Article
Functional heartburn: An underrecognized cause of PPI-refractory symptoms
Functional heartburn is the most common cause of failure of proton pump inhibitor therapy.
Article

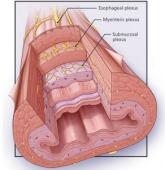
A man with progressive dysphagia
Difficulty swallowing can be caused by problems in the oropharynx or in the esophagus.
Article
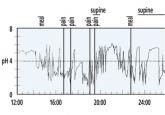
GERD: Diagnosing and treating the burn
If symptoms do not respond to a proton pump inhibitor or are atypical, testing may be needed.