User login
Antipsychotics in the elderly: Reducing risks of stroke and death
In early-stage Alzheimer’s disease, Mrs. P enters a nursing home because her daughter, who usually takes care of her, is hospitalized for cancer chemotherapy. Mrs. P promptly develops paranoid delusions and refuses her medications for high blood pressure and high cholesterol. What are the treatment options? Is any one antipsychotic safer than another?
Writing an antipsychotic prescription for patients such as Mrs. P is no longer a quick scribble. First we learned that atypicals may alter glucose and lipid metabolism in clinically troublesome ways.1,2 Then we learned that antipsychotics can triple the risk for sudden death in older patients with dementia. (See FDA advisory, Related resources.)
How great are the risks, who is at risk, and how strong is the evidence for these new risks? The debate is not yet settled, but the boundaries of good practice for antipsychotic use in older patients are being redrawn. This is particularly true for those with dementia, in whom antipsychotics’ risk/benefit ratio is higher than for older patients with schizophrenia or bipolar disorder.
Unproven effectiveness
Antipsychotics are not FDA-approved for treating dementia-related psychosis. Though antipsychotics are commonly used off-label to treat behavioral disturbances in the elderly with dementia, no standard of care exists for managing these symptoms with drugs. So far, the evidence for antipsychotics’ effectiveness for dementia’s behavioral and psychological symptoms is spotty at best.
Sink et al (Table 1)3 systematically reviewed 14 randomized, controlled trials and concluded “there is no clear evidence that typical antipsychotics are useful for treating neuropsychiatric symptoms [of dementia].” They concluded from 6 studies of atypicals that only olanzapine and risperidone had shown efficacy, but the effects were “modest and further complicated by risk of stroke.” When the benefits are modest, the risks are more difficult to justify.
When medication is necessary, on the other hand, the Expert Consensus Panel for Using Antipsychotic Drugs in Older Patients reported in 2004 that “for agitated dementia with delusions, the experts’ first-line recommendation is an antipsychotic drug alone…. Risperidone (0.5 to 2.0 mg/day) was first line, followed by quetiapine (50 to 150 mg/day) and olanzapine (5.0 to 7.5 mg/day) as high second-line options.”4
CATIE studies. The definitive prospective study of antipsychotics’ effectiveness in dementia has not been completed. The National Institute of Mental Health is sponsoring CATIE—Clinical Antipsychotic Trials of Intervention Effectiveness—a multi-site research program comparing the effectiveness and outcomes of antipsychotics in treating schizophrenia and Alzheimer’s disease. Results of the Alzheimer disease arm5 are expected next year.
The schizophrenia arm comparing four atypical antipsychotics (quetiapine, risperidone, ziprasidone, and olanzapine) and one typical antipsychotic (perphenazine) found:
- Typical and atypical antipsychotics were similarly effective in 1,493 patients with chronic schizophrenia
- 74% of patients discontinued assigned medications before 18 months for lack of efficacy, intolerable side effects, or other reasons.6
Table 1
Timeline: Evidence on risks, efficacy of atypical antipsychotics
| Year | Summary of study findings, FDA warnings |
|---|---|
| 2002 | Higher incidence of stroke seen with risperidone than with placebo in two of four clinical trials (Wooltorton7) Health Canada and Janssen-Ortho warn Canadian physicians of possible link between risperidone and stroke |
| 2003 | FDA warns of increased risk of stroke with risperidone |
| 2004 | Threefold increased risk of sudden cardiac death associated with antipsychotic use in patients age >65, most without dementia (Straus et al11) |
| 2005 | Stroke risk reported no greater in older patients who took atypicals than in those who took typical antipsychotics (Gill et al10) Analysis of 14 controlled trials finds “no clear evidence” that typical antipsychotics are effective in dementia; atypicals’ effects seen as “modest” (Sink et al3) FDA issues warning after finding 60% increase in risk of sudden death in review of 17 trials in older patients receiving atypical antipsychotics for dementia Efficacy of conventional and atypical antipsychotics found similar in patients with chronic schizophrenia (Lieberman et al6) |
Stroke risk
How strong is the evidence for stroke risk among older patients who take antipsychotics? Wooltorton7 first raised concern about increased risk of stroke with risperidone in 2002 in a summary of four clinical trials. Though none was designed to examine stroke risk as the primary outcome, two showed significantly higher incidence of cerebrovascular events with risperidone than with placebo. The stroke rate with risperidone was double that with placebo (4% vs 2%) across the total 1,200 subjects in the four studies.
This preliminary report led to an FDA advisory but surprisingly no definitive studies or systematic reviews. No epidemiologic studies have examined stroke rates in those who take antipsychotics compared with those who don’t, while controlling for common stroke predictors. So we have a warning based on post hoc analyses in two positive and two negative studies, but no sound estimate of how much antipsychotic use in general adds to the risk of stroke.
Atypicals vs. typicals. Are atypicals worse than typicals in their effect on stroke risk?
Herrmann et al8,9 reviewed a health care database of 11,400 older persons and found no statistically significant increase in stroke rate with risperidone or olanzapine compared with typical antipsychotics. This study did not assess whether patients had dementia or primary psychotic disorders.
In a larger retrospective study of 32,710 older persons with dementia, Herrmann’s group10 found no greater stroke risk in those who took atypicals than in those who took typical antipsychotics.
So the evidence for the risk of stroke in older patients who take antipsychotics is based on a few reports and no definitive studies.
Risk of early death
What about the risk of early death? After reviewing 17 clinical trials of atypical antipsychotics in older patients with dementia, the FDA issued its warning in April 2005 about increased mortality risk (see Related resources). Fifteen of the trials showed an increased mortality risk, resulting in an estimated 1.6- to 1.7-fold increase in risk of death, mostly by cardiac or infectious causes.
A year earlier, Straus et al11 reported on risk of sudden cardiac death with antipsychotic use in a population-based, case-control study in the Netherlands. In this longitudinal, observational database of 250,000 patients, 75% were age >65 and <1% had dementia. Current use of antipsychotics was associated with a threefold increase in risk of sudden cardiac death (554 cases), after other predictors of sudden death were factored in. This risk increased with higher antipsychotic dosages and was similarly elevated for patients with and without schizophrenia-related disorders.
Mechanisms unknown
By what mechanisms could antipsychotics precipitate stroke, sudden cardiac death, or pneumonia? A clear biological mechanism has not been proposed, much less proven. The risks seen in clinical trials—usually lasting 12 weeks or less—suggest an acute effect rather than the more-gradual consequences of weight gain, altered lipid metabolism, or diabetes.
Speculations range widely. Possibilities awaiting study include postural hypotension, altered platelet aggregation, increased venous thromboembolism, peripheral vasodilation leading to cardiovascular collapse, acute dystonia, acute cardiomyopathy, arrhythmias related to QT prolongation, and other forms of cardiac toxicity.10,11
Remaining questions
The few studies plus two FDA advisories force clinicians to make complex treatment decisions on insufficient evidence. Here’s what we don’t know:
- The magnitude of stroke or sudden death risk in older patients who take antipsychotics for any diagnosis. (All studies have limitations, and public health policy should not rely on one or two studies, no matter how good they may be.)
- Who is at higher or lower risk with antipsychotic use—men vs women? blacks vs whites?etc.
- Biological mechanisms of an association between antipsychotics and risks of stroke and premature death.
Strategies for reducing risk
We can minimize patients’ clinical risk and our legal risk only by using the limited evidence, expert consensus, and sound clinical judgment. Suggested strategies are listed in Table 2.
Table 2
Strategies to minimize antipsychotic risk in patients age 65 and older
| Review and document risk factors for cardiovascular disease—including stroke—with physical examination, laboratory tests (lipid profile, fasting glucose), and ECG in consultation with a primary care physician or specialist |
| Try nonpharmacologic approaches first whenever possible to manage behavioral disturbances in patients with dementia; document results before trying an antipsychotic |
| Review antipsychotics’ risks and benefits with patient and family |
| Use low dosages and increase gradually, as sudden death risk is dose-related |
| Monitor antipsychotic effectiveness, and discontinue trials of questionable benefit |
| Monitor cardiovascular symptoms, heart rate, blood pressure and body mass index of patients with cardiovascular risk |
| Avoid using sedating antipsychotics for insomnia in patients without psychiatric disorders |

Dr. Wulsin treats psychiatric outpatients and has published reviews on depression and heart disease. He is training director, University of Cincinnati family medicine-psychiatry residency program.
- Food and Drug Administration. Advisory on increased risk of mortality with use of atypical antipsychotics to treat behavioral disturbances in older patients with dementia. www.fda.gov/cder/drug/advisory/antipsychotics.htm.
Drug brand names
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Zimmermann U, Kraus T, Himmerich H, et al. Epidemiology, implications and mechanisms underlying drug-induced weight gain in psychiatric patients. J Psychiatr Res 2003;37(3):193-220.
2. Ryan MC, Thakore JH. Physical consequences of schizophrenia and its treatment: the metabolic syndrome. Life Sci 2002;71(3):239-57.
3. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA 2005;293(5):596-608.
4. Alexopoulos GS, Streim J, Carpenter D, Docherty JP. Using antipsychotic agents in older patients. J Clin Psychiatry 2004;65(suppl 2):5-99.
5. Schneider LS, Ismail MS, Dagerman K, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE): Alzheimer’s disease trial. Schizophr Bull 2003;29(1):57-72.
6. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
7. Wooltorton E. Risperidone (Risperdal): increased rate of cerebrovascular events in dementia trials. CMAJ 2002;167(11):1269-1270.
8. Herrmann N, Mamdani M, Lanctot KL. Atypical antipsychotics and risk of cerebrovascular accidents. Am J Psychiatry 2004;161(6):1113-1115.
9. Herrmann N, Lanctot KL. Do atypical antipsychotics cause stroke? CNS Drugs 2005;19(2):91-103.
10. Gill SS, Rochon PA, Herrmann N, et al. Atypical antipsychotic drugs and risk of ischaemic stroke: population based retrospective cohort study. BMJ 2005;330(7489):445.-
11. Straus SM, Bleumink GS, Dieleman JP, et al. Antipsychotics and the risk of sudden cardiac death. Arch Intern Med 2004;164(12):1293-7.
In early-stage Alzheimer’s disease, Mrs. P enters a nursing home because her daughter, who usually takes care of her, is hospitalized for cancer chemotherapy. Mrs. P promptly develops paranoid delusions and refuses her medications for high blood pressure and high cholesterol. What are the treatment options? Is any one antipsychotic safer than another?
Writing an antipsychotic prescription for patients such as Mrs. P is no longer a quick scribble. First we learned that atypicals may alter glucose and lipid metabolism in clinically troublesome ways.1,2 Then we learned that antipsychotics can triple the risk for sudden death in older patients with dementia. (See FDA advisory, Related resources.)
How great are the risks, who is at risk, and how strong is the evidence for these new risks? The debate is not yet settled, but the boundaries of good practice for antipsychotic use in older patients are being redrawn. This is particularly true for those with dementia, in whom antipsychotics’ risk/benefit ratio is higher than for older patients with schizophrenia or bipolar disorder.
Unproven effectiveness
Antipsychotics are not FDA-approved for treating dementia-related psychosis. Though antipsychotics are commonly used off-label to treat behavioral disturbances in the elderly with dementia, no standard of care exists for managing these symptoms with drugs. So far, the evidence for antipsychotics’ effectiveness for dementia’s behavioral and psychological symptoms is spotty at best.
Sink et al (Table 1)3 systematically reviewed 14 randomized, controlled trials and concluded “there is no clear evidence that typical antipsychotics are useful for treating neuropsychiatric symptoms [of dementia].” They concluded from 6 studies of atypicals that only olanzapine and risperidone had shown efficacy, but the effects were “modest and further complicated by risk of stroke.” When the benefits are modest, the risks are more difficult to justify.
When medication is necessary, on the other hand, the Expert Consensus Panel for Using Antipsychotic Drugs in Older Patients reported in 2004 that “for agitated dementia with delusions, the experts’ first-line recommendation is an antipsychotic drug alone…. Risperidone (0.5 to 2.0 mg/day) was first line, followed by quetiapine (50 to 150 mg/day) and olanzapine (5.0 to 7.5 mg/day) as high second-line options.”4
CATIE studies. The definitive prospective study of antipsychotics’ effectiveness in dementia has not been completed. The National Institute of Mental Health is sponsoring CATIE—Clinical Antipsychotic Trials of Intervention Effectiveness—a multi-site research program comparing the effectiveness and outcomes of antipsychotics in treating schizophrenia and Alzheimer’s disease. Results of the Alzheimer disease arm5 are expected next year.
The schizophrenia arm comparing four atypical antipsychotics (quetiapine, risperidone, ziprasidone, and olanzapine) and one typical antipsychotic (perphenazine) found:
- Typical and atypical antipsychotics were similarly effective in 1,493 patients with chronic schizophrenia
- 74% of patients discontinued assigned medications before 18 months for lack of efficacy, intolerable side effects, or other reasons.6
Table 1
Timeline: Evidence on risks, efficacy of atypical antipsychotics
| Year | Summary of study findings, FDA warnings |
|---|---|
| 2002 | Higher incidence of stroke seen with risperidone than with placebo in two of four clinical trials (Wooltorton7) Health Canada and Janssen-Ortho warn Canadian physicians of possible link between risperidone and stroke |
| 2003 | FDA warns of increased risk of stroke with risperidone |
| 2004 | Threefold increased risk of sudden cardiac death associated with antipsychotic use in patients age >65, most without dementia (Straus et al11) |
| 2005 | Stroke risk reported no greater in older patients who took atypicals than in those who took typical antipsychotics (Gill et al10) Analysis of 14 controlled trials finds “no clear evidence” that typical antipsychotics are effective in dementia; atypicals’ effects seen as “modest” (Sink et al3) FDA issues warning after finding 60% increase in risk of sudden death in review of 17 trials in older patients receiving atypical antipsychotics for dementia Efficacy of conventional and atypical antipsychotics found similar in patients with chronic schizophrenia (Lieberman et al6) |
Stroke risk
How strong is the evidence for stroke risk among older patients who take antipsychotics? Wooltorton7 first raised concern about increased risk of stroke with risperidone in 2002 in a summary of four clinical trials. Though none was designed to examine stroke risk as the primary outcome, two showed significantly higher incidence of cerebrovascular events with risperidone than with placebo. The stroke rate with risperidone was double that with placebo (4% vs 2%) across the total 1,200 subjects in the four studies.
This preliminary report led to an FDA advisory but surprisingly no definitive studies or systematic reviews. No epidemiologic studies have examined stroke rates in those who take antipsychotics compared with those who don’t, while controlling for common stroke predictors. So we have a warning based on post hoc analyses in two positive and two negative studies, but no sound estimate of how much antipsychotic use in general adds to the risk of stroke.
Atypicals vs. typicals. Are atypicals worse than typicals in their effect on stroke risk?
Herrmann et al8,9 reviewed a health care database of 11,400 older persons and found no statistically significant increase in stroke rate with risperidone or olanzapine compared with typical antipsychotics. This study did not assess whether patients had dementia or primary psychotic disorders.
In a larger retrospective study of 32,710 older persons with dementia, Herrmann’s group10 found no greater stroke risk in those who took atypicals than in those who took typical antipsychotics.
So the evidence for the risk of stroke in older patients who take antipsychotics is based on a few reports and no definitive studies.
Risk of early death
What about the risk of early death? After reviewing 17 clinical trials of atypical antipsychotics in older patients with dementia, the FDA issued its warning in April 2005 about increased mortality risk (see Related resources). Fifteen of the trials showed an increased mortality risk, resulting in an estimated 1.6- to 1.7-fold increase in risk of death, mostly by cardiac or infectious causes.
A year earlier, Straus et al11 reported on risk of sudden cardiac death with antipsychotic use in a population-based, case-control study in the Netherlands. In this longitudinal, observational database of 250,000 patients, 75% were age >65 and <1% had dementia. Current use of antipsychotics was associated with a threefold increase in risk of sudden cardiac death (554 cases), after other predictors of sudden death were factored in. This risk increased with higher antipsychotic dosages and was similarly elevated for patients with and without schizophrenia-related disorders.
Mechanisms unknown
By what mechanisms could antipsychotics precipitate stroke, sudden cardiac death, or pneumonia? A clear biological mechanism has not been proposed, much less proven. The risks seen in clinical trials—usually lasting 12 weeks or less—suggest an acute effect rather than the more-gradual consequences of weight gain, altered lipid metabolism, or diabetes.
Speculations range widely. Possibilities awaiting study include postural hypotension, altered platelet aggregation, increased venous thromboembolism, peripheral vasodilation leading to cardiovascular collapse, acute dystonia, acute cardiomyopathy, arrhythmias related to QT prolongation, and other forms of cardiac toxicity.10,11
Remaining questions
The few studies plus two FDA advisories force clinicians to make complex treatment decisions on insufficient evidence. Here’s what we don’t know:
- The magnitude of stroke or sudden death risk in older patients who take antipsychotics for any diagnosis. (All studies have limitations, and public health policy should not rely on one or two studies, no matter how good they may be.)
- Who is at higher or lower risk with antipsychotic use—men vs women? blacks vs whites?etc.
- Biological mechanisms of an association between antipsychotics and risks of stroke and premature death.
Strategies for reducing risk
We can minimize patients’ clinical risk and our legal risk only by using the limited evidence, expert consensus, and sound clinical judgment. Suggested strategies are listed in Table 2.
Table 2
Strategies to minimize antipsychotic risk in patients age 65 and older
| Review and document risk factors for cardiovascular disease—including stroke—with physical examination, laboratory tests (lipid profile, fasting glucose), and ECG in consultation with a primary care physician or specialist |
| Try nonpharmacologic approaches first whenever possible to manage behavioral disturbances in patients with dementia; document results before trying an antipsychotic |
| Review antipsychotics’ risks and benefits with patient and family |
| Use low dosages and increase gradually, as sudden death risk is dose-related |
| Monitor antipsychotic effectiveness, and discontinue trials of questionable benefit |
| Monitor cardiovascular symptoms, heart rate, blood pressure and body mass index of patients with cardiovascular risk |
| Avoid using sedating antipsychotics for insomnia in patients without psychiatric disorders |
Dr. Wulsin treats psychiatric outpatients and has published reviews on depression and heart disease. He is training director, University of Cincinnati family medicine-psychiatry residency program.
- Food and Drug Administration. Advisory on increased risk of mortality with use of atypical antipsychotics to treat behavioral disturbances in older patients with dementia. www.fda.gov/cder/drug/advisory/antipsychotics.htm.
Drug brand names
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
In early-stage Alzheimer’s disease, Mrs. P enters a nursing home because her daughter, who usually takes care of her, is hospitalized for cancer chemotherapy. Mrs. P promptly develops paranoid delusions and refuses her medications for high blood pressure and high cholesterol. What are the treatment options? Is any one antipsychotic safer than another?
Writing an antipsychotic prescription for patients such as Mrs. P is no longer a quick scribble. First we learned that atypicals may alter glucose and lipid metabolism in clinically troublesome ways.1,2 Then we learned that antipsychotics can triple the risk for sudden death in older patients with dementia. (See FDA advisory, Related resources.)
How great are the risks, who is at risk, and how strong is the evidence for these new risks? The debate is not yet settled, but the boundaries of good practice for antipsychotic use in older patients are being redrawn. This is particularly true for those with dementia, in whom antipsychotics’ risk/benefit ratio is higher than for older patients with schizophrenia or bipolar disorder.
Unproven effectiveness
Antipsychotics are not FDA-approved for treating dementia-related psychosis. Though antipsychotics are commonly used off-label to treat behavioral disturbances in the elderly with dementia, no standard of care exists for managing these symptoms with drugs. So far, the evidence for antipsychotics’ effectiveness for dementia’s behavioral and psychological symptoms is spotty at best.
Sink et al (Table 1)3 systematically reviewed 14 randomized, controlled trials and concluded “there is no clear evidence that typical antipsychotics are useful for treating neuropsychiatric symptoms [of dementia].” They concluded from 6 studies of atypicals that only olanzapine and risperidone had shown efficacy, but the effects were “modest and further complicated by risk of stroke.” When the benefits are modest, the risks are more difficult to justify.
When medication is necessary, on the other hand, the Expert Consensus Panel for Using Antipsychotic Drugs in Older Patients reported in 2004 that “for agitated dementia with delusions, the experts’ first-line recommendation is an antipsychotic drug alone…. Risperidone (0.5 to 2.0 mg/day) was first line, followed by quetiapine (50 to 150 mg/day) and olanzapine (5.0 to 7.5 mg/day) as high second-line options.”4
CATIE studies. The definitive prospective study of antipsychotics’ effectiveness in dementia has not been completed. The National Institute of Mental Health is sponsoring CATIE—Clinical Antipsychotic Trials of Intervention Effectiveness—a multi-site research program comparing the effectiveness and outcomes of antipsychotics in treating schizophrenia and Alzheimer’s disease. Results of the Alzheimer disease arm5 are expected next year.
The schizophrenia arm comparing four atypical antipsychotics (quetiapine, risperidone, ziprasidone, and olanzapine) and one typical antipsychotic (perphenazine) found:
- Typical and atypical antipsychotics were similarly effective in 1,493 patients with chronic schizophrenia
- 74% of patients discontinued assigned medications before 18 months for lack of efficacy, intolerable side effects, or other reasons.6
Table 1
Timeline: Evidence on risks, efficacy of atypical antipsychotics
| Year | Summary of study findings, FDA warnings |
|---|---|
| 2002 | Higher incidence of stroke seen with risperidone than with placebo in two of four clinical trials (Wooltorton7) Health Canada and Janssen-Ortho warn Canadian physicians of possible link between risperidone and stroke |
| 2003 | FDA warns of increased risk of stroke with risperidone |
| 2004 | Threefold increased risk of sudden cardiac death associated with antipsychotic use in patients age >65, most without dementia (Straus et al11) |
| 2005 | Stroke risk reported no greater in older patients who took atypicals than in those who took typical antipsychotics (Gill et al10) Analysis of 14 controlled trials finds “no clear evidence” that typical antipsychotics are effective in dementia; atypicals’ effects seen as “modest” (Sink et al3) FDA issues warning after finding 60% increase in risk of sudden death in review of 17 trials in older patients receiving atypical antipsychotics for dementia Efficacy of conventional and atypical antipsychotics found similar in patients with chronic schizophrenia (Lieberman et al6) |
Stroke risk
How strong is the evidence for stroke risk among older patients who take antipsychotics? Wooltorton7 first raised concern about increased risk of stroke with risperidone in 2002 in a summary of four clinical trials. Though none was designed to examine stroke risk as the primary outcome, two showed significantly higher incidence of cerebrovascular events with risperidone than with placebo. The stroke rate with risperidone was double that with placebo (4% vs 2%) across the total 1,200 subjects in the four studies.
This preliminary report led to an FDA advisory but surprisingly no definitive studies or systematic reviews. No epidemiologic studies have examined stroke rates in those who take antipsychotics compared with those who don’t, while controlling for common stroke predictors. So we have a warning based on post hoc analyses in two positive and two negative studies, but no sound estimate of how much antipsychotic use in general adds to the risk of stroke.
Atypicals vs. typicals. Are atypicals worse than typicals in their effect on stroke risk?
Herrmann et al8,9 reviewed a health care database of 11,400 older persons and found no statistically significant increase in stroke rate with risperidone or olanzapine compared with typical antipsychotics. This study did not assess whether patients had dementia or primary psychotic disorders.
In a larger retrospective study of 32,710 older persons with dementia, Herrmann’s group10 found no greater stroke risk in those who took atypicals than in those who took typical antipsychotics.
So the evidence for the risk of stroke in older patients who take antipsychotics is based on a few reports and no definitive studies.
Risk of early death
What about the risk of early death? After reviewing 17 clinical trials of atypical antipsychotics in older patients with dementia, the FDA issued its warning in April 2005 about increased mortality risk (see Related resources). Fifteen of the trials showed an increased mortality risk, resulting in an estimated 1.6- to 1.7-fold increase in risk of death, mostly by cardiac or infectious causes.
A year earlier, Straus et al11 reported on risk of sudden cardiac death with antipsychotic use in a population-based, case-control study in the Netherlands. In this longitudinal, observational database of 250,000 patients, 75% were age >65 and <1% had dementia. Current use of antipsychotics was associated with a threefold increase in risk of sudden cardiac death (554 cases), after other predictors of sudden death were factored in. This risk increased with higher antipsychotic dosages and was similarly elevated for patients with and without schizophrenia-related disorders.
Mechanisms unknown
By what mechanisms could antipsychotics precipitate stroke, sudden cardiac death, or pneumonia? A clear biological mechanism has not been proposed, much less proven. The risks seen in clinical trials—usually lasting 12 weeks or less—suggest an acute effect rather than the more-gradual consequences of weight gain, altered lipid metabolism, or diabetes.
Speculations range widely. Possibilities awaiting study include postural hypotension, altered platelet aggregation, increased venous thromboembolism, peripheral vasodilation leading to cardiovascular collapse, acute dystonia, acute cardiomyopathy, arrhythmias related to QT prolongation, and other forms of cardiac toxicity.10,11
Remaining questions
The few studies plus two FDA advisories force clinicians to make complex treatment decisions on insufficient evidence. Here’s what we don’t know:
- The magnitude of stroke or sudden death risk in older patients who take antipsychotics for any diagnosis. (All studies have limitations, and public health policy should not rely on one or two studies, no matter how good they may be.)
- Who is at higher or lower risk with antipsychotic use—men vs women? blacks vs whites?etc.
- Biological mechanisms of an association between antipsychotics and risks of stroke and premature death.
Strategies for reducing risk
We can minimize patients’ clinical risk and our legal risk only by using the limited evidence, expert consensus, and sound clinical judgment. Suggested strategies are listed in Table 2.
Table 2
Strategies to minimize antipsychotic risk in patients age 65 and older
| Review and document risk factors for cardiovascular disease—including stroke—with physical examination, laboratory tests (lipid profile, fasting glucose), and ECG in consultation with a primary care physician or specialist |
| Try nonpharmacologic approaches first whenever possible to manage behavioral disturbances in patients with dementia; document results before trying an antipsychotic |
| Review antipsychotics’ risks and benefits with patient and family |
| Use low dosages and increase gradually, as sudden death risk is dose-related |
| Monitor antipsychotic effectiveness, and discontinue trials of questionable benefit |
| Monitor cardiovascular symptoms, heart rate, blood pressure and body mass index of patients with cardiovascular risk |
| Avoid using sedating antipsychotics for insomnia in patients without psychiatric disorders |
Dr. Wulsin treats psychiatric outpatients and has published reviews on depression and heart disease. He is training director, University of Cincinnati family medicine-psychiatry residency program.
- Food and Drug Administration. Advisory on increased risk of mortality with use of atypical antipsychotics to treat behavioral disturbances in older patients with dementia. www.fda.gov/cder/drug/advisory/antipsychotics.htm.
Drug brand names
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Zimmermann U, Kraus T, Himmerich H, et al. Epidemiology, implications and mechanisms underlying drug-induced weight gain in psychiatric patients. J Psychiatr Res 2003;37(3):193-220.
2. Ryan MC, Thakore JH. Physical consequences of schizophrenia and its treatment: the metabolic syndrome. Life Sci 2002;71(3):239-57.
3. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA 2005;293(5):596-608.
4. Alexopoulos GS, Streim J, Carpenter D, Docherty JP. Using antipsychotic agents in older patients. J Clin Psychiatry 2004;65(suppl 2):5-99.
5. Schneider LS, Ismail MS, Dagerman K, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE): Alzheimer’s disease trial. Schizophr Bull 2003;29(1):57-72.
6. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
7. Wooltorton E. Risperidone (Risperdal): increased rate of cerebrovascular events in dementia trials. CMAJ 2002;167(11):1269-1270.
8. Herrmann N, Mamdani M, Lanctot KL. Atypical antipsychotics and risk of cerebrovascular accidents. Am J Psychiatry 2004;161(6):1113-1115.
9. Herrmann N, Lanctot KL. Do atypical antipsychotics cause stroke? CNS Drugs 2005;19(2):91-103.
10. Gill SS, Rochon PA, Herrmann N, et al. Atypical antipsychotic drugs and risk of ischaemic stroke: population based retrospective cohort study. BMJ 2005;330(7489):445.-
11. Straus SM, Bleumink GS, Dieleman JP, et al. Antipsychotics and the risk of sudden cardiac death. Arch Intern Med 2004;164(12):1293-7.
1. Zimmermann U, Kraus T, Himmerich H, et al. Epidemiology, implications and mechanisms underlying drug-induced weight gain in psychiatric patients. J Psychiatr Res 2003;37(3):193-220.
2. Ryan MC, Thakore JH. Physical consequences of schizophrenia and its treatment: the metabolic syndrome. Life Sci 2002;71(3):239-57.
3. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA 2005;293(5):596-608.
4. Alexopoulos GS, Streim J, Carpenter D, Docherty JP. Using antipsychotic agents in older patients. J Clin Psychiatry 2004;65(suppl 2):5-99.
5. Schneider LS, Ismail MS, Dagerman K, et al. Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE): Alzheimer’s disease trial. Schizophr Bull 2003;29(1):57-72.
6. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
7. Wooltorton E. Risperidone (Risperdal): increased rate of cerebrovascular events in dementia trials. CMAJ 2002;167(11):1269-1270.
8. Herrmann N, Mamdani M, Lanctot KL. Atypical antipsychotics and risk of cerebrovascular accidents. Am J Psychiatry 2004;161(6):1113-1115.
9. Herrmann N, Lanctot KL. Do atypical antipsychotics cause stroke? CNS Drugs 2005;19(2):91-103.
10. Gill SS, Rochon PA, Herrmann N, et al. Atypical antipsychotic drugs and risk of ischaemic stroke: population based retrospective cohort study. BMJ 2005;330(7489):445.-
11. Straus SM, Bleumink GS, Dieleman JP, et al. Antipsychotics and the risk of sudden cardiac death. Arch Intern Med 2004;164(12):1293-7.
Newly diagnosed hypertension and depressive symptoms: How would you treat?
Medical history
- No other significant medical or psychiatric problems
- Married, with 2 teenaged children
- Employed as an administrator for an insurance company (>50 hrs/wk)
- Drinks 3 to 4 alcoholic beverages/wk
- Does not smoke
- Enjoys fishing and other outdoor activities
- Both parents had hypertension; father also had peripheral vascular disease
Examination
- Patient is in no acute distress
- Approximately 30 pounds over ideal body weight
- Other vital signs are normal
- Normal retinal examination, no carotid bruits, and clear lungs. Cardiac rate and rhythm are regular; no abdominal bruits
- Laboratory studies reveal normal renal function; cholesterol, 184 mg/dL; low-density lipoprotein (LDL) cholesterol, 129 mg/dL; high-density lipoprotein (HDL) cholesterol, 55 mg/dL; triglycerides, 163 mg/dL. Electrocardiogram shows no current or prior evidence of ischemia or left-ventricular strain.
Additional information is required in a number of domains. Blood pressure readings should be repeated to make an accurate diagnosis of hypertension. While the patient may have hypertension, only a single blood pressure reading is elevated. The Joint National Committee on Blood Pressure (JNC 7) specifications1 state that 2 such readings on different days are needed to confirm a diagnosis of hypertension. The symptoms of claudication should be investigated. Physical examination should focus on auscultation for bruits and on the examination of eye grounds to further investigate the possibility of peripheral vascular disease (PVD). In addition, a lipid profile should be drawn. While guidelines are conflicting, consideration should be given to assessing a fasting glucose, potassium, and renal function. Other tests, such as a C-reactive protein, are more controversial.2
The patient opts for drug treatment of his hypertension, and begins taking atenolol 50 mg/d (in addition to aspirin 81 mg/d). He is scheduled to follow-up by phone in 1 week to assure compliance and in 3 months in the office.
On a return visit to the office 3 months later, the patient reports the recent onset of fatigue.
Q: What is the differential diagnosis of the patient’s symptoms? What additional information might you like to know? A:__________________________________
____________________________________
On further questioning he reports that he initially tolerated the beta-blocker without problem, but more recently has experienced low energy and poor sleep (with early morning awakening); he acknowledges decreases in libido, interest in pleasurable activities (eg, hunting, fishing), and his ability to concentrate. He has gained 5 to 10 pounds in the last month.
Although he denies feeling “sad,” he says his emotions seem “flat.” He denies having thoughts of suicide, increased anxiety, symptoms of hypomania, or psychotic symptoms. He describes a mild increase in stress at work, and he feels that the process of preparing for his son to go to college had been “a big burden.” He says there are no other stressors.
The patient’s alcohol use has not changed significantly, and he reports being compliant with his new medication regimen.
When his father died 6 years earlier, he experienced similar symptoms; at no other time have such symptoms occurred. The patient reports no other new physical symptoms, and his physical examination is essentially unchanged from the exam conducted 3 months earlier. His vital signs are normal, including a blood pressure of 128/84 mm Hg.
Consider the differential diagnosis of the patient’s abnormal mood and neurovegetative symptoms. In the primary care setting, the differential diagnosis of depressed mood is broad (Table 1 ), including medical disorders and a variety of psychiatric syndromes.
Medical conditions to consider include a medication induced side effect, hypothyroidism (a metabolic masquerader of depression), anemia, sleep disorder (eg, sleep apnea), and alcohol abuse. PVD should also be considered—his symptoms may be secondary to poor perfusion of the cerebral cortex.
TABLE 1
Partial differential diagnosis of depressed mood and neurovegetative symptoms
| General medical conditions |
| Endocrine: hypothyroidism, Cushing’s syndrome |
| Hematologic: anemia |
| Nutritional: vitamin B12 deficiency |
| Neurologic: movement disorders (eg, Parkinson’s disease, Huntington’s disease), head trauma, seizure disorders |
| Vascular: peripheral vascular disease, cerebrovascular accident |
| Sleep disorders: sleep apnea, narcolepsy |
| Neoplastic: pancreatic, lung, central nervous system neoplasms |
| Substance abuse disorders |
| Alcohol, benzodiazepine, or barbiturate dependence |
| Cocaine or amphetamine withdrawal |
| Psychiatric disorders |
| Major depressive disorder |
| Dysthymia |
| Adjustment disorder with depressed mood |
| Bipolar disorder |
What effects might beta-blockers be having on his mood, energy level, and libido?
You call a psychiatrist colleague for an informal consultation.
Psychiatrist’s comments
It is important to distinguish major depression from other, less severe depressive syndromes. In major depression, 5 out of 9 symptoms (including depressed mood or anhedonia) are present most of the day nearly every day for 2 weeks.
With adjustment disorder and so-called minor depression, symptoms are fewer or less persistent (Table 2).
This distinction is important, as antidepressants are effective for major depression, but they have not yet been shown effective for adjustment disorders or minor depression. Major depression is the “hypertension of mental illness in primary care”—common, often undiagnosed, and associated with poor outcomes. Therefore, accurate diagnosis and appropriate treatment for major depression are essential.
Given the possibility of a depressive syndrome, gather further information to determine the duration of ongoing symptoms, and obtain answers to a short questionnaire (eg, the Beck Depression Inventory [BDI]3 or the PHQ-94). Elicit a family history of mood disorder, or personal history suggestive of thyroid dysfunction, a sleep disorder, or alcohol or drug abuse. Order a complete blood count (CBC) to evaluate for anemia, a thyroid-stimulating hormone (TSH) to evaluate for hypothyroidism, and, if indicated by history, a sleep study.
Beta-blockers and depression. The patient’s symptoms developed in the context of beta-blocker therapy. From the 1970s through the 1990s, the lore was that beta-blockers caused depression and should be avoided in patients with a history of depression. Because of this, many patients with myocardial infarction (MI) and congestive heart failure (CHF) have been denied treatment with beta-blockers when otherwise indicated.
Fortunately, a recent rigorous academic study of this issue was conducted by Ko and colleagues5 to rationally guide treatment. This study involved a meta-analysis of 15 randomized controlled trials of beta-blocker therapy in patients with MI, CHF, or hypertension; the authors found that beta-blockers were associated with a slight (though statistically significant) increase in fatigue and sexual dysfunction, and that their use was not associated with depressive symptoms. This is the best review to date of beta-blockers and depression, and it debunks the myth that beta-blockers cause depression—a myth that has prevented many post-MI patients from receiving much-needed beta-blocker therapy. In short, although idiosyncratic reactions are possible, it is unlikely the patient’s use of atenolol caused his apparent depressive symptoms.
TABLE 2
Major depression, minor depression, and adjustment disorder
| Major depressive disorder |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 5 (out of 9) depressive symptoms, and resulting in functional impairment. |
| Minor depression (research criteria) |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 2 to 4 depressive symptoms, and without history of major depressive disorder. |
| Adjustment disorder |
| Mood or anxiety symptoms occur within 3 months of a stressful life event. Such symptoms are in excess of the symptoms that would normally be expected as a result of the event or impair function. The symptoms do not meet criteria for major depressive disorder, bereavement, or another major psychiatric disorder. |
| Source: Adapted from DSM-IV.14 |
Further primary care evaluation
The patient has no cold intolerance or other symptoms of thyroid dysfunction. He does report a long history of snoring, confirmed by his wife. However, he did not notice feeling more fatigued after starting atenolol.Nonetheless, you switch his antihypertensive medication from atenolol to hydrochlorothiazide. In addition, you order a CBC, serum chemistries, a thyroid panel, and a sleep study. The patient is told to return for a follow-up appointment in 2 weeks and to call before that if symptoms worsen.
A:_______________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
In this situation, the evidence (depressive symptoms in the context of good blood-pressure control) was insufficient to justify a switch from a beta-blocker to hydrochlorothiazide. One could argue that the switch was reasonable regardless of his depressive symptoms; the most recent guidelines from JNC 71 indicate that thiazide diuretics are first-line therapy for hypertension in patients without CAD, and that beta-blockers are not the first-line agent in the patient’s clinical situation.
But discontinuing atenolol because of ongoing depressive symptoms is not supported. The patient may well need a beta-blocker in the future (eg, if he were to develop CAD). By prematurely concluding that the beta-blocker caused adverse effects, we may be denying him an important treatment down the road.
Option 1: 2-week drug holiday
If there was concern that the patient was having an idiosyncratic reaction to atenolol, or if he developed substantial fatigue or sexual dysfunction, a 2-week drug holiday could be conducted while carefully monitoring blood pressure and depressive symptoms. Atenolol could then be restarted to identify a temporal relationship between the symptoms and the medication.
Option 2: Treat for depression
Another option would be to treat the patient as if his symptoms represented depression. Exhibiting 4 of the necessary diagnostic criteria, the patient nearly qualifies for a diagnosis of current major depression. An antidepressant could be started, exercise could be prescribed, or a referral could be made for psychotherapy. However, again there is insufficient evidence that his subsyndromal depression will respond to standard treatments designed for major depressive disorder.
The patient returns as scheduled 2 weeks later. He has tolerated the change in blood pressure medications without difficulty, but he is experiencing persistent anhedonia, terminal insomnia, and low levels of concentration, energy, and libido. He has felt increasingly hopeless and worthless over the past 2 weeks, though he denies having thoughts of suicide. Results on CBC, serum chemistries, thyroid panel, and sleep study are all unremarkable.
The patient now clearly meets criteria for a major depressive episode. As a first step, he should be educated about depression. An excellent self-help book is Getting Your Life Back by Wright and Basco.6 The patient should be taught to monitor his symptoms with the BDI3 or the PHQ-94 to better assess the severity of the current episode, to monitor changes in his symptoms, and to rapidly identify relapses.
Most physicians would start an antidepressant, unless the patient had significant objections. Other treatment options, alone or in concert with antidepressant treatment, include exercise or psychotherapy. The patient is an excellent candidate for exercise, given that he has 3 risk factors for CAD: hypertension, a sedentary lifestyle, and obesity (4, if you include depression). Exercising for at least 30 minutes, 2 to 3 times per week, would likely benefit his physical and mental health. In addition to its cardiac benefits, exercise 3 times weekly was found in at least one trial to be as effective as sertraline in treating major depression in outpatients.7
Choosing an antidepressant. A number of factors should be considered in choosing antidepressants, including efficacy, side effect profile, and cost. Table 3 outlines some of the main considerations in the choice of antidepressants for this patient. Note that tricyclic antidepressants are not listed, being contraindicated in CAD because of their tendency to contribute to arrhythmias in the post-MI period. In this patient’s case, mirtazapine should be avoided because of the possibility of weight gain; venlafaxine should be avoided because of hypertension. Sertraline would be an appropriate choice, given that it has been relatively well-studied in persons with CAD.
The patient begins treatment with fluoxetine (10 mg/d, which is then increased to 20 mg/d after several days). His depressive symptoms gradually diminish; he achieves a “50%” reduction of symptoms at follow-up visit 3 weeks later. Two months after fluoxetine was initiated, the patient is nearly euthymic, reporting only 2 depressive symptoms, and is again engaging in usual recreational activities.
TABLE 3
A comparison of antidepressants in the treatment of depressed patients in cardiac populations
| Medication | Class/mechanism | Risks/side effects | Benefits |
| Citalopram | SSRI | Low cost, minimal drug-drug interactions | |
| Escitalopram | SSRI | Newest/least studied agent | Low cost, minimal drug-drug interactions, possibly faster onset and fewer side effects |
| Fluoxetine | SSRI | Long half-life, more drug-drug interactions | |
| Paroxetine | SSRI | Sedation, mild anticholinergic effects | |
| Sertraline | SSRI | Sedation, mild | Best studied in CAD; few drug interactions |
| Mirtazapine | Atypical antidepressant (5HT2, 5HT3, and alpha2 refceptor blockade) | Sedation, weight gain, possible elevation of lipids | No sexual dysfunction |
| Venlafaxine | Selective serotonin and norepinephrine receptor blockade | Elevated blood pressure in 13% at doses of 300 mg or greater | |
| Bupropion | Increases noradrenergic and dopaminergic activity | Initial anxiety | No sexual dysfunction |
| SSRI, selective serotonin reuptake inhibitor; CAD, coronary artery disease | |||
Q: Is depression, like hypertension, a risk factor for the development of coronary artery disease (CAD)? A:____________________________________________________ _____________________________________________________ _____________________________________________________
Whether depression is a risk factor for CAD depends on how one defines a risk factor and whether one is discussing “major” or “minor” risk factors. At least 15 narrative reviews have been written on the relationship between depression and heart disease, but none has examined the epidemiologic evidence for depression as a major risk factor for CAD (Table 4).8
In looking at the 7 main epidemiologic criteria for a risk factor, depression does very well on 4: strength of association, consistency, dose-response effect, and predictability. Numerous studies have shown that depression is clearly and consistently associated with the development of CAD, and that clinical depression appears to predict CAD more robustly than does depressed mood alone.9-12
On 2 of the criteria, specificity and biological plausibility, there is fair evidence for depression as a CAD risk factor. We do not yet know the relative importance of recurrent major depression, dysthymia, BDI scores of 10 or greater, or some other marker of depression as predictors of CAD.
Because mild depressive symptoms may predict CAD, it is unclear what levels of depression increase the risk of CAD and require intervention. Excellent work exists regarding the development of plausible mechanisms by which depression may lead to CAD; however, these mechanisms have yet to be proven. Therefore, the evidence in this domain can only be rated as fair.
Finally, the evidence is incomplete for one important criterion: response to treatment. Only one study has been designed to examine the effect of depression treatments on cardiac risk reduction. This study (the ENRICHD trial13) was a treatment study of post-MI depression that found that cognitive-behavioral therapy did not have a significant impact on reducing recurrent cardiac events.
Based on the most stringent epidemiologic criteria, depression is almost, but not quite, a risk factor for CAD. However, depression is a minor risk factor for CAD, and may someday be considered a major risk factor. While the mechanisms by which depression may lead to CAD have not yet been established, the association between depression and subsequent CAD likely occurs via 2 pathways.
The first pathway is behavioral. Patients with depression have diminished self-care, possibly increasing other CAD risk factors such as smoking, poor diet/hyperlipidemia, diabetes, physical inactivity, and obesity.
The second pathway by which depression may lead to CAD is neuroendocrine. Hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis and hyperactive sympathomedullary activity may result in elevated cytokine levels, platelet activation, and vascular damage, thereby contributing to CAD.8
TABLE 4
Depression as a risk factor for CAD: a “report card”8
| Risk factor | Strength of evidence |
| Strength of association | Good |
| Predictability | Good |
| Specificity | Fair |
| Consistency | Good |
| Dose-response effect | Good |
| Biological plausibility | Fair |
| Response to treatment | Incomplete |
This case illustrates several important points in the management of depressive symptoms in the family practice setting.
First, patients may present with subsyndromal depressive illness; there is, as yet, no evidence that antidepressants are beneficial in this population, and they expose patients to side effects such as sexual dysfunction.
Second, practitioners in general should not shy away from using beta-blockers where indicated for patients with cardiovascular disease and depression; the link between beta-blockers and depression seems minimal at best.
Third, when patients do present with the syndrome of major depression, it is important to evaluate potential medical contributors (eg, obstructive sleep apnea) when appropriate, and to treat with adequate doses of antidepressants for an adequate duration.
Fourth, the potential effects of depression on the development of CAD give family physicians yet another reason to remain vigilant for the presence of depression in all patients.
Should the FP treat independently? This discussion then leads to the question of when an informal or formal psychiatric consultation is indicated for the treatment of a depressed patient, and when the FP may wish to handle the case independently. The short answer is, of course, “it depends.” As with all areas of medical specialty, FPs will have varying levels of comfort, knowledge, and experience in the treatment of psychiatric disorders, and this will often affect the threshold for obtaining consultation. Furthermore, the number of psychiatric consultants—and thus the opportunity for consultations—varies widely depending on practice location.
Value of informal consultations. In general, FPs are well-equipped to handle patients with uncomplicated major depressive disorder or dysthymia without suicidal ideation or psychotic features. Informal consultation may be useful in cases (as in this case) when it is difficult to distinguish whether the patient meets criteria for major depressive disorder (and therefore requires treatment) or has subthreshold depressive symptoms. In addition, informal consultation can be useful when there is a question about antidepressant agent selection in a specific clinical situation. Finally, informal consultation may be of benefit when there are comorbid psychiatric illnesses, for example, coexisting panic disorder, generalized anxiety disorder, and major depressive disorder.
Opting for formal consultation. Formal psychiatric consultation is often useful when there is a mood disorder with suicidal ideation or psychotic features, when the disorder has been refractory to 2 or more adequate trials of an antidepressant, when there is a question of bipolar disorder (for which monotherapy with antidepressants is contraindicated) or substance use disorder, or for progressively worsening depression despite treatment.
Billing and coding. The logistics of billing for the treatment of comorbid psychiatric disorders by primary care physicians vary with the type of payer and from state to state. Because it is often impractical to modify billing procedures with each patient, it is useful for each practice to develop general billing guidelines for psychiatric disorders billed to Medicaid, Medicare, and the most common managed care organizations in the practice. In general, the physician caring for the patient described in this report would bill for hypertension and depression and get paid under the primary diagnosis of hypertension. When in doubt about whether to bill for a psychiatric disorder, primary care clinicians may include the relevant physical symptom in the billing codes, such as fatigue, headache, insomnia and bill under that code.
· Acknowledgments ·
Portions of this article were presented at the Association of Medicine and Psychiatry Annual Meeting, San Diego, California, November 19, 2003.
1. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Detection, Evaluation, and Treatment of High Blood Report of the Joint National Committee on Prevention, Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
2. Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 2004;350:1387-1397.
3. Beck AT. Beck Depression Inventory. In: Test Critiques, Vol II,. Deyser DJ, Sweetland RC (eds). Kansas City, Mo: Test Corporation of America; 1985;83-87.
4. Spitzer RL, Kroenke K, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-613.
5. Ko DT, Hebert PR, Coffey CS, et al. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA. 2002;288:351-357.
6. Basco MR, Wright JH. Getting Your Life Back: The complete Guide to Recovery from Depression. New York: Touchstone; 2002;
7. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159:2349-2356.
8. Wulsin LR. Is depression a major risk factor for coronary disease? A systematic review of the epidemiologic evidence. Harv Rev Psychiatry. 2004;12:79-93.
9. Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol. 1996;78:613-617.
10. Anda R, Williamson D, Jones D, et al. Depressed affect, hopelessness, and the risk of ischemic heart disease in a cohort of U.S. adults. Epidemiology 1993;4:285-294.
11. Ford DE, Mead LA, Chang PF, et al. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med. 1998;158:1422-1426.
12. Rugulies R. Depression as a predictor for coronary heart disease. a review and meta-analysis. Am J Prev Med 2002;23:51-61.
13. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed.Washington, DC: American Psychiatric Press; 1994.
Drug brand names
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Hydrochlorothiazide • Esidrix, HydroDIURIL, Oretic
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Medical history
- No other significant medical or psychiatric problems
- Married, with 2 teenaged children
- Employed as an administrator for an insurance company (>50 hrs/wk)
- Drinks 3 to 4 alcoholic beverages/wk
- Does not smoke
- Enjoys fishing and other outdoor activities
- Both parents had hypertension; father also had peripheral vascular disease
Examination
- Patient is in no acute distress
- Approximately 30 pounds over ideal body weight
- Other vital signs are normal
- Normal retinal examination, no carotid bruits, and clear lungs. Cardiac rate and rhythm are regular; no abdominal bruits
- Laboratory studies reveal normal renal function; cholesterol, 184 mg/dL; low-density lipoprotein (LDL) cholesterol, 129 mg/dL; high-density lipoprotein (HDL) cholesterol, 55 mg/dL; triglycerides, 163 mg/dL. Electrocardiogram shows no current or prior evidence of ischemia or left-ventricular strain.
Additional information is required in a number of domains. Blood pressure readings should be repeated to make an accurate diagnosis of hypertension. While the patient may have hypertension, only a single blood pressure reading is elevated. The Joint National Committee on Blood Pressure (JNC 7) specifications1 state that 2 such readings on different days are needed to confirm a diagnosis of hypertension. The symptoms of claudication should be investigated. Physical examination should focus on auscultation for bruits and on the examination of eye grounds to further investigate the possibility of peripheral vascular disease (PVD). In addition, a lipid profile should be drawn. While guidelines are conflicting, consideration should be given to assessing a fasting glucose, potassium, and renal function. Other tests, such as a C-reactive protein, are more controversial.2
The patient opts for drug treatment of his hypertension, and begins taking atenolol 50 mg/d (in addition to aspirin 81 mg/d). He is scheduled to follow-up by phone in 1 week to assure compliance and in 3 months in the office.
On a return visit to the office 3 months later, the patient reports the recent onset of fatigue.
Q: What is the differential diagnosis of the patient’s symptoms? What additional information might you like to know? A:__________________________________
____________________________________
On further questioning he reports that he initially tolerated the beta-blocker without problem, but more recently has experienced low energy and poor sleep (with early morning awakening); he acknowledges decreases in libido, interest in pleasurable activities (eg, hunting, fishing), and his ability to concentrate. He has gained 5 to 10 pounds in the last month.
Although he denies feeling “sad,” he says his emotions seem “flat.” He denies having thoughts of suicide, increased anxiety, symptoms of hypomania, or psychotic symptoms. He describes a mild increase in stress at work, and he feels that the process of preparing for his son to go to college had been “a big burden.” He says there are no other stressors.
The patient’s alcohol use has not changed significantly, and he reports being compliant with his new medication regimen.
When his father died 6 years earlier, he experienced similar symptoms; at no other time have such symptoms occurred. The patient reports no other new physical symptoms, and his physical examination is essentially unchanged from the exam conducted 3 months earlier. His vital signs are normal, including a blood pressure of 128/84 mm Hg.
Consider the differential diagnosis of the patient’s abnormal mood and neurovegetative symptoms. In the primary care setting, the differential diagnosis of depressed mood is broad (Table 1 ), including medical disorders and a variety of psychiatric syndromes.
Medical conditions to consider include a medication induced side effect, hypothyroidism (a metabolic masquerader of depression), anemia, sleep disorder (eg, sleep apnea), and alcohol abuse. PVD should also be considered—his symptoms may be secondary to poor perfusion of the cerebral cortex.
TABLE 1
Partial differential diagnosis of depressed mood and neurovegetative symptoms
| General medical conditions |
| Endocrine: hypothyroidism, Cushing’s syndrome |
| Hematologic: anemia |
| Nutritional: vitamin B12 deficiency |
| Neurologic: movement disorders (eg, Parkinson’s disease, Huntington’s disease), head trauma, seizure disorders |
| Vascular: peripheral vascular disease, cerebrovascular accident |
| Sleep disorders: sleep apnea, narcolepsy |
| Neoplastic: pancreatic, lung, central nervous system neoplasms |
| Substance abuse disorders |
| Alcohol, benzodiazepine, or barbiturate dependence |
| Cocaine or amphetamine withdrawal |
| Psychiatric disorders |
| Major depressive disorder |
| Dysthymia |
| Adjustment disorder with depressed mood |
| Bipolar disorder |
What effects might beta-blockers be having on his mood, energy level, and libido?
You call a psychiatrist colleague for an informal consultation.
Psychiatrist’s comments
It is important to distinguish major depression from other, less severe depressive syndromes. In major depression, 5 out of 9 symptoms (including depressed mood or anhedonia) are present most of the day nearly every day for 2 weeks.
With adjustment disorder and so-called minor depression, symptoms are fewer or less persistent (Table 2).
This distinction is important, as antidepressants are effective for major depression, but they have not yet been shown effective for adjustment disorders or minor depression. Major depression is the “hypertension of mental illness in primary care”—common, often undiagnosed, and associated with poor outcomes. Therefore, accurate diagnosis and appropriate treatment for major depression are essential.
Given the possibility of a depressive syndrome, gather further information to determine the duration of ongoing symptoms, and obtain answers to a short questionnaire (eg, the Beck Depression Inventory [BDI]3 or the PHQ-94). Elicit a family history of mood disorder, or personal history suggestive of thyroid dysfunction, a sleep disorder, or alcohol or drug abuse. Order a complete blood count (CBC) to evaluate for anemia, a thyroid-stimulating hormone (TSH) to evaluate for hypothyroidism, and, if indicated by history, a sleep study.
Beta-blockers and depression. The patient’s symptoms developed in the context of beta-blocker therapy. From the 1970s through the 1990s, the lore was that beta-blockers caused depression and should be avoided in patients with a history of depression. Because of this, many patients with myocardial infarction (MI) and congestive heart failure (CHF) have been denied treatment with beta-blockers when otherwise indicated.
Fortunately, a recent rigorous academic study of this issue was conducted by Ko and colleagues5 to rationally guide treatment. This study involved a meta-analysis of 15 randomized controlled trials of beta-blocker therapy in patients with MI, CHF, or hypertension; the authors found that beta-blockers were associated with a slight (though statistically significant) increase in fatigue and sexual dysfunction, and that their use was not associated with depressive symptoms. This is the best review to date of beta-blockers and depression, and it debunks the myth that beta-blockers cause depression—a myth that has prevented many post-MI patients from receiving much-needed beta-blocker therapy. In short, although idiosyncratic reactions are possible, it is unlikely the patient’s use of atenolol caused his apparent depressive symptoms.
TABLE 2
Major depression, minor depression, and adjustment disorder
| Major depressive disorder |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 5 (out of 9) depressive symptoms, and resulting in functional impairment. |
| Minor depression (research criteria) |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 2 to 4 depressive symptoms, and without history of major depressive disorder. |
| Adjustment disorder |
| Mood or anxiety symptoms occur within 3 months of a stressful life event. Such symptoms are in excess of the symptoms that would normally be expected as a result of the event or impair function. The symptoms do not meet criteria for major depressive disorder, bereavement, or another major psychiatric disorder. |
| Source: Adapted from DSM-IV.14 |
Further primary care evaluation
The patient has no cold intolerance or other symptoms of thyroid dysfunction. He does report a long history of snoring, confirmed by his wife. However, he did not notice feeling more fatigued after starting atenolol.Nonetheless, you switch his antihypertensive medication from atenolol to hydrochlorothiazide. In addition, you order a CBC, serum chemistries, a thyroid panel, and a sleep study. The patient is told to return for a follow-up appointment in 2 weeks and to call before that if symptoms worsen.
A:_______________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
In this situation, the evidence (depressive symptoms in the context of good blood-pressure control) was insufficient to justify a switch from a beta-blocker to hydrochlorothiazide. One could argue that the switch was reasonable regardless of his depressive symptoms; the most recent guidelines from JNC 71 indicate that thiazide diuretics are first-line therapy for hypertension in patients without CAD, and that beta-blockers are not the first-line agent in the patient’s clinical situation.
But discontinuing atenolol because of ongoing depressive symptoms is not supported. The patient may well need a beta-blocker in the future (eg, if he were to develop CAD). By prematurely concluding that the beta-blocker caused adverse effects, we may be denying him an important treatment down the road.
Option 1: 2-week drug holiday
If there was concern that the patient was having an idiosyncratic reaction to atenolol, or if he developed substantial fatigue or sexual dysfunction, a 2-week drug holiday could be conducted while carefully monitoring blood pressure and depressive symptoms. Atenolol could then be restarted to identify a temporal relationship between the symptoms and the medication.
Option 2: Treat for depression
Another option would be to treat the patient as if his symptoms represented depression. Exhibiting 4 of the necessary diagnostic criteria, the patient nearly qualifies for a diagnosis of current major depression. An antidepressant could be started, exercise could be prescribed, or a referral could be made for psychotherapy. However, again there is insufficient evidence that his subsyndromal depression will respond to standard treatments designed for major depressive disorder.
The patient returns as scheduled 2 weeks later. He has tolerated the change in blood pressure medications without difficulty, but he is experiencing persistent anhedonia, terminal insomnia, and low levels of concentration, energy, and libido. He has felt increasingly hopeless and worthless over the past 2 weeks, though he denies having thoughts of suicide. Results on CBC, serum chemistries, thyroid panel, and sleep study are all unremarkable.
The patient now clearly meets criteria for a major depressive episode. As a first step, he should be educated about depression. An excellent self-help book is Getting Your Life Back by Wright and Basco.6 The patient should be taught to monitor his symptoms with the BDI3 or the PHQ-94 to better assess the severity of the current episode, to monitor changes in his symptoms, and to rapidly identify relapses.
Most physicians would start an antidepressant, unless the patient had significant objections. Other treatment options, alone or in concert with antidepressant treatment, include exercise or psychotherapy. The patient is an excellent candidate for exercise, given that he has 3 risk factors for CAD: hypertension, a sedentary lifestyle, and obesity (4, if you include depression). Exercising for at least 30 minutes, 2 to 3 times per week, would likely benefit his physical and mental health. In addition to its cardiac benefits, exercise 3 times weekly was found in at least one trial to be as effective as sertraline in treating major depression in outpatients.7
Choosing an antidepressant. A number of factors should be considered in choosing antidepressants, including efficacy, side effect profile, and cost. Table 3 outlines some of the main considerations in the choice of antidepressants for this patient. Note that tricyclic antidepressants are not listed, being contraindicated in CAD because of their tendency to contribute to arrhythmias in the post-MI period. In this patient’s case, mirtazapine should be avoided because of the possibility of weight gain; venlafaxine should be avoided because of hypertension. Sertraline would be an appropriate choice, given that it has been relatively well-studied in persons with CAD.
The patient begins treatment with fluoxetine (10 mg/d, which is then increased to 20 mg/d after several days). His depressive symptoms gradually diminish; he achieves a “50%” reduction of symptoms at follow-up visit 3 weeks later. Two months after fluoxetine was initiated, the patient is nearly euthymic, reporting only 2 depressive symptoms, and is again engaging in usual recreational activities.
TABLE 3
A comparison of antidepressants in the treatment of depressed patients in cardiac populations
| Medication | Class/mechanism | Risks/side effects | Benefits |
| Citalopram | SSRI | Low cost, minimal drug-drug interactions | |
| Escitalopram | SSRI | Newest/least studied agent | Low cost, minimal drug-drug interactions, possibly faster onset and fewer side effects |
| Fluoxetine | SSRI | Long half-life, more drug-drug interactions | |
| Paroxetine | SSRI | Sedation, mild anticholinergic effects | |
| Sertraline | SSRI | Sedation, mild | Best studied in CAD; few drug interactions |
| Mirtazapine | Atypical antidepressant (5HT2, 5HT3, and alpha2 refceptor blockade) | Sedation, weight gain, possible elevation of lipids | No sexual dysfunction |
| Venlafaxine | Selective serotonin and norepinephrine receptor blockade | Elevated blood pressure in 13% at doses of 300 mg or greater | |
| Bupropion | Increases noradrenergic and dopaminergic activity | Initial anxiety | No sexual dysfunction |
| SSRI, selective serotonin reuptake inhibitor; CAD, coronary artery disease | |||
Q: Is depression, like hypertension, a risk factor for the development of coronary artery disease (CAD)? A:____________________________________________________ _____________________________________________________ _____________________________________________________
Whether depression is a risk factor for CAD depends on how one defines a risk factor and whether one is discussing “major” or “minor” risk factors. At least 15 narrative reviews have been written on the relationship between depression and heart disease, but none has examined the epidemiologic evidence for depression as a major risk factor for CAD (Table 4).8
In looking at the 7 main epidemiologic criteria for a risk factor, depression does very well on 4: strength of association, consistency, dose-response effect, and predictability. Numerous studies have shown that depression is clearly and consistently associated with the development of CAD, and that clinical depression appears to predict CAD more robustly than does depressed mood alone.9-12
On 2 of the criteria, specificity and biological plausibility, there is fair evidence for depression as a CAD risk factor. We do not yet know the relative importance of recurrent major depression, dysthymia, BDI scores of 10 or greater, or some other marker of depression as predictors of CAD.
Because mild depressive symptoms may predict CAD, it is unclear what levels of depression increase the risk of CAD and require intervention. Excellent work exists regarding the development of plausible mechanisms by which depression may lead to CAD; however, these mechanisms have yet to be proven. Therefore, the evidence in this domain can only be rated as fair.
Finally, the evidence is incomplete for one important criterion: response to treatment. Only one study has been designed to examine the effect of depression treatments on cardiac risk reduction. This study (the ENRICHD trial13) was a treatment study of post-MI depression that found that cognitive-behavioral therapy did not have a significant impact on reducing recurrent cardiac events.
Based on the most stringent epidemiologic criteria, depression is almost, but not quite, a risk factor for CAD. However, depression is a minor risk factor for CAD, and may someday be considered a major risk factor. While the mechanisms by which depression may lead to CAD have not yet been established, the association between depression and subsequent CAD likely occurs via 2 pathways.
The first pathway is behavioral. Patients with depression have diminished self-care, possibly increasing other CAD risk factors such as smoking, poor diet/hyperlipidemia, diabetes, physical inactivity, and obesity.
The second pathway by which depression may lead to CAD is neuroendocrine. Hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis and hyperactive sympathomedullary activity may result in elevated cytokine levels, platelet activation, and vascular damage, thereby contributing to CAD.8
TABLE 4
Depression as a risk factor for CAD: a “report card”8
| Risk factor | Strength of evidence |
| Strength of association | Good |
| Predictability | Good |
| Specificity | Fair |
| Consistency | Good |
| Dose-response effect | Good |
| Biological plausibility | Fair |
| Response to treatment | Incomplete |
This case illustrates several important points in the management of depressive symptoms in the family practice setting.
First, patients may present with subsyndromal depressive illness; there is, as yet, no evidence that antidepressants are beneficial in this population, and they expose patients to side effects such as sexual dysfunction.
Second, practitioners in general should not shy away from using beta-blockers where indicated for patients with cardiovascular disease and depression; the link between beta-blockers and depression seems minimal at best.
Third, when patients do present with the syndrome of major depression, it is important to evaluate potential medical contributors (eg, obstructive sleep apnea) when appropriate, and to treat with adequate doses of antidepressants for an adequate duration.
Fourth, the potential effects of depression on the development of CAD give family physicians yet another reason to remain vigilant for the presence of depression in all patients.
Should the FP treat independently? This discussion then leads to the question of when an informal or formal psychiatric consultation is indicated for the treatment of a depressed patient, and when the FP may wish to handle the case independently. The short answer is, of course, “it depends.” As with all areas of medical specialty, FPs will have varying levels of comfort, knowledge, and experience in the treatment of psychiatric disorders, and this will often affect the threshold for obtaining consultation. Furthermore, the number of psychiatric consultants—and thus the opportunity for consultations—varies widely depending on practice location.
Value of informal consultations. In general, FPs are well-equipped to handle patients with uncomplicated major depressive disorder or dysthymia without suicidal ideation or psychotic features. Informal consultation may be useful in cases (as in this case) when it is difficult to distinguish whether the patient meets criteria for major depressive disorder (and therefore requires treatment) or has subthreshold depressive symptoms. In addition, informal consultation can be useful when there is a question about antidepressant agent selection in a specific clinical situation. Finally, informal consultation may be of benefit when there are comorbid psychiatric illnesses, for example, coexisting panic disorder, generalized anxiety disorder, and major depressive disorder.
Opting for formal consultation. Formal psychiatric consultation is often useful when there is a mood disorder with suicidal ideation or psychotic features, when the disorder has been refractory to 2 or more adequate trials of an antidepressant, when there is a question of bipolar disorder (for which monotherapy with antidepressants is contraindicated) or substance use disorder, or for progressively worsening depression despite treatment.
Billing and coding. The logistics of billing for the treatment of comorbid psychiatric disorders by primary care physicians vary with the type of payer and from state to state. Because it is often impractical to modify billing procedures with each patient, it is useful for each practice to develop general billing guidelines for psychiatric disorders billed to Medicaid, Medicare, and the most common managed care organizations in the practice. In general, the physician caring for the patient described in this report would bill for hypertension and depression and get paid under the primary diagnosis of hypertension. When in doubt about whether to bill for a psychiatric disorder, primary care clinicians may include the relevant physical symptom in the billing codes, such as fatigue, headache, insomnia and bill under that code.
· Acknowledgments ·
Portions of this article were presented at the Association of Medicine and Psychiatry Annual Meeting, San Diego, California, November 19, 2003.
Medical history
- No other significant medical or psychiatric problems
- Married, with 2 teenaged children
- Employed as an administrator for an insurance company (>50 hrs/wk)
- Drinks 3 to 4 alcoholic beverages/wk
- Does not smoke
- Enjoys fishing and other outdoor activities
- Both parents had hypertension; father also had peripheral vascular disease
Examination
- Patient is in no acute distress
- Approximately 30 pounds over ideal body weight
- Other vital signs are normal
- Normal retinal examination, no carotid bruits, and clear lungs. Cardiac rate and rhythm are regular; no abdominal bruits
- Laboratory studies reveal normal renal function; cholesterol, 184 mg/dL; low-density lipoprotein (LDL) cholesterol, 129 mg/dL; high-density lipoprotein (HDL) cholesterol, 55 mg/dL; triglycerides, 163 mg/dL. Electrocardiogram shows no current or prior evidence of ischemia or left-ventricular strain.
Additional information is required in a number of domains. Blood pressure readings should be repeated to make an accurate diagnosis of hypertension. While the patient may have hypertension, only a single blood pressure reading is elevated. The Joint National Committee on Blood Pressure (JNC 7) specifications1 state that 2 such readings on different days are needed to confirm a diagnosis of hypertension. The symptoms of claudication should be investigated. Physical examination should focus on auscultation for bruits and on the examination of eye grounds to further investigate the possibility of peripheral vascular disease (PVD). In addition, a lipid profile should be drawn. While guidelines are conflicting, consideration should be given to assessing a fasting glucose, potassium, and renal function. Other tests, such as a C-reactive protein, are more controversial.2
The patient opts for drug treatment of his hypertension, and begins taking atenolol 50 mg/d (in addition to aspirin 81 mg/d). He is scheduled to follow-up by phone in 1 week to assure compliance and in 3 months in the office.
On a return visit to the office 3 months later, the patient reports the recent onset of fatigue.
Q: What is the differential diagnosis of the patient’s symptoms? What additional information might you like to know? A:__________________________________
____________________________________
On further questioning he reports that he initially tolerated the beta-blocker without problem, but more recently has experienced low energy and poor sleep (with early morning awakening); he acknowledges decreases in libido, interest in pleasurable activities (eg, hunting, fishing), and his ability to concentrate. He has gained 5 to 10 pounds in the last month.
Although he denies feeling “sad,” he says his emotions seem “flat.” He denies having thoughts of suicide, increased anxiety, symptoms of hypomania, or psychotic symptoms. He describes a mild increase in stress at work, and he feels that the process of preparing for his son to go to college had been “a big burden.” He says there are no other stressors.
The patient’s alcohol use has not changed significantly, and he reports being compliant with his new medication regimen.
When his father died 6 years earlier, he experienced similar symptoms; at no other time have such symptoms occurred. The patient reports no other new physical symptoms, and his physical examination is essentially unchanged from the exam conducted 3 months earlier. His vital signs are normal, including a blood pressure of 128/84 mm Hg.
Consider the differential diagnosis of the patient’s abnormal mood and neurovegetative symptoms. In the primary care setting, the differential diagnosis of depressed mood is broad (Table 1 ), including medical disorders and a variety of psychiatric syndromes.
Medical conditions to consider include a medication induced side effect, hypothyroidism (a metabolic masquerader of depression), anemia, sleep disorder (eg, sleep apnea), and alcohol abuse. PVD should also be considered—his symptoms may be secondary to poor perfusion of the cerebral cortex.
TABLE 1
Partial differential diagnosis of depressed mood and neurovegetative symptoms
| General medical conditions |
| Endocrine: hypothyroidism, Cushing’s syndrome |
| Hematologic: anemia |
| Nutritional: vitamin B12 deficiency |
| Neurologic: movement disorders (eg, Parkinson’s disease, Huntington’s disease), head trauma, seizure disorders |
| Vascular: peripheral vascular disease, cerebrovascular accident |
| Sleep disorders: sleep apnea, narcolepsy |
| Neoplastic: pancreatic, lung, central nervous system neoplasms |
| Substance abuse disorders |
| Alcohol, benzodiazepine, or barbiturate dependence |
| Cocaine or amphetamine withdrawal |
| Psychiatric disorders |
| Major depressive disorder |
| Dysthymia |
| Adjustment disorder with depressed mood |
| Bipolar disorder |
What effects might beta-blockers be having on his mood, energy level, and libido?
You call a psychiatrist colleague for an informal consultation.
Psychiatrist’s comments
It is important to distinguish major depression from other, less severe depressive syndromes. In major depression, 5 out of 9 symptoms (including depressed mood or anhedonia) are present most of the day nearly every day for 2 weeks.
With adjustment disorder and so-called minor depression, symptoms are fewer or less persistent (Table 2).
This distinction is important, as antidepressants are effective for major depression, but they have not yet been shown effective for adjustment disorders or minor depression. Major depression is the “hypertension of mental illness in primary care”—common, often undiagnosed, and associated with poor outcomes. Therefore, accurate diagnosis and appropriate treatment for major depression are essential.
Given the possibility of a depressive syndrome, gather further information to determine the duration of ongoing symptoms, and obtain answers to a short questionnaire (eg, the Beck Depression Inventory [BDI]3 or the PHQ-94). Elicit a family history of mood disorder, or personal history suggestive of thyroid dysfunction, a sleep disorder, or alcohol or drug abuse. Order a complete blood count (CBC) to evaluate for anemia, a thyroid-stimulating hormone (TSH) to evaluate for hypothyroidism, and, if indicated by history, a sleep study.
Beta-blockers and depression. The patient’s symptoms developed in the context of beta-blocker therapy. From the 1970s through the 1990s, the lore was that beta-blockers caused depression and should be avoided in patients with a history of depression. Because of this, many patients with myocardial infarction (MI) and congestive heart failure (CHF) have been denied treatment with beta-blockers when otherwise indicated.
Fortunately, a recent rigorous academic study of this issue was conducted by Ko and colleagues5 to rationally guide treatment. This study involved a meta-analysis of 15 randomized controlled trials of beta-blocker therapy in patients with MI, CHF, or hypertension; the authors found that beta-blockers were associated with a slight (though statistically significant) increase in fatigue and sexual dysfunction, and that their use was not associated with depressive symptoms. This is the best review to date of beta-blockers and depression, and it debunks the myth that beta-blockers cause depression—a myth that has prevented many post-MI patients from receiving much-needed beta-blocker therapy. In short, although idiosyncratic reactions are possible, it is unlikely the patient’s use of atenolol caused his apparent depressive symptoms.
TABLE 2
Major depression, minor depression, and adjustment disorder
| Major depressive disorder |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 5 (out of 9) depressive symptoms, and resulting in functional impairment. |
| Minor depression (research criteria) |
| Requires depressed mood or loss of interest/pleasure (anhedonia) most of the day, nearly every day for 2 weeks, with a total of 2 to 4 depressive symptoms, and without history of major depressive disorder. |
| Adjustment disorder |
| Mood or anxiety symptoms occur within 3 months of a stressful life event. Such symptoms are in excess of the symptoms that would normally be expected as a result of the event or impair function. The symptoms do not meet criteria for major depressive disorder, bereavement, or another major psychiatric disorder. |
| Source: Adapted from DSM-IV.14 |
Further primary care evaluation
The patient has no cold intolerance or other symptoms of thyroid dysfunction. He does report a long history of snoring, confirmed by his wife. However, he did not notice feeling more fatigued after starting atenolol.Nonetheless, you switch his antihypertensive medication from atenolol to hydrochlorothiazide. In addition, you order a CBC, serum chemistries, a thyroid panel, and a sleep study. The patient is told to return for a follow-up appointment in 2 weeks and to call before that if symptoms worsen.
A:_______________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
In this situation, the evidence (depressive symptoms in the context of good blood-pressure control) was insufficient to justify a switch from a beta-blocker to hydrochlorothiazide. One could argue that the switch was reasonable regardless of his depressive symptoms; the most recent guidelines from JNC 71 indicate that thiazide diuretics are first-line therapy for hypertension in patients without CAD, and that beta-blockers are not the first-line agent in the patient’s clinical situation.
But discontinuing atenolol because of ongoing depressive symptoms is not supported. The patient may well need a beta-blocker in the future (eg, if he were to develop CAD). By prematurely concluding that the beta-blocker caused adverse effects, we may be denying him an important treatment down the road.
Option 1: 2-week drug holiday
If there was concern that the patient was having an idiosyncratic reaction to atenolol, or if he developed substantial fatigue or sexual dysfunction, a 2-week drug holiday could be conducted while carefully monitoring blood pressure and depressive symptoms. Atenolol could then be restarted to identify a temporal relationship between the symptoms and the medication.
Option 2: Treat for depression
Another option would be to treat the patient as if his symptoms represented depression. Exhibiting 4 of the necessary diagnostic criteria, the patient nearly qualifies for a diagnosis of current major depression. An antidepressant could be started, exercise could be prescribed, or a referral could be made for psychotherapy. However, again there is insufficient evidence that his subsyndromal depression will respond to standard treatments designed for major depressive disorder.
The patient returns as scheduled 2 weeks later. He has tolerated the change in blood pressure medications without difficulty, but he is experiencing persistent anhedonia, terminal insomnia, and low levels of concentration, energy, and libido. He has felt increasingly hopeless and worthless over the past 2 weeks, though he denies having thoughts of suicide. Results on CBC, serum chemistries, thyroid panel, and sleep study are all unremarkable.
The patient now clearly meets criteria for a major depressive episode. As a first step, he should be educated about depression. An excellent self-help book is Getting Your Life Back by Wright and Basco.6 The patient should be taught to monitor his symptoms with the BDI3 or the PHQ-94 to better assess the severity of the current episode, to monitor changes in his symptoms, and to rapidly identify relapses.
Most physicians would start an antidepressant, unless the patient had significant objections. Other treatment options, alone or in concert with antidepressant treatment, include exercise or psychotherapy. The patient is an excellent candidate for exercise, given that he has 3 risk factors for CAD: hypertension, a sedentary lifestyle, and obesity (4, if you include depression). Exercising for at least 30 minutes, 2 to 3 times per week, would likely benefit his physical and mental health. In addition to its cardiac benefits, exercise 3 times weekly was found in at least one trial to be as effective as sertraline in treating major depression in outpatients.7
Choosing an antidepressant. A number of factors should be considered in choosing antidepressants, including efficacy, side effect profile, and cost. Table 3 outlines some of the main considerations in the choice of antidepressants for this patient. Note that tricyclic antidepressants are not listed, being contraindicated in CAD because of their tendency to contribute to arrhythmias in the post-MI period. In this patient’s case, mirtazapine should be avoided because of the possibility of weight gain; venlafaxine should be avoided because of hypertension. Sertraline would be an appropriate choice, given that it has been relatively well-studied in persons with CAD.
The patient begins treatment with fluoxetine (10 mg/d, which is then increased to 20 mg/d after several days). His depressive symptoms gradually diminish; he achieves a “50%” reduction of symptoms at follow-up visit 3 weeks later. Two months after fluoxetine was initiated, the patient is nearly euthymic, reporting only 2 depressive symptoms, and is again engaging in usual recreational activities.
TABLE 3
A comparison of antidepressants in the treatment of depressed patients in cardiac populations
| Medication | Class/mechanism | Risks/side effects | Benefits |
| Citalopram | SSRI | Low cost, minimal drug-drug interactions | |
| Escitalopram | SSRI | Newest/least studied agent | Low cost, minimal drug-drug interactions, possibly faster onset and fewer side effects |
| Fluoxetine | SSRI | Long half-life, more drug-drug interactions | |
| Paroxetine | SSRI | Sedation, mild anticholinergic effects | |
| Sertraline | SSRI | Sedation, mild | Best studied in CAD; few drug interactions |
| Mirtazapine | Atypical antidepressant (5HT2, 5HT3, and alpha2 refceptor blockade) | Sedation, weight gain, possible elevation of lipids | No sexual dysfunction |
| Venlafaxine | Selective serotonin and norepinephrine receptor blockade | Elevated blood pressure in 13% at doses of 300 mg or greater | |
| Bupropion | Increases noradrenergic and dopaminergic activity | Initial anxiety | No sexual dysfunction |
| SSRI, selective serotonin reuptake inhibitor; CAD, coronary artery disease | |||
Q: Is depression, like hypertension, a risk factor for the development of coronary artery disease (CAD)? A:____________________________________________________ _____________________________________________________ _____________________________________________________
Whether depression is a risk factor for CAD depends on how one defines a risk factor and whether one is discussing “major” or “minor” risk factors. At least 15 narrative reviews have been written on the relationship between depression and heart disease, but none has examined the epidemiologic evidence for depression as a major risk factor for CAD (Table 4).8
In looking at the 7 main epidemiologic criteria for a risk factor, depression does very well on 4: strength of association, consistency, dose-response effect, and predictability. Numerous studies have shown that depression is clearly and consistently associated with the development of CAD, and that clinical depression appears to predict CAD more robustly than does depressed mood alone.9-12
On 2 of the criteria, specificity and biological plausibility, there is fair evidence for depression as a CAD risk factor. We do not yet know the relative importance of recurrent major depression, dysthymia, BDI scores of 10 or greater, or some other marker of depression as predictors of CAD.
Because mild depressive symptoms may predict CAD, it is unclear what levels of depression increase the risk of CAD and require intervention. Excellent work exists regarding the development of plausible mechanisms by which depression may lead to CAD; however, these mechanisms have yet to be proven. Therefore, the evidence in this domain can only be rated as fair.
Finally, the evidence is incomplete for one important criterion: response to treatment. Only one study has been designed to examine the effect of depression treatments on cardiac risk reduction. This study (the ENRICHD trial13) was a treatment study of post-MI depression that found that cognitive-behavioral therapy did not have a significant impact on reducing recurrent cardiac events.
Based on the most stringent epidemiologic criteria, depression is almost, but not quite, a risk factor for CAD. However, depression is a minor risk factor for CAD, and may someday be considered a major risk factor. While the mechanisms by which depression may lead to CAD have not yet been established, the association between depression and subsequent CAD likely occurs via 2 pathways.
The first pathway is behavioral. Patients with depression have diminished self-care, possibly increasing other CAD risk factors such as smoking, poor diet/hyperlipidemia, diabetes, physical inactivity, and obesity.
The second pathway by which depression may lead to CAD is neuroendocrine. Hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis and hyperactive sympathomedullary activity may result in elevated cytokine levels, platelet activation, and vascular damage, thereby contributing to CAD.8
TABLE 4
Depression as a risk factor for CAD: a “report card”8
| Risk factor | Strength of evidence |
| Strength of association | Good |
| Predictability | Good |
| Specificity | Fair |
| Consistency | Good |
| Dose-response effect | Good |
| Biological plausibility | Fair |
| Response to treatment | Incomplete |
This case illustrates several important points in the management of depressive symptoms in the family practice setting.
First, patients may present with subsyndromal depressive illness; there is, as yet, no evidence that antidepressants are beneficial in this population, and they expose patients to side effects such as sexual dysfunction.
Second, practitioners in general should not shy away from using beta-blockers where indicated for patients with cardiovascular disease and depression; the link between beta-blockers and depression seems minimal at best.
Third, when patients do present with the syndrome of major depression, it is important to evaluate potential medical contributors (eg, obstructive sleep apnea) when appropriate, and to treat with adequate doses of antidepressants for an adequate duration.
Fourth, the potential effects of depression on the development of CAD give family physicians yet another reason to remain vigilant for the presence of depression in all patients.
Should the FP treat independently? This discussion then leads to the question of when an informal or formal psychiatric consultation is indicated for the treatment of a depressed patient, and when the FP may wish to handle the case independently. The short answer is, of course, “it depends.” As with all areas of medical specialty, FPs will have varying levels of comfort, knowledge, and experience in the treatment of psychiatric disorders, and this will often affect the threshold for obtaining consultation. Furthermore, the number of psychiatric consultants—and thus the opportunity for consultations—varies widely depending on practice location.
Value of informal consultations. In general, FPs are well-equipped to handle patients with uncomplicated major depressive disorder or dysthymia without suicidal ideation or psychotic features. Informal consultation may be useful in cases (as in this case) when it is difficult to distinguish whether the patient meets criteria for major depressive disorder (and therefore requires treatment) or has subthreshold depressive symptoms. In addition, informal consultation can be useful when there is a question about antidepressant agent selection in a specific clinical situation. Finally, informal consultation may be of benefit when there are comorbid psychiatric illnesses, for example, coexisting panic disorder, generalized anxiety disorder, and major depressive disorder.
Opting for formal consultation. Formal psychiatric consultation is often useful when there is a mood disorder with suicidal ideation or psychotic features, when the disorder has been refractory to 2 or more adequate trials of an antidepressant, when there is a question of bipolar disorder (for which monotherapy with antidepressants is contraindicated) or substance use disorder, or for progressively worsening depression despite treatment.
Billing and coding. The logistics of billing for the treatment of comorbid psychiatric disorders by primary care physicians vary with the type of payer and from state to state. Because it is often impractical to modify billing procedures with each patient, it is useful for each practice to develop general billing guidelines for psychiatric disorders billed to Medicaid, Medicare, and the most common managed care organizations in the practice. In general, the physician caring for the patient described in this report would bill for hypertension and depression and get paid under the primary diagnosis of hypertension. When in doubt about whether to bill for a psychiatric disorder, primary care clinicians may include the relevant physical symptom in the billing codes, such as fatigue, headache, insomnia and bill under that code.
· Acknowledgments ·
Portions of this article were presented at the Association of Medicine and Psychiatry Annual Meeting, San Diego, California, November 19, 2003.
1. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Detection, Evaluation, and Treatment of High Blood Report of the Joint National Committee on Prevention, Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
2. Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 2004;350:1387-1397.
3. Beck AT. Beck Depression Inventory. In: Test Critiques, Vol II,. Deyser DJ, Sweetland RC (eds). Kansas City, Mo: Test Corporation of America; 1985;83-87.
4. Spitzer RL, Kroenke K, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-613.
5. Ko DT, Hebert PR, Coffey CS, et al. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA. 2002;288:351-357.
6. Basco MR, Wright JH. Getting Your Life Back: The complete Guide to Recovery from Depression. New York: Touchstone; 2002;
7. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159:2349-2356.
8. Wulsin LR. Is depression a major risk factor for coronary disease? A systematic review of the epidemiologic evidence. Harv Rev Psychiatry. 2004;12:79-93.
9. Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol. 1996;78:613-617.
10. Anda R, Williamson D, Jones D, et al. Depressed affect, hopelessness, and the risk of ischemic heart disease in a cohort of U.S. adults. Epidemiology 1993;4:285-294.
11. Ford DE, Mead LA, Chang PF, et al. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med. 1998;158:1422-1426.
12. Rugulies R. Depression as a predictor for coronary heart disease. a review and meta-analysis. Am J Prev Med 2002;23:51-61.
13. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed.Washington, DC: American Psychiatric Press; 1994.
Drug brand names
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Hydrochlorothiazide • Esidrix, HydroDIURIL, Oretic
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
1. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Detection, Evaluation, and Treatment of High Blood Report of the Joint National Committee on Prevention, Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
2. Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 2004;350:1387-1397.
3. Beck AT. Beck Depression Inventory. In: Test Critiques, Vol II,. Deyser DJ, Sweetland RC (eds). Kansas City, Mo: Test Corporation of America; 1985;83-87.
4. Spitzer RL, Kroenke K, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-613.
5. Ko DT, Hebert PR, Coffey CS, et al. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA. 2002;288:351-357.
6. Basco MR, Wright JH. Getting Your Life Back: The complete Guide to Recovery from Depression. New York: Touchstone; 2002;
7. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159:2349-2356.
8. Wulsin LR. Is depression a major risk factor for coronary disease? A systematic review of the epidemiologic evidence. Harv Rev Psychiatry. 2004;12:79-93.
9. Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol. 1996;78:613-617.
10. Anda R, Williamson D, Jones D, et al. Depressed affect, hopelessness, and the risk of ischemic heart disease in a cohort of U.S. adults. Epidemiology 1993;4:285-294.
11. Ford DE, Mead LA, Chang PF, et al. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med. 1998;158:1422-1426.
12. Rugulies R. Depression as a predictor for coronary heart disease. a review and meta-analysis. Am J Prev Med 2002;23:51-61.
13. Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA 2003;289:3106-3116.
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed.Washington, DC: American Psychiatric Press; 1994.
Drug brand names
- Atenolol • Tenormin
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Hydrochlorothiazide • Esidrix, HydroDIURIL, Oretic
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Brain/body connection: Treating depression in patients with cardiovascular disease
Depression can exacerbate cardiovascular disease (CVD), and CVD can exacerbate depression (Figure). Thus, effectively treating depression enhances heart disease treatment, particularly if psychiatrists and medical physicians collaborate in providing patient care.
This article describes a patient with risk factors for heart disease, illustrates the physiologic pathways that link depression and CVD, and offers clinical tips to help you improve outcomes for patients with both disorders.
Case report: Trying to ‘get going’
Mr. D, age 51, presents with vegetative symptoms and a personal and family history of CVD, depression, and substance abuse disorders. He was born in a small town in Kentucky and raised in Louisville’s poorest neighborhood. After his mother died at age 42 of “hardening of the arteries,” his father started drinking more, working less, and “never really got going again.”
Figure Neuroendocrine pathways by which depression may cause or promote CVD
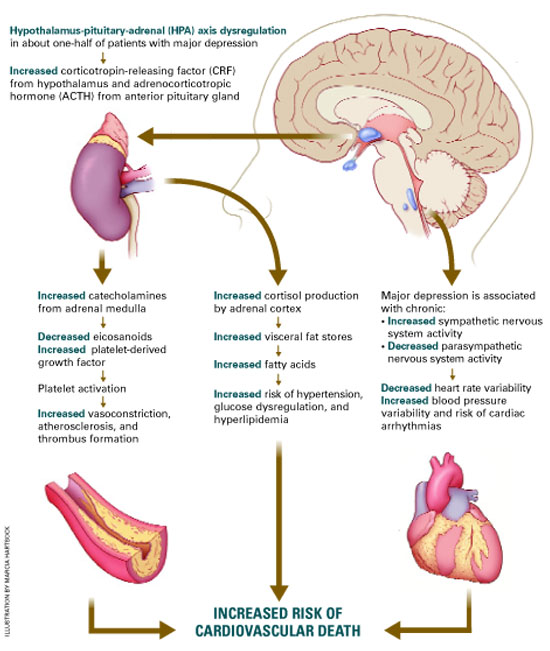
Among patients with a recent myocardial infarction (MI), as many as two-thirds report depressive symptoms.1 Major depression has been reported in:
- 16% to 22% of patients hospitalized post-MI,2,3 compared with 5% in the general population and 10% in the primary care population4
- 15% of patients with unstable angina5 and 20% of patients undergoing coronary artery bypass (CABG) surgery.6
Among the annual 1.5 million Americans who have an acute MI or unstable angina, 40% develop depression immediately thereafter. These 600,000 depressed patients are three times more likely to die within 6 months, compared with post-MI patients who are not depressed.7
Mr. D worked 20 years as a construction contractor, often running several work crews at once. At age 41, he slid into a depressive episode after his second divorce. He struggled with low energy, disturbed sleep, hopelessness, and increased smoking and drinking for 1 year, but he did not seek help.
Two years later, he suffered an inferior wall transmural myocardial infarction. His CVD risk factors included family history of early heart disease, smoking for 32 years, and elevated low-density lipoprotein (LDL) cholesterol. After subsequent episodes of unstable angina, stents were placed in two coronary arteries. Though his cardiologist cleared him to return to work, he felt able to work only part-time and erratically.
During a visit to their family doctor several years later, Mr. D’s wife suggested that her husband might be depressed. Reluctantly, Mr. D consulted a psychiatrist.
The psychiatrist diagnosed major depressive disorder and prescribed sertraline, 50 mg/d. Within 2 months, Mr. D’s symptoms had dropped by 50% on a symptom severity measure. He did not refill his prescription, however, because of concerns about sexual side effects. Two months later he was hospitalized for another episode of unstable angina. His depression had returned within 1 month of stopping sertraline.
The psychiatrist switched him to citalopram, 20 mg/d, and carefully monitored depressive symptoms, side effects, and medication adherence. Aside from talking with the psychiatrist for a half-hour in his family doctor’s office every few weeks, Mr. D refused to undergo psychotherapy. He eventually achieved depression remission with a combination of citalopram, 20 mg/d, and nefazodone, 200 mg/d.
Depression-CVD connection
As in Mr. D’s case, depression and CVD commonly occur together, often with serious consequences (Box). 1-7 The association between depression and CVD is not limited to depression’s effect on existing disease, however. Depression often precedes coronary disease by about 30 years—suggesting possible cause and effect. Two systematic reviews8,9 found that depression increased CVD risk by 64%.
Seven well-controlled studies5-7,10-13 compared the relative effect of depression on the cardiovascular system with that of established CVD predictors. All seven found depression’s independent effect to be significant and comparable to or greater than that of ejection fraction, previous MI history, or number of vessels with >50% narrowing.
Comorbid depression and CVD usually persists months or years,14 and most studies indicate a dose-response relationship; the more severe the depression, the greater the risk for CVD to develop or progress.8,15
The link between depression treatment and CVD risk has not been well-studied. The only randomized, controlled trial found that cognitive therapy for depression did not significantly reduce cardiac events among patients with known CVD.16
Possible mechanisms
Depression’s effect on CVD. How does depression affect CVD development and progression? Both behavioral and biological pathways may be involved.17 The behavioral pathway proposes that depression triggers behaviors—such as smoking, overeating, and sedentary lifestyles—that increase the risk of developing or worsening CVD. The biological pathway proposes that neuroendocrine changes during depression accelerate CVD development.
About one-half of persons with major depression exhibit hypothalamic-pituitary-adrenal (HPA) axis dysregulation, with excessive secretion of corticotropin releasing factor (CRF) and chronically elevated cortisol.18 This HPA dysregulation is related to defective negative feedback at the paraventricular nucleus of the hypothalamus. Chronic HPA axis dysregulation promotes vascular inflammation, and several studies have reported C-reactive protein elevation and cytokine changes in patients with major depression.19,20
Major depression is also associated with excessive sympathetic and diminished parasym-pathetic nervous system activity, potentially contributing to hypertension, increased resting heart rate, decreased heart rate variability, and altered endothelial function.2,21,22 Each of these factors facilitates arterial plaque formation.
Depression may also exacerbate chronic anxiety and other forms of distress. The combined effects of an overtaxed central nervous system, neuroendocrine dysregulation, and unhealthy behaviors may eventually overwhelm the cardiovascular system.
CVD’s effect on depression. How does CVD contribute to depression? The vascular depression hypothesis23 proposes that diffuse heart and brain atherosclerosis restricts perfusion of limbic and cortical structures that regulate mood. A first depressive episode after acute MI or CABG probably represents exacerbation of cerebrovascular insufficiency that preceded the coronary event.
Table
Four keys to effectively treat depression in patients with heart disease
|
In practical terms, this means that pathways linking depression and heart disease include not only biological factors but also:
- psychological factors such as depression, anxiety, and chronic stress
- behavioral factors such as smoking, physical inactivity, and high-fat diet.
How to improve outcomes
Patients with CVD commonly do not receive effective depression treatment:
- Internists and family physicians give preferential attention to physical illness.
- Patients may have insufficient access to mental health specialists.
- Physicians do not adequately monitor depression treatment.
- Patients are reluctant to accept the stigma of mental illness.
By collaborating with primary care physicians, you can improve the likelihood that depression treatment will achieve remission and prevent relapse (Table).
Risk factors for CVD. Depression contributes to heart disease by exacerbating four major CVD risk factors—smoking, diabetes, obesity, and physical inactivity. By effectively treating depression, you may help patients avoid common depressive symptoms—such as overeating and sedentary behaviors—that are related to low energy or fatigue.
Educate middle-aged patients with depression about CVD’s associated risk. Prochaska’s “stages of change” (see Related resources) can help them stop smoking, lose weight, and exercise.
Access to cardiac care. Depressed patients may be less motivated than nondepressed patients to pursue cardiac care.24 Therefore, you may need to:
- encourage your patients to take advantage of indicated state-of-the-art care, including stents, bypass surgery, and medications
- understand patients’ complex cardiac regimens and help them adhere when depression interferes with their motivation.
Effective depression treatment
Patient history. For depressed patients older than 40, take a careful inventory of CVD risk factors:
- family history of heart disease before age 60 for men and age 70 for women
- personal history of smoking, blood pressure >140/90 mm Hg, LDL cholesterol >100 mg/dL, type 2 diabetes, body mass index >30, or physical inactivity (<30 minutes of walking 3 days a week).
In general, the more risk factors, the greater the risk of CVD.
Antidepressant selection. Selective serotonin reuptake inhibitors (SSRIs) are safe and effective for treating major depression in CVD and congestive heart failure.25 Venlafaxine at doses >300 mg/d may increase blood pressure, so use this drug with caution in depressed patients with hypertension.
No controlled clinical trials have gauged the safety and efficacy of bupropion or mirtazapine in patients with CVD.
Tricyclic antidepressants are contraindicated for 6 months post-MI because they may contribute to arrhythmias. Avoid using them in depressed patients with CVD or conduction defects because of their quinidine-like effects on conduction.
Cardiac medications. Contrary to folk wisdom, beta blockers do not cause depression.26 Whether or not a patient is depressed, our primary care and cardiology colleagues can use beta blockers to help regulate the peripheral autonomic nervous system, reducing high blood pressure and the risk of arrhythmias.
SSRIs may increase blood levels of beta blockers, warfarin, and other cardiac medications via cytochrome P-450 isoenzyme inhibition. Make sure warfarin levels and other cardiac drug effects are well monitored when you adjust psychotropic dosages.
Divalproex and SSRIs also may reduce platelet aggregation. Patients who are receiving concomitant aspirin or warfarin may bruise or bleed easily and require dosage reductions or medication changes.
Psychotherapy. All patients with major or minor depression and CVD are considered high-risk and are candidates for a trial of brief psychotherapy. Therapeutic goals are to achieve full remission of depressive symptoms as rapidly as possible, prevent relapse, and maximize adherence to cardiac and depression drug regimens.
Collaborate closely with the cardiologist or primary care physician during the patient’s depressive episode and occasionally during maintenance treatment. Discuss or share notes on the patient’s depressive and cardiac disorders, medication management, symptom monitoring, and behavior changes needed to reduce cardiac risk.
With your added support, patients with depression and CVD are more likely to adhere to antidepressant medications and achieve symptom remission.
- National Institute of Mental Health. Depression and heart disease. www.nimh.nih.gov/publicat/depheart.cfm.
- Dewan NA, Suresh DP, Blomkalns A. Selecting safe psychotropics for post-MI patients. Current Psychiatry. 2003;2(3):15-21.
- Prochaska JO, Norcross JC, DiClemente CC. Changing for good. New York: Avon, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Paroxetine • Paxil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Wulsin is a consultant to Pfizer Inc. and Janssen Pharmaceutica.
Dr. Vieweg is a speaker for Janssen Pharmaceutica, Eli Lilly and Co., Pfizer Inc., Wyeth Pharmaceuticals, Forest Pharmaceuticals, and GlaxoSmithKline.
Dr. Fernandez reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Cassem N, Hackett T. Psychiatric condition in a coronary care unit. Ann Intern Med 1971;75:9-14.
2. Glassman A, Shapiro P. Depression and the course of coronary artery disease. Am J Psychiatry 1998;155:4-11.
3. Carney R, Freedland K, Sheline Y, Weiss E. Depression and coronary heart disease: a review for cardiologists. Clin Cardiol 1997;20:196-200.
4. Katon W, Schulbert H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14:237-47.
5. Lesperance F, Frasure-Smith N, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000;160:1354-60.
6. Connerney I, Shapiro P, McLaughlin J, et al. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001;358:1766-71.
7. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction. Circulation 1995;91:999-1005.
8. Rugulies R. Depression as a predictor for coronary heart disease. Am J Prev Med 2002;23:51-61.
9. Wulsin L, Singal B. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003;65:201-10.
10. Carney R, Rich M, Freedland K, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988;50:627-33.
11. Ladwig K, Roll G, Breithardt G, Borggrefe M. Extracardiac contributions to chest pain perception in patients 6 months after acute myocardial infarction. Am Heart J 1999;137:528-34.
12. Levine J, Covino N, Slack W, et al. Psychological predictors of subsequent medical care among patients hospitalized with cardiac disease. J Cardiopulm Rehabil 1996;16:109-16.
13. Lesperance F, Frasure-Smith N, Talajic M, Bourassa M. Five-year risk of cardiac mortality in relation to initial severity and one-year changes in depression symptoms after myocardial infarction. Circulation 2002;105:1049-53.
14. Dwight M, Stoudemire A. Effects of depressive disorders on coronary artery disease: a review. Harv Rev Psychiatry 1997;5:115-122.
15. Penninx B, Beekman A, Honig A, et al. Depression and cardiac mortality. Arch Gen Psychiatry 2001;58:221-7.
16. Writing committee of the ENRICHD investigators. Effects of treating depression and low perceived social support on clinical events after myocardial infarction. JAMA 2003;289:3106-16.
17. Carney RM, Freedland K, Miller G, Jaffe AS. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
18. Musselman D, Evans D, Nemeroff C. The relationship of depression to cardiovascular disease. Arch Gen Psychiatry 1998;55:580-92.
19. Kop WJ. Chronic and acute psychological risk factors for clinical manifestations of coronary artery disease. Psychosom Med 1999;61:476-86.
20. Miller G, Cohen S, Herbert T. Pathways linking major depression and immunity in ambulatory female patients. Psychosom Med 1999;61:850-60.
21. Carney R, Freedland K, Stein P. Change in heart rate and heart rate variability during treatment for depression in patients with coronary heart disease. Psychosom Med 2000;62:639-47.
22. Carney R, Freedland K, Miller G, Jaffe A. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
23. Alexopoulos G, Meyers B, Young R, et al. Vascular depression hypothesis. Psychosom Med 1997;58:113-121.
24. Ziegelstein R, Fauerbach J, Stevens S, et al. Patients with depression are less likely to follow recommendations to reduce cardiac risk during recovery from a myocardial infarction. Arch Intern Med 2000;160:1818-23.
25. Glassman AH, O’Connor C, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002;288:701-9.
26. Ko D, Hebert P, Coffey C, et al. B-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA 2002;288:351-7.
Depression can exacerbate cardiovascular disease (CVD), and CVD can exacerbate depression (Figure). Thus, effectively treating depression enhances heart disease treatment, particularly if psychiatrists and medical physicians collaborate in providing patient care.
This article describes a patient with risk factors for heart disease, illustrates the physiologic pathways that link depression and CVD, and offers clinical tips to help you improve outcomes for patients with both disorders.
Case report: Trying to ‘get going’
Mr. D, age 51, presents with vegetative symptoms and a personal and family history of CVD, depression, and substance abuse disorders. He was born in a small town in Kentucky and raised in Louisville’s poorest neighborhood. After his mother died at age 42 of “hardening of the arteries,” his father started drinking more, working less, and “never really got going again.”
Figure Neuroendocrine pathways by which depression may cause or promote CVD
Among patients with a recent myocardial infarction (MI), as many as two-thirds report depressive symptoms.1 Major depression has been reported in:
- 16% to 22% of patients hospitalized post-MI,2,3 compared with 5% in the general population and 10% in the primary care population4
- 15% of patients with unstable angina5 and 20% of patients undergoing coronary artery bypass (CABG) surgery.6
Among the annual 1.5 million Americans who have an acute MI or unstable angina, 40% develop depression immediately thereafter. These 600,000 depressed patients are three times more likely to die within 6 months, compared with post-MI patients who are not depressed.7
Mr. D worked 20 years as a construction contractor, often running several work crews at once. At age 41, he slid into a depressive episode after his second divorce. He struggled with low energy, disturbed sleep, hopelessness, and increased smoking and drinking for 1 year, but he did not seek help.
Two years later, he suffered an inferior wall transmural myocardial infarction. His CVD risk factors included family history of early heart disease, smoking for 32 years, and elevated low-density lipoprotein (LDL) cholesterol. After subsequent episodes of unstable angina, stents were placed in two coronary arteries. Though his cardiologist cleared him to return to work, he felt able to work only part-time and erratically.
During a visit to their family doctor several years later, Mr. D’s wife suggested that her husband might be depressed. Reluctantly, Mr. D consulted a psychiatrist.
The psychiatrist diagnosed major depressive disorder and prescribed sertraline, 50 mg/d. Within 2 months, Mr. D’s symptoms had dropped by 50% on a symptom severity measure. He did not refill his prescription, however, because of concerns about sexual side effects. Two months later he was hospitalized for another episode of unstable angina. His depression had returned within 1 month of stopping sertraline.
The psychiatrist switched him to citalopram, 20 mg/d, and carefully monitored depressive symptoms, side effects, and medication adherence. Aside from talking with the psychiatrist for a half-hour in his family doctor’s office every few weeks, Mr. D refused to undergo psychotherapy. He eventually achieved depression remission with a combination of citalopram, 20 mg/d, and nefazodone, 200 mg/d.
Depression-CVD connection
As in Mr. D’s case, depression and CVD commonly occur together, often with serious consequences (Box). 1-7 The association between depression and CVD is not limited to depression’s effect on existing disease, however. Depression often precedes coronary disease by about 30 years—suggesting possible cause and effect. Two systematic reviews8,9 found that depression increased CVD risk by 64%.
Seven well-controlled studies5-7,10-13 compared the relative effect of depression on the cardiovascular system with that of established CVD predictors. All seven found depression’s independent effect to be significant and comparable to or greater than that of ejection fraction, previous MI history, or number of vessels with >50% narrowing.
Comorbid depression and CVD usually persists months or years,14 and most studies indicate a dose-response relationship; the more severe the depression, the greater the risk for CVD to develop or progress.8,15
The link between depression treatment and CVD risk has not been well-studied. The only randomized, controlled trial found that cognitive therapy for depression did not significantly reduce cardiac events among patients with known CVD.16
Possible mechanisms
Depression’s effect on CVD. How does depression affect CVD development and progression? Both behavioral and biological pathways may be involved.17 The behavioral pathway proposes that depression triggers behaviors—such as smoking, overeating, and sedentary lifestyles—that increase the risk of developing or worsening CVD. The biological pathway proposes that neuroendocrine changes during depression accelerate CVD development.
About one-half of persons with major depression exhibit hypothalamic-pituitary-adrenal (HPA) axis dysregulation, with excessive secretion of corticotropin releasing factor (CRF) and chronically elevated cortisol.18 This HPA dysregulation is related to defective negative feedback at the paraventricular nucleus of the hypothalamus. Chronic HPA axis dysregulation promotes vascular inflammation, and several studies have reported C-reactive protein elevation and cytokine changes in patients with major depression.19,20
Major depression is also associated with excessive sympathetic and diminished parasym-pathetic nervous system activity, potentially contributing to hypertension, increased resting heart rate, decreased heart rate variability, and altered endothelial function.2,21,22 Each of these factors facilitates arterial plaque formation.
Depression may also exacerbate chronic anxiety and other forms of distress. The combined effects of an overtaxed central nervous system, neuroendocrine dysregulation, and unhealthy behaviors may eventually overwhelm the cardiovascular system.
CVD’s effect on depression. How does CVD contribute to depression? The vascular depression hypothesis23 proposes that diffuse heart and brain atherosclerosis restricts perfusion of limbic and cortical structures that regulate mood. A first depressive episode after acute MI or CABG probably represents exacerbation of cerebrovascular insufficiency that preceded the coronary event.
Table
Four keys to effectively treat depression in patients with heart disease
|
In practical terms, this means that pathways linking depression and heart disease include not only biological factors but also:
- psychological factors such as depression, anxiety, and chronic stress
- behavioral factors such as smoking, physical inactivity, and high-fat diet.
How to improve outcomes
Patients with CVD commonly do not receive effective depression treatment:
- Internists and family physicians give preferential attention to physical illness.
- Patients may have insufficient access to mental health specialists.
- Physicians do not adequately monitor depression treatment.
- Patients are reluctant to accept the stigma of mental illness.
By collaborating with primary care physicians, you can improve the likelihood that depression treatment will achieve remission and prevent relapse (Table).
Risk factors for CVD. Depression contributes to heart disease by exacerbating four major CVD risk factors—smoking, diabetes, obesity, and physical inactivity. By effectively treating depression, you may help patients avoid common depressive symptoms—such as overeating and sedentary behaviors—that are related to low energy or fatigue.
Educate middle-aged patients with depression about CVD’s associated risk. Prochaska’s “stages of change” (see Related resources) can help them stop smoking, lose weight, and exercise.
Access to cardiac care. Depressed patients may be less motivated than nondepressed patients to pursue cardiac care.24 Therefore, you may need to:
- encourage your patients to take advantage of indicated state-of-the-art care, including stents, bypass surgery, and medications
- understand patients’ complex cardiac regimens and help them adhere when depression interferes with their motivation.
Effective depression treatment
Patient history. For depressed patients older than 40, take a careful inventory of CVD risk factors:
- family history of heart disease before age 60 for men and age 70 for women
- personal history of smoking, blood pressure >140/90 mm Hg, LDL cholesterol >100 mg/dL, type 2 diabetes, body mass index >30, or physical inactivity (<30 minutes of walking 3 days a week).
In general, the more risk factors, the greater the risk of CVD.
Antidepressant selection. Selective serotonin reuptake inhibitors (SSRIs) are safe and effective for treating major depression in CVD and congestive heart failure.25 Venlafaxine at doses >300 mg/d may increase blood pressure, so use this drug with caution in depressed patients with hypertension.
No controlled clinical trials have gauged the safety and efficacy of bupropion or mirtazapine in patients with CVD.
Tricyclic antidepressants are contraindicated for 6 months post-MI because they may contribute to arrhythmias. Avoid using them in depressed patients with CVD or conduction defects because of their quinidine-like effects on conduction.
Cardiac medications. Contrary to folk wisdom, beta blockers do not cause depression.26 Whether or not a patient is depressed, our primary care and cardiology colleagues can use beta blockers to help regulate the peripheral autonomic nervous system, reducing high blood pressure and the risk of arrhythmias.
SSRIs may increase blood levels of beta blockers, warfarin, and other cardiac medications via cytochrome P-450 isoenzyme inhibition. Make sure warfarin levels and other cardiac drug effects are well monitored when you adjust psychotropic dosages.
Divalproex and SSRIs also may reduce platelet aggregation. Patients who are receiving concomitant aspirin or warfarin may bruise or bleed easily and require dosage reductions or medication changes.
Psychotherapy. All patients with major or minor depression and CVD are considered high-risk and are candidates for a trial of brief psychotherapy. Therapeutic goals are to achieve full remission of depressive symptoms as rapidly as possible, prevent relapse, and maximize adherence to cardiac and depression drug regimens.
Collaborate closely with the cardiologist or primary care physician during the patient’s depressive episode and occasionally during maintenance treatment. Discuss or share notes on the patient’s depressive and cardiac disorders, medication management, symptom monitoring, and behavior changes needed to reduce cardiac risk.
With your added support, patients with depression and CVD are more likely to adhere to antidepressant medications and achieve symptom remission.
- National Institute of Mental Health. Depression and heart disease. www.nimh.nih.gov/publicat/depheart.cfm.
- Dewan NA, Suresh DP, Blomkalns A. Selecting safe psychotropics for post-MI patients. Current Psychiatry. 2003;2(3):15-21.
- Prochaska JO, Norcross JC, DiClemente CC. Changing for good. New York: Avon, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Paroxetine • Paxil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Wulsin is a consultant to Pfizer Inc. and Janssen Pharmaceutica.
Dr. Vieweg is a speaker for Janssen Pharmaceutica, Eli Lilly and Co., Pfizer Inc., Wyeth Pharmaceuticals, Forest Pharmaceuticals, and GlaxoSmithKline.
Dr. Fernandez reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Depression can exacerbate cardiovascular disease (CVD), and CVD can exacerbate depression (Figure). Thus, effectively treating depression enhances heart disease treatment, particularly if psychiatrists and medical physicians collaborate in providing patient care.
This article describes a patient with risk factors for heart disease, illustrates the physiologic pathways that link depression and CVD, and offers clinical tips to help you improve outcomes for patients with both disorders.
Case report: Trying to ‘get going’
Mr. D, age 51, presents with vegetative symptoms and a personal and family history of CVD, depression, and substance abuse disorders. He was born in a small town in Kentucky and raised in Louisville’s poorest neighborhood. After his mother died at age 42 of “hardening of the arteries,” his father started drinking more, working less, and “never really got going again.”
Figure Neuroendocrine pathways by which depression may cause or promote CVD
Among patients with a recent myocardial infarction (MI), as many as two-thirds report depressive symptoms.1 Major depression has been reported in:
- 16% to 22% of patients hospitalized post-MI,2,3 compared with 5% in the general population and 10% in the primary care population4
- 15% of patients with unstable angina5 and 20% of patients undergoing coronary artery bypass (CABG) surgery.6
Among the annual 1.5 million Americans who have an acute MI or unstable angina, 40% develop depression immediately thereafter. These 600,000 depressed patients are three times more likely to die within 6 months, compared with post-MI patients who are not depressed.7
Mr. D worked 20 years as a construction contractor, often running several work crews at once. At age 41, he slid into a depressive episode after his second divorce. He struggled with low energy, disturbed sleep, hopelessness, and increased smoking and drinking for 1 year, but he did not seek help.
Two years later, he suffered an inferior wall transmural myocardial infarction. His CVD risk factors included family history of early heart disease, smoking for 32 years, and elevated low-density lipoprotein (LDL) cholesterol. After subsequent episodes of unstable angina, stents were placed in two coronary arteries. Though his cardiologist cleared him to return to work, he felt able to work only part-time and erratically.
During a visit to their family doctor several years later, Mr. D’s wife suggested that her husband might be depressed. Reluctantly, Mr. D consulted a psychiatrist.
The psychiatrist diagnosed major depressive disorder and prescribed sertraline, 50 mg/d. Within 2 months, Mr. D’s symptoms had dropped by 50% on a symptom severity measure. He did not refill his prescription, however, because of concerns about sexual side effects. Two months later he was hospitalized for another episode of unstable angina. His depression had returned within 1 month of stopping sertraline.
The psychiatrist switched him to citalopram, 20 mg/d, and carefully monitored depressive symptoms, side effects, and medication adherence. Aside from talking with the psychiatrist for a half-hour in his family doctor’s office every few weeks, Mr. D refused to undergo psychotherapy. He eventually achieved depression remission with a combination of citalopram, 20 mg/d, and nefazodone, 200 mg/d.
Depression-CVD connection
As in Mr. D’s case, depression and CVD commonly occur together, often with serious consequences (Box). 1-7 The association between depression and CVD is not limited to depression’s effect on existing disease, however. Depression often precedes coronary disease by about 30 years—suggesting possible cause and effect. Two systematic reviews8,9 found that depression increased CVD risk by 64%.
Seven well-controlled studies5-7,10-13 compared the relative effect of depression on the cardiovascular system with that of established CVD predictors. All seven found depression’s independent effect to be significant and comparable to or greater than that of ejection fraction, previous MI history, or number of vessels with >50% narrowing.
Comorbid depression and CVD usually persists months or years,14 and most studies indicate a dose-response relationship; the more severe the depression, the greater the risk for CVD to develop or progress.8,15
The link between depression treatment and CVD risk has not been well-studied. The only randomized, controlled trial found that cognitive therapy for depression did not significantly reduce cardiac events among patients with known CVD.16
Possible mechanisms
Depression’s effect on CVD. How does depression affect CVD development and progression? Both behavioral and biological pathways may be involved.17 The behavioral pathway proposes that depression triggers behaviors—such as smoking, overeating, and sedentary lifestyles—that increase the risk of developing or worsening CVD. The biological pathway proposes that neuroendocrine changes during depression accelerate CVD development.
About one-half of persons with major depression exhibit hypothalamic-pituitary-adrenal (HPA) axis dysregulation, with excessive secretion of corticotropin releasing factor (CRF) and chronically elevated cortisol.18 This HPA dysregulation is related to defective negative feedback at the paraventricular nucleus of the hypothalamus. Chronic HPA axis dysregulation promotes vascular inflammation, and several studies have reported C-reactive protein elevation and cytokine changes in patients with major depression.19,20
Major depression is also associated with excessive sympathetic and diminished parasym-pathetic nervous system activity, potentially contributing to hypertension, increased resting heart rate, decreased heart rate variability, and altered endothelial function.2,21,22 Each of these factors facilitates arterial plaque formation.
Depression may also exacerbate chronic anxiety and other forms of distress. The combined effects of an overtaxed central nervous system, neuroendocrine dysregulation, and unhealthy behaviors may eventually overwhelm the cardiovascular system.
CVD’s effect on depression. How does CVD contribute to depression? The vascular depression hypothesis23 proposes that diffuse heart and brain atherosclerosis restricts perfusion of limbic and cortical structures that regulate mood. A first depressive episode after acute MI or CABG probably represents exacerbation of cerebrovascular insufficiency that preceded the coronary event.
Table
Four keys to effectively treat depression in patients with heart disease
|
In practical terms, this means that pathways linking depression and heart disease include not only biological factors but also:
- psychological factors such as depression, anxiety, and chronic stress
- behavioral factors such as smoking, physical inactivity, and high-fat diet.
How to improve outcomes
Patients with CVD commonly do not receive effective depression treatment:
- Internists and family physicians give preferential attention to physical illness.
- Patients may have insufficient access to mental health specialists.
- Physicians do not adequately monitor depression treatment.
- Patients are reluctant to accept the stigma of mental illness.
By collaborating with primary care physicians, you can improve the likelihood that depression treatment will achieve remission and prevent relapse (Table).
Risk factors for CVD. Depression contributes to heart disease by exacerbating four major CVD risk factors—smoking, diabetes, obesity, and physical inactivity. By effectively treating depression, you may help patients avoid common depressive symptoms—such as overeating and sedentary behaviors—that are related to low energy or fatigue.
Educate middle-aged patients with depression about CVD’s associated risk. Prochaska’s “stages of change” (see Related resources) can help them stop smoking, lose weight, and exercise.
Access to cardiac care. Depressed patients may be less motivated than nondepressed patients to pursue cardiac care.24 Therefore, you may need to:
- encourage your patients to take advantage of indicated state-of-the-art care, including stents, bypass surgery, and medications
- understand patients’ complex cardiac regimens and help them adhere when depression interferes with their motivation.
Effective depression treatment
Patient history. For depressed patients older than 40, take a careful inventory of CVD risk factors:
- family history of heart disease before age 60 for men and age 70 for women
- personal history of smoking, blood pressure >140/90 mm Hg, LDL cholesterol >100 mg/dL, type 2 diabetes, body mass index >30, or physical inactivity (<30 minutes of walking 3 days a week).
In general, the more risk factors, the greater the risk of CVD.
Antidepressant selection. Selective serotonin reuptake inhibitors (SSRIs) are safe and effective for treating major depression in CVD and congestive heart failure.25 Venlafaxine at doses >300 mg/d may increase blood pressure, so use this drug with caution in depressed patients with hypertension.
No controlled clinical trials have gauged the safety and efficacy of bupropion or mirtazapine in patients with CVD.
Tricyclic antidepressants are contraindicated for 6 months post-MI because they may contribute to arrhythmias. Avoid using them in depressed patients with CVD or conduction defects because of their quinidine-like effects on conduction.
Cardiac medications. Contrary to folk wisdom, beta blockers do not cause depression.26 Whether or not a patient is depressed, our primary care and cardiology colleagues can use beta blockers to help regulate the peripheral autonomic nervous system, reducing high blood pressure and the risk of arrhythmias.
SSRIs may increase blood levels of beta blockers, warfarin, and other cardiac medications via cytochrome P-450 isoenzyme inhibition. Make sure warfarin levels and other cardiac drug effects are well monitored when you adjust psychotropic dosages.
Divalproex and SSRIs also may reduce platelet aggregation. Patients who are receiving concomitant aspirin or warfarin may bruise or bleed easily and require dosage reductions or medication changes.
Psychotherapy. All patients with major or minor depression and CVD are considered high-risk and are candidates for a trial of brief psychotherapy. Therapeutic goals are to achieve full remission of depressive symptoms as rapidly as possible, prevent relapse, and maximize adherence to cardiac and depression drug regimens.
Collaborate closely with the cardiologist or primary care physician during the patient’s depressive episode and occasionally during maintenance treatment. Discuss or share notes on the patient’s depressive and cardiac disorders, medication management, symptom monitoring, and behavior changes needed to reduce cardiac risk.
With your added support, patients with depression and CVD are more likely to adhere to antidepressant medications and achieve symptom remission.
- National Institute of Mental Health. Depression and heart disease. www.nimh.nih.gov/publicat/depheart.cfm.
- Dewan NA, Suresh DP, Blomkalns A. Selecting safe psychotropics for post-MI patients. Current Psychiatry. 2003;2(3):15-21.
- Prochaska JO, Norcross JC, DiClemente CC. Changing for good. New York: Avon, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Paroxetine • Paxil
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
Dr. Wulsin is a consultant to Pfizer Inc. and Janssen Pharmaceutica.
Dr. Vieweg is a speaker for Janssen Pharmaceutica, Eli Lilly and Co., Pfizer Inc., Wyeth Pharmaceuticals, Forest Pharmaceuticals, and GlaxoSmithKline.
Dr. Fernandez reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Cassem N, Hackett T. Psychiatric condition in a coronary care unit. Ann Intern Med 1971;75:9-14.
2. Glassman A, Shapiro P. Depression and the course of coronary artery disease. Am J Psychiatry 1998;155:4-11.
3. Carney R, Freedland K, Sheline Y, Weiss E. Depression and coronary heart disease: a review for cardiologists. Clin Cardiol 1997;20:196-200.
4. Katon W, Schulbert H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14:237-47.
5. Lesperance F, Frasure-Smith N, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000;160:1354-60.
6. Connerney I, Shapiro P, McLaughlin J, et al. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001;358:1766-71.
7. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction. Circulation 1995;91:999-1005.
8. Rugulies R. Depression as a predictor for coronary heart disease. Am J Prev Med 2002;23:51-61.
9. Wulsin L, Singal B. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003;65:201-10.
10. Carney R, Rich M, Freedland K, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988;50:627-33.
11. Ladwig K, Roll G, Breithardt G, Borggrefe M. Extracardiac contributions to chest pain perception in patients 6 months after acute myocardial infarction. Am Heart J 1999;137:528-34.
12. Levine J, Covino N, Slack W, et al. Psychological predictors of subsequent medical care among patients hospitalized with cardiac disease. J Cardiopulm Rehabil 1996;16:109-16.
13. Lesperance F, Frasure-Smith N, Talajic M, Bourassa M. Five-year risk of cardiac mortality in relation to initial severity and one-year changes in depression symptoms after myocardial infarction. Circulation 2002;105:1049-53.
14. Dwight M, Stoudemire A. Effects of depressive disorders on coronary artery disease: a review. Harv Rev Psychiatry 1997;5:115-122.
15. Penninx B, Beekman A, Honig A, et al. Depression and cardiac mortality. Arch Gen Psychiatry 2001;58:221-7.
16. Writing committee of the ENRICHD investigators. Effects of treating depression and low perceived social support on clinical events after myocardial infarction. JAMA 2003;289:3106-16.
17. Carney RM, Freedland K, Miller G, Jaffe AS. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
18. Musselman D, Evans D, Nemeroff C. The relationship of depression to cardiovascular disease. Arch Gen Psychiatry 1998;55:580-92.
19. Kop WJ. Chronic and acute psychological risk factors for clinical manifestations of coronary artery disease. Psychosom Med 1999;61:476-86.
20. Miller G, Cohen S, Herbert T. Pathways linking major depression and immunity in ambulatory female patients. Psychosom Med 1999;61:850-60.
21. Carney R, Freedland K, Stein P. Change in heart rate and heart rate variability during treatment for depression in patients with coronary heart disease. Psychosom Med 2000;62:639-47.
22. Carney R, Freedland K, Miller G, Jaffe A. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
23. Alexopoulos G, Meyers B, Young R, et al. Vascular depression hypothesis. Psychosom Med 1997;58:113-121.
24. Ziegelstein R, Fauerbach J, Stevens S, et al. Patients with depression are less likely to follow recommendations to reduce cardiac risk during recovery from a myocardial infarction. Arch Intern Med 2000;160:1818-23.
25. Glassman AH, O’Connor C, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002;288:701-9.
26. Ko D, Hebert P, Coffey C, et al. B-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA 2002;288:351-7.
1. Cassem N, Hackett T. Psychiatric condition in a coronary care unit. Ann Intern Med 1971;75:9-14.
2. Glassman A, Shapiro P. Depression and the course of coronary artery disease. Am J Psychiatry 1998;155:4-11.
3. Carney R, Freedland K, Sheline Y, Weiss E. Depression and coronary heart disease: a review for cardiologists. Clin Cardiol 1997;20:196-200.
4. Katon W, Schulbert H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14:237-47.
5. Lesperance F, Frasure-Smith N, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000;160:1354-60.
6. Connerney I, Shapiro P, McLaughlin J, et al. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001;358:1766-71.
7. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction. Circulation 1995;91:999-1005.
8. Rugulies R. Depression as a predictor for coronary heart disease. Am J Prev Med 2002;23:51-61.
9. Wulsin L, Singal B. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003;65:201-10.
10. Carney R, Rich M, Freedland K, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988;50:627-33.
11. Ladwig K, Roll G, Breithardt G, Borggrefe M. Extracardiac contributions to chest pain perception in patients 6 months after acute myocardial infarction. Am Heart J 1999;137:528-34.
12. Levine J, Covino N, Slack W, et al. Psychological predictors of subsequent medical care among patients hospitalized with cardiac disease. J Cardiopulm Rehabil 1996;16:109-16.
13. Lesperance F, Frasure-Smith N, Talajic M, Bourassa M. Five-year risk of cardiac mortality in relation to initial severity and one-year changes in depression symptoms after myocardial infarction. Circulation 2002;105:1049-53.
14. Dwight M, Stoudemire A. Effects of depressive disorders on coronary artery disease: a review. Harv Rev Psychiatry 1997;5:115-122.
15. Penninx B, Beekman A, Honig A, et al. Depression and cardiac mortality. Arch Gen Psychiatry 2001;58:221-7.
16. Writing committee of the ENRICHD investigators. Effects of treating depression and low perceived social support on clinical events after myocardial infarction. JAMA 2003;289:3106-16.
17. Carney RM, Freedland K, Miller G, Jaffe AS. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
18. Musselman D, Evans D, Nemeroff C. The relationship of depression to cardiovascular disease. Arch Gen Psychiatry 1998;55:580-92.
19. Kop WJ. Chronic and acute psychological risk factors for clinical manifestations of coronary artery disease. Psychosom Med 1999;61:476-86.
20. Miller G, Cohen S, Herbert T. Pathways linking major depression and immunity in ambulatory female patients. Psychosom Med 1999;61:850-60.
21. Carney R, Freedland K, Stein P. Change in heart rate and heart rate variability during treatment for depression in patients with coronary heart disease. Psychosom Med 2000;62:639-47.
22. Carney R, Freedland K, Miller G, Jaffe A. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res 2002;53:897-902.
23. Alexopoulos G, Meyers B, Young R, et al. Vascular depression hypothesis. Psychosom Med 1997;58:113-121.
24. Ziegelstein R, Fauerbach J, Stevens S, et al. Patients with depression are less likely to follow recommendations to reduce cardiac risk during recovery from a myocardial infarction. Arch Intern Med 2000;160:1818-23.
25. Glassman AH, O’Connor C, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002;288:701-9.
26. Ko D, Hebert P, Coffey C, et al. B-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA 2002;288:351-7.