Article

Miliarial Gout in an Immunocompromised Patient
Immunocompromised status may be a risk factor for miliarial gout, especially in patients with a history of gout or hyperuricemia.
Article
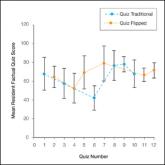
A Comparison of Knowledge Acquisition and Perceived Efficacy of a Traditional vs Flipped Classroom–Based Dermatology Residency Curriculum
Flipped and traditional classroom models were compared in the Duke University Medical Center (Durham, North Carolina) dermatology residency...