User login
Children born from frozen embryos may have increased cancer risk
, a large registry study suggests.
The results, however, “should be interpreted cautiously,” the authors noted, given the low number of cancer cases reported among children born using FET.
Still, the findings do “raise concerns considering the increasing use of FET, in particular freeze-all strategies without clear medical indications,” the authors concluded.
The study was published online in PLOS Medicine.
The number of children born after FET has increased globally and even exceeds the number of those born after fresh embryo transfer in many countries. In the United States, for instance, the FET rate has doubled since 2015; FETs constituted almost 80% of all embryo transfers using assisted reproductive technology (ART) without a donor in 2019.
Despite the benefits associated with FET, which include improved embryo survival and higher live birth rates, some previous research has hinted at a higher risk of childhood cancer in this population.
In the current study, researchers from the University of Gothenburg, Sweden, wanted to better understand the risk of childhood cancer following FET. The investigators analyzed data from 171,774 children born via ART, including 22,630 born after FET, as well as roughly 7.7 million children born after spontaneous conception in Denmark, Finland, Norway, and Sweden.
After a mean follow-up of about 10 years, the incidence rate of cancer diagnosed before age 18 years was 16.7 per 100,000 person-years for children born after spontaneous conception (16,184 cases) and 19.3 per 100,000 person-years for children born after ART (329 cases).
The researchers found no increased risk of cancer before age 18 years in the group of children conceived via ART compared with those conceived spontaneously.
However, children born after FET had a significantly higher risk of cancer compared with children born after fresh embryo transfer (adjusted hazard ratio [aHR], 1.59) and spontaneous conception (aHR, 1.65). Specifically with regard to ART, the incidence rate for those born after FET was 30.1 per 100,000 person-years – 48 total cases – compared with 18.8 per 1000,000 person-years after fresh embryo transfer.
Adjustment for macrosomia, birth weight, or major birth defects influenced the association only marginally.
For specific cancer types, children born after FET had more than a twofold higher risk for leukemia in comparison with those born after fresh embryo transfer (aHR, 2.25) and spontaneous conception (aHR, 2.22).
Still, the authors said these results should be interpreted “cautiously,” given the small number of children diagnosed with cancer after FET. The researchers also acknowledged that they do not know why children born after FET would face a higher risk of cancer.
These findings, however, do align with those from a 2019 Dutch population-based study. In the Dutch study, which included more than 24,000 ART-conceived children and more than 23,000 naturally conceived children, the risk of cancer after ART was not higher overall, but it was greater when only those conceived after FET were considered (aHR 1.80); this increased risk, however, was not statistically significant.
“Since the use of FET is substantially increasing, it is important to tease out whether the increased cancer risk is a true risk increase due to the ART procedures using FET, or due to chance or confounding by other factors,” authors of the 2019 Dutch study, Mandy Spaan, PhD, and Flora E. van Leeuwen, PhD, said in an interview.
“But, as childhood cancer is (fortunately) a rare disease, it is very difficult to study this research question among ART children due to limited numbers,” said Dr. Spaan and Dr. van Leeuwen, who are with the Netherlands Cancer Institute.
Given this, the two experts call for additional large population-based cohort studies to investigate the risk of cancer after ART, especially FET, and for a subsequent analysis that pools these data. They hope this strategy “will lead to reliable estimates” and provide information on the risks of FET in comparison with approaches that involve fresh embryos.
The current study had no commercial funding. The study authors as well as Dr. Spaan and Dr. van Leeuwen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a large registry study suggests.
The results, however, “should be interpreted cautiously,” the authors noted, given the low number of cancer cases reported among children born using FET.
Still, the findings do “raise concerns considering the increasing use of FET, in particular freeze-all strategies without clear medical indications,” the authors concluded.
The study was published online in PLOS Medicine.
The number of children born after FET has increased globally and even exceeds the number of those born after fresh embryo transfer in many countries. In the United States, for instance, the FET rate has doubled since 2015; FETs constituted almost 80% of all embryo transfers using assisted reproductive technology (ART) without a donor in 2019.
Despite the benefits associated with FET, which include improved embryo survival and higher live birth rates, some previous research has hinted at a higher risk of childhood cancer in this population.
In the current study, researchers from the University of Gothenburg, Sweden, wanted to better understand the risk of childhood cancer following FET. The investigators analyzed data from 171,774 children born via ART, including 22,630 born after FET, as well as roughly 7.7 million children born after spontaneous conception in Denmark, Finland, Norway, and Sweden.
After a mean follow-up of about 10 years, the incidence rate of cancer diagnosed before age 18 years was 16.7 per 100,000 person-years for children born after spontaneous conception (16,184 cases) and 19.3 per 100,000 person-years for children born after ART (329 cases).
The researchers found no increased risk of cancer before age 18 years in the group of children conceived via ART compared with those conceived spontaneously.
However, children born after FET had a significantly higher risk of cancer compared with children born after fresh embryo transfer (adjusted hazard ratio [aHR], 1.59) and spontaneous conception (aHR, 1.65). Specifically with regard to ART, the incidence rate for those born after FET was 30.1 per 100,000 person-years – 48 total cases – compared with 18.8 per 1000,000 person-years after fresh embryo transfer.
Adjustment for macrosomia, birth weight, or major birth defects influenced the association only marginally.
For specific cancer types, children born after FET had more than a twofold higher risk for leukemia in comparison with those born after fresh embryo transfer (aHR, 2.25) and spontaneous conception (aHR, 2.22).
Still, the authors said these results should be interpreted “cautiously,” given the small number of children diagnosed with cancer after FET. The researchers also acknowledged that they do not know why children born after FET would face a higher risk of cancer.
These findings, however, do align with those from a 2019 Dutch population-based study. In the Dutch study, which included more than 24,000 ART-conceived children and more than 23,000 naturally conceived children, the risk of cancer after ART was not higher overall, but it was greater when only those conceived after FET were considered (aHR 1.80); this increased risk, however, was not statistically significant.
“Since the use of FET is substantially increasing, it is important to tease out whether the increased cancer risk is a true risk increase due to the ART procedures using FET, or due to chance or confounding by other factors,” authors of the 2019 Dutch study, Mandy Spaan, PhD, and Flora E. van Leeuwen, PhD, said in an interview.
“But, as childhood cancer is (fortunately) a rare disease, it is very difficult to study this research question among ART children due to limited numbers,” said Dr. Spaan and Dr. van Leeuwen, who are with the Netherlands Cancer Institute.
Given this, the two experts call for additional large population-based cohort studies to investigate the risk of cancer after ART, especially FET, and for a subsequent analysis that pools these data. They hope this strategy “will lead to reliable estimates” and provide information on the risks of FET in comparison with approaches that involve fresh embryos.
The current study had no commercial funding. The study authors as well as Dr. Spaan and Dr. van Leeuwen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a large registry study suggests.
The results, however, “should be interpreted cautiously,” the authors noted, given the low number of cancer cases reported among children born using FET.
Still, the findings do “raise concerns considering the increasing use of FET, in particular freeze-all strategies without clear medical indications,” the authors concluded.
The study was published online in PLOS Medicine.
The number of children born after FET has increased globally and even exceeds the number of those born after fresh embryo transfer in many countries. In the United States, for instance, the FET rate has doubled since 2015; FETs constituted almost 80% of all embryo transfers using assisted reproductive technology (ART) without a donor in 2019.
Despite the benefits associated with FET, which include improved embryo survival and higher live birth rates, some previous research has hinted at a higher risk of childhood cancer in this population.
In the current study, researchers from the University of Gothenburg, Sweden, wanted to better understand the risk of childhood cancer following FET. The investigators analyzed data from 171,774 children born via ART, including 22,630 born after FET, as well as roughly 7.7 million children born after spontaneous conception in Denmark, Finland, Norway, and Sweden.
After a mean follow-up of about 10 years, the incidence rate of cancer diagnosed before age 18 years was 16.7 per 100,000 person-years for children born after spontaneous conception (16,184 cases) and 19.3 per 100,000 person-years for children born after ART (329 cases).
The researchers found no increased risk of cancer before age 18 years in the group of children conceived via ART compared with those conceived spontaneously.
However, children born after FET had a significantly higher risk of cancer compared with children born after fresh embryo transfer (adjusted hazard ratio [aHR], 1.59) and spontaneous conception (aHR, 1.65). Specifically with regard to ART, the incidence rate for those born after FET was 30.1 per 100,000 person-years – 48 total cases – compared with 18.8 per 1000,000 person-years after fresh embryo transfer.
Adjustment for macrosomia, birth weight, or major birth defects influenced the association only marginally.
For specific cancer types, children born after FET had more than a twofold higher risk for leukemia in comparison with those born after fresh embryo transfer (aHR, 2.25) and spontaneous conception (aHR, 2.22).
Still, the authors said these results should be interpreted “cautiously,” given the small number of children diagnosed with cancer after FET. The researchers also acknowledged that they do not know why children born after FET would face a higher risk of cancer.
These findings, however, do align with those from a 2019 Dutch population-based study. In the Dutch study, which included more than 24,000 ART-conceived children and more than 23,000 naturally conceived children, the risk of cancer after ART was not higher overall, but it was greater when only those conceived after FET were considered (aHR 1.80); this increased risk, however, was not statistically significant.
“Since the use of FET is substantially increasing, it is important to tease out whether the increased cancer risk is a true risk increase due to the ART procedures using FET, or due to chance or confounding by other factors,” authors of the 2019 Dutch study, Mandy Spaan, PhD, and Flora E. van Leeuwen, PhD, said in an interview.
“But, as childhood cancer is (fortunately) a rare disease, it is very difficult to study this research question among ART children due to limited numbers,” said Dr. Spaan and Dr. van Leeuwen, who are with the Netherlands Cancer Institute.
Given this, the two experts call for additional large population-based cohort studies to investigate the risk of cancer after ART, especially FET, and for a subsequent analysis that pools these data. They hope this strategy “will lead to reliable estimates” and provide information on the risks of FET in comparison with approaches that involve fresh embryos.
The current study had no commercial funding. The study authors as well as Dr. Spaan and Dr. van Leeuwen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PLOS MEDICINE
USPSTF recommends anxiety screening in adults younger than 65
For the first time, the task force is recommending screening all adults aged 64 and younger for anxiety – including pregnant and postpartum women.
This “B” recommendation reflects “moderate certainty” evidence that screening for anxiety in this population has a moderate net benefit, the task force notes in a draft recommendation statement posted on its website.
The recommendation applies to adults aged 19-64 years who do not have a diagnosed mental health disorder or are not showing recognized signs or symptoms of anxiety.
Anxiety disorders are common and often go unrecognized in primary care, leading to long delays in treatment, the task force writes. They add that more evidence is needed to identify ideal screening intervals for all populations.
“A pragmatic approach in the absence of data might include screening all adults who have not been screened previously and using clinical judgment in consideration of risk factors, comorbid conditions, and life events to determine if additional screening of high-risk patients is warranted,” they write.
For adults aged 65 and older, the task force found “insufficient” evidence on the benefits and potential harms of screening for anxiety.
“Evidence on the accuracy of screening tools and the benefits and harms of screening and treatment of screen-detected anxiety in older adults is lacking, and the balance of benefits and harms cannot be determined,” they write.
Jury out on screening for suicide risk
The task force is continuing to recommend screening all adults for depression. This “B” recommendation reflects moderate-certainty evidence that screening for major depression in adults has a moderate net benefit.
However, they note there is not enough evidence to recommend for or against screening for suicide risk in all adults.
They therefore issued an “I” statement, indicating that the balance of benefits and harms cannot be determined at present.
“To address the critical need for supporting the mental health of adults in primary care, the Task Force reviewed the evidence on screening for anxiety, depression, and suicide risk,” task force member Lori Pbert, PhD, University of Massachusetts, Worcester, said in a news release.
“The good news is that screening all adults for depression, including those who are pregnant and postpartum, and screening adults younger than 65 for anxiety can help identify these conditions early so people can be connected to care,” Dr. Pbert said.
“Unfortunately, evidence is limited on screening adults 65 or older for anxiety and screening all adults for suicide risk, so we are urgently calling for more research,” added task force member Gbenga Ogedegbe, MD, MPH, founding director of the Institute for Excellence in Health Equity at NYU Langone Health.
Dr. Ogedegbe, also a professor at New York University, noted that “in the absence of evidence, health care professionals should use their judgment based on individual patient circumstances when determining whether or not to screen.”
The public comment period for the draft recommendations runs until Oct. 17.
A version of this article first appeared on Medscape.com.
For the first time, the task force is recommending screening all adults aged 64 and younger for anxiety – including pregnant and postpartum women.
This “B” recommendation reflects “moderate certainty” evidence that screening for anxiety in this population has a moderate net benefit, the task force notes in a draft recommendation statement posted on its website.
The recommendation applies to adults aged 19-64 years who do not have a diagnosed mental health disorder or are not showing recognized signs or symptoms of anxiety.
Anxiety disorders are common and often go unrecognized in primary care, leading to long delays in treatment, the task force writes. They add that more evidence is needed to identify ideal screening intervals for all populations.
“A pragmatic approach in the absence of data might include screening all adults who have not been screened previously and using clinical judgment in consideration of risk factors, comorbid conditions, and life events to determine if additional screening of high-risk patients is warranted,” they write.
For adults aged 65 and older, the task force found “insufficient” evidence on the benefits and potential harms of screening for anxiety.
“Evidence on the accuracy of screening tools and the benefits and harms of screening and treatment of screen-detected anxiety in older adults is lacking, and the balance of benefits and harms cannot be determined,” they write.
Jury out on screening for suicide risk
The task force is continuing to recommend screening all adults for depression. This “B” recommendation reflects moderate-certainty evidence that screening for major depression in adults has a moderate net benefit.
However, they note there is not enough evidence to recommend for or against screening for suicide risk in all adults.
They therefore issued an “I” statement, indicating that the balance of benefits and harms cannot be determined at present.
“To address the critical need for supporting the mental health of adults in primary care, the Task Force reviewed the evidence on screening for anxiety, depression, and suicide risk,” task force member Lori Pbert, PhD, University of Massachusetts, Worcester, said in a news release.
“The good news is that screening all adults for depression, including those who are pregnant and postpartum, and screening adults younger than 65 for anxiety can help identify these conditions early so people can be connected to care,” Dr. Pbert said.
“Unfortunately, evidence is limited on screening adults 65 or older for anxiety and screening all adults for suicide risk, so we are urgently calling for more research,” added task force member Gbenga Ogedegbe, MD, MPH, founding director of the Institute for Excellence in Health Equity at NYU Langone Health.
Dr. Ogedegbe, also a professor at New York University, noted that “in the absence of evidence, health care professionals should use their judgment based on individual patient circumstances when determining whether or not to screen.”
The public comment period for the draft recommendations runs until Oct. 17.
A version of this article first appeared on Medscape.com.
For the first time, the task force is recommending screening all adults aged 64 and younger for anxiety – including pregnant and postpartum women.
This “B” recommendation reflects “moderate certainty” evidence that screening for anxiety in this population has a moderate net benefit, the task force notes in a draft recommendation statement posted on its website.
The recommendation applies to adults aged 19-64 years who do not have a diagnosed mental health disorder or are not showing recognized signs or symptoms of anxiety.
Anxiety disorders are common and often go unrecognized in primary care, leading to long delays in treatment, the task force writes. They add that more evidence is needed to identify ideal screening intervals for all populations.
“A pragmatic approach in the absence of data might include screening all adults who have not been screened previously and using clinical judgment in consideration of risk factors, comorbid conditions, and life events to determine if additional screening of high-risk patients is warranted,” they write.
For adults aged 65 and older, the task force found “insufficient” evidence on the benefits and potential harms of screening for anxiety.
“Evidence on the accuracy of screening tools and the benefits and harms of screening and treatment of screen-detected anxiety in older adults is lacking, and the balance of benefits and harms cannot be determined,” they write.
Jury out on screening for suicide risk
The task force is continuing to recommend screening all adults for depression. This “B” recommendation reflects moderate-certainty evidence that screening for major depression in adults has a moderate net benefit.
However, they note there is not enough evidence to recommend for or against screening for suicide risk in all adults.
They therefore issued an “I” statement, indicating that the balance of benefits and harms cannot be determined at present.
“To address the critical need for supporting the mental health of adults in primary care, the Task Force reviewed the evidence on screening for anxiety, depression, and suicide risk,” task force member Lori Pbert, PhD, University of Massachusetts, Worcester, said in a news release.
“The good news is that screening all adults for depression, including those who are pregnant and postpartum, and screening adults younger than 65 for anxiety can help identify these conditions early so people can be connected to care,” Dr. Pbert said.
“Unfortunately, evidence is limited on screening adults 65 or older for anxiety and screening all adults for suicide risk, so we are urgently calling for more research,” added task force member Gbenga Ogedegbe, MD, MPH, founding director of the Institute for Excellence in Health Equity at NYU Langone Health.
Dr. Ogedegbe, also a professor at New York University, noted that “in the absence of evidence, health care professionals should use their judgment based on individual patient circumstances when determining whether or not to screen.”
The public comment period for the draft recommendations runs until Oct. 17.
A version of this article first appeared on Medscape.com.
Sugary drinks linked to obesity-related cancer deaths
The study, which included more than 900,000 participants, contributes to previous research suggesting that sugary beverages increase the risk of cancer and cancer-related mortality.
A more surprising finding is that consuming artificially sweetened beverages was linked to an increased risk of death from pancreatic cancer.

“This finding is very interesting,” said Marjorie McCullough, ScD, RD, senior scientific director of epidemiology research, American Cancer Society. She noted that other studies that examined an association between artificially sweetened beverages and pancreatic cancer did not reveal a statistically significant association.
“Our study is the first, to our knowledge, that has found a statistically significant positive association, and it will be important to replicate this finding,” said Dr. McCullough.
The study was published online in Cancer, Epidemiology, Biomarkers, and Prevention.
In the study, Dr. McCullough and colleagues examined associations between drinking sugar-sweetened and artificially sweetened beverages and dying from any cancer or any obesity-related cancers. The researchers also examined this association for 20 individual cancer types.
Participants included 934,777 cancer-free adults from the Cancer Prevention Study-II (CPS-II) prospective cohort. At baseline, adults completed a questionnaire on their medical history, lifestyle exposures, and habits, including how many sugar-sweetened or artificially sweetened drinks they typically consumed each day.
Over a median 28-year follow-up, 135,093 participants died from cancer.
Overall, the researchers determined that consuming two or more sugar-sweetened beverages daily (vs. consuming none) was not associated with all-cancer mortality.
Regarding obesity-related cancers, Dr. McCullough and colleagues found a significant 5% increased risk of death from these cancer (hazard ratio, 1.05); however, this association disappeared after controlling for body mass index (BMI). According to Dr. McCullough, this finding may signal that the association between sugary drinks and obesity-related cancer deaths is at least partly mediated by higher BMI, or excess body fat.
“Weight control is key to cancer prevention,” noted Linda Van Horn, RD, chief of the nutrition division at the Feinberg School of Medicine, Northwestern University, Chicago, who wasn’t involved in the study.
However, with regard to individual cancers, consuming two or more sugar-sweetened drinks each day was associated with an increased risk of dying from colorectal cancer (HR, 1.09) and kidney cancer (HR, 1.17) after adjusting for BMI.
Unexpectedly, sugary beverage intake was associated with a lower risk of esophageal and lung cancer mortality. This association held for lung cancer but not esophageal cancer after restricting the analysis to never-smoking participants (HR, 0.81; 95% confidence interval, 0.70-0.94).
Artificial sweetener and pancreatic cancer?
With respect to artificially sweetened drinks, consuming two or more beverages daily was associated with a 5% increased risk of death from obesity-related cancers (HR, 1.05), but that association became null after controlling for BMI.
However, the link to pancreatic cancer mortality remained after adjusting for BMI (HR, 1.11). This association should be studied further, the researchers say. They say there is a possibility that undiagnosed diabetes influenced the results.
“Continued research on the impact of both beverage types with cancer risk and mortality is warranted to determine whether these associations are causal or confounded by other lifestyle factors and whether they are mediated through BMI,” the researchers write.
Reached for comment, Marcus DaSilva Goncalves, MD, PhD, with Weill Cornell Medicine, New York, noted that the association with colorectal cancer has been previously reported, and he agreed that these “findings strengthen the available evidence of an association between sugar-sweetened beverages and colorectal cancer mortality.”
“Data from my lab in mice have shown that sugar-sweetened beverages deliver fructose directly to colon tumors, which stimulates the survival of cancer cells and growth of tumors,” Dr. Goncalves said.
There are also recent clinical data suggesting that exposure to sugar-sweetened beverages during adolescence and adulthood promotes adenoma formation, the precursor to colorectal cancer, he said.
Regarding artificially sweetened beverage intake, Dr. Goncalves said the effect with pancreatic cancer is “surprising” and that he is not aware of other data, including data from several large studies, that support this relationship.
No specific funding for study has been reported. Dr. McCullough, Ms. Van Horn, and Dr. Goncalves have disclosed no relevant disclosures relationships.
A version of this article first appeared on Medscape.com.
The study, which included more than 900,000 participants, contributes to previous research suggesting that sugary beverages increase the risk of cancer and cancer-related mortality.
A more surprising finding is that consuming artificially sweetened beverages was linked to an increased risk of death from pancreatic cancer.
“This finding is very interesting,” said Marjorie McCullough, ScD, RD, senior scientific director of epidemiology research, American Cancer Society. She noted that other studies that examined an association between artificially sweetened beverages and pancreatic cancer did not reveal a statistically significant association.
“Our study is the first, to our knowledge, that has found a statistically significant positive association, and it will be important to replicate this finding,” said Dr. McCullough.
The study was published online in Cancer, Epidemiology, Biomarkers, and Prevention.
In the study, Dr. McCullough and colleagues examined associations between drinking sugar-sweetened and artificially sweetened beverages and dying from any cancer or any obesity-related cancers. The researchers also examined this association for 20 individual cancer types.
Participants included 934,777 cancer-free adults from the Cancer Prevention Study-II (CPS-II) prospective cohort. At baseline, adults completed a questionnaire on their medical history, lifestyle exposures, and habits, including how many sugar-sweetened or artificially sweetened drinks they typically consumed each day.
Over a median 28-year follow-up, 135,093 participants died from cancer.
Overall, the researchers determined that consuming two or more sugar-sweetened beverages daily (vs. consuming none) was not associated with all-cancer mortality.
Regarding obesity-related cancers, Dr. McCullough and colleagues found a significant 5% increased risk of death from these cancer (hazard ratio, 1.05); however, this association disappeared after controlling for body mass index (BMI). According to Dr. McCullough, this finding may signal that the association between sugary drinks and obesity-related cancer deaths is at least partly mediated by higher BMI, or excess body fat.
“Weight control is key to cancer prevention,” noted Linda Van Horn, RD, chief of the nutrition division at the Feinberg School of Medicine, Northwestern University, Chicago, who wasn’t involved in the study.
However, with regard to individual cancers, consuming two or more sugar-sweetened drinks each day was associated with an increased risk of dying from colorectal cancer (HR, 1.09) and kidney cancer (HR, 1.17) after adjusting for BMI.
Unexpectedly, sugary beverage intake was associated with a lower risk of esophageal and lung cancer mortality. This association held for lung cancer but not esophageal cancer after restricting the analysis to never-smoking participants (HR, 0.81; 95% confidence interval, 0.70-0.94).
Artificial sweetener and pancreatic cancer?
With respect to artificially sweetened drinks, consuming two or more beverages daily was associated with a 5% increased risk of death from obesity-related cancers (HR, 1.05), but that association became null after controlling for BMI.
However, the link to pancreatic cancer mortality remained after adjusting for BMI (HR, 1.11). This association should be studied further, the researchers say. They say there is a possibility that undiagnosed diabetes influenced the results.
“Continued research on the impact of both beverage types with cancer risk and mortality is warranted to determine whether these associations are causal or confounded by other lifestyle factors and whether they are mediated through BMI,” the researchers write.
Reached for comment, Marcus DaSilva Goncalves, MD, PhD, with Weill Cornell Medicine, New York, noted that the association with colorectal cancer has been previously reported, and he agreed that these “findings strengthen the available evidence of an association between sugar-sweetened beverages and colorectal cancer mortality.”
“Data from my lab in mice have shown that sugar-sweetened beverages deliver fructose directly to colon tumors, which stimulates the survival of cancer cells and growth of tumors,” Dr. Goncalves said.
There are also recent clinical data suggesting that exposure to sugar-sweetened beverages during adolescence and adulthood promotes adenoma formation, the precursor to colorectal cancer, he said.
Regarding artificially sweetened beverage intake, Dr. Goncalves said the effect with pancreatic cancer is “surprising” and that he is not aware of other data, including data from several large studies, that support this relationship.
No specific funding for study has been reported. Dr. McCullough, Ms. Van Horn, and Dr. Goncalves have disclosed no relevant disclosures relationships.
A version of this article first appeared on Medscape.com.
The study, which included more than 900,000 participants, contributes to previous research suggesting that sugary beverages increase the risk of cancer and cancer-related mortality.
A more surprising finding is that consuming artificially sweetened beverages was linked to an increased risk of death from pancreatic cancer.
“This finding is very interesting,” said Marjorie McCullough, ScD, RD, senior scientific director of epidemiology research, American Cancer Society. She noted that other studies that examined an association between artificially sweetened beverages and pancreatic cancer did not reveal a statistically significant association.
“Our study is the first, to our knowledge, that has found a statistically significant positive association, and it will be important to replicate this finding,” said Dr. McCullough.
The study was published online in Cancer, Epidemiology, Biomarkers, and Prevention.
In the study, Dr. McCullough and colleagues examined associations between drinking sugar-sweetened and artificially sweetened beverages and dying from any cancer or any obesity-related cancers. The researchers also examined this association for 20 individual cancer types.
Participants included 934,777 cancer-free adults from the Cancer Prevention Study-II (CPS-II) prospective cohort. At baseline, adults completed a questionnaire on their medical history, lifestyle exposures, and habits, including how many sugar-sweetened or artificially sweetened drinks they typically consumed each day.
Over a median 28-year follow-up, 135,093 participants died from cancer.
Overall, the researchers determined that consuming two or more sugar-sweetened beverages daily (vs. consuming none) was not associated with all-cancer mortality.
Regarding obesity-related cancers, Dr. McCullough and colleagues found a significant 5% increased risk of death from these cancer (hazard ratio, 1.05); however, this association disappeared after controlling for body mass index (BMI). According to Dr. McCullough, this finding may signal that the association between sugary drinks and obesity-related cancer deaths is at least partly mediated by higher BMI, or excess body fat.
“Weight control is key to cancer prevention,” noted Linda Van Horn, RD, chief of the nutrition division at the Feinberg School of Medicine, Northwestern University, Chicago, who wasn’t involved in the study.
However, with regard to individual cancers, consuming two or more sugar-sweetened drinks each day was associated with an increased risk of dying from colorectal cancer (HR, 1.09) and kidney cancer (HR, 1.17) after adjusting for BMI.
Unexpectedly, sugary beverage intake was associated with a lower risk of esophageal and lung cancer mortality. This association held for lung cancer but not esophageal cancer after restricting the analysis to never-smoking participants (HR, 0.81; 95% confidence interval, 0.70-0.94).
Artificial sweetener and pancreatic cancer?
With respect to artificially sweetened drinks, consuming two or more beverages daily was associated with a 5% increased risk of death from obesity-related cancers (HR, 1.05), but that association became null after controlling for BMI.
However, the link to pancreatic cancer mortality remained after adjusting for BMI (HR, 1.11). This association should be studied further, the researchers say. They say there is a possibility that undiagnosed diabetes influenced the results.
“Continued research on the impact of both beverage types with cancer risk and mortality is warranted to determine whether these associations are causal or confounded by other lifestyle factors and whether they are mediated through BMI,” the researchers write.
Reached for comment, Marcus DaSilva Goncalves, MD, PhD, with Weill Cornell Medicine, New York, noted that the association with colorectal cancer has been previously reported, and he agreed that these “findings strengthen the available evidence of an association between sugar-sweetened beverages and colorectal cancer mortality.”
“Data from my lab in mice have shown that sugar-sweetened beverages deliver fructose directly to colon tumors, which stimulates the survival of cancer cells and growth of tumors,” Dr. Goncalves said.
There are also recent clinical data suggesting that exposure to sugar-sweetened beverages during adolescence and adulthood promotes adenoma formation, the precursor to colorectal cancer, he said.
Regarding artificially sweetened beverage intake, Dr. Goncalves said the effect with pancreatic cancer is “surprising” and that he is not aware of other data, including data from several large studies, that support this relationship.
No specific funding for study has been reported. Dr. McCullough, Ms. Van Horn, and Dr. Goncalves have disclosed no relevant disclosures relationships.
A version of this article first appeared on Medscape.com.
FROM CANCER, EPIDEMIOLOGY, BIOMARKERS, AND PREVENTION
Is acetaminophen really safer than NSAIDs in heart disease?
New research calls into question the assumption that acetaminophen is safer than NSAIDs for patients with known cardiovascular disease (CVD) or CVD risk factors.
The analysis found a significant correlation between the use of acetaminophen and elevated systolic blood pressure.
While acetaminophen may still be safer than NSAIDs from a bleeding risk standpoint, or in patients with known kidney disease, “the gap may not be as large as once thought,” Rahul Gupta, MD, cardiologist with Lehigh Valley Health Network, Allentown, Pa., said in an interview.

“Cautious use is recommended over the long term, especially in patients with pre-existing hypertension or cardiovascular risk factors,” Dr. Gupta said.
The study was presented at the Hypertension Scientific Sessions, San Diego, sponsored by the American Heart Association.
Acetaminophen is one of the most widely used over-the-counter medications, as it is considered a safer medication for long-term use since it lacks the anti-inflammatory effects of NSAIDs, Dr. Gupta explained.
NSAIDs have been known to raise blood pressure, but the effect of acetaminophen in this regard has not been well studied. Observational studies have shown contradictory results in terms of its effect on blood pressure, he noted.
To investigate further, Dr. Gupta and colleagues did a meta-analysis of three studies that compared the effect of acetaminophen (3-4 g/day) versus placebo on systolic and diastolic ambulatory blood pressure in patients with heart disease or hypertension. Together, the studies included 172 adults (mean age, 60 years; 73% male).
They found that patients receiving acetaminophen had significantly higher systolic blood pressure, compared with those receiving placebo (standard mean difference [SMD] = 0.35; 95% confidence interval, 0.08-0.63; P = .01).
Subgroup analysis of the effect on hypertensive patients showed significant change in systolic blood pressure as well (SMD = 0.38; 95% CI, 0.05-0.71; P = .02).
“Interestingly, there was no significant difference in the effect on diastolic blood pressure,” Dr. Gupta commented.
Reached for comment, Timothy S. Anderson, MD, clinical investigator in the Division of General Medicine at Beth Israel Deaconess Medical Center and assistant professor of medicine at the Harvard Medical School, both in Boston, said this is “an interesting and not particularly well-known issue.”
“However, most of the trials look at very high doses of acetaminophen use (for example, six to eight of the 500 mg pills each day) so we don’t really know whether the more common patterns of using one to two acetaminophen pills every once in a while is problematic,” Dr. Anderson told this news organization.
“We also don’t have data showing a direct harm from these medications with regards to strokes or heart attacks or other downstream consequences of high blood pressure. Ideally we would need a head-to-head trial comparing ibuprofen-type medications to acetaminophen-type medications,” Dr. Anderson said.
The study had no specific funding. Dr. Gupta and Dr. Anderson reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
New research calls into question the assumption that acetaminophen is safer than NSAIDs for patients with known cardiovascular disease (CVD) or CVD risk factors.
The analysis found a significant correlation between the use of acetaminophen and elevated systolic blood pressure.
While acetaminophen may still be safer than NSAIDs from a bleeding risk standpoint, or in patients with known kidney disease, “the gap may not be as large as once thought,” Rahul Gupta, MD, cardiologist with Lehigh Valley Health Network, Allentown, Pa., said in an interview.
“Cautious use is recommended over the long term, especially in patients with pre-existing hypertension or cardiovascular risk factors,” Dr. Gupta said.
The study was presented at the Hypertension Scientific Sessions, San Diego, sponsored by the American Heart Association.
Acetaminophen is one of the most widely used over-the-counter medications, as it is considered a safer medication for long-term use since it lacks the anti-inflammatory effects of NSAIDs, Dr. Gupta explained.
NSAIDs have been known to raise blood pressure, but the effect of acetaminophen in this regard has not been well studied. Observational studies have shown contradictory results in terms of its effect on blood pressure, he noted.
To investigate further, Dr. Gupta and colleagues did a meta-analysis of three studies that compared the effect of acetaminophen (3-4 g/day) versus placebo on systolic and diastolic ambulatory blood pressure in patients with heart disease or hypertension. Together, the studies included 172 adults (mean age, 60 years; 73% male).
They found that patients receiving acetaminophen had significantly higher systolic blood pressure, compared with those receiving placebo (standard mean difference [SMD] = 0.35; 95% confidence interval, 0.08-0.63; P = .01).
Subgroup analysis of the effect on hypertensive patients showed significant change in systolic blood pressure as well (SMD = 0.38; 95% CI, 0.05-0.71; P = .02).
“Interestingly, there was no significant difference in the effect on diastolic blood pressure,” Dr. Gupta commented.
Reached for comment, Timothy S. Anderson, MD, clinical investigator in the Division of General Medicine at Beth Israel Deaconess Medical Center and assistant professor of medicine at the Harvard Medical School, both in Boston, said this is “an interesting and not particularly well-known issue.”
“However, most of the trials look at very high doses of acetaminophen use (for example, six to eight of the 500 mg pills each day) so we don’t really know whether the more common patterns of using one to two acetaminophen pills every once in a while is problematic,” Dr. Anderson told this news organization.
“We also don’t have data showing a direct harm from these medications with regards to strokes or heart attacks or other downstream consequences of high blood pressure. Ideally we would need a head-to-head trial comparing ibuprofen-type medications to acetaminophen-type medications,” Dr. Anderson said.
The study had no specific funding. Dr. Gupta and Dr. Anderson reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
New research calls into question the assumption that acetaminophen is safer than NSAIDs for patients with known cardiovascular disease (CVD) or CVD risk factors.
The analysis found a significant correlation between the use of acetaminophen and elevated systolic blood pressure.
While acetaminophen may still be safer than NSAIDs from a bleeding risk standpoint, or in patients with known kidney disease, “the gap may not be as large as once thought,” Rahul Gupta, MD, cardiologist with Lehigh Valley Health Network, Allentown, Pa., said in an interview.
“Cautious use is recommended over the long term, especially in patients with pre-existing hypertension or cardiovascular risk factors,” Dr. Gupta said.
The study was presented at the Hypertension Scientific Sessions, San Diego, sponsored by the American Heart Association.
Acetaminophen is one of the most widely used over-the-counter medications, as it is considered a safer medication for long-term use since it lacks the anti-inflammatory effects of NSAIDs, Dr. Gupta explained.
NSAIDs have been known to raise blood pressure, but the effect of acetaminophen in this regard has not been well studied. Observational studies have shown contradictory results in terms of its effect on blood pressure, he noted.
To investigate further, Dr. Gupta and colleagues did a meta-analysis of three studies that compared the effect of acetaminophen (3-4 g/day) versus placebo on systolic and diastolic ambulatory blood pressure in patients with heart disease or hypertension. Together, the studies included 172 adults (mean age, 60 years; 73% male).
They found that patients receiving acetaminophen had significantly higher systolic blood pressure, compared with those receiving placebo (standard mean difference [SMD] = 0.35; 95% confidence interval, 0.08-0.63; P = .01).
Subgroup analysis of the effect on hypertensive patients showed significant change in systolic blood pressure as well (SMD = 0.38; 95% CI, 0.05-0.71; P = .02).
“Interestingly, there was no significant difference in the effect on diastolic blood pressure,” Dr. Gupta commented.
Reached for comment, Timothy S. Anderson, MD, clinical investigator in the Division of General Medicine at Beth Israel Deaconess Medical Center and assistant professor of medicine at the Harvard Medical School, both in Boston, said this is “an interesting and not particularly well-known issue.”
“However, most of the trials look at very high doses of acetaminophen use (for example, six to eight of the 500 mg pills each day) so we don’t really know whether the more common patterns of using one to two acetaminophen pills every once in a while is problematic,” Dr. Anderson told this news organization.
“We also don’t have data showing a direct harm from these medications with regards to strokes or heart attacks or other downstream consequences of high blood pressure. Ideally we would need a head-to-head trial comparing ibuprofen-type medications to acetaminophen-type medications,” Dr. Anderson said.
The study had no specific funding. Dr. Gupta and Dr. Anderson reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM HYPERTENSION 2022
Continuous cuffless monitoring may fuel lifestyle change to lower BP
Wearing a cuffless device on the wrist to continuously monitor blood pressure was associated with a significantly lower systolic BP at 6 months among hypertensive adults, real-world results from Europe show.
“We don’t know what they did to reduce their blood pressure,” Jay Shah, MD, Division of Cardiology, Mayo Clinic Arizona, Phoenix, told this news organization.
“The idea is that because they were exposed to their data on a continual basis, that may have prompted them to do something that led to an improvement in their blood pressure, whether it be exercise more, go to their doctor, or change their medication,” said Dr. Shah, who is also chief medical officer for Aktiia.
Dr. Shah presented the study at the Hypertension Scientific Sessions, San Diego.
Empowering data
The study used the Aktiia 24/7 BP monitor; Atkiia funded the trial. The monitor passively and continually monitors BP values from photoplethysmography signals collected via optical sensors at the wrist.
After initial individualized calibration using a cuff-based reference, BP measurements are displayed on a smartphone app, allowing users to consistently monitor their own BP for long periods of time.
Aktiia received CE mark in Europe in January 2021 and is currently under review by the U.S. Food and Drug Administration.
Dr. Shah and colleagues analyzed systolic BP (SBP) trends among 838 real-world Aktiia users in Europe (age 57 ± 11 years; 14% women) who consistently used the monitor for 6 months.
Altogether, they had data on 375 (± 287) app interactions, 3,646 (± 1,417) cuffless readings per user, and 9 (± 7) cuff readings per user.
Traditional cuff SBP averages were calculated monthly and compared with the SBP average of the first month. A t-test analysis was used to detect the difference in SBP between the first and successive months.
On the basis of the mean SBP calculated over 6 months, 136 participants were hypertensive (SBP > 140 mm Hg) and the rest had SBP less than 140 mm Hg.
Hypertensive users saw a statistically significant reduction in SBP of –3.2 mm Hg (95% CI, –0.70 to –5.59; P < .02), beginning at 3 months of continual cuffless BP monitoring, which was sustained through 6 months.
Among users with SBP less than 140 mm Hg, the mean SBP remained unchanged.
“The magnitude of improvement might look modest, but even a 5 mm Hg reduction in systolic BP correlates to a 10% decrease in cardiovascular risk,” Dr. Shah told this news organization.
He noted that “one of the major hurdles is that people may not be aware they have high blood pressure because they don’t feel it. And with a regular cuff, they’ll only see that number when they actually check their blood pressure, which is extremely rare, even for people who have hypertension.”
“Having the ability to show someone their continual blood pressure picture really empowers them to do something to make changes and to be aware, [as well as] to be a more active participant in their health,” Dr. Shah said.
He said that a good analogy is diabetes management, which has transitioned from single finger-stick glucose monitoring to continuous glucose monitoring that provides a complete 24/7 picture of glucose levels.
Transforming technology
Offering perspective on the study, Harlan Krumholz, MD, SM, with Yale New Haven Hospital and Yale School of Medicine, New Haven, Conn., said that having an accurate, affordable, unobtrusive cuffless continuous BP monitor would “transform” BP management.

“This could unlock an era of precision BP management with empowerment of patients to view and act on their numbers,” Dr. Krumholz said in an interview.
“We need data to be confident in the devices – and then research to best leverage the streams of information – and strategies to optimize its use in practice,” Dr. Krumholz added.
“Like any new innovation, we need to mitigate risks and monitor for unintended adverse consequences, but I am bullish on the future of cuffless continuous BP monitors,” Dr. Krumholz said.
Dr. Krumholz said that he “applauds Aktiia for doing studies that assess the effect of the information they are producing on BP over time. We need to know that new approaches not only generate valid information but that they can improve health.”
Ready for prime time?
In June, the European Society of Hypertension issued a statement noting that cuffless BP measurement is a fast-growing and promising field with considerable potential for improving hypertension awareness, management, and control, but because the accuracy of these new devices has not yet been validated, they are not yet suitable for clinical use.
Also providing perspective, Stephen Juraschek, MD, PhD, research director, Hypertension Center of Excellence at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston, said that “there is a lot of interest in cuffless BP monitors due to their ease of measurement, comfort, and ability to obtain BP measurements in multiple settings and environments, and this study showed that the monitoring improved BP over time.”
“It is believed that the increased awareness and feedback may promote healthier behaviors aimed at lowering BP. However, this result should not be conflated with the accuracy of these monitors,” Dr. Juraschek cautioned.
He also noted that there is still no formally approved validation protocol by the Association for the Advancement of Medical Instrumentation.
“While a number of cuffless devices are cleared by the FDA through its 510k mechanism (that is, demonstration of device equivalence), there is no formal stamp of approval or attestation that the measurements are accurate,” Dr. Juraschek said in an interview.
In his view, “more work is needed to understand the validity of these devices. For now, validated, cuff-based home devices are recommended for BP measurement at home, while further work is done to determine the accuracy of these cuffless technologies.”
The study was funded by Aktiia. Dr. Shah is an employee of the company. Dr. Krumholz has no relevant disclosures. Dr. Juraschek is a member of the Validate BP review committee and the AAMI sphygmomanometer committee.
A version of this article first appeared on Medscape.com.
Wearing a cuffless device on the wrist to continuously monitor blood pressure was associated with a significantly lower systolic BP at 6 months among hypertensive adults, real-world results from Europe show.
“We don’t know what they did to reduce their blood pressure,” Jay Shah, MD, Division of Cardiology, Mayo Clinic Arizona, Phoenix, told this news organization.
“The idea is that because they were exposed to their data on a continual basis, that may have prompted them to do something that led to an improvement in their blood pressure, whether it be exercise more, go to their doctor, or change their medication,” said Dr. Shah, who is also chief medical officer for Aktiia.
Dr. Shah presented the study at the Hypertension Scientific Sessions, San Diego.
Empowering data
The study used the Aktiia 24/7 BP monitor; Atkiia funded the trial. The monitor passively and continually monitors BP values from photoplethysmography signals collected via optical sensors at the wrist.
After initial individualized calibration using a cuff-based reference, BP measurements are displayed on a smartphone app, allowing users to consistently monitor their own BP for long periods of time.
Aktiia received CE mark in Europe in January 2021 and is currently under review by the U.S. Food and Drug Administration.
Dr. Shah and colleagues analyzed systolic BP (SBP) trends among 838 real-world Aktiia users in Europe (age 57 ± 11 years; 14% women) who consistently used the monitor for 6 months.
Altogether, they had data on 375 (± 287) app interactions, 3,646 (± 1,417) cuffless readings per user, and 9 (± 7) cuff readings per user.
Traditional cuff SBP averages were calculated monthly and compared with the SBP average of the first month. A t-test analysis was used to detect the difference in SBP between the first and successive months.
On the basis of the mean SBP calculated over 6 months, 136 participants were hypertensive (SBP > 140 mm Hg) and the rest had SBP less than 140 mm Hg.
Hypertensive users saw a statistically significant reduction in SBP of –3.2 mm Hg (95% CI, –0.70 to –5.59; P < .02), beginning at 3 months of continual cuffless BP monitoring, which was sustained through 6 months.
Among users with SBP less than 140 mm Hg, the mean SBP remained unchanged.
“The magnitude of improvement might look modest, but even a 5 mm Hg reduction in systolic BP correlates to a 10% decrease in cardiovascular risk,” Dr. Shah told this news organization.
He noted that “one of the major hurdles is that people may not be aware they have high blood pressure because they don’t feel it. And with a regular cuff, they’ll only see that number when they actually check their blood pressure, which is extremely rare, even for people who have hypertension.”
“Having the ability to show someone their continual blood pressure picture really empowers them to do something to make changes and to be aware, [as well as] to be a more active participant in their health,” Dr. Shah said.
He said that a good analogy is diabetes management, which has transitioned from single finger-stick glucose monitoring to continuous glucose monitoring that provides a complete 24/7 picture of glucose levels.
Transforming technology
Offering perspective on the study, Harlan Krumholz, MD, SM, with Yale New Haven Hospital and Yale School of Medicine, New Haven, Conn., said that having an accurate, affordable, unobtrusive cuffless continuous BP monitor would “transform” BP management.
“This could unlock an era of precision BP management with empowerment of patients to view and act on their numbers,” Dr. Krumholz said in an interview.
“We need data to be confident in the devices – and then research to best leverage the streams of information – and strategies to optimize its use in practice,” Dr. Krumholz added.
“Like any new innovation, we need to mitigate risks and monitor for unintended adverse consequences, but I am bullish on the future of cuffless continuous BP monitors,” Dr. Krumholz said.
Dr. Krumholz said that he “applauds Aktiia for doing studies that assess the effect of the information they are producing on BP over time. We need to know that new approaches not only generate valid information but that they can improve health.”
Ready for prime time?
In June, the European Society of Hypertension issued a statement noting that cuffless BP measurement is a fast-growing and promising field with considerable potential for improving hypertension awareness, management, and control, but because the accuracy of these new devices has not yet been validated, they are not yet suitable for clinical use.
Also providing perspective, Stephen Juraschek, MD, PhD, research director, Hypertension Center of Excellence at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston, said that “there is a lot of interest in cuffless BP monitors due to their ease of measurement, comfort, and ability to obtain BP measurements in multiple settings and environments, and this study showed that the monitoring improved BP over time.”
“It is believed that the increased awareness and feedback may promote healthier behaviors aimed at lowering BP. However, this result should not be conflated with the accuracy of these monitors,” Dr. Juraschek cautioned.
He also noted that there is still no formally approved validation protocol by the Association for the Advancement of Medical Instrumentation.
“While a number of cuffless devices are cleared by the FDA through its 510k mechanism (that is, demonstration of device equivalence), there is no formal stamp of approval or attestation that the measurements are accurate,” Dr. Juraschek said in an interview.
In his view, “more work is needed to understand the validity of these devices. For now, validated, cuff-based home devices are recommended for BP measurement at home, while further work is done to determine the accuracy of these cuffless technologies.”
The study was funded by Aktiia. Dr. Shah is an employee of the company. Dr. Krumholz has no relevant disclosures. Dr. Juraschek is a member of the Validate BP review committee and the AAMI sphygmomanometer committee.
A version of this article first appeared on Medscape.com.
Wearing a cuffless device on the wrist to continuously monitor blood pressure was associated with a significantly lower systolic BP at 6 months among hypertensive adults, real-world results from Europe show.
“We don’t know what they did to reduce their blood pressure,” Jay Shah, MD, Division of Cardiology, Mayo Clinic Arizona, Phoenix, told this news organization.
“The idea is that because they were exposed to their data on a continual basis, that may have prompted them to do something that led to an improvement in their blood pressure, whether it be exercise more, go to their doctor, or change their medication,” said Dr. Shah, who is also chief medical officer for Aktiia.
Dr. Shah presented the study at the Hypertension Scientific Sessions, San Diego.
Empowering data
The study used the Aktiia 24/7 BP monitor; Atkiia funded the trial. The monitor passively and continually monitors BP values from photoplethysmography signals collected via optical sensors at the wrist.
After initial individualized calibration using a cuff-based reference, BP measurements are displayed on a smartphone app, allowing users to consistently monitor their own BP for long periods of time.
Aktiia received CE mark in Europe in January 2021 and is currently under review by the U.S. Food and Drug Administration.
Dr. Shah and colleagues analyzed systolic BP (SBP) trends among 838 real-world Aktiia users in Europe (age 57 ± 11 years; 14% women) who consistently used the monitor for 6 months.
Altogether, they had data on 375 (± 287) app interactions, 3,646 (± 1,417) cuffless readings per user, and 9 (± 7) cuff readings per user.
Traditional cuff SBP averages were calculated monthly and compared with the SBP average of the first month. A t-test analysis was used to detect the difference in SBP between the first and successive months.
On the basis of the mean SBP calculated over 6 months, 136 participants were hypertensive (SBP > 140 mm Hg) and the rest had SBP less than 140 mm Hg.
Hypertensive users saw a statistically significant reduction in SBP of –3.2 mm Hg (95% CI, –0.70 to –5.59; P < .02), beginning at 3 months of continual cuffless BP monitoring, which was sustained through 6 months.
Among users with SBP less than 140 mm Hg, the mean SBP remained unchanged.
“The magnitude of improvement might look modest, but even a 5 mm Hg reduction in systolic BP correlates to a 10% decrease in cardiovascular risk,” Dr. Shah told this news organization.
He noted that “one of the major hurdles is that people may not be aware they have high blood pressure because they don’t feel it. And with a regular cuff, they’ll only see that number when they actually check their blood pressure, which is extremely rare, even for people who have hypertension.”
“Having the ability to show someone their continual blood pressure picture really empowers them to do something to make changes and to be aware, [as well as] to be a more active participant in their health,” Dr. Shah said.
He said that a good analogy is diabetes management, which has transitioned from single finger-stick glucose monitoring to continuous glucose monitoring that provides a complete 24/7 picture of glucose levels.
Transforming technology
Offering perspective on the study, Harlan Krumholz, MD, SM, with Yale New Haven Hospital and Yale School of Medicine, New Haven, Conn., said that having an accurate, affordable, unobtrusive cuffless continuous BP monitor would “transform” BP management.
“This could unlock an era of precision BP management with empowerment of patients to view and act on their numbers,” Dr. Krumholz said in an interview.
“We need data to be confident in the devices – and then research to best leverage the streams of information – and strategies to optimize its use in practice,” Dr. Krumholz added.
“Like any new innovation, we need to mitigate risks and monitor for unintended adverse consequences, but I am bullish on the future of cuffless continuous BP monitors,” Dr. Krumholz said.
Dr. Krumholz said that he “applauds Aktiia for doing studies that assess the effect of the information they are producing on BP over time. We need to know that new approaches not only generate valid information but that they can improve health.”
Ready for prime time?
In June, the European Society of Hypertension issued a statement noting that cuffless BP measurement is a fast-growing and promising field with considerable potential for improving hypertension awareness, management, and control, but because the accuracy of these new devices has not yet been validated, they are not yet suitable for clinical use.
Also providing perspective, Stephen Juraschek, MD, PhD, research director, Hypertension Center of Excellence at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston, said that “there is a lot of interest in cuffless BP monitors due to their ease of measurement, comfort, and ability to obtain BP measurements in multiple settings and environments, and this study showed that the monitoring improved BP over time.”
“It is believed that the increased awareness and feedback may promote healthier behaviors aimed at lowering BP. However, this result should not be conflated with the accuracy of these monitors,” Dr. Juraschek cautioned.
He also noted that there is still no formally approved validation protocol by the Association for the Advancement of Medical Instrumentation.
“While a number of cuffless devices are cleared by the FDA through its 510k mechanism (that is, demonstration of device equivalence), there is no formal stamp of approval or attestation that the measurements are accurate,” Dr. Juraschek said in an interview.
In his view, “more work is needed to understand the validity of these devices. For now, validated, cuff-based home devices are recommended for BP measurement at home, while further work is done to determine the accuracy of these cuffless technologies.”
The study was funded by Aktiia. Dr. Shah is an employee of the company. Dr. Krumholz has no relevant disclosures. Dr. Juraschek is a member of the Validate BP review committee and the AAMI sphygmomanometer committee.
A version of this article first appeared on Medscape.com.
FROM AHA HYPERTENSION 2022
Novel blood test for early-stage liver cancer shows promise
, increasing the likelihood of potentially curative therapy and improved patient prognosis.
HCC accounts for the majority of primary liver cancers and mainly occurs in patients with cirrhosis or chronic hepatitis B virus infection. The prognosis of HCC is poor, largely owing to advanced disease stage at diagnosis.
The current guidelines recommend surveillance with twice-yearly liver ultrasound, with or without serum alpha-fetoprotein, for patients at risk for HCC, although the diagnostic performance is suboptimal.
The new “liquid biopsy” uses HCC-associated extracellular vesicles (EVs) to establish an HCC EV ECG score for distinguishing patients with early-stage HCC from at-risk controls with cirrhosis from a 400-mcL plasma sample.
“We’re the first team looking at extracellular vesicles as a detection biomarker for early-stage liver cancer, and our study showed it had outstanding performance,” study investigator Ju Dong Yang, MD, with Cedars-Sinai Medical Center, Los Angeles, said in a news release.
The study was published online in Hepatology.
In a phase 2 biomarker (case-control) study, the investigators tested their blood test in a training cohort of 106 individuals (45 patients with treatment-naive early-stage HCC and 61 with cirrhosis) and an independent validation cohort with 72 participants (35 patients with treatment-naive early-stage HCC and 37 with cirrhosis).
The HCC EV ECG score had “excellent accuracy” for discriminating between HCC and cirrhosis, with an area under the receiver operating characteristic curve (AUROC) of 0.95 and 0.93 in the training and validation cohorts, respectively, they report.
The diagnostic performance “remained excellent” among the subpopulations of HCC etiology and those with tumors within the Milan criteria.
Adding the serum alpha-fetoprotein level to the HCC EV ECG score did not improve its performance.
The researchers say that further validation of the blood test in a larger phase 2 study and a subsequent phase 3 study are needed to confirm its utility in clinical settings.
“We are planning on doing larger-scale studies to further validate this test and bring it into routine clinical practice here – and globally,” Dr. Yang said.
“In addition to its excellent performance, this marker has the advantages of being user friendly, cost efficient, and having a fast turnaround time – within 6 hours from sample collection to result,” Dan Theodorescu, MD, PhD, director of Cedars-Sinai Cancer, who is not an author on the study, said in the news release.
“Once this marker has been validated in subsequent studies, it can be easily adopted by existing PCR [polymerase chain reaction] facilities,” Dr. Theodorescu added.
The study was supported by an American College of Gastroenterology Junior Faculty Development Award, a Department of Defense Peer Reviewed Cancer Research Program Career Development Award, and the National Institutes of Health. Dr. Yang provides a consulting service for Exact Sciences, Gilead Sciences, and Eisai. Dr. Theodorescu reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, increasing the likelihood of potentially curative therapy and improved patient prognosis.
HCC accounts for the majority of primary liver cancers and mainly occurs in patients with cirrhosis or chronic hepatitis B virus infection. The prognosis of HCC is poor, largely owing to advanced disease stage at diagnosis.
The current guidelines recommend surveillance with twice-yearly liver ultrasound, with or without serum alpha-fetoprotein, for patients at risk for HCC, although the diagnostic performance is suboptimal.
The new “liquid biopsy” uses HCC-associated extracellular vesicles (EVs) to establish an HCC EV ECG score for distinguishing patients with early-stage HCC from at-risk controls with cirrhosis from a 400-mcL plasma sample.
“We’re the first team looking at extracellular vesicles as a detection biomarker for early-stage liver cancer, and our study showed it had outstanding performance,” study investigator Ju Dong Yang, MD, with Cedars-Sinai Medical Center, Los Angeles, said in a news release.
The study was published online in Hepatology.
In a phase 2 biomarker (case-control) study, the investigators tested their blood test in a training cohort of 106 individuals (45 patients with treatment-naive early-stage HCC and 61 with cirrhosis) and an independent validation cohort with 72 participants (35 patients with treatment-naive early-stage HCC and 37 with cirrhosis).
The HCC EV ECG score had “excellent accuracy” for discriminating between HCC and cirrhosis, with an area under the receiver operating characteristic curve (AUROC) of 0.95 and 0.93 in the training and validation cohorts, respectively, they report.
The diagnostic performance “remained excellent” among the subpopulations of HCC etiology and those with tumors within the Milan criteria.
Adding the serum alpha-fetoprotein level to the HCC EV ECG score did not improve its performance.
The researchers say that further validation of the blood test in a larger phase 2 study and a subsequent phase 3 study are needed to confirm its utility in clinical settings.
“We are planning on doing larger-scale studies to further validate this test and bring it into routine clinical practice here – and globally,” Dr. Yang said.
“In addition to its excellent performance, this marker has the advantages of being user friendly, cost efficient, and having a fast turnaround time – within 6 hours from sample collection to result,” Dan Theodorescu, MD, PhD, director of Cedars-Sinai Cancer, who is not an author on the study, said in the news release.
“Once this marker has been validated in subsequent studies, it can be easily adopted by existing PCR [polymerase chain reaction] facilities,” Dr. Theodorescu added.
The study was supported by an American College of Gastroenterology Junior Faculty Development Award, a Department of Defense Peer Reviewed Cancer Research Program Career Development Award, and the National Institutes of Health. Dr. Yang provides a consulting service for Exact Sciences, Gilead Sciences, and Eisai. Dr. Theodorescu reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, increasing the likelihood of potentially curative therapy and improved patient prognosis.
HCC accounts for the majority of primary liver cancers and mainly occurs in patients with cirrhosis or chronic hepatitis B virus infection. The prognosis of HCC is poor, largely owing to advanced disease stage at diagnosis.
The current guidelines recommend surveillance with twice-yearly liver ultrasound, with or without serum alpha-fetoprotein, for patients at risk for HCC, although the diagnostic performance is suboptimal.
The new “liquid biopsy” uses HCC-associated extracellular vesicles (EVs) to establish an HCC EV ECG score for distinguishing patients with early-stage HCC from at-risk controls with cirrhosis from a 400-mcL plasma sample.
“We’re the first team looking at extracellular vesicles as a detection biomarker for early-stage liver cancer, and our study showed it had outstanding performance,” study investigator Ju Dong Yang, MD, with Cedars-Sinai Medical Center, Los Angeles, said in a news release.
The study was published online in Hepatology.
In a phase 2 biomarker (case-control) study, the investigators tested their blood test in a training cohort of 106 individuals (45 patients with treatment-naive early-stage HCC and 61 with cirrhosis) and an independent validation cohort with 72 participants (35 patients with treatment-naive early-stage HCC and 37 with cirrhosis).
The HCC EV ECG score had “excellent accuracy” for discriminating between HCC and cirrhosis, with an area under the receiver operating characteristic curve (AUROC) of 0.95 and 0.93 in the training and validation cohorts, respectively, they report.
The diagnostic performance “remained excellent” among the subpopulations of HCC etiology and those with tumors within the Milan criteria.
Adding the serum alpha-fetoprotein level to the HCC EV ECG score did not improve its performance.
The researchers say that further validation of the blood test in a larger phase 2 study and a subsequent phase 3 study are needed to confirm its utility in clinical settings.
“We are planning on doing larger-scale studies to further validate this test and bring it into routine clinical practice here – and globally,” Dr. Yang said.
“In addition to its excellent performance, this marker has the advantages of being user friendly, cost efficient, and having a fast turnaround time – within 6 hours from sample collection to result,” Dan Theodorescu, MD, PhD, director of Cedars-Sinai Cancer, who is not an author on the study, said in the news release.
“Once this marker has been validated in subsequent studies, it can be easily adopted by existing PCR [polymerase chain reaction] facilities,” Dr. Theodorescu added.
The study was supported by an American College of Gastroenterology Junior Faculty Development Award, a Department of Defense Peer Reviewed Cancer Research Program Career Development Award, and the National Institutes of Health. Dr. Yang provides a consulting service for Exact Sciences, Gilead Sciences, and Eisai. Dr. Theodorescu reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HEPATOLOGY
Game-changing results in fluid resuscitation for acute pancreatitis
Early, aggressive fluid resuscitation in acute pancreatitis led to a higher incidence of fluid overload without improving clinical outcomes in the landmark WATERFALL trial.
Early aggressive hydration is widely recommended for the management of acute pancreatitis, but evidence for this practice is limited.
“The WATERFALL trial demonstrates that aggressive fluid resuscitation in acute pancreatitis is not safe, it is not associated with improved outcomes, and it should be abandoned,” Enrique de-Madaria, MD, PhD, with Hospital General Universitario Dr. Balmis, Alicante, Spain, told this news organization.
The trial settles a “new and clear reference for fluid resuscitation in this frequent disease: lactated Ringer’s solution 1.5 mL/kg per hour (preceded by a 10 mL/kg bolus over 2 hours only in case of hypovolemia),” added Dr. de-Madaria, president of the Spanish Association of Gastroenterology.
“This moderate fluid resuscitation strategy is associated with a much lower frequency of fluid overload and a trend toward improved outcomes. For such reasons, it should be considered as a new standard of care in the early management of acute pancreatitis,” Dr. de-Madaria said.
The WATERFALL trial results were published in the New England Journal of Medicine.
The results are “stunning and, given the carefully crafted trial methods, irrefutable,” Timothy Gardner, MD, with the section of gastroenterology and hepatology, Dartmouth–Hitchcock Medical Center, Lebanon, N.H., wrote in a linked editorial.
Trial details
The trial was conducted at 18 centers across India, Italy, Mexico, and Spain. Patients who presented with acute pancreatitis were randomly allocated to aggressive or moderate resuscitation with lactated Ringer’s solution.
Aggressive fluid resuscitation consisted of a bolus of 20 mL/kg of body weight, followed by 3 mL/kg per hour. Moderate fluid resuscitation consisted of a bolus of 10 mL/kg in patients with hypovolemia or no bolus in patients with normovolemia, followed by 1.5 mL/kg per hour in all patients in this group.
Patients were assessed at 12, 24, 48, and 72 hours, and fluid resuscitation was adjusted according to clinical status.
A total of 249 patients were included in the interim analysis – 122 in the aggressive-resuscitation group and 127 in the moderate-resuscitation group.
The data and safety monitoring board terminated the trial at the first interim safety analysis as a result of the development of fluid overload in 20.5% of the patients in the aggressive-resuscitation group versus 6.3% of those in the moderate-resuscitation group (adjusted relative risk, 2.85; 95% confidence interval, 1.36-5.94; P = .004).
“An increased risk of fluid overload was detected in the overall population of patients and also in subgroups of patients without systemic inflammatory response syndrome at baseline, patients with SIRS at baseline (thus, with a higher risk of development of severe pancreatitis), and patients with hypovolemia,” the investigators reported.
This clear signal of harm was coupled with no significant difference in the incidence of moderately severe or severe pancreatitis (22.1% in the aggressive-resuscitation group and 17.3% in the moderate-resuscitation group; aRR, 1.30; 95% CI, 0.78-2.18; P = .32).
Patients in the aggressive-resuscitation group spent a median of 6 days in the hospital, compared with 5 days for patients in the moderate-resuscitation group.
“These findings do not support current management guidelines, which recommend early aggressive resuscitation for the treatment of acute pancreatitis,” the study team wrote.
‘Landmark’ trial
This is a “landmark” trial and “so clinically relevant because of its choice of real world-appropriate aggressive-resuscitation and moderate-resuscitation treatment groups, its use of pancreatitis severity as the main clinical outcome, and its reliance on the carefully defined variable of fluid overload as the main safety outcome,” Dr. Gardner wrote in his editorial.
“Unlike in most other randomized, controlled trials of fluid resuscitation in acute pancreatitis, patients with varying baseline pancreatitis severity were included, and changes in the rate of resuscitation were determined on the basis of a dynamic assessment of hemodynamic testing, imaging, and clinical factors,” he added.
Dr. Gardner said the WATERFALL trial results lead to several conclusions.
First, the need to focus on a steady rate of initial resuscitation – no more than 1.5 mL/kg of body weight per hour. Clinicians should administer a bolus of 10 mL/kg only if there are signs of initial hypovolemia.
Second, that careful clinical and hemodynamic monitoring are essential during the first 72 hours after admission to make sure that patients remain euvolemic and to avoid fluid overload.
Third, that diuresis in patients with fluid overload in the first 72 hours is most likely beneficial and certainly not detrimental to important clinical outcomes.
Dr. Gardner said the trial also highlights the need to focus research efforts on evaluating other pharmacologic therapies instead of crystalloid fluids.
“Performing randomized controlled trials in acute pancreatitis is notoriously difficult, and the limited human and financial resources that are available for appropriately powered trials in this field post WATERFALL are much better spent on comparative-effectiveness and placebo-controlled trials evaluating new therapeutic agents,” Dr. Gardner said.
“Now that we have gone over the WATERFALL, it is time to look downstream at new targets to treat this challenging disease,” he concluded.
Support for the trial was provided by Instituto de Salud Carlos III, the Spanish Association of Gastroenterology, and ISABIAL (Instituto de Investigación Sanitaria y Biomédica de Alicante).
A version of this article first appeared on Medscape.com.
Early, aggressive fluid resuscitation in acute pancreatitis led to a higher incidence of fluid overload without improving clinical outcomes in the landmark WATERFALL trial.
Early aggressive hydration is widely recommended for the management of acute pancreatitis, but evidence for this practice is limited.
“The WATERFALL trial demonstrates that aggressive fluid resuscitation in acute pancreatitis is not safe, it is not associated with improved outcomes, and it should be abandoned,” Enrique de-Madaria, MD, PhD, with Hospital General Universitario Dr. Balmis, Alicante, Spain, told this news organization.
The trial settles a “new and clear reference for fluid resuscitation in this frequent disease: lactated Ringer’s solution 1.5 mL/kg per hour (preceded by a 10 mL/kg bolus over 2 hours only in case of hypovolemia),” added Dr. de-Madaria, president of the Spanish Association of Gastroenterology.
“This moderate fluid resuscitation strategy is associated with a much lower frequency of fluid overload and a trend toward improved outcomes. For such reasons, it should be considered as a new standard of care in the early management of acute pancreatitis,” Dr. de-Madaria said.
The WATERFALL trial results were published in the New England Journal of Medicine.
The results are “stunning and, given the carefully crafted trial methods, irrefutable,” Timothy Gardner, MD, with the section of gastroenterology and hepatology, Dartmouth–Hitchcock Medical Center, Lebanon, N.H., wrote in a linked editorial.
Trial details
The trial was conducted at 18 centers across India, Italy, Mexico, and Spain. Patients who presented with acute pancreatitis were randomly allocated to aggressive or moderate resuscitation with lactated Ringer’s solution.
Aggressive fluid resuscitation consisted of a bolus of 20 mL/kg of body weight, followed by 3 mL/kg per hour. Moderate fluid resuscitation consisted of a bolus of 10 mL/kg in patients with hypovolemia or no bolus in patients with normovolemia, followed by 1.5 mL/kg per hour in all patients in this group.
Patients were assessed at 12, 24, 48, and 72 hours, and fluid resuscitation was adjusted according to clinical status.
A total of 249 patients were included in the interim analysis – 122 in the aggressive-resuscitation group and 127 in the moderate-resuscitation group.
The data and safety monitoring board terminated the trial at the first interim safety analysis as a result of the development of fluid overload in 20.5% of the patients in the aggressive-resuscitation group versus 6.3% of those in the moderate-resuscitation group (adjusted relative risk, 2.85; 95% confidence interval, 1.36-5.94; P = .004).
“An increased risk of fluid overload was detected in the overall population of patients and also in subgroups of patients without systemic inflammatory response syndrome at baseline, patients with SIRS at baseline (thus, with a higher risk of development of severe pancreatitis), and patients with hypovolemia,” the investigators reported.
This clear signal of harm was coupled with no significant difference in the incidence of moderately severe or severe pancreatitis (22.1% in the aggressive-resuscitation group and 17.3% in the moderate-resuscitation group; aRR, 1.30; 95% CI, 0.78-2.18; P = .32).
Patients in the aggressive-resuscitation group spent a median of 6 days in the hospital, compared with 5 days for patients in the moderate-resuscitation group.
“These findings do not support current management guidelines, which recommend early aggressive resuscitation for the treatment of acute pancreatitis,” the study team wrote.
‘Landmark’ trial
This is a “landmark” trial and “so clinically relevant because of its choice of real world-appropriate aggressive-resuscitation and moderate-resuscitation treatment groups, its use of pancreatitis severity as the main clinical outcome, and its reliance on the carefully defined variable of fluid overload as the main safety outcome,” Dr. Gardner wrote in his editorial.
“Unlike in most other randomized, controlled trials of fluid resuscitation in acute pancreatitis, patients with varying baseline pancreatitis severity were included, and changes in the rate of resuscitation were determined on the basis of a dynamic assessment of hemodynamic testing, imaging, and clinical factors,” he added.
Dr. Gardner said the WATERFALL trial results lead to several conclusions.
First, the need to focus on a steady rate of initial resuscitation – no more than 1.5 mL/kg of body weight per hour. Clinicians should administer a bolus of 10 mL/kg only if there are signs of initial hypovolemia.
Second, that careful clinical and hemodynamic monitoring are essential during the first 72 hours after admission to make sure that patients remain euvolemic and to avoid fluid overload.
Third, that diuresis in patients with fluid overload in the first 72 hours is most likely beneficial and certainly not detrimental to important clinical outcomes.
Dr. Gardner said the trial also highlights the need to focus research efforts on evaluating other pharmacologic therapies instead of crystalloid fluids.
“Performing randomized controlled trials in acute pancreatitis is notoriously difficult, and the limited human and financial resources that are available for appropriately powered trials in this field post WATERFALL are much better spent on comparative-effectiveness and placebo-controlled trials evaluating new therapeutic agents,” Dr. Gardner said.
“Now that we have gone over the WATERFALL, it is time to look downstream at new targets to treat this challenging disease,” he concluded.
Support for the trial was provided by Instituto de Salud Carlos III, the Spanish Association of Gastroenterology, and ISABIAL (Instituto de Investigación Sanitaria y Biomédica de Alicante).
A version of this article first appeared on Medscape.com.
Early, aggressive fluid resuscitation in acute pancreatitis led to a higher incidence of fluid overload without improving clinical outcomes in the landmark WATERFALL trial.
Early aggressive hydration is widely recommended for the management of acute pancreatitis, but evidence for this practice is limited.
“The WATERFALL trial demonstrates that aggressive fluid resuscitation in acute pancreatitis is not safe, it is not associated with improved outcomes, and it should be abandoned,” Enrique de-Madaria, MD, PhD, with Hospital General Universitario Dr. Balmis, Alicante, Spain, told this news organization.
The trial settles a “new and clear reference for fluid resuscitation in this frequent disease: lactated Ringer’s solution 1.5 mL/kg per hour (preceded by a 10 mL/kg bolus over 2 hours only in case of hypovolemia),” added Dr. de-Madaria, president of the Spanish Association of Gastroenterology.
“This moderate fluid resuscitation strategy is associated with a much lower frequency of fluid overload and a trend toward improved outcomes. For such reasons, it should be considered as a new standard of care in the early management of acute pancreatitis,” Dr. de-Madaria said.
The WATERFALL trial results were published in the New England Journal of Medicine.
The results are “stunning and, given the carefully crafted trial methods, irrefutable,” Timothy Gardner, MD, with the section of gastroenterology and hepatology, Dartmouth–Hitchcock Medical Center, Lebanon, N.H., wrote in a linked editorial.
Trial details
The trial was conducted at 18 centers across India, Italy, Mexico, and Spain. Patients who presented with acute pancreatitis were randomly allocated to aggressive or moderate resuscitation with lactated Ringer’s solution.
Aggressive fluid resuscitation consisted of a bolus of 20 mL/kg of body weight, followed by 3 mL/kg per hour. Moderate fluid resuscitation consisted of a bolus of 10 mL/kg in patients with hypovolemia or no bolus in patients with normovolemia, followed by 1.5 mL/kg per hour in all patients in this group.
Patients were assessed at 12, 24, 48, and 72 hours, and fluid resuscitation was adjusted according to clinical status.
A total of 249 patients were included in the interim analysis – 122 in the aggressive-resuscitation group and 127 in the moderate-resuscitation group.
The data and safety monitoring board terminated the trial at the first interim safety analysis as a result of the development of fluid overload in 20.5% of the patients in the aggressive-resuscitation group versus 6.3% of those in the moderate-resuscitation group (adjusted relative risk, 2.85; 95% confidence interval, 1.36-5.94; P = .004).
“An increased risk of fluid overload was detected in the overall population of patients and also in subgroups of patients without systemic inflammatory response syndrome at baseline, patients with SIRS at baseline (thus, with a higher risk of development of severe pancreatitis), and patients with hypovolemia,” the investigators reported.
This clear signal of harm was coupled with no significant difference in the incidence of moderately severe or severe pancreatitis (22.1% in the aggressive-resuscitation group and 17.3% in the moderate-resuscitation group; aRR, 1.30; 95% CI, 0.78-2.18; P = .32).
Patients in the aggressive-resuscitation group spent a median of 6 days in the hospital, compared with 5 days for patients in the moderate-resuscitation group.
“These findings do not support current management guidelines, which recommend early aggressive resuscitation for the treatment of acute pancreatitis,” the study team wrote.
‘Landmark’ trial
This is a “landmark” trial and “so clinically relevant because of its choice of real world-appropriate aggressive-resuscitation and moderate-resuscitation treatment groups, its use of pancreatitis severity as the main clinical outcome, and its reliance on the carefully defined variable of fluid overload as the main safety outcome,” Dr. Gardner wrote in his editorial.
“Unlike in most other randomized, controlled trials of fluid resuscitation in acute pancreatitis, patients with varying baseline pancreatitis severity were included, and changes in the rate of resuscitation were determined on the basis of a dynamic assessment of hemodynamic testing, imaging, and clinical factors,” he added.
Dr. Gardner said the WATERFALL trial results lead to several conclusions.
First, the need to focus on a steady rate of initial resuscitation – no more than 1.5 mL/kg of body weight per hour. Clinicians should administer a bolus of 10 mL/kg only if there are signs of initial hypovolemia.
Second, that careful clinical and hemodynamic monitoring are essential during the first 72 hours after admission to make sure that patients remain euvolemic and to avoid fluid overload.
Third, that diuresis in patients with fluid overload in the first 72 hours is most likely beneficial and certainly not detrimental to important clinical outcomes.
Dr. Gardner said the trial also highlights the need to focus research efforts on evaluating other pharmacologic therapies instead of crystalloid fluids.
“Performing randomized controlled trials in acute pancreatitis is notoriously difficult, and the limited human and financial resources that are available for appropriately powered trials in this field post WATERFALL are much better spent on comparative-effectiveness and placebo-controlled trials evaluating new therapeutic agents,” Dr. Gardner said.
“Now that we have gone over the WATERFALL, it is time to look downstream at new targets to treat this challenging disease,” he concluded.
Support for the trial was provided by Instituto de Salud Carlos III, the Spanish Association of Gastroenterology, and ISABIAL (Instituto de Investigación Sanitaria y Biomédica de Alicante).
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Mental health in America: ‘The kids are not alright’
A new report shines a light on the toll the pandemic and other stressors have taken on the mental health of U.S. children and adolescents over the last 6 years.
The report shows a dramatic increase in use of acute care services for depression, anxiety, and other mental health conditions, especially among teens and preteens.
The report – The Kids Are Not Alright: Pediatric Mental Health Care Utilization from 2016-2021 – is the work of researchers at the Clarify Health Institute, the research arm of Clarify Health.
The results are “deeply concerning” and should “spark a conversation” around the need to improve access, utilization, and quality of pediatric behavioral health services, Niall Brennan, chief analytics and privacy officer for the Clarify Health Institute, told this news organization.
‘Startling’ trends
Leveraging an observational, national sample of insurance claims from more than 20 million children aged 1-19 years annually, the researchers observed several disturbing trends in mental health care.
From 2016 to 2021, inpatient (IP) admissions rose 61% (from 30 to 48 visits annually per 1,000) and emergency department visits rose 20% (from 55 to 66 visits annually per 1,000).
Mental health IP admissions ranged from a low of 27% in the West North Central region to a high of 137% in the Middle Atlantic region.
There were substantial increases from 2016 to 2021 in mental health IP admissions among children of all age groups, but particularly among adolescents 12 to 15 years old, increasing 84% among girls and 83% among boys in this age group.
There was also a sharp increase in mental health ED visits among girls and boys aged 12-15 years, increasing 20% overall during the study period.
Mental health IP use grew faster from 2016 to 2021 among children with commercial insurance than among those with Medicaid (103% vs. 40%).
In contrast, mental health–specific ED visits declined 10% among children with commercial insurance and increased by 20% among those with Medicaid.
ED utilization rates in 2021 were nearly twice as high in the Medicaid population, compared with those for children with commercial insurance.
These are “startling” increases, Mr. Brennan said in an interview.
These trends “reinforce health care leaders’ responsibility to address children’s mental health, especially when considering that half of all mental health conditions onset during adolescence and carry into adulthood,” Jean Drouin, MD, Clarify Health’s chief executive office and cofounder, adds in a news release.
“With a growing consensus that mental, behavioral, and physical health intersect, this research report aims to spark a conversation about the overall wellbeing of America’s next generation,” Dr. Drouin says.
Concern for the future
Commenting on the new report, Anish Dube, MD, chair of the American Psychiatric Association’s Council on Children, Adolescents, and their Families, said the findings are “concerning, though unsurprising.”
“They confirm what those of us in clinical practice have experienced in the last several years. The need for mental health services continues to rise every year, while access to adequate help remains lacking,” Dr. Dube said.
“With the recent COVID-19 pandemic, concerns about the effects of climate change, global political uncertainty, and a rapidly changing employment landscape, young people in particular are vulnerable to worries about their future and feelings of helplessness and hopelessness,” he added.
Dr. Dube said there is no one right solution, and addressing this problem must consider individual and local factors.
However, some of the broader interventions needed to tackle the problem include increasing access to care by enforcing mental health parity and increasing the number of trained and qualified mental health professionals, such as child and adolescent psychiatrists, who can assess and treat these conditions in young people before they become major crises and lead to acute interventions like inpatient hospitalization.
“Public health interventions aimed at schools and families in raising awareness of mental health and well-being, and simple, cost-effective interventions to practice mental wellness will also help reduce the burden of mental illness in young people,” Dr. Dube added.
“The APA continues to fight for mental health parity enforcement and for meaningful access to mental health care for children, adolescents, and their families,” Dr. Dube said.
This research was conducted by the Clarify Health Institute. Mr. Brennan and Dr. Dube report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new report shines a light on the toll the pandemic and other stressors have taken on the mental health of U.S. children and adolescents over the last 6 years.
The report shows a dramatic increase in use of acute care services for depression, anxiety, and other mental health conditions, especially among teens and preteens.
The report – The Kids Are Not Alright: Pediatric Mental Health Care Utilization from 2016-2021 – is the work of researchers at the Clarify Health Institute, the research arm of Clarify Health.
The results are “deeply concerning” and should “spark a conversation” around the need to improve access, utilization, and quality of pediatric behavioral health services, Niall Brennan, chief analytics and privacy officer for the Clarify Health Institute, told this news organization.
‘Startling’ trends
Leveraging an observational, national sample of insurance claims from more than 20 million children aged 1-19 years annually, the researchers observed several disturbing trends in mental health care.
From 2016 to 2021, inpatient (IP) admissions rose 61% (from 30 to 48 visits annually per 1,000) and emergency department visits rose 20% (from 55 to 66 visits annually per 1,000).
Mental health IP admissions ranged from a low of 27% in the West North Central region to a high of 137% in the Middle Atlantic region.
There were substantial increases from 2016 to 2021 in mental health IP admissions among children of all age groups, but particularly among adolescents 12 to 15 years old, increasing 84% among girls and 83% among boys in this age group.
There was also a sharp increase in mental health ED visits among girls and boys aged 12-15 years, increasing 20% overall during the study period.
Mental health IP use grew faster from 2016 to 2021 among children with commercial insurance than among those with Medicaid (103% vs. 40%).
In contrast, mental health–specific ED visits declined 10% among children with commercial insurance and increased by 20% among those with Medicaid.
ED utilization rates in 2021 were nearly twice as high in the Medicaid population, compared with those for children with commercial insurance.
These are “startling” increases, Mr. Brennan said in an interview.
These trends “reinforce health care leaders’ responsibility to address children’s mental health, especially when considering that half of all mental health conditions onset during adolescence and carry into adulthood,” Jean Drouin, MD, Clarify Health’s chief executive office and cofounder, adds in a news release.
“With a growing consensus that mental, behavioral, and physical health intersect, this research report aims to spark a conversation about the overall wellbeing of America’s next generation,” Dr. Drouin says.
Concern for the future
Commenting on the new report, Anish Dube, MD, chair of the American Psychiatric Association’s Council on Children, Adolescents, and their Families, said the findings are “concerning, though unsurprising.”
“They confirm what those of us in clinical practice have experienced in the last several years. The need for mental health services continues to rise every year, while access to adequate help remains lacking,” Dr. Dube said.
“With the recent COVID-19 pandemic, concerns about the effects of climate change, global political uncertainty, and a rapidly changing employment landscape, young people in particular are vulnerable to worries about their future and feelings of helplessness and hopelessness,” he added.
Dr. Dube said there is no one right solution, and addressing this problem must consider individual and local factors.
However, some of the broader interventions needed to tackle the problem include increasing access to care by enforcing mental health parity and increasing the number of trained and qualified mental health professionals, such as child and adolescent psychiatrists, who can assess and treat these conditions in young people before they become major crises and lead to acute interventions like inpatient hospitalization.
“Public health interventions aimed at schools and families in raising awareness of mental health and well-being, and simple, cost-effective interventions to practice mental wellness will also help reduce the burden of mental illness in young people,” Dr. Dube added.
“The APA continues to fight for mental health parity enforcement and for meaningful access to mental health care for children, adolescents, and their families,” Dr. Dube said.
This research was conducted by the Clarify Health Institute. Mr. Brennan and Dr. Dube report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new report shines a light on the toll the pandemic and other stressors have taken on the mental health of U.S. children and adolescents over the last 6 years.
The report shows a dramatic increase in use of acute care services for depression, anxiety, and other mental health conditions, especially among teens and preteens.
The report – The Kids Are Not Alright: Pediatric Mental Health Care Utilization from 2016-2021 – is the work of researchers at the Clarify Health Institute, the research arm of Clarify Health.
The results are “deeply concerning” and should “spark a conversation” around the need to improve access, utilization, and quality of pediatric behavioral health services, Niall Brennan, chief analytics and privacy officer for the Clarify Health Institute, told this news organization.
‘Startling’ trends
Leveraging an observational, national sample of insurance claims from more than 20 million children aged 1-19 years annually, the researchers observed several disturbing trends in mental health care.
From 2016 to 2021, inpatient (IP) admissions rose 61% (from 30 to 48 visits annually per 1,000) and emergency department visits rose 20% (from 55 to 66 visits annually per 1,000).
Mental health IP admissions ranged from a low of 27% in the West North Central region to a high of 137% in the Middle Atlantic region.
There were substantial increases from 2016 to 2021 in mental health IP admissions among children of all age groups, but particularly among adolescents 12 to 15 years old, increasing 84% among girls and 83% among boys in this age group.
There was also a sharp increase in mental health ED visits among girls and boys aged 12-15 years, increasing 20% overall during the study period.
Mental health IP use grew faster from 2016 to 2021 among children with commercial insurance than among those with Medicaid (103% vs. 40%).
In contrast, mental health–specific ED visits declined 10% among children with commercial insurance and increased by 20% among those with Medicaid.
ED utilization rates in 2021 were nearly twice as high in the Medicaid population, compared with those for children with commercial insurance.
These are “startling” increases, Mr. Brennan said in an interview.
These trends “reinforce health care leaders’ responsibility to address children’s mental health, especially when considering that half of all mental health conditions onset during adolescence and carry into adulthood,” Jean Drouin, MD, Clarify Health’s chief executive office and cofounder, adds in a news release.
“With a growing consensus that mental, behavioral, and physical health intersect, this research report aims to spark a conversation about the overall wellbeing of America’s next generation,” Dr. Drouin says.
Concern for the future
Commenting on the new report, Anish Dube, MD, chair of the American Psychiatric Association’s Council on Children, Adolescents, and their Families, said the findings are “concerning, though unsurprising.”
“They confirm what those of us in clinical practice have experienced in the last several years. The need for mental health services continues to rise every year, while access to adequate help remains lacking,” Dr. Dube said.
“With the recent COVID-19 pandemic, concerns about the effects of climate change, global political uncertainty, and a rapidly changing employment landscape, young people in particular are vulnerable to worries about their future and feelings of helplessness and hopelessness,” he added.
Dr. Dube said there is no one right solution, and addressing this problem must consider individual and local factors.
However, some of the broader interventions needed to tackle the problem include increasing access to care by enforcing mental health parity and increasing the number of trained and qualified mental health professionals, such as child and adolescent psychiatrists, who can assess and treat these conditions in young people before they become major crises and lead to acute interventions like inpatient hospitalization.
“Public health interventions aimed at schools and families in raising awareness of mental health and well-being, and simple, cost-effective interventions to practice mental wellness will also help reduce the burden of mental illness in young people,” Dr. Dube added.
“The APA continues to fight for mental health parity enforcement and for meaningful access to mental health care for children, adolescents, and their families,” Dr. Dube said.
This research was conducted by the Clarify Health Institute. Mr. Brennan and Dr. Dube report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Should patients stand for office BP readings?
a new study suggests.
Combining three standing and three seated BP measurements in the same visit may lead to a “quicker diagnosis and save people a trip back to the office,” Wanpen Vongpatanasin, MD, professor of internal medicine and director of the hypertension section, cardiology division, UT Southwestern Medical Center, Dallas, said in an interview.
The study was presented at the Hypertension Scientific Sessions, sponsored by the American Heart Association.
Practice changing?
Clinical guidelines recommend office BP be taken in a seated position for most patients.
However, research has suggested that the sensitivity of seated office BP in diagnosing hypertension is about 50%, with high specificity around 90% during a single visit, Dr. Vongpatanasin explained.
At the follow-up visit, however, the second office BP yielded higher sensitivity to 80% but specificity fell to 55%. Nevertheless, the accuracy of standing BP measurements for diagnosing hypertension has not been investigated.
In a cross-sectional study, Dr. Vongpatanasin and colleagues determined the accuracy of both seated and standing BP for diagnosing hypertension in a single visit in 125 healthy adults who had not had a previous diagnosis of hypertension and were not taking any BP medications. The cohort had a mean age of 49 years, 62% were women, and 24% were Black.
During each office visit, seated BP was measured three times, then standing BP was measured three times using an automated and validated device.
Average seated BP was 123/76 mm Hg and average standing BP was 126/80 mm Hg.
Of the 125 participants, 42 (34%) had hypertension, defined as 24-hour ambulatory systolic/diastolic BP (SBP/DBP) of ≥ 125/75 mm Hg.
The sensitivity and specificity of seated SBP for hypertension was 43% and 92%, respectively.
“Interestingly, with standing SBP, sensitivity was improved to 74% and specificity dropped to 65% – which is okay; you will have to confirm a positive test anyway and when screening for a common disease you’d rather have a high sensitivity rather than low sensitivity to pick it up in this case,” Dr. Vongpatanasin said.
The area under receiver operating characteristic curve (AUROC) of standing SBP was significantly higher than seated SBP (Bayes factor [BF] = 11.8) when hypertension was defined as 24-hour SBP ≥ 125 mm Hg.
Similarly, when hypertension was defined as 24-hour DBP ≥ 75 mm Hg or daytime DBP ≥ 80 mm Hg, the AUROC of standing DBP was higher than seated DBP (all BF > 3).
The addition of standing to seated BP improved detection of hypertension compared with seated BP alone based on 24-hour SBP/DBP ≥ 125/75 mm Hg or daytime SBP/DBP ≥ 130/80 mm Hg (all BF > 3).
“In our hypertension clinic, we always measure both seated and standing BP in all of our patients,” John Giacona, PA-C, a PhD candidate at UT Southwestern Medical Center and coauthor of the study, told this news organization,
Multiple readings most important
Reached for comment, Johanna Contreras, MD, a cardiologist at Mount Sinai Hospital in New York, noted that diagnosing hypertension is “difficult” and she agrees that multiple readings are important.
“I usually take at least two readings in two different visits before I tell the patient they have high blood pressure,” Dr. Contreras said in an interview.
Dr. Contreras said she takes blood pressure both seated and standing.
“I’m not sure standing versus seated makes a big difference. However, when the patient first comes into the office, it is really important to let them rest and calm down before taking the blood pressure,” she said.
The study had no commercial funding. The authors and Dr. Contreras have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
a new study suggests.
Combining three standing and three seated BP measurements in the same visit may lead to a “quicker diagnosis and save people a trip back to the office,” Wanpen Vongpatanasin, MD, professor of internal medicine and director of the hypertension section, cardiology division, UT Southwestern Medical Center, Dallas, said in an interview.
The study was presented at the Hypertension Scientific Sessions, sponsored by the American Heart Association.
Practice changing?
Clinical guidelines recommend office BP be taken in a seated position for most patients.
However, research has suggested that the sensitivity of seated office BP in diagnosing hypertension is about 50%, with high specificity around 90% during a single visit, Dr. Vongpatanasin explained.
At the follow-up visit, however, the second office BP yielded higher sensitivity to 80% but specificity fell to 55%. Nevertheless, the accuracy of standing BP measurements for diagnosing hypertension has not been investigated.
In a cross-sectional study, Dr. Vongpatanasin and colleagues determined the accuracy of both seated and standing BP for diagnosing hypertension in a single visit in 125 healthy adults who had not had a previous diagnosis of hypertension and were not taking any BP medications. The cohort had a mean age of 49 years, 62% were women, and 24% were Black.
During each office visit, seated BP was measured three times, then standing BP was measured three times using an automated and validated device.
Average seated BP was 123/76 mm Hg and average standing BP was 126/80 mm Hg.
Of the 125 participants, 42 (34%) had hypertension, defined as 24-hour ambulatory systolic/diastolic BP (SBP/DBP) of ≥ 125/75 mm Hg.
The sensitivity and specificity of seated SBP for hypertension was 43% and 92%, respectively.
“Interestingly, with standing SBP, sensitivity was improved to 74% and specificity dropped to 65% – which is okay; you will have to confirm a positive test anyway and when screening for a common disease you’d rather have a high sensitivity rather than low sensitivity to pick it up in this case,” Dr. Vongpatanasin said.
The area under receiver operating characteristic curve (AUROC) of standing SBP was significantly higher than seated SBP (Bayes factor [BF] = 11.8) when hypertension was defined as 24-hour SBP ≥ 125 mm Hg.
Similarly, when hypertension was defined as 24-hour DBP ≥ 75 mm Hg or daytime DBP ≥ 80 mm Hg, the AUROC of standing DBP was higher than seated DBP (all BF > 3).
The addition of standing to seated BP improved detection of hypertension compared with seated BP alone based on 24-hour SBP/DBP ≥ 125/75 mm Hg or daytime SBP/DBP ≥ 130/80 mm Hg (all BF > 3).
“In our hypertension clinic, we always measure both seated and standing BP in all of our patients,” John Giacona, PA-C, a PhD candidate at UT Southwestern Medical Center and coauthor of the study, told this news organization,
Multiple readings most important
Reached for comment, Johanna Contreras, MD, a cardiologist at Mount Sinai Hospital in New York, noted that diagnosing hypertension is “difficult” and she agrees that multiple readings are important.
“I usually take at least two readings in two different visits before I tell the patient they have high blood pressure,” Dr. Contreras said in an interview.
Dr. Contreras said she takes blood pressure both seated and standing.
“I’m not sure standing versus seated makes a big difference. However, when the patient first comes into the office, it is really important to let them rest and calm down before taking the blood pressure,” she said.
The study had no commercial funding. The authors and Dr. Contreras have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
a new study suggests.
Combining three standing and three seated BP measurements in the same visit may lead to a “quicker diagnosis and save people a trip back to the office,” Wanpen Vongpatanasin, MD, professor of internal medicine and director of the hypertension section, cardiology division, UT Southwestern Medical Center, Dallas, said in an interview.
The study was presented at the Hypertension Scientific Sessions, sponsored by the American Heart Association.
Practice changing?
Clinical guidelines recommend office BP be taken in a seated position for most patients.
However, research has suggested that the sensitivity of seated office BP in diagnosing hypertension is about 50%, with high specificity around 90% during a single visit, Dr. Vongpatanasin explained.
At the follow-up visit, however, the second office BP yielded higher sensitivity to 80% but specificity fell to 55%. Nevertheless, the accuracy of standing BP measurements for diagnosing hypertension has not been investigated.
In a cross-sectional study, Dr. Vongpatanasin and colleagues determined the accuracy of both seated and standing BP for diagnosing hypertension in a single visit in 125 healthy adults who had not had a previous diagnosis of hypertension and were not taking any BP medications. The cohort had a mean age of 49 years, 62% were women, and 24% were Black.
During each office visit, seated BP was measured three times, then standing BP was measured three times using an automated and validated device.
Average seated BP was 123/76 mm Hg and average standing BP was 126/80 mm Hg.
Of the 125 participants, 42 (34%) had hypertension, defined as 24-hour ambulatory systolic/diastolic BP (SBP/DBP) of ≥ 125/75 mm Hg.
The sensitivity and specificity of seated SBP for hypertension was 43% and 92%, respectively.
“Interestingly, with standing SBP, sensitivity was improved to 74% and specificity dropped to 65% – which is okay; you will have to confirm a positive test anyway and when screening for a common disease you’d rather have a high sensitivity rather than low sensitivity to pick it up in this case,” Dr. Vongpatanasin said.
The area under receiver operating characteristic curve (AUROC) of standing SBP was significantly higher than seated SBP (Bayes factor [BF] = 11.8) when hypertension was defined as 24-hour SBP ≥ 125 mm Hg.
Similarly, when hypertension was defined as 24-hour DBP ≥ 75 mm Hg or daytime DBP ≥ 80 mm Hg, the AUROC of standing DBP was higher than seated DBP (all BF > 3).
The addition of standing to seated BP improved detection of hypertension compared with seated BP alone based on 24-hour SBP/DBP ≥ 125/75 mm Hg or daytime SBP/DBP ≥ 130/80 mm Hg (all BF > 3).
“In our hypertension clinic, we always measure both seated and standing BP in all of our patients,” John Giacona, PA-C, a PhD candidate at UT Southwestern Medical Center and coauthor of the study, told this news organization,
Multiple readings most important
Reached for comment, Johanna Contreras, MD, a cardiologist at Mount Sinai Hospital in New York, noted that diagnosing hypertension is “difficult” and she agrees that multiple readings are important.
“I usually take at least two readings in two different visits before I tell the patient they have high blood pressure,” Dr. Contreras said in an interview.
Dr. Contreras said she takes blood pressure both seated and standing.
“I’m not sure standing versus seated makes a big difference. However, when the patient first comes into the office, it is really important to let them rest and calm down before taking the blood pressure,” she said.
The study had no commercial funding. The authors and Dr. Contreras have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HYPERTENSION 2022
TBI is an unrecognized risk factor for cardiovascular disease
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
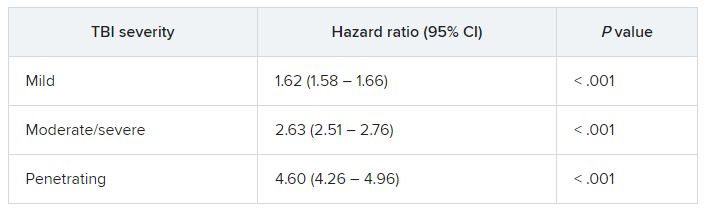
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(CVD). More severe TBI is associated with higher risk of CVD, new research shows.
Given the relatively young age of post-9/11–era veterans with TBI, there may be an increased burden of heart disease in the future as these veterans age and develop traditional risk factors for CVD, the investigators, led by Ian J. Stewart, MD, with Uniformed Services University, Bethesda, Md., wrote.
The study was published online in JAMA Neurology.
Novel data
Since Sept. 11, 2001, 4.5 million people have served in the U.S. military, with their time in service defined by the long-running wars in Iraq and Afghanistan. Estimates suggest that up to 20% of post-9/11 veterans sustained a TBI.
While some evidence suggests that TBI increases the risk of CVD, prior reports have focused mainly on cerebrovascular outcomes. Until now, the potential association of TBI with CVD has not been comprehensively examined in post-9/11–era veterans.
The retrospective cohort study included 1,559,928 predominantly male post-9/11 veterans, including 301,169 (19.3%) with a history of TBI and 1,258,759 (81%) with no TBI history.
In fully adjusted models, compared with veterans with no TBI history, a history of mild, moderate/severe, or penetrating TBI was associated with increased risk of developing the composite CVD endpoint (coronary artery disease, stroke, peripheral artery disease, and CVD death).
TBIs of all severities were associated with the individual components of the composite outcome, except penetrating TBI and CVD death.
“The association of TBI with subsequent CVD was not attenuated in multivariable models, suggesting that TBI may be accounting for risk that is independent from the other variables,” Dr. Stewart and colleagues wrote.
They noted that the risk was highest shortly after injury, but TBI remained significantly associated with CVD for years after the initial insult.
Why TBI may raise the risk of subsequent CVD remains unclear.
It’s possible that patients with TBI develop more traditional risk factors for CVD through time than do patients without TBI. A study in mice found that TBI led to increased rates of atherosclerosis, the researchers said.
An additional mechanism may be disruption of autonomic regulation, which has been known to occur after TBI.
Another potential pathway is through mental health diagnoses, such as posttraumatic stress disorder; a large body of work has identified associations between PTSD and CVD, including among post-9/11 veterans.
Further work is needed to determine how this risk can be modified to improve outcomes for post-9/11–era veterans, the researchers write.
Unrecognized CVD risk factor?
Reached for comment, Shaheen E. Lakhan, MD, PhD, a neurologist and researcher from Boston who wasn’t involved in the study, said the effects of TBI on heart health are “very underreported, and most clinicians would not make the link.”
“When the brain suffers a traumatic injury, it activates a cascade of neuro-inflammation that goes haywire in an attempt to protect further brain damage. Oftentimes, these inflammatory by-products leak into the body, especially in trauma, when the barriers are broken between brain and body, and can cause systemic body inflammation, which is well associated with heart disease,” Dr. Lakhan said.
In addition, Dr. Lakhan said, “TBI itself localized to just the brain can negatively affect good health habits, leading to worsening heart health, too.”
“Research like this brings light where not much exists and underscores the importance of protecting our brains from physical trauma,” he said.
The study was supported by the assistant secretary of defense for health affairs, endorsed by the Department of Defense through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium, and by the U.S. Department of Veterans Affairs. Dr. Stewart and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.