Article
Osteochondroma With Contiguous Bronchogenic Cyst of the Scapula
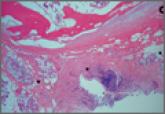
Osteochondroma is a benign bone tumor composed of a bony protrusion with an overlying cartilage cap. Osteochondromas arise in the scapula in 3% to...
Osteochondroma is a benign bone tumor composed of a bony protrusion with an overlying cartilage cap. Osteochondromas arise in the scapula in 3% to...