User login
The Obesity Problem in U.S. Hospitals
The United States is growing. That is, its individual inhabitants are getting bigger. Depending on the source, anywhere from 30% to 50% of the American population is now obese.1-3 By all accounts, the percentage of obese adults in our country has risen considerably over the past two decades and continues to rise.
When asked about challenges in treating the obese patient, many medical professionals will expound on bariatric treatments and surgeries—programs designed to help patients lose weight. Addressed far less frequently are the challenges faced by physicians—specifically hospitalists—in treating the obese patient for a routine or emergency medical problem or traumatic injury.
Complicating Factors
Obesity is a contributing factor to a myriad of medical problems. The American Heart Association lists obesity as one of several modifiable independent risk factors for cardiovascular disease.4 Overweight individuals are also at higher risk for a long list of other diseases, including high blood pressure, high cholesterol, type 2 diabetes, stroke, gallbladder disease, arthritis, sleep disturbances and problems breathing, and certain types of cancers.5 There is also growing evidence that obesity may be a risk factor for asthma.6
Obese patients may delay seeking medical care for a number of reasons, including self-consciousness about their weight, fear of negative comments from physicians and staff, or past negative experiences with hospitals or staff.2 When patients delay seeking appropriate preventive care, they are more likely to end up in the emergency department or be admitted to the hospital and, consequently, under the care of a hospitalist.
The Transport Conundrum
Furniture, equipment, medical supplies, and everything else commonly used in the hospital are designed to accommodate the average-size adult. In fact, for many morbidly obese patients, the difficulty begins immediately upon arrival at (or even before reaching) the hospital.
When a patient suffers an acute illness or traumatic injury, the logical reaction in many cases is to call an ambulance for transport to the hospital. For a large person, this can create the first dilemma in receiving care. Many ambulance companies now have stretchers with weight ratings of up to 700 pounds. However, moving a stretcher loaded with several hundred pounds of patient can be quite a challenge for ambulance personnel—even with extra crew members available.
If the patient is not ambulatory, the crew must find a way to place the patient onto the stretcher and then to move the stretcher into their ambulance. They can face the difficulty of not only lifting and moving such a heavy load, but also moving through doorways, down stairs, and across uneven surfaces. Simply dealing with the logistics of moving the patient safely can be time-consuming and can cause a delay in administering emergency care to the patient.
Upon arrival at the hospital, the same dilemmas will arise in transferring the patient from the ambulance stretcher to a hospital bed. Many devices designed to aid in lifting and moving patients are not rated for use with the morbidly obese patient. There must be sufficient staff on hand to facilitate transfer of the patient, and the staff must be well educated in lifting and moving techniques safe for staff and patient.
The issues regarding the lifting and moving of obese patients present significant safety implications for hospital employees. Michael Allswede, DO, residency program director for Emergency Medicine Residency at Conemaugh Health Systems in Johnstown, Pa., says that this particular issue is compounded by the fact that many hospital employees are overweight themselves. “You basically have obese people trying to lift obese people,” he says.
In a Novation survey of VHA member hospitals released in December 2004, 28% of respondents reported an increase in workplace injuries—primarily back injuries—related to lifting obese patients.7 The National Council of Compensation estimates the average cost per healthcare worker injury to be $8,400.8 This increase in worker’s compensation claims clearly has a significant financial impact on hospitals.
Diagnosis Made Difficult
Once the patient is situated, the medical staff faces the challenge of how to best assess the patient as accurately as possible. Basic vital signs can be difficult to obtain. With several layers of fat between the arteries and skin surface, pulses can be difficult—if not impossible—to palpate. Blood pressure cuffs must be large enough to avoid obtaining false readings. It can be difficult to auscultate lung sounds and cardiac rhythms; it may also be impossible to assess the abdomen by typical hands-on examination techniques. Even visualizing the entire skin surface can be difficult and time-consuming.
Obtaining diagnostic studies presents yet another challenge: Needles used for drawing blood may not be long enough to reach a vein through the layers of fat. CT and MRI images may not be possible if the gantry does not have a high enough weight rating, and there is also the possibility that the patient simply will not fit into the machine. Because body fat basically places a pillow between internal organs and the sensoring unit, ultrasound images may be impossible to obtain. Even something as simple as a chest X-ray may be difficult to interpret because of the difficulty of trying to diagnose the density difference between infected lung lobes versus the chest around it.
Dr. Allswede says that with the usual preferred diagnostic tools often rendered useless doctors have only two choices: “We can watch and wait, or we can perform invasive procedures.”
When an invasive procedure is necessary, Dr. Allswede cautions, physicians cannot rely on normal body landmarks to aid in location of underlying organs. Procedures such as placement of central lines, chest tubes, and peritoneal lavage can become a guessing game for the physician. “The normal body markings don’t align with body cavities,” he explains. “It becomes more difficult to do landmark locating for procedures.”
ABCs of Treating Obese Patients
Even the most basic medical management can be made difficult by obesity. Management of airway, breathing, and circulation is generally straightforward, and the protocols and procedures are standard; however, in the extremely obese patient problems can arise that are generally unseen in the average patient.
Morbidly obese patients desaturate more quickly than other adults. This can make it even more imperative than usual that a patent airway be obtained and maintained. Obesity makes it more difficult for the physician to visualize the laryngeal structures when attempting to intubate. Further, ventilation is made more difficult because of reduced pulmonary compliance, increased chest wall resistance, increased airway resistance, abnormal diaphragmatic position, and increased upper airway resistance.3
These patients have increased blood volumes, increased cardiac output, increased left ventricular volume, and lowered systemic vascular resistance. They may display atypical cardiac rhythms. Obtaining venous access can be extremely difficult in obese patients.3
Some of these problems can be solved by patient positioning, but some may require improvised techniques and/or specialized equipment.
Drug dosages must be modified for a morbidly obese patient; however, this is not simply a matter of larger body equaling larger dose. The physician must differentiate between fat-soluble and water-soluble medications, and obtain an estimate of the patient’s weight and body mass index to determine the proper dose of any given medication. Having a quick reference chart available for the most commonly used medications may be somewhat helpful, but it would be impossible to anticipate every possible drug-dosing dilemma. Figuring the proper dose can take some time, time that is not always available in a life-threatening situation.
Costly Solutions
Rising costs of caring for obese patients results in increased costs for everybody. The Centers for Disease Control estimates that the cost of caring for an overweight or obese patient is an average of 37% more than the cost of caring for a person of normal weight. This adds an average of $732 annually to the medical bill of every patient.8
In an effort to provide quality medical care to larger patients, many hospitals must purchase specialized equipment and supplies. There are hundreds of products available designed to help facilitate medical care of obese patients. Some hospitals are investing a great deal of money in caring for obese individuals, from lifting and moving equipment such as stretchers, wheelchairs, and lifts, to furniture such as beds and chairs, to medical equipment, including blood pressure cuffs, longer needles, and retractors.
Some facilities are making structural changes, such as widening doorways and hallways, to accommodate the passage of the larger equipment loaded with the larger patient. The 2004 Novation survey reported the mean estimated cost of new supplies to be $43,015. The mean cost of renovations in 2004 was $22,000 (compared with $15,250 in 2003).7
Conclusion
There is no doubt that the treatment of obese patients presents unique, sometimes expensive, challenges to hospitals and hospitalists. Hospitals have a responsibility to have the necessary diagnostic and treatment equipment available. Hospitalists have a responsibility to be familiar with the ways they can modify existing procedures and techniques to achieve a more desirable outcome in the obese patient. Above all, every effort must be expended to ensure that the obese patient is given the same respect and the same quality of care as every other patient. TH
Sheri Polley is based in Pennsylvania.
References
- Weight Loss & Obesity Resource Center. Medical Care for Obese Patients. Available at: http://weightlossobesity.com/obesity/medical-care-for-obese-patients.html. Last accessed May 17, 2006.
- Weight Control Information Network. Medical Care for Obese Patients. Available at: http://win.niddk.nih.gov/publications/medical.htm. Last accessed May 17, 2006.
- Brunette DD. Resuscitation of the morbidly obese patient. Am J Emerg Med. 2004 Jan;22(1):40-47.
- Criqui MH. Obesity, risk factors, and predicting cardiovascular events. Circulation. 2005 Apr 19;111 (15):1869-1870. Available online at: http://circ.ahajournals.org/cgi/content/full/111/15/1869. Last accessed May 17, 2006.
- New York Office for the Aging 2001–2004. Overweight & Obesity. Available at: www.agingwell.state.ny.us/prevention/overweight.htm. Last accessed May 22, 2006.
- Medical News Today. Is obesity a risk factor for asthma? Available at: www.medicalnewstoday.com/medicalnews.php?newsid=24118. Last accessed May 17, 2006.
- VHA. 2004 obese patient care survey market research report. Available at: www.vha.com/portal/server.pt/gateway/PTARGS_0_2_1534_234_0_43/http%3B/remote.vha.com/public/research/docs/obestpatientcare.pdf. Last accessed May 6, 2006.
- Akridge J. Bariatrics products help hospitals serve growing market. Healthcare Purchasing News. 2004 Mar. Available at: www.highbeam.com/library/docfree.asp?DOCID=1G1:124790587&num=1&ctrlInfo=Round20%3AMode20a%3ASR%3AResult&ao=&FreePremium=BOTH&tab=lib. Last accessed July19, 2006.
Classic Literature
1903 Article Introduces Early Electrocardiogram
By Jamie Newman, MD FACP
Einthoven W. The galvanometric registration of the Human Electrocardiogram, likewise a review of the use of the capillary electrometer in physiology. Pfluger’s Arch.1903;99:472-480.
This landmark article represents one of the greatest achievements in the diagnosis of diseases of the heart. In tandem with the work of Werner Forssman and the first cardiac catheterization, it is the basis for modern cardiology.
Willem Einthoven was Dutch and served as the chair of physiology and histology at the University of Leiden, the Netherlands, for four decades. He based his work on the prior efforts of Luigi Galvani, Carlo Matteucci, and—most importantly—A.D. Waller, who showed that “leads” placed externally could measure the electric activity of the heart, using a capillary electrometer. (See Figure 1.) This device used a column of mercury, which responded to electric current but was inexact and not clinically useful.
In 1903, Einthoven used a galvanometer to measure this current. In this article he describes the physical principles of the electrocardiogram, as well as some early tracings. (See Figure 2.)
In 1924, he was awarded the Nobel Prize in physiology or medicine.
The United States is growing. That is, its individual inhabitants are getting bigger. Depending on the source, anywhere from 30% to 50% of the American population is now obese.1-3 By all accounts, the percentage of obese adults in our country has risen considerably over the past two decades and continues to rise.
When asked about challenges in treating the obese patient, many medical professionals will expound on bariatric treatments and surgeries—programs designed to help patients lose weight. Addressed far less frequently are the challenges faced by physicians—specifically hospitalists—in treating the obese patient for a routine or emergency medical problem or traumatic injury.
Complicating Factors
Obesity is a contributing factor to a myriad of medical problems. The American Heart Association lists obesity as one of several modifiable independent risk factors for cardiovascular disease.4 Overweight individuals are also at higher risk for a long list of other diseases, including high blood pressure, high cholesterol, type 2 diabetes, stroke, gallbladder disease, arthritis, sleep disturbances and problems breathing, and certain types of cancers.5 There is also growing evidence that obesity may be a risk factor for asthma.6
Obese patients may delay seeking medical care for a number of reasons, including self-consciousness about their weight, fear of negative comments from physicians and staff, or past negative experiences with hospitals or staff.2 When patients delay seeking appropriate preventive care, they are more likely to end up in the emergency department or be admitted to the hospital and, consequently, under the care of a hospitalist.
The Transport Conundrum
Furniture, equipment, medical supplies, and everything else commonly used in the hospital are designed to accommodate the average-size adult. In fact, for many morbidly obese patients, the difficulty begins immediately upon arrival at (or even before reaching) the hospital.
When a patient suffers an acute illness or traumatic injury, the logical reaction in many cases is to call an ambulance for transport to the hospital. For a large person, this can create the first dilemma in receiving care. Many ambulance companies now have stretchers with weight ratings of up to 700 pounds. However, moving a stretcher loaded with several hundred pounds of patient can be quite a challenge for ambulance personnel—even with extra crew members available.
If the patient is not ambulatory, the crew must find a way to place the patient onto the stretcher and then to move the stretcher into their ambulance. They can face the difficulty of not only lifting and moving such a heavy load, but also moving through doorways, down stairs, and across uneven surfaces. Simply dealing with the logistics of moving the patient safely can be time-consuming and can cause a delay in administering emergency care to the patient.
Upon arrival at the hospital, the same dilemmas will arise in transferring the patient from the ambulance stretcher to a hospital bed. Many devices designed to aid in lifting and moving patients are not rated for use with the morbidly obese patient. There must be sufficient staff on hand to facilitate transfer of the patient, and the staff must be well educated in lifting and moving techniques safe for staff and patient.
The issues regarding the lifting and moving of obese patients present significant safety implications for hospital employees. Michael Allswede, DO, residency program director for Emergency Medicine Residency at Conemaugh Health Systems in Johnstown, Pa., says that this particular issue is compounded by the fact that many hospital employees are overweight themselves. “You basically have obese people trying to lift obese people,” he says.
In a Novation survey of VHA member hospitals released in December 2004, 28% of respondents reported an increase in workplace injuries—primarily back injuries—related to lifting obese patients.7 The National Council of Compensation estimates the average cost per healthcare worker injury to be $8,400.8 This increase in worker’s compensation claims clearly has a significant financial impact on hospitals.
Diagnosis Made Difficult
Once the patient is situated, the medical staff faces the challenge of how to best assess the patient as accurately as possible. Basic vital signs can be difficult to obtain. With several layers of fat between the arteries and skin surface, pulses can be difficult—if not impossible—to palpate. Blood pressure cuffs must be large enough to avoid obtaining false readings. It can be difficult to auscultate lung sounds and cardiac rhythms; it may also be impossible to assess the abdomen by typical hands-on examination techniques. Even visualizing the entire skin surface can be difficult and time-consuming.
Obtaining diagnostic studies presents yet another challenge: Needles used for drawing blood may not be long enough to reach a vein through the layers of fat. CT and MRI images may not be possible if the gantry does not have a high enough weight rating, and there is also the possibility that the patient simply will not fit into the machine. Because body fat basically places a pillow between internal organs and the sensoring unit, ultrasound images may be impossible to obtain. Even something as simple as a chest X-ray may be difficult to interpret because of the difficulty of trying to diagnose the density difference between infected lung lobes versus the chest around it.
Dr. Allswede says that with the usual preferred diagnostic tools often rendered useless doctors have only two choices: “We can watch and wait, or we can perform invasive procedures.”
When an invasive procedure is necessary, Dr. Allswede cautions, physicians cannot rely on normal body landmarks to aid in location of underlying organs. Procedures such as placement of central lines, chest tubes, and peritoneal lavage can become a guessing game for the physician. “The normal body markings don’t align with body cavities,” he explains. “It becomes more difficult to do landmark locating for procedures.”
ABCs of Treating Obese Patients
Even the most basic medical management can be made difficult by obesity. Management of airway, breathing, and circulation is generally straightforward, and the protocols and procedures are standard; however, in the extremely obese patient problems can arise that are generally unseen in the average patient.
Morbidly obese patients desaturate more quickly than other adults. This can make it even more imperative than usual that a patent airway be obtained and maintained. Obesity makes it more difficult for the physician to visualize the laryngeal structures when attempting to intubate. Further, ventilation is made more difficult because of reduced pulmonary compliance, increased chest wall resistance, increased airway resistance, abnormal diaphragmatic position, and increased upper airway resistance.3
These patients have increased blood volumes, increased cardiac output, increased left ventricular volume, and lowered systemic vascular resistance. They may display atypical cardiac rhythms. Obtaining venous access can be extremely difficult in obese patients.3
Some of these problems can be solved by patient positioning, but some may require improvised techniques and/or specialized equipment.
Drug dosages must be modified for a morbidly obese patient; however, this is not simply a matter of larger body equaling larger dose. The physician must differentiate between fat-soluble and water-soluble medications, and obtain an estimate of the patient’s weight and body mass index to determine the proper dose of any given medication. Having a quick reference chart available for the most commonly used medications may be somewhat helpful, but it would be impossible to anticipate every possible drug-dosing dilemma. Figuring the proper dose can take some time, time that is not always available in a life-threatening situation.
Costly Solutions
Rising costs of caring for obese patients results in increased costs for everybody. The Centers for Disease Control estimates that the cost of caring for an overweight or obese patient is an average of 37% more than the cost of caring for a person of normal weight. This adds an average of $732 annually to the medical bill of every patient.8
In an effort to provide quality medical care to larger patients, many hospitals must purchase specialized equipment and supplies. There are hundreds of products available designed to help facilitate medical care of obese patients. Some hospitals are investing a great deal of money in caring for obese individuals, from lifting and moving equipment such as stretchers, wheelchairs, and lifts, to furniture such as beds and chairs, to medical equipment, including blood pressure cuffs, longer needles, and retractors.
Some facilities are making structural changes, such as widening doorways and hallways, to accommodate the passage of the larger equipment loaded with the larger patient. The 2004 Novation survey reported the mean estimated cost of new supplies to be $43,015. The mean cost of renovations in 2004 was $22,000 (compared with $15,250 in 2003).7
Conclusion
There is no doubt that the treatment of obese patients presents unique, sometimes expensive, challenges to hospitals and hospitalists. Hospitals have a responsibility to have the necessary diagnostic and treatment equipment available. Hospitalists have a responsibility to be familiar with the ways they can modify existing procedures and techniques to achieve a more desirable outcome in the obese patient. Above all, every effort must be expended to ensure that the obese patient is given the same respect and the same quality of care as every other patient. TH
Sheri Polley is based in Pennsylvania.
References
- Weight Loss & Obesity Resource Center. Medical Care for Obese Patients. Available at: http://weightlossobesity.com/obesity/medical-care-for-obese-patients.html. Last accessed May 17, 2006.
- Weight Control Information Network. Medical Care for Obese Patients. Available at: http://win.niddk.nih.gov/publications/medical.htm. Last accessed May 17, 2006.
- Brunette DD. Resuscitation of the morbidly obese patient. Am J Emerg Med. 2004 Jan;22(1):40-47.
- Criqui MH. Obesity, risk factors, and predicting cardiovascular events. Circulation. 2005 Apr 19;111 (15):1869-1870. Available online at: http://circ.ahajournals.org/cgi/content/full/111/15/1869. Last accessed May 17, 2006.
- New York Office for the Aging 2001–2004. Overweight & Obesity. Available at: www.agingwell.state.ny.us/prevention/overweight.htm. Last accessed May 22, 2006.
- Medical News Today. Is obesity a risk factor for asthma? Available at: www.medicalnewstoday.com/medicalnews.php?newsid=24118. Last accessed May 17, 2006.
- VHA. 2004 obese patient care survey market research report. Available at: www.vha.com/portal/server.pt/gateway/PTARGS_0_2_1534_234_0_43/http%3B/remote.vha.com/public/research/docs/obestpatientcare.pdf. Last accessed May 6, 2006.
- Akridge J. Bariatrics products help hospitals serve growing market. Healthcare Purchasing News. 2004 Mar. Available at: www.highbeam.com/library/docfree.asp?DOCID=1G1:124790587&num=1&ctrlInfo=Round20%3AMode20a%3ASR%3AResult&ao=&FreePremium=BOTH&tab=lib. Last accessed July19, 2006.
Classic Literature
1903 Article Introduces Early Electrocardiogram
By Jamie Newman, MD FACP
Einthoven W. The galvanometric registration of the Human Electrocardiogram, likewise a review of the use of the capillary electrometer in physiology. Pfluger’s Arch.1903;99:472-480.
This landmark article represents one of the greatest achievements in the diagnosis of diseases of the heart. In tandem with the work of Werner Forssman and the first cardiac catheterization, it is the basis for modern cardiology.
Willem Einthoven was Dutch and served as the chair of physiology and histology at the University of Leiden, the Netherlands, for four decades. He based his work on the prior efforts of Luigi Galvani, Carlo Matteucci, and—most importantly—A.D. Waller, who showed that “leads” placed externally could measure the electric activity of the heart, using a capillary electrometer. (See Figure 1.) This device used a column of mercury, which responded to electric current but was inexact and not clinically useful.
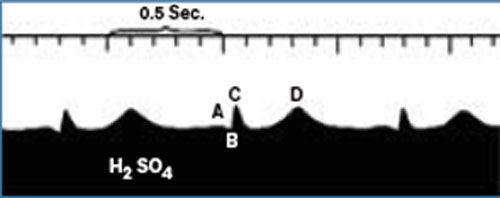
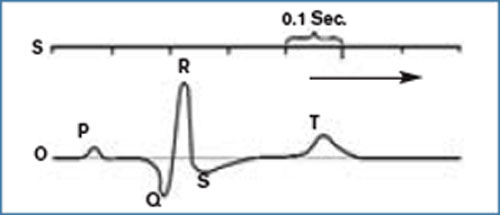
In 1903, Einthoven used a galvanometer to measure this current. In this article he describes the physical principles of the electrocardiogram, as well as some early tracings. (See Figure 2.)
In 1924, he was awarded the Nobel Prize in physiology or medicine.
The United States is growing. That is, its individual inhabitants are getting bigger. Depending on the source, anywhere from 30% to 50% of the American population is now obese.1-3 By all accounts, the percentage of obese adults in our country has risen considerably over the past two decades and continues to rise.
When asked about challenges in treating the obese patient, many medical professionals will expound on bariatric treatments and surgeries—programs designed to help patients lose weight. Addressed far less frequently are the challenges faced by physicians—specifically hospitalists—in treating the obese patient for a routine or emergency medical problem or traumatic injury.
Complicating Factors
Obesity is a contributing factor to a myriad of medical problems. The American Heart Association lists obesity as one of several modifiable independent risk factors for cardiovascular disease.4 Overweight individuals are also at higher risk for a long list of other diseases, including high blood pressure, high cholesterol, type 2 diabetes, stroke, gallbladder disease, arthritis, sleep disturbances and problems breathing, and certain types of cancers.5 There is also growing evidence that obesity may be a risk factor for asthma.6
Obese patients may delay seeking medical care for a number of reasons, including self-consciousness about their weight, fear of negative comments from physicians and staff, or past negative experiences with hospitals or staff.2 When patients delay seeking appropriate preventive care, they are more likely to end up in the emergency department or be admitted to the hospital and, consequently, under the care of a hospitalist.
The Transport Conundrum
Furniture, equipment, medical supplies, and everything else commonly used in the hospital are designed to accommodate the average-size adult. In fact, for many morbidly obese patients, the difficulty begins immediately upon arrival at (or even before reaching) the hospital.
When a patient suffers an acute illness or traumatic injury, the logical reaction in many cases is to call an ambulance for transport to the hospital. For a large person, this can create the first dilemma in receiving care. Many ambulance companies now have stretchers with weight ratings of up to 700 pounds. However, moving a stretcher loaded with several hundred pounds of patient can be quite a challenge for ambulance personnel—even with extra crew members available.
If the patient is not ambulatory, the crew must find a way to place the patient onto the stretcher and then to move the stretcher into their ambulance. They can face the difficulty of not only lifting and moving such a heavy load, but also moving through doorways, down stairs, and across uneven surfaces. Simply dealing with the logistics of moving the patient safely can be time-consuming and can cause a delay in administering emergency care to the patient.
Upon arrival at the hospital, the same dilemmas will arise in transferring the patient from the ambulance stretcher to a hospital bed. Many devices designed to aid in lifting and moving patients are not rated for use with the morbidly obese patient. There must be sufficient staff on hand to facilitate transfer of the patient, and the staff must be well educated in lifting and moving techniques safe for staff and patient.
The issues regarding the lifting and moving of obese patients present significant safety implications for hospital employees. Michael Allswede, DO, residency program director for Emergency Medicine Residency at Conemaugh Health Systems in Johnstown, Pa., says that this particular issue is compounded by the fact that many hospital employees are overweight themselves. “You basically have obese people trying to lift obese people,” he says.
In a Novation survey of VHA member hospitals released in December 2004, 28% of respondents reported an increase in workplace injuries—primarily back injuries—related to lifting obese patients.7 The National Council of Compensation estimates the average cost per healthcare worker injury to be $8,400.8 This increase in worker’s compensation claims clearly has a significant financial impact on hospitals.
Diagnosis Made Difficult
Once the patient is situated, the medical staff faces the challenge of how to best assess the patient as accurately as possible. Basic vital signs can be difficult to obtain. With several layers of fat between the arteries and skin surface, pulses can be difficult—if not impossible—to palpate. Blood pressure cuffs must be large enough to avoid obtaining false readings. It can be difficult to auscultate lung sounds and cardiac rhythms; it may also be impossible to assess the abdomen by typical hands-on examination techniques. Even visualizing the entire skin surface can be difficult and time-consuming.
Obtaining diagnostic studies presents yet another challenge: Needles used for drawing blood may not be long enough to reach a vein through the layers of fat. CT and MRI images may not be possible if the gantry does not have a high enough weight rating, and there is also the possibility that the patient simply will not fit into the machine. Because body fat basically places a pillow between internal organs and the sensoring unit, ultrasound images may be impossible to obtain. Even something as simple as a chest X-ray may be difficult to interpret because of the difficulty of trying to diagnose the density difference between infected lung lobes versus the chest around it.
Dr. Allswede says that with the usual preferred diagnostic tools often rendered useless doctors have only two choices: “We can watch and wait, or we can perform invasive procedures.”
When an invasive procedure is necessary, Dr. Allswede cautions, physicians cannot rely on normal body landmarks to aid in location of underlying organs. Procedures such as placement of central lines, chest tubes, and peritoneal lavage can become a guessing game for the physician. “The normal body markings don’t align with body cavities,” he explains. “It becomes more difficult to do landmark locating for procedures.”
ABCs of Treating Obese Patients
Even the most basic medical management can be made difficult by obesity. Management of airway, breathing, and circulation is generally straightforward, and the protocols and procedures are standard; however, in the extremely obese patient problems can arise that are generally unseen in the average patient.
Morbidly obese patients desaturate more quickly than other adults. This can make it even more imperative than usual that a patent airway be obtained and maintained. Obesity makes it more difficult for the physician to visualize the laryngeal structures when attempting to intubate. Further, ventilation is made more difficult because of reduced pulmonary compliance, increased chest wall resistance, increased airway resistance, abnormal diaphragmatic position, and increased upper airway resistance.3
These patients have increased blood volumes, increased cardiac output, increased left ventricular volume, and lowered systemic vascular resistance. They may display atypical cardiac rhythms. Obtaining venous access can be extremely difficult in obese patients.3
Some of these problems can be solved by patient positioning, but some may require improvised techniques and/or specialized equipment.
Drug dosages must be modified for a morbidly obese patient; however, this is not simply a matter of larger body equaling larger dose. The physician must differentiate between fat-soluble and water-soluble medications, and obtain an estimate of the patient’s weight and body mass index to determine the proper dose of any given medication. Having a quick reference chart available for the most commonly used medications may be somewhat helpful, but it would be impossible to anticipate every possible drug-dosing dilemma. Figuring the proper dose can take some time, time that is not always available in a life-threatening situation.
Costly Solutions
Rising costs of caring for obese patients results in increased costs for everybody. The Centers for Disease Control estimates that the cost of caring for an overweight or obese patient is an average of 37% more than the cost of caring for a person of normal weight. This adds an average of $732 annually to the medical bill of every patient.8
In an effort to provide quality medical care to larger patients, many hospitals must purchase specialized equipment and supplies. There are hundreds of products available designed to help facilitate medical care of obese patients. Some hospitals are investing a great deal of money in caring for obese individuals, from lifting and moving equipment such as stretchers, wheelchairs, and lifts, to furniture such as beds and chairs, to medical equipment, including blood pressure cuffs, longer needles, and retractors.
Some facilities are making structural changes, such as widening doorways and hallways, to accommodate the passage of the larger equipment loaded with the larger patient. The 2004 Novation survey reported the mean estimated cost of new supplies to be $43,015. The mean cost of renovations in 2004 was $22,000 (compared with $15,250 in 2003).7
Conclusion
There is no doubt that the treatment of obese patients presents unique, sometimes expensive, challenges to hospitals and hospitalists. Hospitals have a responsibility to have the necessary diagnostic and treatment equipment available. Hospitalists have a responsibility to be familiar with the ways they can modify existing procedures and techniques to achieve a more desirable outcome in the obese patient. Above all, every effort must be expended to ensure that the obese patient is given the same respect and the same quality of care as every other patient. TH
Sheri Polley is based in Pennsylvania.
References
- Weight Loss & Obesity Resource Center. Medical Care for Obese Patients. Available at: http://weightlossobesity.com/obesity/medical-care-for-obese-patients.html. Last accessed May 17, 2006.
- Weight Control Information Network. Medical Care for Obese Patients. Available at: http://win.niddk.nih.gov/publications/medical.htm. Last accessed May 17, 2006.
- Brunette DD. Resuscitation of the morbidly obese patient. Am J Emerg Med. 2004 Jan;22(1):40-47.
- Criqui MH. Obesity, risk factors, and predicting cardiovascular events. Circulation. 2005 Apr 19;111 (15):1869-1870. Available online at: http://circ.ahajournals.org/cgi/content/full/111/15/1869. Last accessed May 17, 2006.
- New York Office for the Aging 2001–2004. Overweight & Obesity. Available at: www.agingwell.state.ny.us/prevention/overweight.htm. Last accessed May 22, 2006.
- Medical News Today. Is obesity a risk factor for asthma? Available at: www.medicalnewstoday.com/medicalnews.php?newsid=24118. Last accessed May 17, 2006.
- VHA. 2004 obese patient care survey market research report. Available at: www.vha.com/portal/server.pt/gateway/PTARGS_0_2_1534_234_0_43/http%3B/remote.vha.com/public/research/docs/obestpatientcare.pdf. Last accessed May 6, 2006.
- Akridge J. Bariatrics products help hospitals serve growing market. Healthcare Purchasing News. 2004 Mar. Available at: www.highbeam.com/library/docfree.asp?DOCID=1G1:124790587&num=1&ctrlInfo=Round20%3AMode20a%3ASR%3AResult&ao=&FreePremium=BOTH&tab=lib. Last accessed July19, 2006.
Classic Literature
1903 Article Introduces Early Electrocardiogram
By Jamie Newman, MD FACP
Einthoven W. The galvanometric registration of the Human Electrocardiogram, likewise a review of the use of the capillary electrometer in physiology. Pfluger’s Arch.1903;99:472-480.
This landmark article represents one of the greatest achievements in the diagnosis of diseases of the heart. In tandem with the work of Werner Forssman and the first cardiac catheterization, it is the basis for modern cardiology.
Willem Einthoven was Dutch and served as the chair of physiology and histology at the University of Leiden, the Netherlands, for four decades. He based his work on the prior efforts of Luigi Galvani, Carlo Matteucci, and—most importantly—A.D. Waller, who showed that “leads” placed externally could measure the electric activity of the heart, using a capillary electrometer. (See Figure 1.) This device used a column of mercury, which responded to electric current but was inexact and not clinically useful.
In 1903, Einthoven used a galvanometer to measure this current. In this article he describes the physical principles of the electrocardiogram, as well as some early tracings. (See Figure 2.)
In 1924, he was awarded the Nobel Prize in physiology or medicine.