly urge CMS to include the same proposed work relative value units (RVUs) in the final rule,” the letter stated.
The RUC was careful to ensure that these codes went through the standard survey process and that the data supporting the changes was very strong. The letter emphasized: “The RUC approval of these recommendations, which requires support from at least two-thirds of the RUC members, indicates wide recognition of the work changes in evaluation and management in the 10 years since CMS last reviewed the codes. During our investigation into the increased intensity of evaluation and management services and throughout the RUC process for determining accurate, current work RVUs, we became increasingly aware that enormous changes in patient and physician practice characteristics necessitated these changes.”
In addition, the letter urged CMS to make the required budget neutrality adjustments that result from the five-year review to the conversion factor rather than by an adjustment to the work RVUs. CMS is required by law to offset increases in costs with a mandatory adjustment to keep 2007 expenditures roughly equal to their 2006 level. In the proposed rule, the agency recommended cutting work RVUs by 10% in order to achieve budget neutrality.
SHM joined the AMA and more than 70 other physician organizations in a separate letter. That letter asked CMS not to apply a 10% cut to the work component of the fee schedule, but instead to make an adjustment to the Medicare conversion factor.
“Applying budget neutrality to the work RVUs to offset the improvements in E/M and other services is a step backward and we strongly urge CMS to instead apply any necessary adjustments to the conversion factor,” the organizations said in an August 21 letter to CMS.
When the agency reduced the work RVUs in the past, it created confusion among private insurers, the letter said. Since 1998, similar reductions have been applied to the conversion factor. “CMS does not explain why it proposes to alter this long utilized method and move backward to an approach that the agency itself remarked was inappropriate.”
SHM and the physician community have also lobbied Congress to block a 5.1% cut in the Medicare physician fee schedule that will take effect on January 1, 2007, unless lawmakers take action this fall.
For more news on the five-year review, the 2007 update, and other issues, visit the advocacy and policy section of the SHM Web site at www.hospitalmedicine.org.
Allendorf is senior advisor of Advocacy and Government Affairs for SHM.
SHM intensified its advocacy efforts over the past several months in support of proposed changes to the Medicare physician fee schedule that would significantly increase payments to hospitalists for many services next year, if adopted by the Centers for Medicare and Medicaid Services (CMS). In June, CMS proposed to make the largest increase in the work relative value units (RVUs) assigned to evaluation and management (E/M) services since Medicare implemented the physician fee schedule in 1992. E/M codes, which represent the time and effort that physicians spend to evaluate patient conditions, have long been viewed as undervalued. Since the release of the proposed rule, SHM has voiced its strong support for CMS’ proposed changes. (See “Calculating the Future of Medicare Payments,” Oct., p. 1).
In an August 18 letter, SHM joined the American College of Physicians (ACP) and 12 other physician groups in urging CMS Administrator Mark McClellan, MD, to include in the final rule the proposed increases in the RVUs assigned to office and hospital visits, and consultations. The groups applauded CMS’ decision to accept the recommendations made by the AMA Relative Value Scale Update Committee (RUC) regarding the evaluation and management codes under the five-year review. “We support the decision to include them in this proposed rule and we strongly urge CMS to include the same proposed work relative value units (RVUs) in the final rule,” the letter stated.
The RUC was careful to ensure that these codes went through the standard survey process and that the data supporting the changes was very strong. The letter emphasized: “The RUC approval of these recommendations, which requires support from at least two-thirds of the RUC members, indicates wide recognition of the work changes in evaluation and management in the 10 years since CMS last reviewed the codes. During our investigation into the increased intensity of evaluation and management services and throughout the RUC process for determining accurate, current work RVUs, we became increasingly aware that enormous changes in patient and physician practice characteristics necessitated these changes.”
In addition, the letter urged CMS to make the required budget neutrality adjustments that result from the five-year review to the conversion factor rather than by an adjustment to the work RVUs. CMS is required by law to offset increases in costs with a mandatory adjustment to keep 2007 expenditures roughly equal to their 2006 level. In the proposed rule, the agency recommended cutting work RVUs by 10% in order to achieve budget neutrality.
SHM joined the AMA and more than 70 other physician organizations in a separate letter. That letter asked CMS not to apply a 10% cut to the work component of the fee schedule, but instead to make an adjustment to the Medicare conversion factor.
“Applying budget neutrality to the work RVUs to offset the improvements in E/M and other services is a step backward and we strongly urge CMS to instead apply any necessary adjustments to the conversion factor,” the organizations said in an August 21 letter to CMS.
When the agency reduced the work RVUs in the past, it created confusion among private insurers, the letter said. Since 1998, similar reductions have been applied to the conversion factor. “CMS does not explain why it proposes to alter this long utilized method and move backward to an approach that the agency itself remarked was inappropriate.”
SHM and the physician community have also lobbied Congress to block a 5.1% cut in the Medicare physician fee schedule that will take effect on January 1, 2007, unless lawmakers take action this fall.
For more news on the five-year review, the 2007 update, and other issues, visit the advocacy and policy section of the SHM Web site at www.hospitalmedicine.org.
Allendorf is senior advisor of Advocacy and Government Affairs for SHM.
SHM intensified its advocacy efforts over the past several months in support of proposed changes to the Medicare physician fee schedule that would significantly increase payments to hospitalists for many services next year, if adopted by the Centers for Medicare and Medicaid Services (CMS). In June, CMS proposed to make the largest increase in the work relative value units (RVUs) assigned to evaluation and management (E/M) services since Medicare implemented the physician fee schedule in 1992. E/M codes, which represent the time and effort that physicians spend to evaluate patient conditions, have long been viewed as undervalued. Since the release of the proposed rule, SHM has voiced its strong support for CMS’ proposed changes. (See “Calculating the Future of Medicare Payments,” Oct., p. 1).
In an August 18 letter, SHM joined the American College of Physicians (ACP) and 12 other physician groups in urging CMS Administrator Mark McClellan, MD, to include in the final rule the proposed increases in the RVUs assigned to office and hospital visits, and consultations. The groups applauded CMS’ decision to accept the recommendations made by the AMA Relative Value Scale Update Committee (RUC) regarding the evaluation and management codes under the five-year review. “We support the decision to include them in this proposed rule and we strongly urge CMS to include the same proposed work relative value units (RVUs) in the final rule,” the letter stated.
The RUC was careful to ensure that these codes went through the standard survey process and that the data supporting the changes was very strong. The letter emphasized: “The RUC approval of these recommendations, which requires support from at least two-thirds of the RUC members, indicates wide recognition of the work changes in evaluation and management in the 10 years since CMS last reviewed the codes. During our investigation into the increased intensity of evaluation and management services and throughout the RUC process for determining accurate, current work RVUs, we became increasingly aware that enormous changes in patient and physician practice characteristics necessitated these changes.”
In addition, the letter urged CMS to make the required budget neutrality adjustments that result from the five-year review to the conversion factor rather than by an adjustment to the work RVUs. CMS is required by law to offset increases in costs with a mandatory adjustment to keep 2007 expenditures roughly equal to their 2006 level. In the proposed rule, the agency recommended cutting work RVUs by 10% in order to achieve budget neutrality.
SHM joined the AMA and more than 70 other physician organizations in a separate letter. That letter asked CMS not to apply a 10% cut to the work component of the fee schedule, but instead to make an adjustment to the Medicare conversion factor.
“Applying budget neutrality to the work RVUs to offset the improvements in E/M and other services is a step backward and we strongly urge CMS to instead apply any necessary adjustments to the conversion factor,” the organizations said in an August 21 letter to CMS.
When the agency reduced the work RVUs in the past, it created confusion among private insurers, the letter said. Since 1998, similar reductions have been applied to the conversion factor. “CMS does not explain why it proposes to alter this long utilized method and move backward to an approach that the agency itself remarked was inappropriate.”
SHM and the physician community have also lobbied Congress to block a 5.1% cut in the Medicare physician fee schedule that will take effect on January 1, 2007, unless lawmakers take action this fall.
For more news on the five-year review, the 2007 update, and other issues, visit the advocacy and policy section of the SHM Web site at www.hospitalmedicine.org.
Allendorf is senior advisor of Advocacy and Government Affairs for SHM.
SHM Shapes Pay for Performance
Federal officials are increasingly embracing pay for performance (P4P) in an effort to promote high-quality, cost effective care in government health programs. As the Centers for Medicaid and Medicare Services (CMS) and Congress move forward to implement this concept, SHM is working to ensure that the views of hospitalists are represented in this important debate.
More than 100 P4P programs are already up and running in the private sector in an attempt to reward quality healthcare by setting different payment levels for providers based on how well they meet benchmarks of quality and efficiency. CMS is testing the feasibility of applying this concept to the Medicare program through a number of initiatives.
SHM’s Public Policy and Hospital Quality and Patient Safety committees have been involved in evaluating CMS’ Physician Voluntary Reporting Program (PVRP), launched earlier this year and widely believed to be the precursor to an eventual P4P program for physicians’ services. Under this initiative, physicians are encouraged to submit quality data on a “starter set” of 16 evidence-based measures for certain primary care, surgery, nephrology, and emergency medical services. Physicians who participate in the program receive confidential reports on their performance.
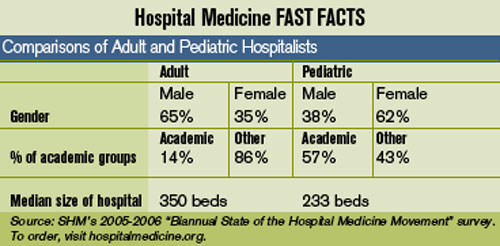
SHM has recommended that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable as a way of becoming more familiar with the program. Because these initial 16 measures have only limited relevance to services billed by hospitalists, SHM is engaged in discussions with lawmakers and their staffs, CMS officials, and consensus organizations involved in developing quality measures, to expand the program’s scope.
As part of Advocacy Day on May 3, some 70 SHM members met with legislators and their staffs and conveyed SHM’s support for initiatives like the PVRP that seek to measure resource use and improve quality, to attain better value for the Medicare program. (See coverage in The Hospitalist SHM Meeting Reporter, July 2006, p. 1.) Participants also educated lawmakers on the role of hospitalists in helping their institutions meet quality reporting requirements mandated under the Medicare Modernization Act, which ties annual hospital payment updates to the submission of performance data for 10 quality measures. The participants also expressed SHM’s interest in working with CMS on demonstration projects that assess the contributions of hospital medicine programs to improved patient care and more efficient management of hospital resources.
In addition to Congress and CMS, non-governmental groups such as the National Quality Forum (NQF), the American Medical Association Physician Consortium for Performance Improvement (PCPI), and the Ambulatory Care Quality Alliance are actively engaged in providing input to CMS on the PVRP and other P4P-related initiatives. SHM has joined the PCPI, which works with medical specialty organizations to develop physician-level performance measures.
As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM will also participate in two upcoming workgroups—one on emergency medicine, which will focus on treating for MI and pneumonia, and another on geriatrics, which will look at falls, urinary incontinence, and end-of-life care. At least through 2006, the PCPI is focusing on measures that fall under the CMS contract and will be included in the PVRP.
SHM is also a member of the NQF, a nonprofit organization that Congress has charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. NQF is seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on new consensus standards for hospital care. This project, sponsored by the AHRQ, will address issues of patient safety, pediatrics, and inpatient care. SHM will submit nominations during this process and plans to be fully engaged.
To further develop its agenda on performance and quality standards in inpatient hospital care, SHM recently established a new Performance and Standards Task Force. This task force is charged with developing a coordinated approach for SHM to work with external organizations in the performance and standards and quality arena and comprises the chairs of the PPC and HQPS committees and other SHM leaders active in organizations like the JCAHO and the IHI.
P4P is here to stay. SHM is well positioned to influence the development and implementation of inpatient quality measures that may eventually become part of a Medicare P4P program for physician services. TH
Allendorf is senior advisor for Advocacy and Government Affairs at SHM. Epstein is senior advisor for Quality Standards and Compliance at SHM.
SHM: BEHIND THE SCENES
How SHM Manages Your Money
By Steven Poitras

In the past three months you have read articles from my peers, including one by Todd Von Deak concerning the great strides he is making in the membership department by ensuring that we are generating the most benefits for our members; one from Scott Johnson, who is taking us into the future with regard to information services; and from Geri Barnes, our education and quality initiatives director, who is helping drive our organizational mission of promoting excellence in the practice of hospital medicine.
This month I want to tell you about our organization, its structure, and what we are collectively doing to ensure that the dues and grants we receive are put to good use to benefit our members and ensure our place in driving hospital medicine forward.
Studies show that 70% of small businesses and small non-profit organizations survive their first year, 30% survive their second year, and only 20% survive after five years. SHM will celebrate its 10th year in 2007. Congratulations and thank you. It’s you, our members, who have taken us this far. It’s you, our members, who will take us into the next 10, 20, 50 years, and beyond. We are not the same organization we were 10 years ago, and I suspect we will not be the same organization in 10 years that we are today.
Over the years I have worked and consulted in many organizations ranging from small mom-and-pops to large, multinational corporations. More often than not, despite a common desire to succeed, conflict exists within various constituencies (e.g., employees, executive management, board of directors) that leads to differing opinions on the best strategy for the company moving forward. I’m proud to say that this isn’t the case with SHM.
We have formulated a business model that uses tried-and-true corporate tools to ensure our members receive the maximum possible value in areas of the greatest impact. It encompasses both our paid and non-paid staff and volunteers to validate what matters most. Your dollars are put to good use. We concentrate on doing things that can be done and done well. If it’s a great idea but doesn’t get to the heart of what our members need or want, we won’t siphon off money and time. We receive money from our members and grantors with the intent of fulfilling a promise or mission. We try to understand what can be accomplished, and then we apply our resources to those goals, ensuring that a higher percentage of those resources are going to mission critical programs and services.
Both our members and grantors look for a strong return on their investment for the monies they send and set aside for our cause. Performance standards are necessary, not only to ensure high level delivery of services but also to ensure our organization’s fiscal responsibility. We employ a staff with many qualifications and backgrounds and coordinate our efforts further with diverse, educated, and dedicated volunteers who are experts in their areas.
Not only is our staff concerned with producing measurable results attributed to the dollars we receive, but we are also measuring mission success in numeric terms other than profit and loss, most specifically within our education and quality initiatives as well as our membership departments. Together these departments are spearheading metrics initiatives that are, for the most part, completely new to our organization but essential to our growth. We involve our staff at all levels of the organization in the pursuit of obtaining these metrics. We strive to collaboratively fulfill SHM’s objectives, and our adaptability allows us to scan the external environment and respond to the ever-changing needs of our members and grantors. Consistency of these values and the internal systems from our information services department that support problem solving, efficiency, and effectiveness at every level across our organizational boundaries help us obtain fulfilling our mission.
Communication about our direction is provided at every opportunity: staff meetings, board meetings, brown-bag lunches, and one-on-one employee discussions. Teamwork is emphasized as the primary means for accomplishing work. When decisions need to be made, all employees and volunteers are sought for counsel and advice from them, their peers, and others who might have insight about our programs. Armed with knowledge, strategic and tactical objectives that are clearly defined and pursued with greater focus, conviction, and diligence our employees embrace the change that is so evident in our fast moving organization.
Everyone in our organization understands where we are going, how we intend to get there, and how he or she fits into our organization’s strategy. The culture of our organization has shifted, but our focus on the benefits of hospital medicine has remained constant. By utilizing these strategic planning tools and techniques, we are redeveloping and revitalizing our corporate mission statement by understanding our organizations strengths, weaknesses, opportunities, threats, and actual and potential competitive advantages. This allows us to move beyond just mere expectations to actually setting the standard by which everyone will be judged.
Our employees, volunteers, members, and grantors remind us that while the business is managed on a daily basis, during our strategic planning and project implementation we focus our strategy on the vital few rather than the trivial many. This allows us to put our organization on the right track for survival and long-term growth.
As we grow, we will search harder and further for experts to help us fulfill our promise of setting SHM as the standard in hospital medicine. I encourage your feedback. Please reach me at spoitras@hospitalmedicine.org. You will find that I am always accessible and open to your thoughts and ideas.
Next month you will hear from Laura Allendorf, senior advisor for advocacy and government affairs.
Poitras is director of Business Operations at SHM.
Federal officials are increasingly embracing pay for performance (P4P) in an effort to promote high-quality, cost effective care in government health programs. As the Centers for Medicaid and Medicare Services (CMS) and Congress move forward to implement this concept, SHM is working to ensure that the views of hospitalists are represented in this important debate.
More than 100 P4P programs are already up and running in the private sector in an attempt to reward quality healthcare by setting different payment levels for providers based on how well they meet benchmarks of quality and efficiency. CMS is testing the feasibility of applying this concept to the Medicare program through a number of initiatives.
SHM’s Public Policy and Hospital Quality and Patient Safety committees have been involved in evaluating CMS’ Physician Voluntary Reporting Program (PVRP), launched earlier this year and widely believed to be the precursor to an eventual P4P program for physicians’ services. Under this initiative, physicians are encouraged to submit quality data on a “starter set” of 16 evidence-based measures for certain primary care, surgery, nephrology, and emergency medical services. Physicians who participate in the program receive confidential reports on their performance.
SHM has recommended that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable as a way of becoming more familiar with the program. Because these initial 16 measures have only limited relevance to services billed by hospitalists, SHM is engaged in discussions with lawmakers and their staffs, CMS officials, and consensus organizations involved in developing quality measures, to expand the program’s scope.
As part of Advocacy Day on May 3, some 70 SHM members met with legislators and their staffs and conveyed SHM’s support for initiatives like the PVRP that seek to measure resource use and improve quality, to attain better value for the Medicare program. (See coverage in The Hospitalist SHM Meeting Reporter, July 2006, p. 1.) Participants also educated lawmakers on the role of hospitalists in helping their institutions meet quality reporting requirements mandated under the Medicare Modernization Act, which ties annual hospital payment updates to the submission of performance data for 10 quality measures. The participants also expressed SHM’s interest in working with CMS on demonstration projects that assess the contributions of hospital medicine programs to improved patient care and more efficient management of hospital resources.
In addition to Congress and CMS, non-governmental groups such as the National Quality Forum (NQF), the American Medical Association Physician Consortium for Performance Improvement (PCPI), and the Ambulatory Care Quality Alliance are actively engaged in providing input to CMS on the PVRP and other P4P-related initiatives. SHM has joined the PCPI, which works with medical specialty organizations to develop physician-level performance measures.
As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM will also participate in two upcoming workgroups—one on emergency medicine, which will focus on treating for MI and pneumonia, and another on geriatrics, which will look at falls, urinary incontinence, and end-of-life care. At least through 2006, the PCPI is focusing on measures that fall under the CMS contract and will be included in the PVRP.
SHM is also a member of the NQF, a nonprofit organization that Congress has charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. NQF is seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on new consensus standards for hospital care. This project, sponsored by the AHRQ, will address issues of patient safety, pediatrics, and inpatient care. SHM will submit nominations during this process and plans to be fully engaged.
To further develop its agenda on performance and quality standards in inpatient hospital care, SHM recently established a new Performance and Standards Task Force. This task force is charged with developing a coordinated approach for SHM to work with external organizations in the performance and standards and quality arena and comprises the chairs of the PPC and HQPS committees and other SHM leaders active in organizations like the JCAHO and the IHI.
P4P is here to stay. SHM is well positioned to influence the development and implementation of inpatient quality measures that may eventually become part of a Medicare P4P program for physician services. TH
Allendorf is senior advisor for Advocacy and Government Affairs at SHM. Epstein is senior advisor for Quality Standards and Compliance at SHM.
SHM: BEHIND THE SCENES
How SHM Manages Your Money
By Steven Poitras
In the past three months you have read articles from my peers, including one by Todd Von Deak concerning the great strides he is making in the membership department by ensuring that we are generating the most benefits for our members; one from Scott Johnson, who is taking us into the future with regard to information services; and from Geri Barnes, our education and quality initiatives director, who is helping drive our organizational mission of promoting excellence in the practice of hospital medicine.
This month I want to tell you about our organization, its structure, and what we are collectively doing to ensure that the dues and grants we receive are put to good use to benefit our members and ensure our place in driving hospital medicine forward.
Studies show that 70% of small businesses and small non-profit organizations survive their first year, 30% survive their second year, and only 20% survive after five years. SHM will celebrate its 10th year in 2007. Congratulations and thank you. It’s you, our members, who have taken us this far. It’s you, our members, who will take us into the next 10, 20, 50 years, and beyond. We are not the same organization we were 10 years ago, and I suspect we will not be the same organization in 10 years that we are today.
Over the years I have worked and consulted in many organizations ranging from small mom-and-pops to large, multinational corporations. More often than not, despite a common desire to succeed, conflict exists within various constituencies (e.g., employees, executive management, board of directors) that leads to differing opinions on the best strategy for the company moving forward. I’m proud to say that this isn’t the case with SHM.
We have formulated a business model that uses tried-and-true corporate tools to ensure our members receive the maximum possible value in areas of the greatest impact. It encompasses both our paid and non-paid staff and volunteers to validate what matters most. Your dollars are put to good use. We concentrate on doing things that can be done and done well. If it’s a great idea but doesn’t get to the heart of what our members need or want, we won’t siphon off money and time. We receive money from our members and grantors with the intent of fulfilling a promise or mission. We try to understand what can be accomplished, and then we apply our resources to those goals, ensuring that a higher percentage of those resources are going to mission critical programs and services.
Both our members and grantors look for a strong return on their investment for the monies they send and set aside for our cause. Performance standards are necessary, not only to ensure high level delivery of services but also to ensure our organization’s fiscal responsibility. We employ a staff with many qualifications and backgrounds and coordinate our efforts further with diverse, educated, and dedicated volunteers who are experts in their areas.
Not only is our staff concerned with producing measurable results attributed to the dollars we receive, but we are also measuring mission success in numeric terms other than profit and loss, most specifically within our education and quality initiatives as well as our membership departments. Together these departments are spearheading metrics initiatives that are, for the most part, completely new to our organization but essential to our growth. We involve our staff at all levels of the organization in the pursuit of obtaining these metrics. We strive to collaboratively fulfill SHM’s objectives, and our adaptability allows us to scan the external environment and respond to the ever-changing needs of our members and grantors. Consistency of these values and the internal systems from our information services department that support problem solving, efficiency, and effectiveness at every level across our organizational boundaries help us obtain fulfilling our mission.
Communication about our direction is provided at every opportunity: staff meetings, board meetings, brown-bag lunches, and one-on-one employee discussions. Teamwork is emphasized as the primary means for accomplishing work. When decisions need to be made, all employees and volunteers are sought for counsel and advice from them, their peers, and others who might have insight about our programs. Armed with knowledge, strategic and tactical objectives that are clearly defined and pursued with greater focus, conviction, and diligence our employees embrace the change that is so evident in our fast moving organization.
Everyone in our organization understands where we are going, how we intend to get there, and how he or she fits into our organization’s strategy. The culture of our organization has shifted, but our focus on the benefits of hospital medicine has remained constant. By utilizing these strategic planning tools and techniques, we are redeveloping and revitalizing our corporate mission statement by understanding our organizations strengths, weaknesses, opportunities, threats, and actual and potential competitive advantages. This allows us to move beyond just mere expectations to actually setting the standard by which everyone will be judged.
Our employees, volunteers, members, and grantors remind us that while the business is managed on a daily basis, during our strategic planning and project implementation we focus our strategy on the vital few rather than the trivial many. This allows us to put our organization on the right track for survival and long-term growth.
As we grow, we will search harder and further for experts to help us fulfill our promise of setting SHM as the standard in hospital medicine. I encourage your feedback. Please reach me at spoitras@hospitalmedicine.org. You will find that I am always accessible and open to your thoughts and ideas.
Next month you will hear from Laura Allendorf, senior advisor for advocacy and government affairs.
Poitras is director of Business Operations at SHM.
Federal officials are increasingly embracing pay for performance (P4P) in an effort to promote high-quality, cost effective care in government health programs. As the Centers for Medicaid and Medicare Services (CMS) and Congress move forward to implement this concept, SHM is working to ensure that the views of hospitalists are represented in this important debate.
More than 100 P4P programs are already up and running in the private sector in an attempt to reward quality healthcare by setting different payment levels for providers based on how well they meet benchmarks of quality and efficiency. CMS is testing the feasibility of applying this concept to the Medicare program through a number of initiatives.
SHM’s Public Policy and Hospital Quality and Patient Safety committees have been involved in evaluating CMS’ Physician Voluntary Reporting Program (PVRP), launched earlier this year and widely believed to be the precursor to an eventual P4P program for physicians’ services. Under this initiative, physicians are encouraged to submit quality data on a “starter set” of 16 evidence-based measures for certain primary care, surgery, nephrology, and emergency medical services. Physicians who participate in the program receive confidential reports on their performance.
SHM has recommended that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable as a way of becoming more familiar with the program. Because these initial 16 measures have only limited relevance to services billed by hospitalists, SHM is engaged in discussions with lawmakers and their staffs, CMS officials, and consensus organizations involved in developing quality measures, to expand the program’s scope.
As part of Advocacy Day on May 3, some 70 SHM members met with legislators and their staffs and conveyed SHM’s support for initiatives like the PVRP that seek to measure resource use and improve quality, to attain better value for the Medicare program. (See coverage in The Hospitalist SHM Meeting Reporter, July 2006, p. 1.) Participants also educated lawmakers on the role of hospitalists in helping their institutions meet quality reporting requirements mandated under the Medicare Modernization Act, which ties annual hospital payment updates to the submission of performance data for 10 quality measures. The participants also expressed SHM’s interest in working with CMS on demonstration projects that assess the contributions of hospital medicine programs to improved patient care and more efficient management of hospital resources.
In addition to Congress and CMS, non-governmental groups such as the National Quality Forum (NQF), the American Medical Association Physician Consortium for Performance Improvement (PCPI), and the Ambulatory Care Quality Alliance are actively engaged in providing input to CMS on the PVRP and other P4P-related initiatives. SHM has joined the PCPI, which works with medical specialty organizations to develop physician-level performance measures.
As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM will also participate in two upcoming workgroups—one on emergency medicine, which will focus on treating for MI and pneumonia, and another on geriatrics, which will look at falls, urinary incontinence, and end-of-life care. At least through 2006, the PCPI is focusing on measures that fall under the CMS contract and will be included in the PVRP.
SHM is also a member of the NQF, a nonprofit organization that Congress has charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. NQF is seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on new consensus standards for hospital care. This project, sponsored by the AHRQ, will address issues of patient safety, pediatrics, and inpatient care. SHM will submit nominations during this process and plans to be fully engaged.
To further develop its agenda on performance and quality standards in inpatient hospital care, SHM recently established a new Performance and Standards Task Force. This task force is charged with developing a coordinated approach for SHM to work with external organizations in the performance and standards and quality arena and comprises the chairs of the PPC and HQPS committees and other SHM leaders active in organizations like the JCAHO and the IHI.
P4P is here to stay. SHM is well positioned to influence the development and implementation of inpatient quality measures that may eventually become part of a Medicare P4P program for physician services. TH
Allendorf is senior advisor for Advocacy and Government Affairs at SHM. Epstein is senior advisor for Quality Standards and Compliance at SHM.
SHM: BEHIND THE SCENES
How SHM Manages Your Money
By Steven Poitras
In the past three months you have read articles from my peers, including one by Todd Von Deak concerning the great strides he is making in the membership department by ensuring that we are generating the most benefits for our members; one from Scott Johnson, who is taking us into the future with regard to information services; and from Geri Barnes, our education and quality initiatives director, who is helping drive our organizational mission of promoting excellence in the practice of hospital medicine.
This month I want to tell you about our organization, its structure, and what we are collectively doing to ensure that the dues and grants we receive are put to good use to benefit our members and ensure our place in driving hospital medicine forward.
Studies show that 70% of small businesses and small non-profit organizations survive their first year, 30% survive their second year, and only 20% survive after five years. SHM will celebrate its 10th year in 2007. Congratulations and thank you. It’s you, our members, who have taken us this far. It’s you, our members, who will take us into the next 10, 20, 50 years, and beyond. We are not the same organization we were 10 years ago, and I suspect we will not be the same organization in 10 years that we are today.
Over the years I have worked and consulted in many organizations ranging from small mom-and-pops to large, multinational corporations. More often than not, despite a common desire to succeed, conflict exists within various constituencies (e.g., employees, executive management, board of directors) that leads to differing opinions on the best strategy for the company moving forward. I’m proud to say that this isn’t the case with SHM.
We have formulated a business model that uses tried-and-true corporate tools to ensure our members receive the maximum possible value in areas of the greatest impact. It encompasses both our paid and non-paid staff and volunteers to validate what matters most. Your dollars are put to good use. We concentrate on doing things that can be done and done well. If it’s a great idea but doesn’t get to the heart of what our members need or want, we won’t siphon off money and time. We receive money from our members and grantors with the intent of fulfilling a promise or mission. We try to understand what can be accomplished, and then we apply our resources to those goals, ensuring that a higher percentage of those resources are going to mission critical programs and services.
Both our members and grantors look for a strong return on their investment for the monies they send and set aside for our cause. Performance standards are necessary, not only to ensure high level delivery of services but also to ensure our organization’s fiscal responsibility. We employ a staff with many qualifications and backgrounds and coordinate our efforts further with diverse, educated, and dedicated volunteers who are experts in their areas.
Not only is our staff concerned with producing measurable results attributed to the dollars we receive, but we are also measuring mission success in numeric terms other than profit and loss, most specifically within our education and quality initiatives as well as our membership departments. Together these departments are spearheading metrics initiatives that are, for the most part, completely new to our organization but essential to our growth. We involve our staff at all levels of the organization in the pursuit of obtaining these metrics. We strive to collaboratively fulfill SHM’s objectives, and our adaptability allows us to scan the external environment and respond to the ever-changing needs of our members and grantors. Consistency of these values and the internal systems from our information services department that support problem solving, efficiency, and effectiveness at every level across our organizational boundaries help us obtain fulfilling our mission.
Communication about our direction is provided at every opportunity: staff meetings, board meetings, brown-bag lunches, and one-on-one employee discussions. Teamwork is emphasized as the primary means for accomplishing work. When decisions need to be made, all employees and volunteers are sought for counsel and advice from them, their peers, and others who might have insight about our programs. Armed with knowledge, strategic and tactical objectives that are clearly defined and pursued with greater focus, conviction, and diligence our employees embrace the change that is so evident in our fast moving organization.
Everyone in our organization understands where we are going, how we intend to get there, and how he or she fits into our organization’s strategy. The culture of our organization has shifted, but our focus on the benefits of hospital medicine has remained constant. By utilizing these strategic planning tools and techniques, we are redeveloping and revitalizing our corporate mission statement by understanding our organizations strengths, weaknesses, opportunities, threats, and actual and potential competitive advantages. This allows us to move beyond just mere expectations to actually setting the standard by which everyone will be judged.
Our employees, volunteers, members, and grantors remind us that while the business is managed on a daily basis, during our strategic planning and project implementation we focus our strategy on the vital few rather than the trivial many. This allows us to put our organization on the right track for survival and long-term growth.
As we grow, we will search harder and further for experts to help us fulfill our promise of setting SHM as the standard in hospital medicine. I encourage your feedback. Please reach me at spoitras@hospitalmedicine.org. You will find that I am always accessible and open to your thoughts and ideas.
Next month you will hear from Laura Allendorf, senior advisor for advocacy and government affairs.
Poitras is director of Business Operations at SHM.