User login
Telemedicine Can Help Solve Intensivist Shortage
Having spent my medical career in the ICU and the hospital, I have followed the recent articles on the struggle to care for ICU patients with interest. Gretchen Henkel’s article on hospitalists filling ICU manpower gaps (“The New Intensivists,” October 2008, p. 1) poses a very real question for community hospitals, which face the greatest challenges in this area. Two issues are common: 1) difficulty in providing 24/7 ICU coverage and 2) the competing priorities that ICU medical leaders face. For these challenges, telemedicine offers a possible solution.
This unique, high-intensity, multidisciplinary approach to the patient population—an integral part of intensivist training—is a proven process shown to have meaningful results in the ICU. However, the team approach to managing ICU patients can be hard to come by. As suggested in Henkel’s article, there are several ways to approach this, but simply having a hospitalist consult on an ICU patient is not, I believe, a solution. Not only can this add to the strain on a hospitalist team, but a proactive approach to the ICU patient also can be hampered by the need for hospitalists to be present in the medical-surgical areas. Ideally, an intensivist should lead a multiprofessional team; however, there is a tremendous intensivist shortage, with less than 20% of ICUs staffed with them. Telemedicine offers a way to bridge the gap of expertise and manpower in many settings, bringing intensivists to the forefront of the ICU multidisciplinary team.
For the multidisciplinary approach to be effective, a physician must be committed to creating the team and identifying the measures that it will impact. In many community hospitals, this is the ICU medical director. However, competing priorities can make this directive difficult to achieve. Teleintensivists, intensivists that practice medicine via telemedicine, proactively establish best practices and a multidisciplinary approach, thus dramatically affecting the quality and financial metrics of the ICU.
Lack of 24/7 ICU coverage is another big challenge for community hospitals. Trying to meet this challenge by simply adding intensivists is likely to be met with defeat, given the shortage of hospitalists. And adding more hospitalists in the ICU continues to drive the hospitalist shortage. There is a variety of solutions for bedside procedures; however, the constant need to respond to phone calls and unpredictable patient interventions remains. While utilizing midlevel providers can help, this approach is not likely to support the demand of the aging population.
Hospitals increasingly are considering telemedicine to meet the 24/7 need. Teleintensivists have risen to add manpower and immediate response to ICU patients. Without the distraction of constant interruptions and with a process to manage the deluge of data, community hospitals with teleintensivist programs are seeing a drop in ventilator-associated pneumonia, better blood glucose management, and compliance with sepsis and other bundles.
This proactive approach to ICU patient care has led to significant decreases in mortality and lengths of stay.
A recent article in The New York Times focused on “disruptive innovation” in healthcare.1 Given the pressing issues facing the industry, disruptive innovation―at the bedside as well as with telemedicine technology―will be a key factor in meeting our ICU needs successfully.
Mary Jo Gorman, MD, MBA
Editor’s note: Dr. Gorman, a former SHM president, is the CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine. TH
Reference
1. Rae-Dupree J. Disruptive innovation, applied to health care. The New York Times Web site. Available at: www.nytimes.com/2009/02/01/business/01unbox.html?scp=1&sq=disruptive%20innovation&st=cse. Accessed March 3, 2009.
Having spent my medical career in the ICU and the hospital, I have followed the recent articles on the struggle to care for ICU patients with interest. Gretchen Henkel’s article on hospitalists filling ICU manpower gaps (“The New Intensivists,” October 2008, p. 1) poses a very real question for community hospitals, which face the greatest challenges in this area. Two issues are common: 1) difficulty in providing 24/7 ICU coverage and 2) the competing priorities that ICU medical leaders face. For these challenges, telemedicine offers a possible solution.
This unique, high-intensity, multidisciplinary approach to the patient population—an integral part of intensivist training—is a proven process shown to have meaningful results in the ICU. However, the team approach to managing ICU patients can be hard to come by. As suggested in Henkel’s article, there are several ways to approach this, but simply having a hospitalist consult on an ICU patient is not, I believe, a solution. Not only can this add to the strain on a hospitalist team, but a proactive approach to the ICU patient also can be hampered by the need for hospitalists to be present in the medical-surgical areas. Ideally, an intensivist should lead a multiprofessional team; however, there is a tremendous intensivist shortage, with less than 20% of ICUs staffed with them. Telemedicine offers a way to bridge the gap of expertise and manpower in many settings, bringing intensivists to the forefront of the ICU multidisciplinary team.
For the multidisciplinary approach to be effective, a physician must be committed to creating the team and identifying the measures that it will impact. In many community hospitals, this is the ICU medical director. However, competing priorities can make this directive difficult to achieve. Teleintensivists, intensivists that practice medicine via telemedicine, proactively establish best practices and a multidisciplinary approach, thus dramatically affecting the quality and financial metrics of the ICU.
Lack of 24/7 ICU coverage is another big challenge for community hospitals. Trying to meet this challenge by simply adding intensivists is likely to be met with defeat, given the shortage of hospitalists. And adding more hospitalists in the ICU continues to drive the hospitalist shortage. There is a variety of solutions for bedside procedures; however, the constant need to respond to phone calls and unpredictable patient interventions remains. While utilizing midlevel providers can help, this approach is not likely to support the demand of the aging population.
Hospitals increasingly are considering telemedicine to meet the 24/7 need. Teleintensivists have risen to add manpower and immediate response to ICU patients. Without the distraction of constant interruptions and with a process to manage the deluge of data, community hospitals with teleintensivist programs are seeing a drop in ventilator-associated pneumonia, better blood glucose management, and compliance with sepsis and other bundles.
This proactive approach to ICU patient care has led to significant decreases in mortality and lengths of stay.
A recent article in The New York Times focused on “disruptive innovation” in healthcare.1 Given the pressing issues facing the industry, disruptive innovation―at the bedside as well as with telemedicine technology―will be a key factor in meeting our ICU needs successfully.
Mary Jo Gorman, MD, MBA
Editor’s note: Dr. Gorman, a former SHM president, is the CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine. TH
Reference
1. Rae-Dupree J. Disruptive innovation, applied to health care. The New York Times Web site. Available at: www.nytimes.com/2009/02/01/business/01unbox.html?scp=1&sq=disruptive%20innovation&st=cse. Accessed March 3, 2009.
Having spent my medical career in the ICU and the hospital, I have followed the recent articles on the struggle to care for ICU patients with interest. Gretchen Henkel’s article on hospitalists filling ICU manpower gaps (“The New Intensivists,” October 2008, p. 1) poses a very real question for community hospitals, which face the greatest challenges in this area. Two issues are common: 1) difficulty in providing 24/7 ICU coverage and 2) the competing priorities that ICU medical leaders face. For these challenges, telemedicine offers a possible solution.
This unique, high-intensity, multidisciplinary approach to the patient population—an integral part of intensivist training—is a proven process shown to have meaningful results in the ICU. However, the team approach to managing ICU patients can be hard to come by. As suggested in Henkel’s article, there are several ways to approach this, but simply having a hospitalist consult on an ICU patient is not, I believe, a solution. Not only can this add to the strain on a hospitalist team, but a proactive approach to the ICU patient also can be hampered by the need for hospitalists to be present in the medical-surgical areas. Ideally, an intensivist should lead a multiprofessional team; however, there is a tremendous intensivist shortage, with less than 20% of ICUs staffed with them. Telemedicine offers a way to bridge the gap of expertise and manpower in many settings, bringing intensivists to the forefront of the ICU multidisciplinary team.
For the multidisciplinary approach to be effective, a physician must be committed to creating the team and identifying the measures that it will impact. In many community hospitals, this is the ICU medical director. However, competing priorities can make this directive difficult to achieve. Teleintensivists, intensivists that practice medicine via telemedicine, proactively establish best practices and a multidisciplinary approach, thus dramatically affecting the quality and financial metrics of the ICU.
Lack of 24/7 ICU coverage is another big challenge for community hospitals. Trying to meet this challenge by simply adding intensivists is likely to be met with defeat, given the shortage of hospitalists. And adding more hospitalists in the ICU continues to drive the hospitalist shortage. There is a variety of solutions for bedside procedures; however, the constant need to respond to phone calls and unpredictable patient interventions remains. While utilizing midlevel providers can help, this approach is not likely to support the demand of the aging population.
Hospitals increasingly are considering telemedicine to meet the 24/7 need. Teleintensivists have risen to add manpower and immediate response to ICU patients. Without the distraction of constant interruptions and with a process to manage the deluge of data, community hospitals with teleintensivist programs are seeing a drop in ventilator-associated pneumonia, better blood glucose management, and compliance with sepsis and other bundles.
This proactive approach to ICU patient care has led to significant decreases in mortality and lengths of stay.
A recent article in The New York Times focused on “disruptive innovation” in healthcare.1 Given the pressing issues facing the industry, disruptive innovation―at the bedside as well as with telemedicine technology―will be a key factor in meeting our ICU needs successfully.
Mary Jo Gorman, MD, MBA
Editor’s note: Dr. Gorman, a former SHM president, is the CEO of St. Louis-based Advanced ICU Care, which provides intensivists to community hospitals using telemedicine. TH
Reference
1. Rae-Dupree J. Disruptive innovation, applied to health care. The New York Times Web site. Available at: www.nytimes.com/2009/02/01/business/01unbox.html?scp=1&sq=disruptive%20innovation&st=cse. Accessed March 3, 2009.
A Fond Farewell

Whatever with the past has gone, the best is always yet to come.
—Lucy Larcom, 19th century poet and writer
It is hard to believe, but this is my last column to write as president of SHM. It has been another remarkable year for hospital medicine. The field continues to grow, and that presents our growing organization with many challenges. Once again, we are rising to the challenge, and it has been a big year at SHM. Most of what we have done has had very little to do with me, but is the result of tremendous work by our many members and our staff.
Just a few highlights of the last 12 months:
- The number of hospitalists surpassed 20,000;
- The number of Hospital Medicine Groups (HMGs) grew to more than 2,000;
- Registration for the SHM Annual Meeting exceeded 1,000 for the first time;
- Almost 200 abstracts were submitted to the SHM Poster Competition;
- The Journal of Hospital Medicine (JHM) published its first issue in 2006 and within a year took its place with established journals by being listed by the National Library of Medicine in PubMed; and
- In a landmark decision, the ABIM Board approved Focused Recognition of Hospital Medicine as part of Internal Medicine Maintenance of Certification.
The board spent two days with our key committee chairmen and staff to examine our current projects and direction. This will lay the groundwork for continuing the dialogue about how we can best serve our members and be prepared to meet the needs of the sea change in healthcare.
- Don Berwick invited SHM leadership to represent the only medical professional society on stage at the Institute for Healthcare Improvement (IHI) Annual Convention as IHI announced its latest national quality improvement campaign;
- SHM embarked on a unique effort to use one-on-one hospitalist leader mentoring to push the implementation of quality improvement to the front lines;
- The SHM board approved funds for a study that will examine the feasibility of a foundation to support research and education in hospital medicine;
- SHM became a player in advocacy when almost 100 hospitalists met with their legislators in Washington, D.C.;
- More than 400 SHM members used the Legislative Action Center to write to their legislators as SHM lobbied Congress to improve Medicare reimbursement; and
- SHM grew into a solid organization with more than $5 million in revenues.
We continue to receive grant funding to support our efforts in quality improvement and to export our resources to the front lines of healthcare. A growing number of organizations recognize our expanding role in caring for the country’s patients. We have a reputation for moving relentlessly forward. This makes us different than many other organizations. It is a characteristic that we need to hold onto as the organization grows and ages.
My best wishes to the next slate of officers and to all of our members. Thank you for the opportunity; it’s been a privilege. There are more great things to come! TH
Dr. Gorman is the outgoing president of SHM.
Whatever with the past has gone, the best is always yet to come.
—Lucy Larcom, 19th century poet and writer
It is hard to believe, but this is my last column to write as president of SHM. It has been another remarkable year for hospital medicine. The field continues to grow, and that presents our growing organization with many challenges. Once again, we are rising to the challenge, and it has been a big year at SHM. Most of what we have done has had very little to do with me, but is the result of tremendous work by our many members and our staff.
Just a few highlights of the last 12 months:
- The number of hospitalists surpassed 20,000;
- The number of Hospital Medicine Groups (HMGs) grew to more than 2,000;
- Registration for the SHM Annual Meeting exceeded 1,000 for the first time;
- Almost 200 abstracts were submitted to the SHM Poster Competition;
- The Journal of Hospital Medicine (JHM) published its first issue in 2006 and within a year took its place with established journals by being listed by the National Library of Medicine in PubMed; and
- In a landmark decision, the ABIM Board approved Focused Recognition of Hospital Medicine as part of Internal Medicine Maintenance of Certification.
The board spent two days with our key committee chairmen and staff to examine our current projects and direction. This will lay the groundwork for continuing the dialogue about how we can best serve our members and be prepared to meet the needs of the sea change in healthcare.
- Don Berwick invited SHM leadership to represent the only medical professional society on stage at the Institute for Healthcare Improvement (IHI) Annual Convention as IHI announced its latest national quality improvement campaign;
- SHM embarked on a unique effort to use one-on-one hospitalist leader mentoring to push the implementation of quality improvement to the front lines;
- The SHM board approved funds for a study that will examine the feasibility of a foundation to support research and education in hospital medicine;
- SHM became a player in advocacy when almost 100 hospitalists met with their legislators in Washington, D.C.;
- More than 400 SHM members used the Legislative Action Center to write to their legislators as SHM lobbied Congress to improve Medicare reimbursement; and
- SHM grew into a solid organization with more than $5 million in revenues.
We continue to receive grant funding to support our efforts in quality improvement and to export our resources to the front lines of healthcare. A growing number of organizations recognize our expanding role in caring for the country’s patients. We have a reputation for moving relentlessly forward. This makes us different than many other organizations. It is a characteristic that we need to hold onto as the organization grows and ages.
My best wishes to the next slate of officers and to all of our members. Thank you for the opportunity; it’s been a privilege. There are more great things to come! TH
Dr. Gorman is the outgoing president of SHM.
Whatever with the past has gone, the best is always yet to come.
—Lucy Larcom, 19th century poet and writer
It is hard to believe, but this is my last column to write as president of SHM. It has been another remarkable year for hospital medicine. The field continues to grow, and that presents our growing organization with many challenges. Once again, we are rising to the challenge, and it has been a big year at SHM. Most of what we have done has had very little to do with me, but is the result of tremendous work by our many members and our staff.
Just a few highlights of the last 12 months:
- The number of hospitalists surpassed 20,000;
- The number of Hospital Medicine Groups (HMGs) grew to more than 2,000;
- Registration for the SHM Annual Meeting exceeded 1,000 for the first time;
- Almost 200 abstracts were submitted to the SHM Poster Competition;
- The Journal of Hospital Medicine (JHM) published its first issue in 2006 and within a year took its place with established journals by being listed by the National Library of Medicine in PubMed; and
- In a landmark decision, the ABIM Board approved Focused Recognition of Hospital Medicine as part of Internal Medicine Maintenance of Certification.
The board spent two days with our key committee chairmen and staff to examine our current projects and direction. This will lay the groundwork for continuing the dialogue about how we can best serve our members and be prepared to meet the needs of the sea change in healthcare.
- Don Berwick invited SHM leadership to represent the only medical professional society on stage at the Institute for Healthcare Improvement (IHI) Annual Convention as IHI announced its latest national quality improvement campaign;
- SHM embarked on a unique effort to use one-on-one hospitalist leader mentoring to push the implementation of quality improvement to the front lines;
- The SHM board approved funds for a study that will examine the feasibility of a foundation to support research and education in hospital medicine;
- SHM became a player in advocacy when almost 100 hospitalists met with their legislators in Washington, D.C.;
- More than 400 SHM members used the Legislative Action Center to write to their legislators as SHM lobbied Congress to improve Medicare reimbursement; and
- SHM grew into a solid organization with more than $5 million in revenues.
We continue to receive grant funding to support our efforts in quality improvement and to export our resources to the front lines of healthcare. A growing number of organizations recognize our expanding role in caring for the country’s patients. We have a reputation for moving relentlessly forward. This makes us different than many other organizations. It is a characteristic that we need to hold onto as the organization grows and ages.
My best wishes to the next slate of officers and to all of our members. Thank you for the opportunity; it’s been a privilege. There are more great things to come! TH
Dr. Gorman is the outgoing president of SHM.
Face the Future

We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
Are You Satisfied?

“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
Learn to Lead

Everyone has it within his power to say, this I am today, that I shall be tomorrow.— Louis L’Amour
Professional advancement means different things to different people. For some, it is important to be the leader of their medical group—whether it is a hospital group or a private practice. For others, it means being associate professor or department chair. And, for a few, it will mean becoming the chief executive officer of a hospital or healthcare company. Much of this comes down to trying to make a difference to the patients and other people around us, as well as trying to bring about improvements in healthcare.
To many physicians, trying to make a difference has been limited to making sure we are doing a good job—diagnostically, pharmacologically, and emotionally—for our individual patients. However, as we become adept at serving the individual patient, we often feel a need to take on more challenges. Medical staff leadership is one way to affect the care of many by directing the actions of the group.
Healthcare is a large component of our country’s economy, and this is not likely to change. In addition, it is an area with many challenges: the aging population, the uninsured population, new pharmaceutical developments, and medical device discoveries. There will be a continued demand for individuals who can understand this very complex intersection of business and medicine.
Fill in the Gaps and Offer Your Help
How many times have we heard our colleagues complain that “the problems never change and nothing gets done around here”? No doubt, change is tough, but taking a role in your department or at your hospital is a way to start. Many hospitalists are filling in the leadership gaps as other specialists move to outpatient centers or into the office. Posts that have traditionally been held by cardiology or urology are changing.
Give some thought to where you might help out. A commitment to something as simple as the Pharmacy and Therapeutics Committee can lead to changes for all the patients as well as get you started on your new career path. Every chief of staff and vice president of medical affairs is looking for volunteers who are interested in projects and can follow through. This applies to department chairmen as well. Given the commitment we all have to our patients and our lives, the offer of help for even just one project is a breath of fresh air to those who have the responsibility for the group or department. Depending on your area of interest—patient safety, quality improvement, patient or medical student education, or process improvement—a project can be created that furthers your institution and addresses your interests.
Worried that there is no room for you at the table? Think again. If your department chair or chief of staff is not asking for help, it may be that their requests have fallen on deaf ears for so long that they have stopped asking. If you have identified a project that interests you, it may interest others also. Ask if there is a way that you can work with others on an existing project. Alternatively, ask if there is a project that needs doing that has no one to do it. Many projects need a political and medical champion; they would welcome your offer to help. Volunteer and be prepared to take on a project that is not your favorite but that may give you experience for other projects. Your initiative will certainly get the attention of the chairperson or others because you are solving a problem for them.
Ask, Listen, and Learn
In addition, this is just a beginning step that will lead to further leadership positions for many. Gaining experience with what works and with how you can accomplish initiatives will lead to bigger opportunities. Embedding yourself in the fabric of your organization provides an opportunity for others to see you work and interact. Seek the advice of those whom you trust and who appear to be successful. Listen to feedback and adjust accordingly. Take classes on leadership, financial performance, process improvement, or in areas that appeal to you and that address what you want to accomplish. Before you know it, you will be chief of staff, division chair, or chief medical officer. Knowing where you want to end up is always an advantage, but many individuals find their way through different experiences and exposures. Sometimes where you end up is not what you expected, but the journey is usually interesting.
Different career choices come at different times. Focusing on family, whether it is making time for children, caring for elderly parents, or supporting a spouse’s career choice may require less career focus for a time. However, as your responsibilities change, new opportunities arise. Finding a mentor or trusted individual who can advise you during these times is helpful.
Develop and Demonstrate Executive Expertise
As the hospital environment changes and hospitalists become the primary providers of care in the acute care setting, they will become hospital coordinators, in conjunction with the emergency department and other specialists. They will develop a knowledge that can be leveraged to improve processes, reduce errors, and improve outcomes. A different set of skills is needed to be successful as an executive. It requires a different way of problem solving; it requires studying and applying new lessons. The successful person develops this new expertise. The effect this person makes in applying these new skills will lead to increased roles and responsibilities. There will be continuing demand for individuals who can access, plan, and implement change within our complex systems. There will also be continuing challenges in healthcare, including the areas of medical education, research, the uninsured, and the aging population. Skills acquired now could be applied as the vice president of medical affairs or as chief medical officer.
Historically, the chief executive officer of a hospital or an integrated system has been a non-medical person with business expertise in healthcare. Hospitalists may fill this role more and more in the future. Many individuals are starting their careers in the hospital. This experience will allow them to develop skills their prior colleagues did not have. It will expose them to teamwork, results orientation, and mentors. We are a young group of professionals with many career years ahead of us. Hospitals are increasingly recognizing that the expertise of committed physician partners is critical to their success. This combination of interest and opportunity will groom many individuals, some of whom will affect healthcare for generations.
Bringing our knowledge of medicine to business, and creating crossroads and interactions, can advance our careers at the same time it improves the healthcare of others. This type of career path is not out of reach for you, and to think it all started with the Pharmacy and Therapeutics Committee. TH
Dr. Gorman is the president of SHM.
Everyone has it within his power to say, this I am today, that I shall be tomorrow.— Louis L’Amour
Professional advancement means different things to different people. For some, it is important to be the leader of their medical group—whether it is a hospital group or a private practice. For others, it means being associate professor or department chair. And, for a few, it will mean becoming the chief executive officer of a hospital or healthcare company. Much of this comes down to trying to make a difference to the patients and other people around us, as well as trying to bring about improvements in healthcare.
To many physicians, trying to make a difference has been limited to making sure we are doing a good job—diagnostically, pharmacologically, and emotionally—for our individual patients. However, as we become adept at serving the individual patient, we often feel a need to take on more challenges. Medical staff leadership is one way to affect the care of many by directing the actions of the group.
Healthcare is a large component of our country’s economy, and this is not likely to change. In addition, it is an area with many challenges: the aging population, the uninsured population, new pharmaceutical developments, and medical device discoveries. There will be a continued demand for individuals who can understand this very complex intersection of business and medicine.
Fill in the Gaps and Offer Your Help
How many times have we heard our colleagues complain that “the problems never change and nothing gets done around here”? No doubt, change is tough, but taking a role in your department or at your hospital is a way to start. Many hospitalists are filling in the leadership gaps as other specialists move to outpatient centers or into the office. Posts that have traditionally been held by cardiology or urology are changing.
Give some thought to where you might help out. A commitment to something as simple as the Pharmacy and Therapeutics Committee can lead to changes for all the patients as well as get you started on your new career path. Every chief of staff and vice president of medical affairs is looking for volunteers who are interested in projects and can follow through. This applies to department chairmen as well. Given the commitment we all have to our patients and our lives, the offer of help for even just one project is a breath of fresh air to those who have the responsibility for the group or department. Depending on your area of interest—patient safety, quality improvement, patient or medical student education, or process improvement—a project can be created that furthers your institution and addresses your interests.
Worried that there is no room for you at the table? Think again. If your department chair or chief of staff is not asking for help, it may be that their requests have fallen on deaf ears for so long that they have stopped asking. If you have identified a project that interests you, it may interest others also. Ask if there is a way that you can work with others on an existing project. Alternatively, ask if there is a project that needs doing that has no one to do it. Many projects need a political and medical champion; they would welcome your offer to help. Volunteer and be prepared to take on a project that is not your favorite but that may give you experience for other projects. Your initiative will certainly get the attention of the chairperson or others because you are solving a problem for them.
Ask, Listen, and Learn
In addition, this is just a beginning step that will lead to further leadership positions for many. Gaining experience with what works and with how you can accomplish initiatives will lead to bigger opportunities. Embedding yourself in the fabric of your organization provides an opportunity for others to see you work and interact. Seek the advice of those whom you trust and who appear to be successful. Listen to feedback and adjust accordingly. Take classes on leadership, financial performance, process improvement, or in areas that appeal to you and that address what you want to accomplish. Before you know it, you will be chief of staff, division chair, or chief medical officer. Knowing where you want to end up is always an advantage, but many individuals find their way through different experiences and exposures. Sometimes where you end up is not what you expected, but the journey is usually interesting.
Different career choices come at different times. Focusing on family, whether it is making time for children, caring for elderly parents, or supporting a spouse’s career choice may require less career focus for a time. However, as your responsibilities change, new opportunities arise. Finding a mentor or trusted individual who can advise you during these times is helpful.
Develop and Demonstrate Executive Expertise
As the hospital environment changes and hospitalists become the primary providers of care in the acute care setting, they will become hospital coordinators, in conjunction with the emergency department and other specialists. They will develop a knowledge that can be leveraged to improve processes, reduce errors, and improve outcomes. A different set of skills is needed to be successful as an executive. It requires a different way of problem solving; it requires studying and applying new lessons. The successful person develops this new expertise. The effect this person makes in applying these new skills will lead to increased roles and responsibilities. There will be continuing demand for individuals who can access, plan, and implement change within our complex systems. There will also be continuing challenges in healthcare, including the areas of medical education, research, the uninsured, and the aging population. Skills acquired now could be applied as the vice president of medical affairs or as chief medical officer.
Historically, the chief executive officer of a hospital or an integrated system has been a non-medical person with business expertise in healthcare. Hospitalists may fill this role more and more in the future. Many individuals are starting their careers in the hospital. This experience will allow them to develop skills their prior colleagues did not have. It will expose them to teamwork, results orientation, and mentors. We are a young group of professionals with many career years ahead of us. Hospitals are increasingly recognizing that the expertise of committed physician partners is critical to their success. This combination of interest and opportunity will groom many individuals, some of whom will affect healthcare for generations.
Bringing our knowledge of medicine to business, and creating crossroads and interactions, can advance our careers at the same time it improves the healthcare of others. This type of career path is not out of reach for you, and to think it all started with the Pharmacy and Therapeutics Committee. TH
Dr. Gorman is the president of SHM.
Everyone has it within his power to say, this I am today, that I shall be tomorrow.— Louis L’Amour
Professional advancement means different things to different people. For some, it is important to be the leader of their medical group—whether it is a hospital group or a private practice. For others, it means being associate professor or department chair. And, for a few, it will mean becoming the chief executive officer of a hospital or healthcare company. Much of this comes down to trying to make a difference to the patients and other people around us, as well as trying to bring about improvements in healthcare.
To many physicians, trying to make a difference has been limited to making sure we are doing a good job—diagnostically, pharmacologically, and emotionally—for our individual patients. However, as we become adept at serving the individual patient, we often feel a need to take on more challenges. Medical staff leadership is one way to affect the care of many by directing the actions of the group.
Healthcare is a large component of our country’s economy, and this is not likely to change. In addition, it is an area with many challenges: the aging population, the uninsured population, new pharmaceutical developments, and medical device discoveries. There will be a continued demand for individuals who can understand this very complex intersection of business and medicine.
Fill in the Gaps and Offer Your Help
How many times have we heard our colleagues complain that “the problems never change and nothing gets done around here”? No doubt, change is tough, but taking a role in your department or at your hospital is a way to start. Many hospitalists are filling in the leadership gaps as other specialists move to outpatient centers or into the office. Posts that have traditionally been held by cardiology or urology are changing.
Give some thought to where you might help out. A commitment to something as simple as the Pharmacy and Therapeutics Committee can lead to changes for all the patients as well as get you started on your new career path. Every chief of staff and vice president of medical affairs is looking for volunteers who are interested in projects and can follow through. This applies to department chairmen as well. Given the commitment we all have to our patients and our lives, the offer of help for even just one project is a breath of fresh air to those who have the responsibility for the group or department. Depending on your area of interest—patient safety, quality improvement, patient or medical student education, or process improvement—a project can be created that furthers your institution and addresses your interests.
Worried that there is no room for you at the table? Think again. If your department chair or chief of staff is not asking for help, it may be that their requests have fallen on deaf ears for so long that they have stopped asking. If you have identified a project that interests you, it may interest others also. Ask if there is a way that you can work with others on an existing project. Alternatively, ask if there is a project that needs doing that has no one to do it. Many projects need a political and medical champion; they would welcome your offer to help. Volunteer and be prepared to take on a project that is not your favorite but that may give you experience for other projects. Your initiative will certainly get the attention of the chairperson or others because you are solving a problem for them.
Ask, Listen, and Learn
In addition, this is just a beginning step that will lead to further leadership positions for many. Gaining experience with what works and with how you can accomplish initiatives will lead to bigger opportunities. Embedding yourself in the fabric of your organization provides an opportunity for others to see you work and interact. Seek the advice of those whom you trust and who appear to be successful. Listen to feedback and adjust accordingly. Take classes on leadership, financial performance, process improvement, or in areas that appeal to you and that address what you want to accomplish. Before you know it, you will be chief of staff, division chair, or chief medical officer. Knowing where you want to end up is always an advantage, but many individuals find their way through different experiences and exposures. Sometimes where you end up is not what you expected, but the journey is usually interesting.
Different career choices come at different times. Focusing on family, whether it is making time for children, caring for elderly parents, or supporting a spouse’s career choice may require less career focus for a time. However, as your responsibilities change, new opportunities arise. Finding a mentor or trusted individual who can advise you during these times is helpful.
Develop and Demonstrate Executive Expertise
As the hospital environment changes and hospitalists become the primary providers of care in the acute care setting, they will become hospital coordinators, in conjunction with the emergency department and other specialists. They will develop a knowledge that can be leveraged to improve processes, reduce errors, and improve outcomes. A different set of skills is needed to be successful as an executive. It requires a different way of problem solving; it requires studying and applying new lessons. The successful person develops this new expertise. The effect this person makes in applying these new skills will lead to increased roles and responsibilities. There will be continuing demand for individuals who can access, plan, and implement change within our complex systems. There will also be continuing challenges in healthcare, including the areas of medical education, research, the uninsured, and the aging population. Skills acquired now could be applied as the vice president of medical affairs or as chief medical officer.
Historically, the chief executive officer of a hospital or an integrated system has been a non-medical person with business expertise in healthcare. Hospitalists may fill this role more and more in the future. Many individuals are starting their careers in the hospital. This experience will allow them to develop skills their prior colleagues did not have. It will expose them to teamwork, results orientation, and mentors. We are a young group of professionals with many career years ahead of us. Hospitals are increasingly recognizing that the expertise of committed physician partners is critical to their success. This combination of interest and opportunity will groom many individuals, some of whom will affect healthcare for generations.
Bringing our knowledge of medicine to business, and creating crossroads and interactions, can advance our careers at the same time it improves the healthcare of others. This type of career path is not out of reach for you, and to think it all started with the Pharmacy and Therapeutics Committee. TH
Dr. Gorman is the president of SHM.
SHM Varietals

Gardens are not made by sitting in the shade.—Rudyard Kipling
For those of us who live in a climate where the vegetation dies in the winter, this is a great time of year. In the spring our plants and trees revive themselves and begin to give us color and aromas. We tend to our plants and add to our gardens with new flowers. We plant our seeds for vegetables and anxiously await the first fruit.
As I watched my garden blossoming this year, I was reminded of our Society. Perhaps, this is too poetic a comparison, but one that I think fits. No garden is pretty if it comprises all the same plant or grass or color. One of the most appealing things about a garden is its great variety. There are many variations of plants: grasses, flowers, trees, and groundcover. In a great garden, there may be many types of grass in many colors and shapes. There are flowers of various kinds. They all bloom at different times from spring to fall. Their colors range from white to the darkest blues and purples. Their fragrances are apparent in the morning or evening or at night. Some of them are phosphorescent. There are rocks and stones, water features, birds, and insects. Each part of the garden has a different role and yet together they create a peaceful and pleasing environment—a place we want to be. Without the many kinds of sites, smells, and sounds, a garden would not be interesting or pleasing to us.
Our organization is like a garden: We have many types of groups that make up the whole. For instance, we have groups of specialties. We are pediatricians. We are family medicine physicians. We are internists.
We have different professions. Our nurse practitioner and physician assistant members have a unique role. Their support of the organization and insights into patient care and care delivery give us all another perspective. In this complex age of pharmacology and polypharmacy, our pharmacy members assist us all in compiling a treatment plan for patients that helps them and does as little harm as possible. They educate us all about the many interactions and side effects of our medications.
We practice in different settings. Some of us see patients at the bedside in a community hospital. There we attempt to bring the best knowledge and skill we can to care for the individual. In addition, we bring our ideas and innovation to all the patients in our hospital by establishing new treatment plans and processes. We educate our nursing staffs and our fellow physicians. We educate our administrators about healthcare changes that can improve our community and our patients. We create liaisons with other specialists in the emergency department, the operating room, and in the ICU. Some of us practice at the bedside in a teaching setting. We care for patients with residents and medical students. We hope to bring to them a good example of empathy and care at the bedside as well as medical knowledge consistent with the best medical practice. Here, we also create liaisons with other specialists in the emergency department, the operating room, and in the ICU. By working in a multidisciplinary fashion, we hope to advance the care of all hospitalized patients.
We contribute by leading research and studies that discover new methods or new types of care. These results guide others at the bedside and in training. We have different interests. Thanks to this diversity we have individuals working on many topics to advance our specialty. Some individuals pursue public policy. They want to advance our field through the actions of the government and the national payers. The members’ focus on education has led to the core competency product, many wonderful national meetings, and active committee work. Those interested in research strive to produce a world-class journal, research opportunities, and a place for all hospitalists’ researchers. Quality and safety are important to our national healthcare. Our members have created resource rooms to disseminate information on these topics. Others, still, want to advance our field through the study of lifestyle and practice setting issues. Finally, we move toward recognition as a board certified specialty.
Regardless of how one looks at our SHM garden, we would be less of an organization without our variety and diversity. We continue to strive to meet the needs of and provide opportunities for all our members, regardless of their interests, practice setting, or discipline. We do not have a finished garden because gardens are always a work in progress, but we hope to continue to be the best place for all hospitalists to grow. TH
Dr. Gorman is the president of SHM.
Gardens are not made by sitting in the shade.—Rudyard Kipling
For those of us who live in a climate where the vegetation dies in the winter, this is a great time of year. In the spring our plants and trees revive themselves and begin to give us color and aromas. We tend to our plants and add to our gardens with new flowers. We plant our seeds for vegetables and anxiously await the first fruit.
As I watched my garden blossoming this year, I was reminded of our Society. Perhaps, this is too poetic a comparison, but one that I think fits. No garden is pretty if it comprises all the same plant or grass or color. One of the most appealing things about a garden is its great variety. There are many variations of plants: grasses, flowers, trees, and groundcover. In a great garden, there may be many types of grass in many colors and shapes. There are flowers of various kinds. They all bloom at different times from spring to fall. Their colors range from white to the darkest blues and purples. Their fragrances are apparent in the morning or evening or at night. Some of them are phosphorescent. There are rocks and stones, water features, birds, and insects. Each part of the garden has a different role and yet together they create a peaceful and pleasing environment—a place we want to be. Without the many kinds of sites, smells, and sounds, a garden would not be interesting or pleasing to us.
Our organization is like a garden: We have many types of groups that make up the whole. For instance, we have groups of specialties. We are pediatricians. We are family medicine physicians. We are internists.
We have different professions. Our nurse practitioner and physician assistant members have a unique role. Their support of the organization and insights into patient care and care delivery give us all another perspective. In this complex age of pharmacology and polypharmacy, our pharmacy members assist us all in compiling a treatment plan for patients that helps them and does as little harm as possible. They educate us all about the many interactions and side effects of our medications.
We practice in different settings. Some of us see patients at the bedside in a community hospital. There we attempt to bring the best knowledge and skill we can to care for the individual. In addition, we bring our ideas and innovation to all the patients in our hospital by establishing new treatment plans and processes. We educate our nursing staffs and our fellow physicians. We educate our administrators about healthcare changes that can improve our community and our patients. We create liaisons with other specialists in the emergency department, the operating room, and in the ICU. Some of us practice at the bedside in a teaching setting. We care for patients with residents and medical students. We hope to bring to them a good example of empathy and care at the bedside as well as medical knowledge consistent with the best medical practice. Here, we also create liaisons with other specialists in the emergency department, the operating room, and in the ICU. By working in a multidisciplinary fashion, we hope to advance the care of all hospitalized patients.
We contribute by leading research and studies that discover new methods or new types of care. These results guide others at the bedside and in training. We have different interests. Thanks to this diversity we have individuals working on many topics to advance our specialty. Some individuals pursue public policy. They want to advance our field through the actions of the government and the national payers. The members’ focus on education has led to the core competency product, many wonderful national meetings, and active committee work. Those interested in research strive to produce a world-class journal, research opportunities, and a place for all hospitalists’ researchers. Quality and safety are important to our national healthcare. Our members have created resource rooms to disseminate information on these topics. Others, still, want to advance our field through the study of lifestyle and practice setting issues. Finally, we move toward recognition as a board certified specialty.
Regardless of how one looks at our SHM garden, we would be less of an organization without our variety and diversity. We continue to strive to meet the needs of and provide opportunities for all our members, regardless of their interests, practice setting, or discipline. We do not have a finished garden because gardens are always a work in progress, but we hope to continue to be the best place for all hospitalists to grow. TH
Dr. Gorman is the president of SHM.
Gardens are not made by sitting in the shade.—Rudyard Kipling
For those of us who live in a climate where the vegetation dies in the winter, this is a great time of year. In the spring our plants and trees revive themselves and begin to give us color and aromas. We tend to our plants and add to our gardens with new flowers. We plant our seeds for vegetables and anxiously await the first fruit.
As I watched my garden blossoming this year, I was reminded of our Society. Perhaps, this is too poetic a comparison, but one that I think fits. No garden is pretty if it comprises all the same plant or grass or color. One of the most appealing things about a garden is its great variety. There are many variations of plants: grasses, flowers, trees, and groundcover. In a great garden, there may be many types of grass in many colors and shapes. There are flowers of various kinds. They all bloom at different times from spring to fall. Their colors range from white to the darkest blues and purples. Their fragrances are apparent in the morning or evening or at night. Some of them are phosphorescent. There are rocks and stones, water features, birds, and insects. Each part of the garden has a different role and yet together they create a peaceful and pleasing environment—a place we want to be. Without the many kinds of sites, smells, and sounds, a garden would not be interesting or pleasing to us.
Our organization is like a garden: We have many types of groups that make up the whole. For instance, we have groups of specialties. We are pediatricians. We are family medicine physicians. We are internists.
We have different professions. Our nurse practitioner and physician assistant members have a unique role. Their support of the organization and insights into patient care and care delivery give us all another perspective. In this complex age of pharmacology and polypharmacy, our pharmacy members assist us all in compiling a treatment plan for patients that helps them and does as little harm as possible. They educate us all about the many interactions and side effects of our medications.
We practice in different settings. Some of us see patients at the bedside in a community hospital. There we attempt to bring the best knowledge and skill we can to care for the individual. In addition, we bring our ideas and innovation to all the patients in our hospital by establishing new treatment plans and processes. We educate our nursing staffs and our fellow physicians. We educate our administrators about healthcare changes that can improve our community and our patients. We create liaisons with other specialists in the emergency department, the operating room, and in the ICU. Some of us practice at the bedside in a teaching setting. We care for patients with residents and medical students. We hope to bring to them a good example of empathy and care at the bedside as well as medical knowledge consistent with the best medical practice. Here, we also create liaisons with other specialists in the emergency department, the operating room, and in the ICU. By working in a multidisciplinary fashion, we hope to advance the care of all hospitalized patients.
We contribute by leading research and studies that discover new methods or new types of care. These results guide others at the bedside and in training. We have different interests. Thanks to this diversity we have individuals working on many topics to advance our specialty. Some individuals pursue public policy. They want to advance our field through the actions of the government and the national payers. The members’ focus on education has led to the core competency product, many wonderful national meetings, and active committee work. Those interested in research strive to produce a world-class journal, research opportunities, and a place for all hospitalists’ researchers. Quality and safety are important to our national healthcare. Our members have created resource rooms to disseminate information on these topics. Others, still, want to advance our field through the study of lifestyle and practice setting issues. Finally, we move toward recognition as a board certified specialty.
Regardless of how one looks at our SHM garden, we would be less of an organization without our variety and diversity. We continue to strive to meet the needs of and provide opportunities for all our members, regardless of their interests, practice setting, or discipline. We do not have a finished garden because gardens are always a work in progress, but we hope to continue to be the best place for all hospitalists to grow. TH
Dr. Gorman is the president of SHM.
The Importance of Following

He who has no faith in others shall find no faith in them.—Lao Tzu
We hear a lot about leading. There are best-selling books on the topic, courses in leading, articles on leading, and admonishments to lead. But is there an art to following? Many of us work on our leadership skills. We spend time trying to better understand those around us and their motivations and interests. We attempt to identify their strengths and engage them in projects that match their skills. We learn to give feedback in constructive ways so that others can improve. We try to understand the other’s perspective.
But when it’s our turn to follow, are we as diligent?
Regardless of our role at the hospital, within our group or in our medical community, we need to follow as well as lead. We may be a leader of our group, but a follower with the rest of the medical staff. We may lead some aspects of patient care, but follow on other aspects. How does our performance as a follower affect the group’s outcomes? Does it matter?
Some would say that there are four fundamental responsibilities of a follower.
Responsibility #1: Don’t act like a victim
As a project or program gets underway don’t be defensive or whine. Attempt to understand the rationale behind the project. Most leaders don’t wake up and invent things to keep people busy. They have a goal that usually addresses underperformance in some area. Operating room turnaround time may not seem important to you—discover why it matters to someone else. When a plan is presented, approach it with an open mind and suggest ways to improve the plan or its implementation. Even if the advantages of change are not apparent to you, give them a try before you make up your mind; you might discover that the new way is an improvement. Be straightforward with your concerns, but once the decision is made, play with the team.
We all knew families of brothers who seemed to fight among themselves. But if an outsider picked on one of them, the group banded together to defend each other. Make sure your team knows that they can count on you. Withdrawing from participation is certain to sabotage a project. Once your behaviors establish your reputation as a person who acts like a victim, you can be sure to be excluded from future projects or participation.
Worse than withdrawing is commiserating with others about your bad situation and demoralizing the group you are in. If you believe that the activity is unfair or dishonest, get outside opinions from other colleagues. Someone who is in another group or another field can be very helpful. In other disciplines (business, agriculture, manufacturing, and law), what you are being asked to do may be accepted as part of change. Solicit several opinions (and not just your family members). And when all is said and done, give it a try. Nothing is forever and every great journey starts with a single step—you might be in for a pleasant surprise.
Responsibility #2: Engage Yourself
Almost no one gets it right from the start. If you have ideas on improvement, not only speak up—take responsibility. Work with the project leader to supervise some part of it or assist in creating a monitoring tool or feedback loop. Every project has a number of tasks that need to be completed; volunteer to take responsibility for some part.
Engage others in finding ways to improve the process. Hospital-based processes are extremely complex and involve many stakeholders, entities, and professions. A number of pieces usually need attention. As the project progresses, be creative. Solve problems with open discussion and make improvements along the way. Focus on the end goal and suggest, implement, and monitor adjustments. Any sizable project will take time. Hospitalists and other physicians are used to seeing action and immediate reaction: Lasix relieves heart failure; nebulizers relieve shortness of breath. However, projects that really change organizations are long and arduous. They are multimonth and many times multiyear. This is quite a learning curve for many practitioners.
Responsibility #3: Do What you say
We certainly expect this of our leaders; we should expect it of ourselves as followers. It is difficult to lead a project when others on the team are late on deadlines or fail to show up. Volunteer to do only what you can. If you are overextended and don’t complete your part, the project can be crippled. Budget your time and energy to successfully meet expectations. If you get stuck on an assignment, ask for help. Delaying until the project is greatly behind can result in loss of your credibility and the whole project coming to a halt. Identify what you don’t know and identify ways to get the information you need. Many facilities and groups have a number of resources to assist you. They have members with experience expertise and other references available. SHM provides resources and online help at your fingertips.
Responsibility #4: stay the course
As mentioned above, the timelines on many projects take weeks and months. Don’t be discouraged if your progress is not as smooth as expected. Remember, you are remaking healthcare. Focus on your strategic priorities: Are they aligned with your patient care values? If you are off track, reanalyze. Look for the ways that the process is failing and revise the process. Maybe the wrong person is assigned to a task that is not to their strength. Review what you were trying to achieve. Maybe there is another path to get there. Follow directions and processes and support the design.
These are some ideas about the responsibilities of a follower. Keep in mind that others need you to follow just as you need them to lead. Performing as a good follower has some outcomes that help you. You can learn important successes with the right leader. The group’s goals can be accomplished more readily. If you can follow others and assist them in being successful with their goals, you can expect them to follow you in return. Have some faith in your leader; work at being a good follower and then you’ll be leading, too!
I would like to recognize the Petrous Group (www.petrous.net) for sharing their material for this column. TH
Dr. Gorman is the president of SHM.
He who has no faith in others shall find no faith in them.—Lao Tzu
We hear a lot about leading. There are best-selling books on the topic, courses in leading, articles on leading, and admonishments to lead. But is there an art to following? Many of us work on our leadership skills. We spend time trying to better understand those around us and their motivations and interests. We attempt to identify their strengths and engage them in projects that match their skills. We learn to give feedback in constructive ways so that others can improve. We try to understand the other’s perspective.
But when it’s our turn to follow, are we as diligent?
Regardless of our role at the hospital, within our group or in our medical community, we need to follow as well as lead. We may be a leader of our group, but a follower with the rest of the medical staff. We may lead some aspects of patient care, but follow on other aspects. How does our performance as a follower affect the group’s outcomes? Does it matter?
Some would say that there are four fundamental responsibilities of a follower.
Responsibility #1: Don’t act like a victim
As a project or program gets underway don’t be defensive or whine. Attempt to understand the rationale behind the project. Most leaders don’t wake up and invent things to keep people busy. They have a goal that usually addresses underperformance in some area. Operating room turnaround time may not seem important to you—discover why it matters to someone else. When a plan is presented, approach it with an open mind and suggest ways to improve the plan or its implementation. Even if the advantages of change are not apparent to you, give them a try before you make up your mind; you might discover that the new way is an improvement. Be straightforward with your concerns, but once the decision is made, play with the team.
We all knew families of brothers who seemed to fight among themselves. But if an outsider picked on one of them, the group banded together to defend each other. Make sure your team knows that they can count on you. Withdrawing from participation is certain to sabotage a project. Once your behaviors establish your reputation as a person who acts like a victim, you can be sure to be excluded from future projects or participation.
Worse than withdrawing is commiserating with others about your bad situation and demoralizing the group you are in. If you believe that the activity is unfair or dishonest, get outside opinions from other colleagues. Someone who is in another group or another field can be very helpful. In other disciplines (business, agriculture, manufacturing, and law), what you are being asked to do may be accepted as part of change. Solicit several opinions (and not just your family members). And when all is said and done, give it a try. Nothing is forever and every great journey starts with a single step—you might be in for a pleasant surprise.
Responsibility #2: Engage Yourself
Almost no one gets it right from the start. If you have ideas on improvement, not only speak up—take responsibility. Work with the project leader to supervise some part of it or assist in creating a monitoring tool or feedback loop. Every project has a number of tasks that need to be completed; volunteer to take responsibility for some part.
Engage others in finding ways to improve the process. Hospital-based processes are extremely complex and involve many stakeholders, entities, and professions. A number of pieces usually need attention. As the project progresses, be creative. Solve problems with open discussion and make improvements along the way. Focus on the end goal and suggest, implement, and monitor adjustments. Any sizable project will take time. Hospitalists and other physicians are used to seeing action and immediate reaction: Lasix relieves heart failure; nebulizers relieve shortness of breath. However, projects that really change organizations are long and arduous. They are multimonth and many times multiyear. This is quite a learning curve for many practitioners.
Responsibility #3: Do What you say
We certainly expect this of our leaders; we should expect it of ourselves as followers. It is difficult to lead a project when others on the team are late on deadlines or fail to show up. Volunteer to do only what you can. If you are overextended and don’t complete your part, the project can be crippled. Budget your time and energy to successfully meet expectations. If you get stuck on an assignment, ask for help. Delaying until the project is greatly behind can result in loss of your credibility and the whole project coming to a halt. Identify what you don’t know and identify ways to get the information you need. Many facilities and groups have a number of resources to assist you. They have members with experience expertise and other references available. SHM provides resources and online help at your fingertips.
Responsibility #4: stay the course
As mentioned above, the timelines on many projects take weeks and months. Don’t be discouraged if your progress is not as smooth as expected. Remember, you are remaking healthcare. Focus on your strategic priorities: Are they aligned with your patient care values? If you are off track, reanalyze. Look for the ways that the process is failing and revise the process. Maybe the wrong person is assigned to a task that is not to their strength. Review what you were trying to achieve. Maybe there is another path to get there. Follow directions and processes and support the design.
These are some ideas about the responsibilities of a follower. Keep in mind that others need you to follow just as you need them to lead. Performing as a good follower has some outcomes that help you. You can learn important successes with the right leader. The group’s goals can be accomplished more readily. If you can follow others and assist them in being successful with their goals, you can expect them to follow you in return. Have some faith in your leader; work at being a good follower and then you’ll be leading, too!
I would like to recognize the Petrous Group (www.petrous.net) for sharing their material for this column. TH
Dr. Gorman is the president of SHM.
He who has no faith in others shall find no faith in them.—Lao Tzu
We hear a lot about leading. There are best-selling books on the topic, courses in leading, articles on leading, and admonishments to lead. But is there an art to following? Many of us work on our leadership skills. We spend time trying to better understand those around us and their motivations and interests. We attempt to identify their strengths and engage them in projects that match their skills. We learn to give feedback in constructive ways so that others can improve. We try to understand the other’s perspective.
But when it’s our turn to follow, are we as diligent?
Regardless of our role at the hospital, within our group or in our medical community, we need to follow as well as lead. We may be a leader of our group, but a follower with the rest of the medical staff. We may lead some aspects of patient care, but follow on other aspects. How does our performance as a follower affect the group’s outcomes? Does it matter?
Some would say that there are four fundamental responsibilities of a follower.
Responsibility #1: Don’t act like a victim
As a project or program gets underway don’t be defensive or whine. Attempt to understand the rationale behind the project. Most leaders don’t wake up and invent things to keep people busy. They have a goal that usually addresses underperformance in some area. Operating room turnaround time may not seem important to you—discover why it matters to someone else. When a plan is presented, approach it with an open mind and suggest ways to improve the plan or its implementation. Even if the advantages of change are not apparent to you, give them a try before you make up your mind; you might discover that the new way is an improvement. Be straightforward with your concerns, but once the decision is made, play with the team.
We all knew families of brothers who seemed to fight among themselves. But if an outsider picked on one of them, the group banded together to defend each other. Make sure your team knows that they can count on you. Withdrawing from participation is certain to sabotage a project. Once your behaviors establish your reputation as a person who acts like a victim, you can be sure to be excluded from future projects or participation.
Worse than withdrawing is commiserating with others about your bad situation and demoralizing the group you are in. If you believe that the activity is unfair or dishonest, get outside opinions from other colleagues. Someone who is in another group or another field can be very helpful. In other disciplines (business, agriculture, manufacturing, and law), what you are being asked to do may be accepted as part of change. Solicit several opinions (and not just your family members). And when all is said and done, give it a try. Nothing is forever and every great journey starts with a single step—you might be in for a pleasant surprise.
Responsibility #2: Engage Yourself
Almost no one gets it right from the start. If you have ideas on improvement, not only speak up—take responsibility. Work with the project leader to supervise some part of it or assist in creating a monitoring tool or feedback loop. Every project has a number of tasks that need to be completed; volunteer to take responsibility for some part.
Engage others in finding ways to improve the process. Hospital-based processes are extremely complex and involve many stakeholders, entities, and professions. A number of pieces usually need attention. As the project progresses, be creative. Solve problems with open discussion and make improvements along the way. Focus on the end goal and suggest, implement, and monitor adjustments. Any sizable project will take time. Hospitalists and other physicians are used to seeing action and immediate reaction: Lasix relieves heart failure; nebulizers relieve shortness of breath. However, projects that really change organizations are long and arduous. They are multimonth and many times multiyear. This is quite a learning curve for many practitioners.
Responsibility #3: Do What you say
We certainly expect this of our leaders; we should expect it of ourselves as followers. It is difficult to lead a project when others on the team are late on deadlines or fail to show up. Volunteer to do only what you can. If you are overextended and don’t complete your part, the project can be crippled. Budget your time and energy to successfully meet expectations. If you get stuck on an assignment, ask for help. Delaying until the project is greatly behind can result in loss of your credibility and the whole project coming to a halt. Identify what you don’t know and identify ways to get the information you need. Many facilities and groups have a number of resources to assist you. They have members with experience expertise and other references available. SHM provides resources and online help at your fingertips.
Responsibility #4: stay the course
As mentioned above, the timelines on many projects take weeks and months. Don’t be discouraged if your progress is not as smooth as expected. Remember, you are remaking healthcare. Focus on your strategic priorities: Are they aligned with your patient care values? If you are off track, reanalyze. Look for the ways that the process is failing and revise the process. Maybe the wrong person is assigned to a task that is not to their strength. Review what you were trying to achieve. Maybe there is another path to get there. Follow directions and processes and support the design.
These are some ideas about the responsibilities of a follower. Keep in mind that others need you to follow just as you need them to lead. Performing as a good follower has some outcomes that help you. You can learn important successes with the right leader. The group’s goals can be accomplished more readily. If you can follow others and assist them in being successful with their goals, you can expect them to follow you in return. Have some faith in your leader; work at being a good follower and then you’ll be leading, too!
I would like to recognize the Petrous Group (www.petrous.net) for sharing their material for this column. TH
Dr. Gorman is the president of SHM.
Facility Partnerships

“There’s no limit to how complicated things can get, on account of one thing always leading to another.”—E.B. White, Charlotte’s Web
E.B. White may not have been talking about hospitalists and their facilities, but he could have been. We are intricately involved in our facilities and, as we begin to make changes for our patients by changing the system and its processes, one thing leads to another.
Why should we bother to have partnerships with our facilities?
Hospitalist medicine has a unique feature: We need a facility to practice in. An ambulatory physician, while maintaining an office, can choose from a number of facilities. Unlike some procedural specialists, we cannot take our patients to an outpatient surgical center or other venue. If our hospital is not performing well, we have a difficult practice situation. It is imperative that we work with our facilities to ensure their success. We can create a rewarding practice environment by creating a highly functioning partnership.
If our goal is to deliver great care to patient populations, we cannot do this alone. In order for us to leverage our specialized knowledge we must leverage and master our partnerships with our facility. Ideally, in a partnership the objectives, values, and approaches are mutually reinforcing. There is agreement on the short-term and long-term goals. By operating with others in this partnership, new levels of unexpected performance are generated.
But partnership is a difficult thing. Though we are intricately entwined with the hospitals in which we practice, often we are not partnering. Partnerships occur at different levels. We may be partnering at a level that does not encourage results. In the dysfunctional partnership, the parties perceive little or no mutual benefit. They apply competitive negotiation skills to get their way regardless of the impact on relationships or outcomes. No one is really committed to anyone. Many times in a partnership, we demand what we want:
- A case manager for our team, seven days a week;
- A better office or computer system;
- Better emergency department procedures; or
- More time off.
Such demands without discussion and without consideration of the other’s point of view occur in a dysfunctional partnership.
But we have the opportunity to move these discussions in a positive manner because there are so many things that we directly control that cause the success or failure of our facilities. Our recognition of these needs can create an opportunity for us to prove our ability to partner. Typically, physicians have not supported administrative initiatives. It is well known that most administrators see the doctors as a project to work around instead of a partner in their success. Indeed for years many doctors established a sport of thwarting administrative plans and ideas; however, we need to proactively establish a new paradigm where we are the partners in improving care for our patient populations. Stuck for ideas on overlapping opportunity? Here are a few thoughts.
Everyone hears about medical record timeliness at their facilities. But why does anyone care about this? Does the Medical Executive Committee like to send out suspension letters? Do the individuals in medical records like to harass doctors? Of course not; this is a matter of vital financial interest to the hospital. The medical record cannot be billed until the record is complete: all consultations, discharge information, admission dictations, and all signatures.
Imagine how it must be to have your income held up because of someone else’s failure to perform. Imagine how frustrated you would be if your paycheck was held up because a nurse had not finish charting. A proactive stance on this mission-critical issue for the hospital demonstrates the group’s commitment to its partner. Taking a proactive stance on this often leads to reorganizing and reworking the medical records department processes. Taking the first step demonstrates your interest in the needs of others. It may lead to an electronic medical record or new systems. A partnership starts to evolve.
Patient satisfaction is a tricky item. It varies greatly and is based on how and when information is collected. We can take the stance that these are flawed results and of no interest to us, or we can choose to identify the key elements that we can affect. By choosing to participate in a project, our partnership can grow. This may mean learning a great detail about something non-medical and then figuring out how to best communicate that to the physician team. It may involve learning from other experts: risk management specialists, skilled executives, and statisticians. It may result in changing the system of collection, reporting, and feedback. This change benefits all parties, not just one over the other.
A project that has great value for our partners is to improve their financial performance by collaborating on documentation. A hospital is paid very differently than a physician. The hospital’s income depends on what physicians write in the chart. This puts them in a position of dependence on physician handwriting! The difficulty for doctors is that the term definitions in some cases do not correspond to medical terms. By creating a program where the physicians meet weekly with a facility expert, dialogue can foster a partnership. The physicians provide the willingness to learn and the facility provides the expertise and time in a supportive manner. The physician gains an appreciation for the idiosyncrasies of hospital payments and can assist in improving the case mix index and diagnosis capture. When hospitalists and the hospital work together the facility becomes more financially stable and, therefore, the future jobs of the hospitalist group become more secure.
Everyone likes working in a happy and safe environment. As part of that environment, we have responsibilities to our fellow workers. We can complain about performance of our non-physicians colleagues or we can proactively partner to improve our relationships with them. In addition to the obvious—treating them with respect and as part of the team—we can create processes to improve their daily work.
How much variation is there among the way your group approaches diagnoses? Can the nursing and pharmacy staff assume a consistent approach for each patient? Our goal—to create care for patient populations not individual patients—must address this. Do you extract their expertise when designing these care programs? It can be of great value to us in assisting our patients and redesigning care. It creates an environment of value and satisfaction that leads to retention. Why do we care about retention? A stable nursing, therapy, social work, and case management staff adds to our daily satisfaction. We can’t get there alone. We need to partner with our co-workers with inclusion and education.
How about the emergency department? There is often a strain in our relationship with these important colleagues. Are we creating programs, process, and guidelines with our professional colleagues that work for everyone? There are many important points of collaboration, and sometimes we need to extend a hand first to get forward momentum.
Some partnerships are characterized by an integration of value and skills—interdependence. Commitment and coordination across activities is a common factor. If our goal is to achieve an excellence in partnering with our facilities, we need to begin the dialogue about what we can accomplish in common that supports both parties. It appears we are interdependent, but moving to partnership is a more mature step.
There are endless projects on which we can collaborate to move our patients, our communities, our facilities, and ourselves to a better place. Let’s start with one action toward one goal. As one thing leads to another, we can achieve things that we never thought possible. TH
Dr. Gorman is the president of SHM.
“There’s no limit to how complicated things can get, on account of one thing always leading to another.”—E.B. White, Charlotte’s Web
E.B. White may not have been talking about hospitalists and their facilities, but he could have been. We are intricately involved in our facilities and, as we begin to make changes for our patients by changing the system and its processes, one thing leads to another.
Why should we bother to have partnerships with our facilities?
Hospitalist medicine has a unique feature: We need a facility to practice in. An ambulatory physician, while maintaining an office, can choose from a number of facilities. Unlike some procedural specialists, we cannot take our patients to an outpatient surgical center or other venue. If our hospital is not performing well, we have a difficult practice situation. It is imperative that we work with our facilities to ensure their success. We can create a rewarding practice environment by creating a highly functioning partnership.
If our goal is to deliver great care to patient populations, we cannot do this alone. In order for us to leverage our specialized knowledge we must leverage and master our partnerships with our facility. Ideally, in a partnership the objectives, values, and approaches are mutually reinforcing. There is agreement on the short-term and long-term goals. By operating with others in this partnership, new levels of unexpected performance are generated.
But partnership is a difficult thing. Though we are intricately entwined with the hospitals in which we practice, often we are not partnering. Partnerships occur at different levels. We may be partnering at a level that does not encourage results. In the dysfunctional partnership, the parties perceive little or no mutual benefit. They apply competitive negotiation skills to get their way regardless of the impact on relationships or outcomes. No one is really committed to anyone. Many times in a partnership, we demand what we want:
- A case manager for our team, seven days a week;
- A better office or computer system;
- Better emergency department procedures; or
- More time off.
Such demands without discussion and without consideration of the other’s point of view occur in a dysfunctional partnership.
But we have the opportunity to move these discussions in a positive manner because there are so many things that we directly control that cause the success or failure of our facilities. Our recognition of these needs can create an opportunity for us to prove our ability to partner. Typically, physicians have not supported administrative initiatives. It is well known that most administrators see the doctors as a project to work around instead of a partner in their success. Indeed for years many doctors established a sport of thwarting administrative plans and ideas; however, we need to proactively establish a new paradigm where we are the partners in improving care for our patient populations. Stuck for ideas on overlapping opportunity? Here are a few thoughts.
Everyone hears about medical record timeliness at their facilities. But why does anyone care about this? Does the Medical Executive Committee like to send out suspension letters? Do the individuals in medical records like to harass doctors? Of course not; this is a matter of vital financial interest to the hospital. The medical record cannot be billed until the record is complete: all consultations, discharge information, admission dictations, and all signatures.
Imagine how it must be to have your income held up because of someone else’s failure to perform. Imagine how frustrated you would be if your paycheck was held up because a nurse had not finish charting. A proactive stance on this mission-critical issue for the hospital demonstrates the group’s commitment to its partner. Taking a proactive stance on this often leads to reorganizing and reworking the medical records department processes. Taking the first step demonstrates your interest in the needs of others. It may lead to an electronic medical record or new systems. A partnership starts to evolve.
Patient satisfaction is a tricky item. It varies greatly and is based on how and when information is collected. We can take the stance that these are flawed results and of no interest to us, or we can choose to identify the key elements that we can affect. By choosing to participate in a project, our partnership can grow. This may mean learning a great detail about something non-medical and then figuring out how to best communicate that to the physician team. It may involve learning from other experts: risk management specialists, skilled executives, and statisticians. It may result in changing the system of collection, reporting, and feedback. This change benefits all parties, not just one over the other.
A project that has great value for our partners is to improve their financial performance by collaborating on documentation. A hospital is paid very differently than a physician. The hospital’s income depends on what physicians write in the chart. This puts them in a position of dependence on physician handwriting! The difficulty for doctors is that the term definitions in some cases do not correspond to medical terms. By creating a program where the physicians meet weekly with a facility expert, dialogue can foster a partnership. The physicians provide the willingness to learn and the facility provides the expertise and time in a supportive manner. The physician gains an appreciation for the idiosyncrasies of hospital payments and can assist in improving the case mix index and diagnosis capture. When hospitalists and the hospital work together the facility becomes more financially stable and, therefore, the future jobs of the hospitalist group become more secure.
Everyone likes working in a happy and safe environment. As part of that environment, we have responsibilities to our fellow workers. We can complain about performance of our non-physicians colleagues or we can proactively partner to improve our relationships with them. In addition to the obvious—treating them with respect and as part of the team—we can create processes to improve their daily work.
How much variation is there among the way your group approaches diagnoses? Can the nursing and pharmacy staff assume a consistent approach for each patient? Our goal—to create care for patient populations not individual patients—must address this. Do you extract their expertise when designing these care programs? It can be of great value to us in assisting our patients and redesigning care. It creates an environment of value and satisfaction that leads to retention. Why do we care about retention? A stable nursing, therapy, social work, and case management staff adds to our daily satisfaction. We can’t get there alone. We need to partner with our co-workers with inclusion and education.
How about the emergency department? There is often a strain in our relationship with these important colleagues. Are we creating programs, process, and guidelines with our professional colleagues that work for everyone? There are many important points of collaboration, and sometimes we need to extend a hand first to get forward momentum.
Some partnerships are characterized by an integration of value and skills—interdependence. Commitment and coordination across activities is a common factor. If our goal is to achieve an excellence in partnering with our facilities, we need to begin the dialogue about what we can accomplish in common that supports both parties. It appears we are interdependent, but moving to partnership is a more mature step.
There are endless projects on which we can collaborate to move our patients, our communities, our facilities, and ourselves to a better place. Let’s start with one action toward one goal. As one thing leads to another, we can achieve things that we never thought possible. TH
Dr. Gorman is the president of SHM.
“There’s no limit to how complicated things can get, on account of one thing always leading to another.”—E.B. White, Charlotte’s Web
E.B. White may not have been talking about hospitalists and their facilities, but he could have been. We are intricately involved in our facilities and, as we begin to make changes for our patients by changing the system and its processes, one thing leads to another.
Why should we bother to have partnerships with our facilities?
Hospitalist medicine has a unique feature: We need a facility to practice in. An ambulatory physician, while maintaining an office, can choose from a number of facilities. Unlike some procedural specialists, we cannot take our patients to an outpatient surgical center or other venue. If our hospital is not performing well, we have a difficult practice situation. It is imperative that we work with our facilities to ensure their success. We can create a rewarding practice environment by creating a highly functioning partnership.
If our goal is to deliver great care to patient populations, we cannot do this alone. In order for us to leverage our specialized knowledge we must leverage and master our partnerships with our facility. Ideally, in a partnership the objectives, values, and approaches are mutually reinforcing. There is agreement on the short-term and long-term goals. By operating with others in this partnership, new levels of unexpected performance are generated.
But partnership is a difficult thing. Though we are intricately entwined with the hospitals in which we practice, often we are not partnering. Partnerships occur at different levels. We may be partnering at a level that does not encourage results. In the dysfunctional partnership, the parties perceive little or no mutual benefit. They apply competitive negotiation skills to get their way regardless of the impact on relationships or outcomes. No one is really committed to anyone. Many times in a partnership, we demand what we want:
- A case manager for our team, seven days a week;
- A better office or computer system;
- Better emergency department procedures; or
- More time off.
Such demands without discussion and without consideration of the other’s point of view occur in a dysfunctional partnership.
But we have the opportunity to move these discussions in a positive manner because there are so many things that we directly control that cause the success or failure of our facilities. Our recognition of these needs can create an opportunity for us to prove our ability to partner. Typically, physicians have not supported administrative initiatives. It is well known that most administrators see the doctors as a project to work around instead of a partner in their success. Indeed for years many doctors established a sport of thwarting administrative plans and ideas; however, we need to proactively establish a new paradigm where we are the partners in improving care for our patient populations. Stuck for ideas on overlapping opportunity? Here are a few thoughts.
Everyone hears about medical record timeliness at their facilities. But why does anyone care about this? Does the Medical Executive Committee like to send out suspension letters? Do the individuals in medical records like to harass doctors? Of course not; this is a matter of vital financial interest to the hospital. The medical record cannot be billed until the record is complete: all consultations, discharge information, admission dictations, and all signatures.
Imagine how it must be to have your income held up because of someone else’s failure to perform. Imagine how frustrated you would be if your paycheck was held up because a nurse had not finish charting. A proactive stance on this mission-critical issue for the hospital demonstrates the group’s commitment to its partner. Taking a proactive stance on this often leads to reorganizing and reworking the medical records department processes. Taking the first step demonstrates your interest in the needs of others. It may lead to an electronic medical record or new systems. A partnership starts to evolve.
Patient satisfaction is a tricky item. It varies greatly and is based on how and when information is collected. We can take the stance that these are flawed results and of no interest to us, or we can choose to identify the key elements that we can affect. By choosing to participate in a project, our partnership can grow. This may mean learning a great detail about something non-medical and then figuring out how to best communicate that to the physician team. It may involve learning from other experts: risk management specialists, skilled executives, and statisticians. It may result in changing the system of collection, reporting, and feedback. This change benefits all parties, not just one over the other.
A project that has great value for our partners is to improve their financial performance by collaborating on documentation. A hospital is paid very differently than a physician. The hospital’s income depends on what physicians write in the chart. This puts them in a position of dependence on physician handwriting! The difficulty for doctors is that the term definitions in some cases do not correspond to medical terms. By creating a program where the physicians meet weekly with a facility expert, dialogue can foster a partnership. The physicians provide the willingness to learn and the facility provides the expertise and time in a supportive manner. The physician gains an appreciation for the idiosyncrasies of hospital payments and can assist in improving the case mix index and diagnosis capture. When hospitalists and the hospital work together the facility becomes more financially stable and, therefore, the future jobs of the hospitalist group become more secure.
Everyone likes working in a happy and safe environment. As part of that environment, we have responsibilities to our fellow workers. We can complain about performance of our non-physicians colleagues or we can proactively partner to improve our relationships with them. In addition to the obvious—treating them with respect and as part of the team—we can create processes to improve their daily work.
How much variation is there among the way your group approaches diagnoses? Can the nursing and pharmacy staff assume a consistent approach for each patient? Our goal—to create care for patient populations not individual patients—must address this. Do you extract their expertise when designing these care programs? It can be of great value to us in assisting our patients and redesigning care. It creates an environment of value and satisfaction that leads to retention. Why do we care about retention? A stable nursing, therapy, social work, and case management staff adds to our daily satisfaction. We can’t get there alone. We need to partner with our co-workers with inclusion and education.
How about the emergency department? There is often a strain in our relationship with these important colleagues. Are we creating programs, process, and guidelines with our professional colleagues that work for everyone? There are many important points of collaboration, and sometimes we need to extend a hand first to get forward momentum.
Some partnerships are characterized by an integration of value and skills—interdependence. Commitment and coordination across activities is a common factor. If our goal is to achieve an excellence in partnering with our facilities, we need to begin the dialogue about what we can accomplish in common that supports both parties. It appears we are interdependent, but moving to partnership is a more mature step.
There are endless projects on which we can collaborate to move our patients, our communities, our facilities, and ourselves to a better place. Let’s start with one action toward one goal. As one thing leads to another, we can achieve things that we never thought possible. TH
Dr. Gorman is the president of SHM.
Hospital Medicine Breaks Through

Opportunity is missed by most people because it is dressed in overalls and looks like work.—Thomas A. Edison, U.S. inventor (1847-1931)
Many revolutions in medicine have come through scientific breakthroughs: penicillin, drug coated cardiac stents, pulse oximetry. We are witnessing a great medical breakthrough based not on science but on work transformation. The traditional approach has required one physician to provide answers to one patient at a time. As knowledge of medicine has increased, this has gradually been supplanted by multiple agencies caring for one patient. This partially coordinated system is not meeting the needs of the public, the patients, or the providers. We have begun the revolution to a new approach to patient care. Not unlike the transformation of car manufacturing in the last century, healthcare participants are re-examining the assumptions about the way we deliver care to patients in various settings.
Hospital medicine is leading the way in this new approach to patient care. This approach is shifting the focus from the single patient to the patient population. It is much easier to see a patient and decide their individual care than to work to change a system of care. Changing the system of care will demand many things of us, including:
- We will learn new ways of doing things. We did not learn systems approaches in medical school or residency. We were going about the business of absorbing and applying medical and technical knowledge to heal those around us. Measuring the quality of what we did, collating results, applying new programs, and re-measuring were not part of our daily learning.
Understanding that poor outcomes are the result of broken systems and not individual mistakes is only the beginning. As systems approaches are applied to throughput issues, pre-operative care, and ICU care, we will transform the care of numerous patients—not just the patient under our individual care. In order to do this, we will embrace new sciences. It is no longer sufficient to place blame on something that did not work correctly. We must engage in the process of identifying root causes and participate in revisions to prevent future errors.
- We will learn to be team players. As doctors our definition of team often means that the doctor is the captain and everyone else takes orders. But in today’s medical complex this is not the definition of a team. The many individuals who deliver care in an often uncoordinated way have expertise that exceeds ours in various aspects of patient care. Collaborating and delegating to each individual’s expertise leads to improved outcomes. Participating while others lead and respecting their contributions is necessary to achieve transformation of hospital care.
- We will develop partnerships with our institutions. The traditional approach of the medical staff as an adversary to the administration no longer holds. That approach will yield to an approach of common goal setting, problem solving, and shared gain. For this we will learn new languages and a new respect for trying to move a complex organization in a new direction.
- We will work under greater scrutiny than physicians before us. The discussion about quality in the past has been—in many ways—lip service. A number of organizations continue to note that we are not creating excellence in healthcare with our current approaches. As the public and private agencies that pay for healthcare increasingly question what they are buying, measurement of and payment for actual results will escalate. We may see the day where institutions and practitioners are paid directly on results achieved and not on the patient encounter that is defined simply as a patient-healthcare interaction.
- We will embrace technology. Given the vast information that needs to be marshaled for use in patient care, the tools of technology will allow us to focus on the bigger picture while we are reminded of small items that need compliance. Exhorting someone to remember all care benchmark items and interventions creates minimal improvement. Harnessing technology to automatically do what is required (or to prompt someone on the care team to do it) allows us to focus on what no one else can do—provide solace, guidance, and advocacy.
- We will learn to be specialists. There is some debate as we evolve on what we should be doing for patients. Who should care for the orthopedic patient? What about the appendicitis patient with no other medical problems? We still think in terms of what is beneath us professionally and what is unnecessary. This is not the thinking of a specialist.
A specialist assumes if they are asked for an opinion that the physician asking recognizes their own knowledge gap and needs assistance. As we become experts in medical care in the hospital, our knowledge will continue to exceed others. Our ability to understand the vagaries of health plan limits, patient care needs, facility and home care availabilities gives us an opportunity to use our expertise to advocate for patients. The recommendations and problem solving that we bring to the bedside are independent of the patient’s diagnosis, age, or gender. If all we give is solace or information, is that not a great enough contribution to the care of a patient?
- We will retrain those in our institutions who have been doing things the same way for many years. Nursing will understand that availability means better job satisfaction for them and more timely care for their patients. We will train others in medical advances and set the protocols and benchmarks in a more timely way. We can leverage the knowledge we have for the great volume of care we deliver, thus bringing to many patients the latest recommendations. In conjunction with our hospital colleagues, pharmacy, nursing, and others, we can create change at a faster pace than has traditionally been possible.
- We will teach those in training programs that this new approach to healthcare includes much more than our ability to pick the correct antibiotic. Our responsibilities are broader than ever before and now include transition management, resource allocation, advocacy for vulnerable and elderly populations, and prevention of hospital and system errors.
- We will define ourselves for others. We will establish our specialty through advocacy, training, and board certification. We will define our role in partnering with our institutions, colleagues, and the healthcare system. We will lead by example to our colleagues and organizations.
- And finally, we will work. We are in a position to transform the system in which we care for patients. This unprecedented opportunity of a lifetime will take dialogue, compromise, and sweat. It will not be an easy task. But as we harness our members’ energy, intelligence, and ideas we will lead the way to a revolutionized healthcare system. Let’s not miss this opportunity. TH
Dr. Gorman is the president of SHM.
Opportunity is missed by most people because it is dressed in overalls and looks like work.—Thomas A. Edison, U.S. inventor (1847-1931)
Many revolutions in medicine have come through scientific breakthroughs: penicillin, drug coated cardiac stents, pulse oximetry. We are witnessing a great medical breakthrough based not on science but on work transformation. The traditional approach has required one physician to provide answers to one patient at a time. As knowledge of medicine has increased, this has gradually been supplanted by multiple agencies caring for one patient. This partially coordinated system is not meeting the needs of the public, the patients, or the providers. We have begun the revolution to a new approach to patient care. Not unlike the transformation of car manufacturing in the last century, healthcare participants are re-examining the assumptions about the way we deliver care to patients in various settings.
Hospital medicine is leading the way in this new approach to patient care. This approach is shifting the focus from the single patient to the patient population. It is much easier to see a patient and decide their individual care than to work to change a system of care. Changing the system of care will demand many things of us, including:
- We will learn new ways of doing things. We did not learn systems approaches in medical school or residency. We were going about the business of absorbing and applying medical and technical knowledge to heal those around us. Measuring the quality of what we did, collating results, applying new programs, and re-measuring were not part of our daily learning.
Understanding that poor outcomes are the result of broken systems and not individual mistakes is only the beginning. As systems approaches are applied to throughput issues, pre-operative care, and ICU care, we will transform the care of numerous patients—not just the patient under our individual care. In order to do this, we will embrace new sciences. It is no longer sufficient to place blame on something that did not work correctly. We must engage in the process of identifying root causes and participate in revisions to prevent future errors.
- We will learn to be team players. As doctors our definition of team often means that the doctor is the captain and everyone else takes orders. But in today’s medical complex this is not the definition of a team. The many individuals who deliver care in an often uncoordinated way have expertise that exceeds ours in various aspects of patient care. Collaborating and delegating to each individual’s expertise leads to improved outcomes. Participating while others lead and respecting their contributions is necessary to achieve transformation of hospital care.
- We will develop partnerships with our institutions. The traditional approach of the medical staff as an adversary to the administration no longer holds. That approach will yield to an approach of common goal setting, problem solving, and shared gain. For this we will learn new languages and a new respect for trying to move a complex organization in a new direction.
- We will work under greater scrutiny than physicians before us. The discussion about quality in the past has been—in many ways—lip service. A number of organizations continue to note that we are not creating excellence in healthcare with our current approaches. As the public and private agencies that pay for healthcare increasingly question what they are buying, measurement of and payment for actual results will escalate. We may see the day where institutions and practitioners are paid directly on results achieved and not on the patient encounter that is defined simply as a patient-healthcare interaction.
- We will embrace technology. Given the vast information that needs to be marshaled for use in patient care, the tools of technology will allow us to focus on the bigger picture while we are reminded of small items that need compliance. Exhorting someone to remember all care benchmark items and interventions creates minimal improvement. Harnessing technology to automatically do what is required (or to prompt someone on the care team to do it) allows us to focus on what no one else can do—provide solace, guidance, and advocacy.
- We will learn to be specialists. There is some debate as we evolve on what we should be doing for patients. Who should care for the orthopedic patient? What about the appendicitis patient with no other medical problems? We still think in terms of what is beneath us professionally and what is unnecessary. This is not the thinking of a specialist.
A specialist assumes if they are asked for an opinion that the physician asking recognizes their own knowledge gap and needs assistance. As we become experts in medical care in the hospital, our knowledge will continue to exceed others. Our ability to understand the vagaries of health plan limits, patient care needs, facility and home care availabilities gives us an opportunity to use our expertise to advocate for patients. The recommendations and problem solving that we bring to the bedside are independent of the patient’s diagnosis, age, or gender. If all we give is solace or information, is that not a great enough contribution to the care of a patient?
- We will retrain those in our institutions who have been doing things the same way for many years. Nursing will understand that availability means better job satisfaction for them and more timely care for their patients. We will train others in medical advances and set the protocols and benchmarks in a more timely way. We can leverage the knowledge we have for the great volume of care we deliver, thus bringing to many patients the latest recommendations. In conjunction with our hospital colleagues, pharmacy, nursing, and others, we can create change at a faster pace than has traditionally been possible.
- We will teach those in training programs that this new approach to healthcare includes much more than our ability to pick the correct antibiotic. Our responsibilities are broader than ever before and now include transition management, resource allocation, advocacy for vulnerable and elderly populations, and prevention of hospital and system errors.
- We will define ourselves for others. We will establish our specialty through advocacy, training, and board certification. We will define our role in partnering with our institutions, colleagues, and the healthcare system. We will lead by example to our colleagues and organizations.
- And finally, we will work. We are in a position to transform the system in which we care for patients. This unprecedented opportunity of a lifetime will take dialogue, compromise, and sweat. It will not be an easy task. But as we harness our members’ energy, intelligence, and ideas we will lead the way to a revolutionized healthcare system. Let’s not miss this opportunity. TH
Dr. Gorman is the president of SHM.
Opportunity is missed by most people because it is dressed in overalls and looks like work.—Thomas A. Edison, U.S. inventor (1847-1931)
Many revolutions in medicine have come through scientific breakthroughs: penicillin, drug coated cardiac stents, pulse oximetry. We are witnessing a great medical breakthrough based not on science but on work transformation. The traditional approach has required one physician to provide answers to one patient at a time. As knowledge of medicine has increased, this has gradually been supplanted by multiple agencies caring for one patient. This partially coordinated system is not meeting the needs of the public, the patients, or the providers. We have begun the revolution to a new approach to patient care. Not unlike the transformation of car manufacturing in the last century, healthcare participants are re-examining the assumptions about the way we deliver care to patients in various settings.
Hospital medicine is leading the way in this new approach to patient care. This approach is shifting the focus from the single patient to the patient population. It is much easier to see a patient and decide their individual care than to work to change a system of care. Changing the system of care will demand many things of us, including:
- We will learn new ways of doing things. We did not learn systems approaches in medical school or residency. We were going about the business of absorbing and applying medical and technical knowledge to heal those around us. Measuring the quality of what we did, collating results, applying new programs, and re-measuring were not part of our daily learning.
Understanding that poor outcomes are the result of broken systems and not individual mistakes is only the beginning. As systems approaches are applied to throughput issues, pre-operative care, and ICU care, we will transform the care of numerous patients—not just the patient under our individual care. In order to do this, we will embrace new sciences. It is no longer sufficient to place blame on something that did not work correctly. We must engage in the process of identifying root causes and participate in revisions to prevent future errors.
- We will learn to be team players. As doctors our definition of team often means that the doctor is the captain and everyone else takes orders. But in today’s medical complex this is not the definition of a team. The many individuals who deliver care in an often uncoordinated way have expertise that exceeds ours in various aspects of patient care. Collaborating and delegating to each individual’s expertise leads to improved outcomes. Participating while others lead and respecting their contributions is necessary to achieve transformation of hospital care.
- We will develop partnerships with our institutions. The traditional approach of the medical staff as an adversary to the administration no longer holds. That approach will yield to an approach of common goal setting, problem solving, and shared gain. For this we will learn new languages and a new respect for trying to move a complex organization in a new direction.
- We will work under greater scrutiny than physicians before us. The discussion about quality in the past has been—in many ways—lip service. A number of organizations continue to note that we are not creating excellence in healthcare with our current approaches. As the public and private agencies that pay for healthcare increasingly question what they are buying, measurement of and payment for actual results will escalate. We may see the day where institutions and practitioners are paid directly on results achieved and not on the patient encounter that is defined simply as a patient-healthcare interaction.
- We will embrace technology. Given the vast information that needs to be marshaled for use in patient care, the tools of technology will allow us to focus on the bigger picture while we are reminded of small items that need compliance. Exhorting someone to remember all care benchmark items and interventions creates minimal improvement. Harnessing technology to automatically do what is required (or to prompt someone on the care team to do it) allows us to focus on what no one else can do—provide solace, guidance, and advocacy.
- We will learn to be specialists. There is some debate as we evolve on what we should be doing for patients. Who should care for the orthopedic patient? What about the appendicitis patient with no other medical problems? We still think in terms of what is beneath us professionally and what is unnecessary. This is not the thinking of a specialist.
A specialist assumes if they are asked for an opinion that the physician asking recognizes their own knowledge gap and needs assistance. As we become experts in medical care in the hospital, our knowledge will continue to exceed others. Our ability to understand the vagaries of health plan limits, patient care needs, facility and home care availabilities gives us an opportunity to use our expertise to advocate for patients. The recommendations and problem solving that we bring to the bedside are independent of the patient’s diagnosis, age, or gender. If all we give is solace or information, is that not a great enough contribution to the care of a patient?
- We will retrain those in our institutions who have been doing things the same way for many years. Nursing will understand that availability means better job satisfaction for them and more timely care for their patients. We will train others in medical advances and set the protocols and benchmarks in a more timely way. We can leverage the knowledge we have for the great volume of care we deliver, thus bringing to many patients the latest recommendations. In conjunction with our hospital colleagues, pharmacy, nursing, and others, we can create change at a faster pace than has traditionally been possible.
- We will teach those in training programs that this new approach to healthcare includes much more than our ability to pick the correct antibiotic. Our responsibilities are broader than ever before and now include transition management, resource allocation, advocacy for vulnerable and elderly populations, and prevention of hospital and system errors.
- We will define ourselves for others. We will establish our specialty through advocacy, training, and board certification. We will define our role in partnering with our institutions, colleagues, and the healthcare system. We will lead by example to our colleagues and organizations.
- And finally, we will work. We are in a position to transform the system in which we care for patients. This unprecedented opportunity of a lifetime will take dialogue, compromise, and sweat. It will not be an easy task. But as we harness our members’ energy, intelligence, and ideas we will lead the way to a revolutionized healthcare system. Let’s not miss this opportunity. TH
Dr. Gorman is the president of SHM.
Five-Year Review of Codes Begins
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
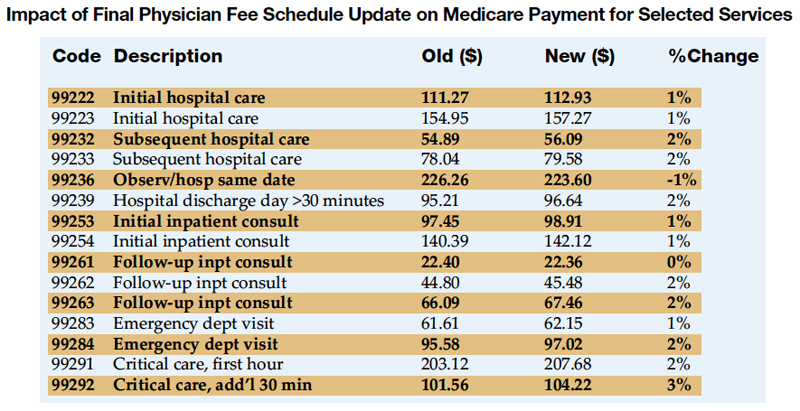
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at mjgorman@ipcm.com.
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at mjgorman@ipcm.com.
The Medicare Physician Fee Schedule indicates how much each physician service will be reimbursed by Medicare. Payment rates are a combination of three components: physician work, practice expense, and professional liability (malpractice). The Centers for Medicare and Medicaid Services (CMS) assigns relative value units (RVU) to each component, largely based on recommendations made by the Relative Value Update Committee (RUC).
Each billing code is to be reviewed at least once every 5 years to determine its RVU. The second Five-Year Review process has just begun and will review physician work RVU. By approximately March 15 this year, the American Medical Association (AMA) will have collected responses. Surveys will be sent to those specialty societies that expressed an interest in surveying the codes. Once the surveys are completed, specialty societies make their coding recommendations to the AMA. The Society of Hospitalist Medicine (SHM) will be making recommendations to the AMA in conjunction with our other colleagues who use similar codes.
In September, the recommendations are forwarded to the RUC for review. The RUC recommendations are then forwarded to CMS for consideration. Once CMS has completed their review, they typically publish a Notice of Proposed Rulemaking (NPRM) on Five-Year Review in March (in this case, March 2006). The Final Rule is expected to be released November 2006, and the new physician work RVU assignments will be implemented January 1, 2007.
Many cognitive specialty groups began to organize before the current Five-Year Review process started, in order to more efficiently coordinate efforts regarding codes of mutual interest. SHM has joined other such specialties in signing on to a unified letter to CMS regarding this Five-Year Review.
The 2005 Physician Fee Schedule was recently released. Below are the rates for selected services frequently rendered by hospitalists.
Dr. Gorman can be contacted at mjgorman@ipcm.com.