News
Direct Measurement of T3 Is Likely Vital, Say Researchers
T3 may be an important test to identify subclinical changes in thyroid function, say researchers.
News
Early age at first period raises type 2 diabetes risk
“Women with early-life exposures such as early age at menarche need to be further examined for diabetes and prevention research and strategies for...
News
‘Smart’ stethoscope spots peripartum cardiomyopathy
Finding that 4% of the women in the intervention arm had reduced ejection fraction is “absolutely startling ... and speaks to how important...
News
Better postpartum BP control with self-monitoring: POP-HT
“This trial identifies a potential need for a paradigm shift in the way women affected by hypertensive pregnancy are managed postnatally,” said Dr...
News
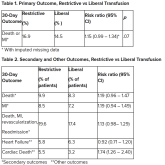
In MI with anemia, results may favor liberal transfusion: MINT
This study is “not a home run,” for the primary outcome, however, many of the outcomes tended to be in favor of a liberal transfusion strategy.
News
Newer antiobesity meds lower the body’s defended fat mass
“These medications change [the defended fat mass] to something that is more normal, rather than ‘fixing’ it.”
News
Beyond semaglutide, a coming pipeline of new antiobesity meds
With the two highest doses of retatrutide, 100% of participants lost ≥ 5% of weight. “I’m not sure how many other times I will ever be able to say...
Audio
What predicts successful weight loss maintenance in WeightWatchers?
Future interventions to prevent weight regain should target overeating in response to internal and external food cues and declines in self-...
News
Antidepressants ‘don’t blunt’ semaglutide and weight loss
“Semaglutide 2.4 mg provides an effective treatment option for weight management, regardless of antidepressant use at baseline.”
News

Alert! A decade of type 2 diabetes shortens life by 3.5 years
“I personally think the findings show that we should treat cardiovascular risk factors more aggressively in people diagnosed with [type 2]...
News
Optimal antiplatelet regimen in ‘bi-risk’ ACS?
OPT-BIRISK tested an antiplatelet strategy “in challenging patients at increased risk for bleeding and ischemic events, but I don’t think we can...
News
Longer edoxaban may benefit cancer patients with distal DVT
“This is the first and only randomized trial to show the superiority of longer duration over shorter duration of anticoagulation therapy for...
News

Muvalaplin and olpasiran show early promise in lowering Lp(a)
“For the first time we have an oral agent” that lowers Lp(a) levels. However, “we will still need to determine if this leads to a reduction in...
News
Cardiac arrest centers no benefit in OHCA without STEMI
On the other hand, patients with MI “will benefit from going straight to a heart attack center and having an attempt at reopening the artery.”
News
ESC issues new guidelines on infective endocarditis
Diagnosing a lethal, rare, but not uncommon disease such as endocarditis “is something that clinicians struggle with every day,” he noted,...