User login
Protocol Pilot
Evidence from randomized controlled trials and historical series convincingly demonstrates that tight glycemic control in the critical care setting reduces mortality, length of hospital stay, and other morbidities.1-6 Several protocols targeting a range of glucoses have been published.7-10 We modified a protocol used at the University of Washington (Seattle) that targeted glucoses of 80-180 mg/dl to aim for a tighter glycemic goal range of 80-110 mg/dl and effectively lowered blood glucoses in our intensive care unit (ICU) with a low rate of hypoglycemia.9 We share here our protocol and results over the past year.
Methods
Column protocols have the advantage of accommodating rates of insulin infusion adjustment to the individual patient’s degree of insulin resistance. If glucoses are not falling appropriately using one column, a protocol is followed to move to a more aggressive column. If glucoses fall precipitously, a similar process guides the nurse to a less aggressive column. The column format avoids the need for nurses to do calculations, which reduces the possibility of error.
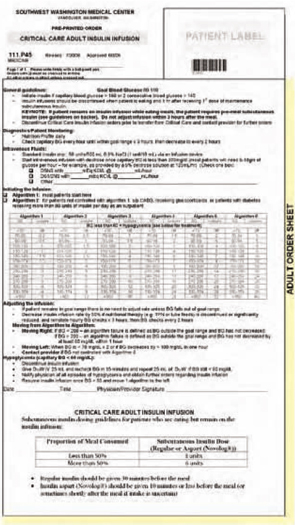
In August 2005, in our ICU, we piloted a four-column protocol used at the University of Washington. This protocol was designed with an initial target glucose range of 80-180 mg/dl, and during our pilot it did not work well because we were targeting a glucose range of 80-110 mg/dl. Our ICU nursing staff at Southwest Washington Medical Center (SWMC), Vancouver, preferred to revise the column format rather than switch to a different type of protocol such as the Portland Protocol. We therefore created a new six-column protocol targeting the 80-110 mg/dl glucose range. (See Figure 1, above.)
In creating this protocol, we reviewed infusion rates in an unpublished Oregon Health and Sciences University (OHSU), Portland, six-column protocol and the Georgia Hospital Association, Marietta, 10-column protocol.11,12 Our current version includes new glucose ranges of 70-89 mg/dl, 90-99 mg/dl, and 100-109 mg/dl to allow for more rate adjustments within the overall target range, while our previous version had only one glucose category of 70-109 mg/dl within the target range.
Nursing feedback also led us to modify criteria for moving to the right (more aggressive) column as follows: If blood glucose is lower than 200, algorithm failure is defined as glucose outside of goal range and not decreased since previous reading; if blood glucose is greater than or equal to 200, algorithm failure is defined as glucose outside of goal range and has not decreased by at least 60 mg/dl within one hour. The longest interval we allow between glucometer checks for stable patients is two hours. Automatic triggers for implementing the protocol include two consecutive glucoses over 140 mg/dl or a single glucose over 180 mg/dl.
Our revised protocol succeeded when we intensified nursing education, solicited frequent nursing feedback, and organized the procedure so that ICU nurse managers drove the process with a responsive physician/pharmacist team.
Results
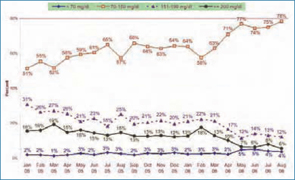
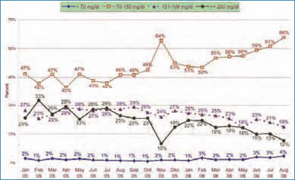
In March 2006 we instituted the revised six-column insulin infusion protocol in our ICU. The percent of glucometer readings in the ICU between 70-150 mg/dl increased from 58% in February 2006 to 78% in August of 2006. (See Figure 2, above.) In our cardiac care unit (CCU), where an older, non-column insulin infusion protocol continued to be used, glucoses went from 50% in the 70-150 mg/dl range in February 2006 to 61% in that range in July 2006. When we began the six-column ICU insulin infusion protocol in the CCU in August 2006, 66% of glucoses were in the 70-150 range. (See Figure 3, p. 43.)
The percentage of glucoses below 70 mg/dl increased from 2%-3% using the four-column protocol to 4%-5% using the six-column protocol, as the percentage of glucoses between 70-150 mg/dl rose above 70%.
The main complaint from nurses relates to the need for frequent (hourly to twice hourly) glucose monitoring, which was also a complaint with earlier protocols in our institution.
Discussion
These results compare favorably with those achieved by acknowledged leaders in critical care glycemic control in the United States.13 We have achieved them with the use of a safe column protocol that our critical care nurses are now comfortable using. The hypoglycemia rates with our protocol have been lower than those seen in some other published protocols. The Berghe protocol, for example, reported 5% of patients experiencing glucoses lower than or equal to 40 mg/dl, while our protocol resulted in 4%-5% of glucose values lower than 70 mg/dl.
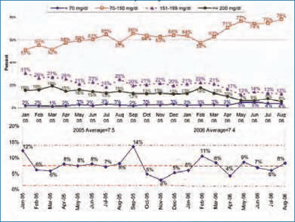
Mortality rates in our ICU have fallen from 14% in September 2005 to 11% in February 2006 to 8% in August 2006. Although this decline in mortality has occurred over the range of time in which we have improved glycemic control in our ICU, multiple other mortality reduction initiatives, any or all of which could account for the decline, occurred simultaneously in our hospital; in addition, mortality rates were falling before the introduction of the new insulin infusion protocol.
Head-to-head comparisons of existing protocols, using agreed upon glucometrics such as time-to-goal range and degree of glycemic variability, are needed.14 Testing new protocols, including proactive insulin infusion adjustments at the time of administration of known caloric loads—such as antibiotics delivered as a bolus in D5W solution—or at the time of initiation of high dose steroids or epinephrine drips, may be a means to keep a higher percentage of blood sugars in range. Ultimately, continuous blood sensing devices with closed loop insulin infusion responses are desired.
For now, our protocol offers a user-friendly means of getting a high percentage of critical care patients into a reasonable glycemic range with a low risk of hypoglycemia. Others are free to use and/or modify it. TH
The authors work at Southwest Washington Medical Center, Vancouver, Wash.
References
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Malmberg K, Norhammar A, Wedel H, et al. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626-2632.
- Furnary AP, Wu Y, Bookin SO. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland diabetic project. Endocr Pract. 2006 Mar-Apr;12 Suppl 3:22-26.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc. 2004 Aug;79(8):992-1000.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004 Oct 11;164(18):2005-2011.
- Goldberg PA. Memoirs of a root canal salesman: the successful implementation of a hospital-wide intravenous insulin infusion protocol. Endocr Pract. 2006;12 Suppl 3:79-85.
- Markovitz LJ, Weichmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract. 2002 Jan-Feb;8(1):10-18.
- Ku SY, Sayre CA, Hirsch IB, et al. New insulin infusion protocol improves blood glucose control in hospitalized patients without increasing hypoglycemia. Jt Comm J Qual Patient Saf. 2005 Mar;31(3):141-147.
- Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and continuous intravenous insulin infusions on outcomes of cardiac surgical procedures: the Portland Diabetic Project. Endocr Pract. 2004 Mar-Apr;10 Suppl 2:21-33.
- In a written communication from Andy Ahmann, MD, OHSU, in 2006.
- Georgia Hospital Association Diabetes Protocols. Chart 6b. Available at: www.adaendo.com/GHA/index.html. Accessed October 29, 2006.
- In a written communication from Terry Clemmer, MD, director, Critical Care Medicine, LDS Hospital, Salt Lake City, Utah, in October 2006.
- Braithwaite SS, Godara H, Song HJ, et al. No patient left behind: evaluation and design of intravenous insulin infusion algorithms. Endocr Pract. 2006 Jul-Aug;12 Suppl 3:72-78.
Evidence from randomized controlled trials and historical series convincingly demonstrates that tight glycemic control in the critical care setting reduces mortality, length of hospital stay, and other morbidities.1-6 Several protocols targeting a range of glucoses have been published.7-10 We modified a protocol used at the University of Washington (Seattle) that targeted glucoses of 80-180 mg/dl to aim for a tighter glycemic goal range of 80-110 mg/dl and effectively lowered blood glucoses in our intensive care unit (ICU) with a low rate of hypoglycemia.9 We share here our protocol and results over the past year.
Methods
Column protocols have the advantage of accommodating rates of insulin infusion adjustment to the individual patient’s degree of insulin resistance. If glucoses are not falling appropriately using one column, a protocol is followed to move to a more aggressive column. If glucoses fall precipitously, a similar process guides the nurse to a less aggressive column. The column format avoids the need for nurses to do calculations, which reduces the possibility of error.
In August 2005, in our ICU, we piloted a four-column protocol used at the University of Washington. This protocol was designed with an initial target glucose range of 80-180 mg/dl, and during our pilot it did not work well because we were targeting a glucose range of 80-110 mg/dl. Our ICU nursing staff at Southwest Washington Medical Center (SWMC), Vancouver, preferred to revise the column format rather than switch to a different type of protocol such as the Portland Protocol. We therefore created a new six-column protocol targeting the 80-110 mg/dl glucose range. (See Figure 1, above.)
In creating this protocol, we reviewed infusion rates in an unpublished Oregon Health and Sciences University (OHSU), Portland, six-column protocol and the Georgia Hospital Association, Marietta, 10-column protocol.11,12 Our current version includes new glucose ranges of 70-89 mg/dl, 90-99 mg/dl, and 100-109 mg/dl to allow for more rate adjustments within the overall target range, while our previous version had only one glucose category of 70-109 mg/dl within the target range.
Nursing feedback also led us to modify criteria for moving to the right (more aggressive) column as follows: If blood glucose is lower than 200, algorithm failure is defined as glucose outside of goal range and not decreased since previous reading; if blood glucose is greater than or equal to 200, algorithm failure is defined as glucose outside of goal range and has not decreased by at least 60 mg/dl within one hour. The longest interval we allow between glucometer checks for stable patients is two hours. Automatic triggers for implementing the protocol include two consecutive glucoses over 140 mg/dl or a single glucose over 180 mg/dl.
Our revised protocol succeeded when we intensified nursing education, solicited frequent nursing feedback, and organized the procedure so that ICU nurse managers drove the process with a responsive physician/pharmacist team.
Results
In March 2006 we instituted the revised six-column insulin infusion protocol in our ICU. The percent of glucometer readings in the ICU between 70-150 mg/dl increased from 58% in February 2006 to 78% in August of 2006. (See Figure 2, above.) In our cardiac care unit (CCU), where an older, non-column insulin infusion protocol continued to be used, glucoses went from 50% in the 70-150 mg/dl range in February 2006 to 61% in that range in July 2006. When we began the six-column ICU insulin infusion protocol in the CCU in August 2006, 66% of glucoses were in the 70-150 range. (See Figure 3, p. 43.)
The percentage of glucoses below 70 mg/dl increased from 2%-3% using the four-column protocol to 4%-5% using the six-column protocol, as the percentage of glucoses between 70-150 mg/dl rose above 70%.
The main complaint from nurses relates to the need for frequent (hourly to twice hourly) glucose monitoring, which was also a complaint with earlier protocols in our institution.
Discussion
These results compare favorably with those achieved by acknowledged leaders in critical care glycemic control in the United States.13 We have achieved them with the use of a safe column protocol that our critical care nurses are now comfortable using. The hypoglycemia rates with our protocol have been lower than those seen in some other published protocols. The Berghe protocol, for example, reported 5% of patients experiencing glucoses lower than or equal to 40 mg/dl, while our protocol resulted in 4%-5% of glucose values lower than 70 mg/dl.
Mortality rates in our ICU have fallen from 14% in September 2005 to 11% in February 2006 to 8% in August 2006. Although this decline in mortality has occurred over the range of time in which we have improved glycemic control in our ICU, multiple other mortality reduction initiatives, any or all of which could account for the decline, occurred simultaneously in our hospital; in addition, mortality rates were falling before the introduction of the new insulin infusion protocol.
Head-to-head comparisons of existing protocols, using agreed upon glucometrics such as time-to-goal range and degree of glycemic variability, are needed.14 Testing new protocols, including proactive insulin infusion adjustments at the time of administration of known caloric loads—such as antibiotics delivered as a bolus in D5W solution—or at the time of initiation of high dose steroids or epinephrine drips, may be a means to keep a higher percentage of blood sugars in range. Ultimately, continuous blood sensing devices with closed loop insulin infusion responses are desired.
For now, our protocol offers a user-friendly means of getting a high percentage of critical care patients into a reasonable glycemic range with a low risk of hypoglycemia. Others are free to use and/or modify it. TH
The authors work at Southwest Washington Medical Center, Vancouver, Wash.
References
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Malmberg K, Norhammar A, Wedel H, et al. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626-2632.
- Furnary AP, Wu Y, Bookin SO. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland diabetic project. Endocr Pract. 2006 Mar-Apr;12 Suppl 3:22-26.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc. 2004 Aug;79(8):992-1000.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004 Oct 11;164(18):2005-2011.
- Goldberg PA. Memoirs of a root canal salesman: the successful implementation of a hospital-wide intravenous insulin infusion protocol. Endocr Pract. 2006;12 Suppl 3:79-85.
- Markovitz LJ, Weichmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract. 2002 Jan-Feb;8(1):10-18.
- Ku SY, Sayre CA, Hirsch IB, et al. New insulin infusion protocol improves blood glucose control in hospitalized patients without increasing hypoglycemia. Jt Comm J Qual Patient Saf. 2005 Mar;31(3):141-147.
- Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and continuous intravenous insulin infusions on outcomes of cardiac surgical procedures: the Portland Diabetic Project. Endocr Pract. 2004 Mar-Apr;10 Suppl 2:21-33.
- In a written communication from Andy Ahmann, MD, OHSU, in 2006.
- Georgia Hospital Association Diabetes Protocols. Chart 6b. Available at: www.adaendo.com/GHA/index.html. Accessed October 29, 2006.
- In a written communication from Terry Clemmer, MD, director, Critical Care Medicine, LDS Hospital, Salt Lake City, Utah, in October 2006.
- Braithwaite SS, Godara H, Song HJ, et al. No patient left behind: evaluation and design of intravenous insulin infusion algorithms. Endocr Pract. 2006 Jul-Aug;12 Suppl 3:72-78.
Evidence from randomized controlled trials and historical series convincingly demonstrates that tight glycemic control in the critical care setting reduces mortality, length of hospital stay, and other morbidities.1-6 Several protocols targeting a range of glucoses have been published.7-10 We modified a protocol used at the University of Washington (Seattle) that targeted glucoses of 80-180 mg/dl to aim for a tighter glycemic goal range of 80-110 mg/dl and effectively lowered blood glucoses in our intensive care unit (ICU) with a low rate of hypoglycemia.9 We share here our protocol and results over the past year.
Methods
Column protocols have the advantage of accommodating rates of insulin infusion adjustment to the individual patient’s degree of insulin resistance. If glucoses are not falling appropriately using one column, a protocol is followed to move to a more aggressive column. If glucoses fall precipitously, a similar process guides the nurse to a less aggressive column. The column format avoids the need for nurses to do calculations, which reduces the possibility of error.
In August 2005, in our ICU, we piloted a four-column protocol used at the University of Washington. This protocol was designed with an initial target glucose range of 80-180 mg/dl, and during our pilot it did not work well because we were targeting a glucose range of 80-110 mg/dl. Our ICU nursing staff at Southwest Washington Medical Center (SWMC), Vancouver, preferred to revise the column format rather than switch to a different type of protocol such as the Portland Protocol. We therefore created a new six-column protocol targeting the 80-110 mg/dl glucose range. (See Figure 1, above.)
In creating this protocol, we reviewed infusion rates in an unpublished Oregon Health and Sciences University (OHSU), Portland, six-column protocol and the Georgia Hospital Association, Marietta, 10-column protocol.11,12 Our current version includes new glucose ranges of 70-89 mg/dl, 90-99 mg/dl, and 100-109 mg/dl to allow for more rate adjustments within the overall target range, while our previous version had only one glucose category of 70-109 mg/dl within the target range.
Nursing feedback also led us to modify criteria for moving to the right (more aggressive) column as follows: If blood glucose is lower than 200, algorithm failure is defined as glucose outside of goal range and not decreased since previous reading; if blood glucose is greater than or equal to 200, algorithm failure is defined as glucose outside of goal range and has not decreased by at least 60 mg/dl within one hour. The longest interval we allow between glucometer checks for stable patients is two hours. Automatic triggers for implementing the protocol include two consecutive glucoses over 140 mg/dl or a single glucose over 180 mg/dl.
Our revised protocol succeeded when we intensified nursing education, solicited frequent nursing feedback, and organized the procedure so that ICU nurse managers drove the process with a responsive physician/pharmacist team.
Results
In March 2006 we instituted the revised six-column insulin infusion protocol in our ICU. The percent of glucometer readings in the ICU between 70-150 mg/dl increased from 58% in February 2006 to 78% in August of 2006. (See Figure 2, above.) In our cardiac care unit (CCU), where an older, non-column insulin infusion protocol continued to be used, glucoses went from 50% in the 70-150 mg/dl range in February 2006 to 61% in that range in July 2006. When we began the six-column ICU insulin infusion protocol in the CCU in August 2006, 66% of glucoses were in the 70-150 range. (See Figure 3, p. 43.)
The percentage of glucoses below 70 mg/dl increased from 2%-3% using the four-column protocol to 4%-5% using the six-column protocol, as the percentage of glucoses between 70-150 mg/dl rose above 70%.
The main complaint from nurses relates to the need for frequent (hourly to twice hourly) glucose monitoring, which was also a complaint with earlier protocols in our institution.
Discussion
These results compare favorably with those achieved by acknowledged leaders in critical care glycemic control in the United States.13 We have achieved them with the use of a safe column protocol that our critical care nurses are now comfortable using. The hypoglycemia rates with our protocol have been lower than those seen in some other published protocols. The Berghe protocol, for example, reported 5% of patients experiencing glucoses lower than or equal to 40 mg/dl, while our protocol resulted in 4%-5% of glucose values lower than 70 mg/dl.
Mortality rates in our ICU have fallen from 14% in September 2005 to 11% in February 2006 to 8% in August 2006. Although this decline in mortality has occurred over the range of time in which we have improved glycemic control in our ICU, multiple other mortality reduction initiatives, any or all of which could account for the decline, occurred simultaneously in our hospital; in addition, mortality rates were falling before the introduction of the new insulin infusion protocol.
Head-to-head comparisons of existing protocols, using agreed upon glucometrics such as time-to-goal range and degree of glycemic variability, are needed.14 Testing new protocols, including proactive insulin infusion adjustments at the time of administration of known caloric loads—such as antibiotics delivered as a bolus in D5W solution—or at the time of initiation of high dose steroids or epinephrine drips, may be a means to keep a higher percentage of blood sugars in range. Ultimately, continuous blood sensing devices with closed loop insulin infusion responses are desired.
For now, our protocol offers a user-friendly means of getting a high percentage of critical care patients into a reasonable glycemic range with a low risk of hypoglycemia. Others are free to use and/or modify it. TH
The authors work at Southwest Washington Medical Center, Vancouver, Wash.
References
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Malmberg K, Norhammar A, Wedel H, et al. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626-2632.
- Furnary AP, Wu Y, Bookin SO. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland diabetic project. Endocr Pract. 2006 Mar-Apr;12 Suppl 3:22-26.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc. 2004 Aug;79(8):992-1000.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004 Oct 11;164(18):2005-2011.
- Goldberg PA. Memoirs of a root canal salesman: the successful implementation of a hospital-wide intravenous insulin infusion protocol. Endocr Pract. 2006;12 Suppl 3:79-85.
- Markovitz LJ, Weichmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract. 2002 Jan-Feb;8(1):10-18.
- Ku SY, Sayre CA, Hirsch IB, et al. New insulin infusion protocol improves blood glucose control in hospitalized patients without increasing hypoglycemia. Jt Comm J Qual Patient Saf. 2005 Mar;31(3):141-147.
- Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and continuous intravenous insulin infusions on outcomes of cardiac surgical procedures: the Portland Diabetic Project. Endocr Pract. 2004 Mar-Apr;10 Suppl 2:21-33.
- In a written communication from Andy Ahmann, MD, OHSU, in 2006.
- Georgia Hospital Association Diabetes Protocols. Chart 6b. Available at: www.adaendo.com/GHA/index.html. Accessed October 29, 2006.
- In a written communication from Terry Clemmer, MD, director, Critical Care Medicine, LDS Hospital, Salt Lake City, Utah, in October 2006.
- Braithwaite SS, Godara H, Song HJ, et al. No patient left behind: evaluation and design of intravenous insulin infusion algorithms. Endocr Pract. 2006 Jul-Aug;12 Suppl 3:72-78.