User login
Foods can still trigger eosinophilic esophagitis after allergy outgrown
SAN DIEGO – Seventeen of 425 children who had eosinophilic esophagitis caused by a specific food developed the condition after outgrowing the allergy to that food, a retrospective study found.
People who outgrow a food allergy may be at risk of developing eosinophilic esophagitis (EoE) to the same food, Dr. Jonathan Spergel said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
He and his associates studied data on 1,025 children with EoE seen at the Children’s Hospital of Philadelphia in 2000-2012 to assess the prevalence of food allergy. In 425 children (42%), a specific food was identified as the EoE culprit – reintroducing the food to the diet caused esophageal changes on biopsy or biopsy changes normalized when the food was removed from the diet.

Eighty-four children had a history of IgE-mediated food allergy. Milk, egg, wheat, and soy were the most common food triggers of EoE in the 425 children in the study and in a subset of 17 who had outgrown IgE-mediated allergy to the specific food, reported Dr. Spergel, chief of the allergy section at the Children’s Hospital of Philadelphia. Sixteen of the 17 patients had atopic disease. The most common foods causing IgE-mediated allergy were peanuts, tree nuts, eggs, and milk.
The development of EoE coincided with reintroducing the food triggers. The time between outgrowing an allergy and reintroducing the food, triggering EoE, averaged 2 years but ranged from 6 months to 5 years.
Notably, two of the children who outgrew their food allergy had a normal biopsy of the esophagus when they had the food allergy, he said.
The findings support other recent studies suggesting that the pathophysiologies of EoE and IgE-mediated food allergy are distinct from each other, and that both can occur in the same individual to the same food, Dr. Spergel said. The mechanism by which EoE develops is poorly understood.
"I think these kids probably always had EoE to the food, but they weren’t eating it" because of the allergy, he said. "From 1% to 15% on oral immunotherapy get EoE, depending on which group you look at. I don’t think we caused" EoE by giving oral immunotherapy, he added. "We uncovered it."
Although it is rare for children who outgrow a food allergy to later develop EoE to that food, it’s worth keeping in mind if a child starts vomiting often or complains of stomachaches months or years later, Dr. Spergel said. Keeping the possibility in mind may help clinicians rule out other etiologies and detect EoE faster. "You have to take it seriously and get it checked out," he said.
Of the 84 patients with IgE-mediated food allergy, the 17 who outgrew the allergy and then developed EoE to the same food were significantly older (12 years, on average), compared with 67 patients who developed EoE from a different food from the one that caused their allergy.
The lead author on the study was Dr. Solrun Melkorka Meggadottir, a fellow at the Children’s Hospital of Philadelphia. The findings have been submitted to the Journal of Allergy and Clinical Immunology.
Dr. Spergel and Dr. Meggadottir reported having no relevant financial disclosures.
On Twitter @sherryboschert
 |
|
Just because patients who had a food allergy now tolerate a food doesn’t mean that they’re going to be absolutely clear. One of the questions we have is whether these people really had EoE before but, because they also had IgE-mediated food allergy and weren’t eating the food, they didn’t have the demonstration of EoE.
We also know from several of our oral immunotherapy trials that some of these patients, once they go on oral immunotherapy, do develop EoE as well. I think it’s something we have to be watching for.
Dr. Hugh A. Sampson is a professor of pediatrics, allergy, and immunology at Icahn School of Medicine at Mount Sinai, New York. He made these comments during a press briefing at the meeting. Dr. Sampsom disclosed relationships with Danone, Thermo Fisher Scientific, Allertein Therapeutics, Regeneron, and Novartis.
|
|
Just because patients who had a food allergy now tolerate a food doesn’t mean that they’re going to be absolutely clear. One of the questions we have is whether these people really had EoE before but, because they also had IgE-mediated food allergy and weren’t eating the food, they didn’t have the demonstration of EoE.
We also know from several of our oral immunotherapy trials that some of these patients, once they go on oral immunotherapy, do develop EoE as well. I think it’s something we have to be watching for.
Dr. Hugh A. Sampson is a professor of pediatrics, allergy, and immunology at Icahn School of Medicine at Mount Sinai, New York. He made these comments during a press briefing at the meeting. Dr. Sampsom disclosed relationships with Danone, Thermo Fisher Scientific, Allertein Therapeutics, Regeneron, and Novartis.
|
|
Just because patients who had a food allergy now tolerate a food doesn’t mean that they’re going to be absolutely clear. One of the questions we have is whether these people really had EoE before but, because they also had IgE-mediated food allergy and weren’t eating the food, they didn’t have the demonstration of EoE.
We also know from several of our oral immunotherapy trials that some of these patients, once they go on oral immunotherapy, do develop EoE as well. I think it’s something we have to be watching for.
Dr. Hugh A. Sampson is a professor of pediatrics, allergy, and immunology at Icahn School of Medicine at Mount Sinai, New York. He made these comments during a press briefing at the meeting. Dr. Sampsom disclosed relationships with Danone, Thermo Fisher Scientific, Allertein Therapeutics, Regeneron, and Novartis.
SAN DIEGO – Seventeen of 425 children who had eosinophilic esophagitis caused by a specific food developed the condition after outgrowing the allergy to that food, a retrospective study found.
People who outgrow a food allergy may be at risk of developing eosinophilic esophagitis (EoE) to the same food, Dr. Jonathan Spergel said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
He and his associates studied data on 1,025 children with EoE seen at the Children’s Hospital of Philadelphia in 2000-2012 to assess the prevalence of food allergy. In 425 children (42%), a specific food was identified as the EoE culprit – reintroducing the food to the diet caused esophageal changes on biopsy or biopsy changes normalized when the food was removed from the diet.
Eighty-four children had a history of IgE-mediated food allergy. Milk, egg, wheat, and soy were the most common food triggers of EoE in the 425 children in the study and in a subset of 17 who had outgrown IgE-mediated allergy to the specific food, reported Dr. Spergel, chief of the allergy section at the Children’s Hospital of Philadelphia. Sixteen of the 17 patients had atopic disease. The most common foods causing IgE-mediated allergy were peanuts, tree nuts, eggs, and milk.
The development of EoE coincided with reintroducing the food triggers. The time between outgrowing an allergy and reintroducing the food, triggering EoE, averaged 2 years but ranged from 6 months to 5 years.
Notably, two of the children who outgrew their food allergy had a normal biopsy of the esophagus when they had the food allergy, he said.
The findings support other recent studies suggesting that the pathophysiologies of EoE and IgE-mediated food allergy are distinct from each other, and that both can occur in the same individual to the same food, Dr. Spergel said. The mechanism by which EoE develops is poorly understood.
"I think these kids probably always had EoE to the food, but they weren’t eating it" because of the allergy, he said. "From 1% to 15% on oral immunotherapy get EoE, depending on which group you look at. I don’t think we caused" EoE by giving oral immunotherapy, he added. "We uncovered it."
Although it is rare for children who outgrow a food allergy to later develop EoE to that food, it’s worth keeping in mind if a child starts vomiting often or complains of stomachaches months or years later, Dr. Spergel said. Keeping the possibility in mind may help clinicians rule out other etiologies and detect EoE faster. "You have to take it seriously and get it checked out," he said.
Of the 84 patients with IgE-mediated food allergy, the 17 who outgrew the allergy and then developed EoE to the same food were significantly older (12 years, on average), compared with 67 patients who developed EoE from a different food from the one that caused their allergy.
The lead author on the study was Dr. Solrun Melkorka Meggadottir, a fellow at the Children’s Hospital of Philadelphia. The findings have been submitted to the Journal of Allergy and Clinical Immunology.
Dr. Spergel and Dr. Meggadottir reported having no relevant financial disclosures.
On Twitter @sherryboschert
SAN DIEGO – Seventeen of 425 children who had eosinophilic esophagitis caused by a specific food developed the condition after outgrowing the allergy to that food, a retrospective study found.
People who outgrow a food allergy may be at risk of developing eosinophilic esophagitis (EoE) to the same food, Dr. Jonathan Spergel said during a press briefing at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
He and his associates studied data on 1,025 children with EoE seen at the Children’s Hospital of Philadelphia in 2000-2012 to assess the prevalence of food allergy. In 425 children (42%), a specific food was identified as the EoE culprit – reintroducing the food to the diet caused esophageal changes on biopsy or biopsy changes normalized when the food was removed from the diet.
Eighty-four children had a history of IgE-mediated food allergy. Milk, egg, wheat, and soy were the most common food triggers of EoE in the 425 children in the study and in a subset of 17 who had outgrown IgE-mediated allergy to the specific food, reported Dr. Spergel, chief of the allergy section at the Children’s Hospital of Philadelphia. Sixteen of the 17 patients had atopic disease. The most common foods causing IgE-mediated allergy were peanuts, tree nuts, eggs, and milk.
The development of EoE coincided with reintroducing the food triggers. The time between outgrowing an allergy and reintroducing the food, triggering EoE, averaged 2 years but ranged from 6 months to 5 years.
Notably, two of the children who outgrew their food allergy had a normal biopsy of the esophagus when they had the food allergy, he said.
The findings support other recent studies suggesting that the pathophysiologies of EoE and IgE-mediated food allergy are distinct from each other, and that both can occur in the same individual to the same food, Dr. Spergel said. The mechanism by which EoE develops is poorly understood.
"I think these kids probably always had EoE to the food, but they weren’t eating it" because of the allergy, he said. "From 1% to 15% on oral immunotherapy get EoE, depending on which group you look at. I don’t think we caused" EoE by giving oral immunotherapy, he added. "We uncovered it."
Although it is rare for children who outgrow a food allergy to later develop EoE to that food, it’s worth keeping in mind if a child starts vomiting often or complains of stomachaches months or years later, Dr. Spergel said. Keeping the possibility in mind may help clinicians rule out other etiologies and detect EoE faster. "You have to take it seriously and get it checked out," he said.
Of the 84 patients with IgE-mediated food allergy, the 17 who outgrew the allergy and then developed EoE to the same food were significantly older (12 years, on average), compared with 67 patients who developed EoE from a different food from the one that caused their allergy.
The lead author on the study was Dr. Solrun Melkorka Meggadottir, a fellow at the Children’s Hospital of Philadelphia. The findings have been submitted to the Journal of Allergy and Clinical Immunology.
Dr. Spergel and Dr. Meggadottir reported having no relevant financial disclosures.
On Twitter @sherryboschert
AT 2014 AAAAI ANNUAL MEETING
Major finding: Seventeen of 425 children with eosinophilic esophagitis caused by a specific food redeveloped the condition after outgrowing an allergy to the same food.
Data source: A retrospective study of data on 1,025 children seen at one institution for eosinophilic esophagitis.
Disclosures: Dr. Spergel and Dr. Meggadottir reported having no relevant financial disclosures.

Stroke risk jumps after head, neck trauma
SAN DIEGO – Eleven of every 100,000 patients younger than 50 years who were seen for traumatic injury developed an ischemic stroke within 4 weeks, a study of data on 1.3 million people found.
Patients with head or neck trauma were three times more likely overall to have a stroke than were those who had other forms of trauma, although the risk varied by age, Dr. Heather Fullerton said in a press briefing at the International Stroke Conference, sponsored by the American Heart Association. Among those with head or neck trauma, ischemic strokes occurred in 0.01% of the children and in 0.05% of the adults within a month of being seen.
Rates in both those age groups were significantly higher than rates reported in the literature for similar ages in the general population, she added.
"Strokes are something that affect young people, not just older people, particularly after a traumatic event," the findings showed, so people should apply the FAST criteria for recognizing the warning signs of stroke to potential stroke victims of any age, Dr. Fullerton said. The FAST acronym refers to the face (does the smile droop?), the arms (if arms are raised, does one drift downward?), speech (slurred or strange?), and time (get emergency help if these signs are present).

"People should seek emergency care for those symptoms regardless of their age, but especially if they happen to have a recent traumatic event," said Dr. Fullerton, professor of neurology at the University of California, San Francisco, and director of the pediatric stroke and cerebrovascular disease center there. Emergency departments see more than 2 million people under age 50 every month for nonfatal traumatic injuries in the United States.
The investigators analyzed data on patients aged 50 years or younger who were insured by Kaiser Permanente and seen in emergency departments or admitted for trauma at either Kaiser or non-Kaiser hospitals in 1997-2011. A neurologist reviewed the records and excluded cases inconsistent with ischemic stroke.
Combining the findings with other national data, she estimated that 214 people younger than 50 years develop an ischemic stroke after a traumatic injury every month in the United States.
Among patients with head or neck trauma, 48 of every 100,000 adults in the study developed a stroke within a month, compared with stroke rates in the general population of young adults of approximately 10/100,000 adults per year, not per month, she said.
In children with head or neck trauma, 11/100,000 in the study developed stroke within a month, compared with general population rates of approximately 2.5 strokes per 100,000 children per year, not per month. Previous research by Dr. Fullerton and her associates suggests that the highest risk in children is within the first week after trauma, she added.
Trauma can tear blood vessels that lead to the brain and cause blood clots resulting in ischemic stroke. Ten percent of patients in the study who developed a stroke were diagnosed with tears in blood vessels leading to the brain, but some of these arterial dissections were diagnosed after the stroke occurred. Most of the strokes in the study probably were due to arterial dissection but were possibly mild enough that an obvious tear didn’t show up on imaging, Dr. Fullerton suggested.
The researchers next are planning a nested case-control study to help identify trauma patients at the highest risk of stroke and to examine the possibilities for stroke prevention.
The American Heart Association funded the current study. The investigators reported having no financial disclosures.
On Twitter @sherryboschert
SAN DIEGO – Eleven of every 100,000 patients younger than 50 years who were seen for traumatic injury developed an ischemic stroke within 4 weeks, a study of data on 1.3 million people found.
Patients with head or neck trauma were three times more likely overall to have a stroke than were those who had other forms of trauma, although the risk varied by age, Dr. Heather Fullerton said in a press briefing at the International Stroke Conference, sponsored by the American Heart Association. Among those with head or neck trauma, ischemic strokes occurred in 0.01% of the children and in 0.05% of the adults within a month of being seen.
Rates in both those age groups were significantly higher than rates reported in the literature for similar ages in the general population, she added.
"Strokes are something that affect young people, not just older people, particularly after a traumatic event," the findings showed, so people should apply the FAST criteria for recognizing the warning signs of stroke to potential stroke victims of any age, Dr. Fullerton said. The FAST acronym refers to the face (does the smile droop?), the arms (if arms are raised, does one drift downward?), speech (slurred or strange?), and time (get emergency help if these signs are present).
"People should seek emergency care for those symptoms regardless of their age, but especially if they happen to have a recent traumatic event," said Dr. Fullerton, professor of neurology at the University of California, San Francisco, and director of the pediatric stroke and cerebrovascular disease center there. Emergency departments see more than 2 million people under age 50 every month for nonfatal traumatic injuries in the United States.
The investigators analyzed data on patients aged 50 years or younger who were insured by Kaiser Permanente and seen in emergency departments or admitted for trauma at either Kaiser or non-Kaiser hospitals in 1997-2011. A neurologist reviewed the records and excluded cases inconsistent with ischemic stroke.
Combining the findings with other national data, she estimated that 214 people younger than 50 years develop an ischemic stroke after a traumatic injury every month in the United States.
Among patients with head or neck trauma, 48 of every 100,000 adults in the study developed a stroke within a month, compared with stroke rates in the general population of young adults of approximately 10/100,000 adults per year, not per month, she said.
In children with head or neck trauma, 11/100,000 in the study developed stroke within a month, compared with general population rates of approximately 2.5 strokes per 100,000 children per year, not per month. Previous research by Dr. Fullerton and her associates suggests that the highest risk in children is within the first week after trauma, she added.
Trauma can tear blood vessels that lead to the brain and cause blood clots resulting in ischemic stroke. Ten percent of patients in the study who developed a stroke were diagnosed with tears in blood vessels leading to the brain, but some of these arterial dissections were diagnosed after the stroke occurred. Most of the strokes in the study probably were due to arterial dissection but were possibly mild enough that an obvious tear didn’t show up on imaging, Dr. Fullerton suggested.
The researchers next are planning a nested case-control study to help identify trauma patients at the highest risk of stroke and to examine the possibilities for stroke prevention.
The American Heart Association funded the current study. The investigators reported having no financial disclosures.
On Twitter @sherryboschert
SAN DIEGO – Eleven of every 100,000 patients younger than 50 years who were seen for traumatic injury developed an ischemic stroke within 4 weeks, a study of data on 1.3 million people found.
Patients with head or neck trauma were three times more likely overall to have a stroke than were those who had other forms of trauma, although the risk varied by age, Dr. Heather Fullerton said in a press briefing at the International Stroke Conference, sponsored by the American Heart Association. Among those with head or neck trauma, ischemic strokes occurred in 0.01% of the children and in 0.05% of the adults within a month of being seen.
Rates in both those age groups were significantly higher than rates reported in the literature for similar ages in the general population, she added.
"Strokes are something that affect young people, not just older people, particularly after a traumatic event," the findings showed, so people should apply the FAST criteria for recognizing the warning signs of stroke to potential stroke victims of any age, Dr. Fullerton said. The FAST acronym refers to the face (does the smile droop?), the arms (if arms are raised, does one drift downward?), speech (slurred or strange?), and time (get emergency help if these signs are present).
"People should seek emergency care for those symptoms regardless of their age, but especially if they happen to have a recent traumatic event," said Dr. Fullerton, professor of neurology at the University of California, San Francisco, and director of the pediatric stroke and cerebrovascular disease center there. Emergency departments see more than 2 million people under age 50 every month for nonfatal traumatic injuries in the United States.
The investigators analyzed data on patients aged 50 years or younger who were insured by Kaiser Permanente and seen in emergency departments or admitted for trauma at either Kaiser or non-Kaiser hospitals in 1997-2011. A neurologist reviewed the records and excluded cases inconsistent with ischemic stroke.
Combining the findings with other national data, she estimated that 214 people younger than 50 years develop an ischemic stroke after a traumatic injury every month in the United States.
Among patients with head or neck trauma, 48 of every 100,000 adults in the study developed a stroke within a month, compared with stroke rates in the general population of young adults of approximately 10/100,000 adults per year, not per month, she said.
In children with head or neck trauma, 11/100,000 in the study developed stroke within a month, compared with general population rates of approximately 2.5 strokes per 100,000 children per year, not per month. Previous research by Dr. Fullerton and her associates suggests that the highest risk in children is within the first week after trauma, she added.
Trauma can tear blood vessels that lead to the brain and cause blood clots resulting in ischemic stroke. Ten percent of patients in the study who developed a stroke were diagnosed with tears in blood vessels leading to the brain, but some of these arterial dissections were diagnosed after the stroke occurred. Most of the strokes in the study probably were due to arterial dissection but were possibly mild enough that an obvious tear didn’t show up on imaging, Dr. Fullerton suggested.
The researchers next are planning a nested case-control study to help identify trauma patients at the highest risk of stroke and to examine the possibilities for stroke prevention.
The American Heart Association funded the current study. The investigators reported having no financial disclosures.
On Twitter @sherryboschert
AT THE INTERNATIONAL STROKE CONFERENCE
Major finding: Eleven of every 100,000 patients developed a stroke within 4 weeks of traumatic injury.
Data source: A retrospective analysis of data on 1.3 million Kaiser patients younger than 50 years who were seen in emergency departments or hospitals for trauma in 1997-2011.
Disclosures: The American Heart Association funded the study. The investigators reported having no financial disclosures.

Magnesium for stroke failed but fast treatment feasible
SAN DIEGO – Having paramedics give intravenous magnesium to patients with acute stroke in the ambulance did not improve stroke-related disability 3 months later in a randomized, double-blind, placebo controlled trial of 1,700 patients.
Patients in both the magnesium and placebo groups had an average modified Rankin Scale score of 2.7, indicating slight to moderate levels of disability at 3 months.
But the negative results were balanced by the demonstration that stroke patients can receive potentially neuroprotective agents in the field, before arrival at a hospital, said Dr. Jeffrey L. Saver. The median time to treatment was 45 minutes after symptom onset and 74% of patients started treatment within an hour of symptoms, the "golden hour" when treatment may produce the best odds of survival and lowest odds of long-term neurological damage, he said at the International Stroke Conference. Another 25% of patients were treated within 1-2 hours of initial symptoms.

Already plans are underway to test other investigational therapies in the field, as researchers are encouraged by these results from the Field Administration of Stroke Therapy – Magnesium (FAST-MAG) trial, he said.
In a Danish trial, investigators are studying prehospital remote ischemic perconditioning for stroke patients. British and U.S. researchers are giving glyceryl trinitrate in the ambulance. Canadian researchers soon will start testing in-ambulance administration of NA-1, another potentially neuroprotective drug, said Dr. Saver, professor of neurology and director of the stroke center at the University of California, Los Angeles.
"We know that every minute that goes by without treatment, 2 million nerve cells are lost" after a stroke, he said at a press briefing.
The only approved treatment for strokes caused by clots is tissue plasminogen activator (TPA), which can’t be administered in ambulances because imaging studies are needed first to confirm a clot and avoid potentially harming patients with hemorrhagic stroke by giving them TPA.
The FAST-MAG study coordinated 315 ambulances, 40 emergency medical service agencies, 60 hospitals, and 2,988 paramedics in two California counties to evaluate 1,700 stroke patients in the field in 2005-2012 and begin IV treatment within 2 hours of symptom onset.
Patients aged 40-95 years with a likely stroke as identified by the Los Angeles Prehospital Stroke Screen received magnesium sulfate or matched saline placebo in the ambulance in a loading dose of 4 g over 15 minutes if they were within 2 hours of symptom onset and had neurological deficits present for 15 minutes or longer. When they arrived at the hospital, they received a maintenance infusion of 16 g magnesium or placebo over 24 hours.
"These were fairly severe stroke patients," with a mean pretreatment stroke severity score of 4 on the Los Angeles Motor Scale, which is roughly equivalent to a 13 on the National Institutes of Health Stroke Scale (NIHSS), he said at the conference, sponsored by the American Heart Association. They had a mean NIHSS score of 11 on arrival at emergency departments. The time from intake on the scene to the hospital door averaged 33 minutes, faster than an average 35 minutes in Los Angeles in prior data.
The final diagnoses included cerebral ischemia in 73% of patients, intracranial hemorrhage in 23%, and stroke mimics in 4%.
In six previous trials of neuroprotective agents in 5,345 patients, times from enrollment to treatment average longer than 3 hours in 92% of patients, 2-3 hours in 6%, 1-2 hours in 1%, and 0-1 hours in only 0.2% of patients, Dr. Saver said. (Percentages don’t equal 100% because of rounding.)
Overall rates of serious adverse events did not differ significantly between groups in the current study. The magnesium group had significantly higher rates of any respiratory complications (8% vs. 5%), hypotension (7% vs. 4%), and dyspnea or respiratory distress (4% vs. 2%), and a lower rate of neoplasms (1% vs. 2%), compared with the placebo group.
Previous animal studies found that IV magnesium dilated brain blood vessels and increased blood flow, and previous small trials in humans showed no overall harm or benefit but provided hints that magnesium might help if administered with a few hours of a stroke.
Dr. Saver reported having no financial disclosures. The trial was partly supported by the National Institute of Neurological Disorders and Stroke.
On Twitter @sherryboschert
SAN DIEGO – Having paramedics give intravenous magnesium to patients with acute stroke in the ambulance did not improve stroke-related disability 3 months later in a randomized, double-blind, placebo controlled trial of 1,700 patients.
Patients in both the magnesium and placebo groups had an average modified Rankin Scale score of 2.7, indicating slight to moderate levels of disability at 3 months.
But the negative results were balanced by the demonstration that stroke patients can receive potentially neuroprotective agents in the field, before arrival at a hospital, said Dr. Jeffrey L. Saver. The median time to treatment was 45 minutes after symptom onset and 74% of patients started treatment within an hour of symptoms, the "golden hour" when treatment may produce the best odds of survival and lowest odds of long-term neurological damage, he said at the International Stroke Conference. Another 25% of patients were treated within 1-2 hours of initial symptoms.
Already plans are underway to test other investigational therapies in the field, as researchers are encouraged by these results from the Field Administration of Stroke Therapy – Magnesium (FAST-MAG) trial, he said.
In a Danish trial, investigators are studying prehospital remote ischemic perconditioning for stroke patients. British and U.S. researchers are giving glyceryl trinitrate in the ambulance. Canadian researchers soon will start testing in-ambulance administration of NA-1, another potentially neuroprotective drug, said Dr. Saver, professor of neurology and director of the stroke center at the University of California, Los Angeles.
"We know that every minute that goes by without treatment, 2 million nerve cells are lost" after a stroke, he said at a press briefing.
The only approved treatment for strokes caused by clots is tissue plasminogen activator (TPA), which can’t be administered in ambulances because imaging studies are needed first to confirm a clot and avoid potentially harming patients with hemorrhagic stroke by giving them TPA.
The FAST-MAG study coordinated 315 ambulances, 40 emergency medical service agencies, 60 hospitals, and 2,988 paramedics in two California counties to evaluate 1,700 stroke patients in the field in 2005-2012 and begin IV treatment within 2 hours of symptom onset.
Patients aged 40-95 years with a likely stroke as identified by the Los Angeles Prehospital Stroke Screen received magnesium sulfate or matched saline placebo in the ambulance in a loading dose of 4 g over 15 minutes if they were within 2 hours of symptom onset and had neurological deficits present for 15 minutes or longer. When they arrived at the hospital, they received a maintenance infusion of 16 g magnesium or placebo over 24 hours.
"These were fairly severe stroke patients," with a mean pretreatment stroke severity score of 4 on the Los Angeles Motor Scale, which is roughly equivalent to a 13 on the National Institutes of Health Stroke Scale (NIHSS), he said at the conference, sponsored by the American Heart Association. They had a mean NIHSS score of 11 on arrival at emergency departments. The time from intake on the scene to the hospital door averaged 33 minutes, faster than an average 35 minutes in Los Angeles in prior data.
The final diagnoses included cerebral ischemia in 73% of patients, intracranial hemorrhage in 23%, and stroke mimics in 4%.
In six previous trials of neuroprotective agents in 5,345 patients, times from enrollment to treatment average longer than 3 hours in 92% of patients, 2-3 hours in 6%, 1-2 hours in 1%, and 0-1 hours in only 0.2% of patients, Dr. Saver said. (Percentages don’t equal 100% because of rounding.)
Overall rates of serious adverse events did not differ significantly between groups in the current study. The magnesium group had significantly higher rates of any respiratory complications (8% vs. 5%), hypotension (7% vs. 4%), and dyspnea or respiratory distress (4% vs. 2%), and a lower rate of neoplasms (1% vs. 2%), compared with the placebo group.
Previous animal studies found that IV magnesium dilated brain blood vessels and increased blood flow, and previous small trials in humans showed no overall harm or benefit but provided hints that magnesium might help if administered with a few hours of a stroke.
Dr. Saver reported having no financial disclosures. The trial was partly supported by the National Institute of Neurological Disorders and Stroke.
On Twitter @sherryboschert
SAN DIEGO – Having paramedics give intravenous magnesium to patients with acute stroke in the ambulance did not improve stroke-related disability 3 months later in a randomized, double-blind, placebo controlled trial of 1,700 patients.
Patients in both the magnesium and placebo groups had an average modified Rankin Scale score of 2.7, indicating slight to moderate levels of disability at 3 months.
But the negative results were balanced by the demonstration that stroke patients can receive potentially neuroprotective agents in the field, before arrival at a hospital, said Dr. Jeffrey L. Saver. The median time to treatment was 45 minutes after symptom onset and 74% of patients started treatment within an hour of symptoms, the "golden hour" when treatment may produce the best odds of survival and lowest odds of long-term neurological damage, he said at the International Stroke Conference. Another 25% of patients were treated within 1-2 hours of initial symptoms.
Already plans are underway to test other investigational therapies in the field, as researchers are encouraged by these results from the Field Administration of Stroke Therapy – Magnesium (FAST-MAG) trial, he said.
In a Danish trial, investigators are studying prehospital remote ischemic perconditioning for stroke patients. British and U.S. researchers are giving glyceryl trinitrate in the ambulance. Canadian researchers soon will start testing in-ambulance administration of NA-1, another potentially neuroprotective drug, said Dr. Saver, professor of neurology and director of the stroke center at the University of California, Los Angeles.
"We know that every minute that goes by without treatment, 2 million nerve cells are lost" after a stroke, he said at a press briefing.
The only approved treatment for strokes caused by clots is tissue plasminogen activator (TPA), which can’t be administered in ambulances because imaging studies are needed first to confirm a clot and avoid potentially harming patients with hemorrhagic stroke by giving them TPA.
The FAST-MAG study coordinated 315 ambulances, 40 emergency medical service agencies, 60 hospitals, and 2,988 paramedics in two California counties to evaluate 1,700 stroke patients in the field in 2005-2012 and begin IV treatment within 2 hours of symptom onset.
Patients aged 40-95 years with a likely stroke as identified by the Los Angeles Prehospital Stroke Screen received magnesium sulfate or matched saline placebo in the ambulance in a loading dose of 4 g over 15 minutes if they were within 2 hours of symptom onset and had neurological deficits present for 15 minutes or longer. When they arrived at the hospital, they received a maintenance infusion of 16 g magnesium or placebo over 24 hours.
"These were fairly severe stroke patients," with a mean pretreatment stroke severity score of 4 on the Los Angeles Motor Scale, which is roughly equivalent to a 13 on the National Institutes of Health Stroke Scale (NIHSS), he said at the conference, sponsored by the American Heart Association. They had a mean NIHSS score of 11 on arrival at emergency departments. The time from intake on the scene to the hospital door averaged 33 minutes, faster than an average 35 minutes in Los Angeles in prior data.
The final diagnoses included cerebral ischemia in 73% of patients, intracranial hemorrhage in 23%, and stroke mimics in 4%.
In six previous trials of neuroprotective agents in 5,345 patients, times from enrollment to treatment average longer than 3 hours in 92% of patients, 2-3 hours in 6%, 1-2 hours in 1%, and 0-1 hours in only 0.2% of patients, Dr. Saver said. (Percentages don’t equal 100% because of rounding.)
Overall rates of serious adverse events did not differ significantly between groups in the current study. The magnesium group had significantly higher rates of any respiratory complications (8% vs. 5%), hypotension (7% vs. 4%), and dyspnea or respiratory distress (4% vs. 2%), and a lower rate of neoplasms (1% vs. 2%), compared with the placebo group.
Previous animal studies found that IV magnesium dilated brain blood vessels and increased blood flow, and previous small trials in humans showed no overall harm or benefit but provided hints that magnesium might help if administered with a few hours of a stroke.
Dr. Saver reported having no financial disclosures. The trial was partly supported by the National Institute of Neurological Disorders and Stroke.
On Twitter @sherryboschert
AT THE INTERNATIONAL STROKE CONFERENCE
Major finding: Median time from stroke symptom onset to treatment was 45 minutes and 74% of patients started treatment within 1 hour, but disability scores at 3 months did not differ significantly between magnesium and placebo groups.
Data source: A multicenter, randomized, double-blind, placebo-controlled trial of IV magnesium or placebo given in the ambulance to 1,700 patients with a likely stroke.
Disclosures: Dr. Saver reported having no financial disclosures. The trial was partly supported by the National Institute of Neurological Disorders and Stroke.

Palliative care is not just for the dying
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.

Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
On Twitter @sherryboschert
 |
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.
Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.
Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
On Twitter @sherryboschert
EXPERT ANALYSIS FROM THE CRITICAL CARE CONGRESS

Palliative care is not just for the dying
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.

Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
If you’re interested in more about these topics, you can join a discussion on this topic within the Critical Care e-Community. Simply log in to ecommunity.chestnet.org and find the Critical Care group. If you’re not part of the Critical Care NetWork, log in to chestnet.org and add the Critical Care NetWork to your profile.
Questions? Contact communityadmin@chestnet.org.
On Twitter @sherryboschert
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
|
| Dr. Geoffrey P. Dunn |
This is an excellent perspective on the ongoing assimilation of palliative care principles and practices into the venue where it is most needed. Dr. Cooper, who is board certified in hospice and palliative medicine in addition to her surgical certification, is eminently qualified to speak to this topic. She represents a new generation of surgeons who see the potential for palliative care principles and practices for all seriously ill surgical patients.
She is right in suggesting we understand palliative care as a way of caring, not a prognostic indicator. As far back as 1999, intensivist and pulmonologist Judith Nelson argued in a memorable editorial in Annals of Internal Medicine that we should not try to pick and choose who needs palliative care in the ICU setting because prognosis is so hard to determine, but rather meet the comfort and quality of life needs of all ICU patients and their families.
Geoffrey P. Dunn, M.D., an ACS Fellow based in Erie, Pa., is chair of the ACS Surgical Palliative Care Task Force.
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.
Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
If you’re interested in more about these topics, you can join a discussion on this topic within the Critical Care e-Community. Simply log in to ecommunity.chestnet.org and find the Critical Care group. If you’re not part of the Critical Care NetWork, log in to chestnet.org and add the Critical Care NetWork to your profile.
Questions? Contact communityadmin@chestnet.org.
On Twitter @sherryboschert
SAN FRANCISCO – Palliative care is not just for the dying.
Understanding that premise is the first step to integrating palliative care into intensive care units, Dr. Zara Cooper said. Palliative care treats patient illness and can be delivered concurrently in the ICU with curative care that treats disease.
As options for curative treatment decrease, the role of palliative care may increase and does not stop at the patient’s death. "It’s important that we provide ongoing bereavement support not only to family members and survivors but also to caregivers and members of our medical team," added Dr. Cooper, an assistant professor of surgery at Harvard Medical School and a surgical intensivist at Brigham and Women’s Hospital, Boston.
Getting intensive care colleagues to agree on a definition of palliative care is the first barrier to integrating palliative care into an ICU, Dr. Cooper said. She paraphrased the World Health Organization’s definition by saying, "Palliative care makes patients feel better." It is specialized medical care that focuses on preventing and relieving symptoms, pain, and stress associated with life-threatening illness – whatever the diagnosis – and is appropriate at any stage in a serious illness.
Typically provided by a team, palliative care may involve physicians, nurses, social workers, pharmacists, chaplains, pain experts, ethicists, rehabilitation therapists, psychiatry consultants, and bereavement counselors. The team can take a load off busy intensivists by handling the often lengthy conversations with patients and families facing life-threatening illness, she said at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Palliative care providers can be embedded in ICUs or in a team that’s available as consultants. "I think we have to do both" models, depending on the needs of individual institutions, said Dr. Cooper.
Once a definition is agreed upon, the next steps to convincing colleagues and administrators to make better use of palliative care are to make it relevant for them and to normalize its presence in the ICU, she said. "Palliative care is just as essential as med management, antibiotics, pharmacology – it’s part of what we do well."
Predicting which patients will die, and when, is difficult. Patient preferences for care or end-of-life treatment often are unclear. The goals of treatment depend on the patient’s condition and must be dynamic. "Is it end-of-life care if we don’t know the patient is dying?" she asked.
One way to consider which ICU patients might benefit from palliative care is to ask, "Would I be surprised if this patient died within a year?" even if discharged from the ICU or the hospital, she suggested.
Four studies in the medical literature separately reported that 20% of Americans die in the hospital after an ICU admission, 80% of deaths in ICUs occur after life support is withdrawn or withheld, nearly half of dying patients receive unwanted therapy, and a majority of dying patients experience pain and suffering, Dr. Cooper said. Five other studies reported high mortality rates in patients with sepsis, acute respiratory distress syndrome, ICU stays longer than 14 days, admission to long-term acute care, or initiation of dialysis in the elderly.
A recent study of 25,558 elderly patients undergoing emergency surgery reported 30-day mortality rates of 37% in those with preexisting do-not-resuscitate (DNR) orders and 22% in those without DNR orders. Major complications occurred in more than 40% in each group (Ann. Surg. 2012;256:453-61). Risk factors increase the likelihood of death, but "all of these patients are experiencing serious illness" and would benefit from palliative care, Dr. Cooper said.
One recent study of 518 patients in three ICUs found good adherence to only two of nine palliative care processes – pain assessment and management. Interdisciplinary family meetings had been held by day 5 in the ICU for less than 20% of patients, and adherence to six other palliative care practices ranged from 8% to 43% (Crit. Care Med. 2012;40:1105-12).
Normalizing palliative care in the ICU means adopting the attitude that "it’s just part of what we do, the same way that we manage our vents, etc." Dr. Cooper said.
Adopting proactive screening criteria (patient factors) that trigger palliative care consultations would reduce utilization of ICUs without increasing mortality, and would increase the availability of palliative care for patients and families, according to a recent report from the Improving Palliative Care in the ICU Project’s advisory board (Crit. Care Med. 2013;41:2318-27).
The triggers should be specific to each ICU and patient population and developed through a process with stakeholders, with outcomes evaluated. "This is not a one-size-fits-all strategy," Dr. Cooper said. "The triggers in the MICU [medical ICU] and the SICU [surgical ICU] cannot be the same. It won’t work. I’ve actually seen that in my own institution," Dr. Cooper said.
The triggers also shouldn’t focus only on the patients most obviously likely to die or they will perpetuate the misconception that palliative care is only for the dying, she added.
To integrate palliative care into an ICU, "just do it," she said. "Commit yourself" to intensive symptom management and multidisciplinary family meetings within 72 hours of ICU admission. Institute an intensive communication plan to provide emotional, educational, and decision support for patients and families. Offer pastoral and psychosocial support. Start end-of-life-care discussions sooner, and provide bereavement services when patients die.
Lastly, don’t hesitate to bill insurers for these services, Dr. Cooper said. In-person or phone meetings about treatment options when the patient lacks the capacity to decide can be billed as critical care, as can discussions about DNR codes. Also bill for treating acute pain, agitation, delirium, and other life-threatening symptoms as critical care.
Dr. Cooper reported having no financial disclosures.
If you’re interested in more about these topics, you can join a discussion on this topic within the Critical Care e-Community. Simply log in to ecommunity.chestnet.org and find the Critical Care group. If you’re not part of the Critical Care NetWork, log in to chestnet.org and add the Critical Care NetWork to your profile.
Questions? Contact communityadmin@chestnet.org.
On Twitter @sherryboschert
EXPERT ANALYSIS FROM THE CRITICAL CARE CONGRESS

'Target: Stroke' program gets most patients timely treatment
SAN DIEGO – The percentage of patients arriving at hospitals with ischemic stroke who were treated with tissue plasminogen activator within the recommended 60 minutes increased from 30% to 53% on average at 1,030 hospitals engaged in the Target: Stroke program in the past 4 years.
Average time from arrival to treatment showed a significant decrease of 15 minutes, from 74 to 59 minutes. Clinical outcomes confirmed Target: Stroke’s motto that "time lost is brain lost," showing significant improvements in rates of death, symptomatic intracerebral hemorrhage, and the likelihood of being discharged home, Dr. Gregg C. Fonarow and his associates reported at the International Stroke Conference.

The study analyzed data on 71,169 patients seen for ischemic stroke at U.S. hospitals that implemented the Target: Stroke program, comparing practices and outcomes before the program launched (2003-2009) with data from after program implementation (2010-2013) and adjusting the results for patient and hospital characteristics.
Average in-hospital mortality decreased from 10% in 27,319 patients seen before Target: Stroke to 8% in the 43,850 seen after the start of the program. The proportion of patients discharged home increased from 38% to 43%, rates of symptomatic intracranial hemorrhage decreased from 6% to 5%, and complications from tissue plasminogen activator (TPA) treatment decreased from 7% to 6%, said Dr. Fonarow, chair of cardiovascular medicine and science at the University of California, Los Angeles.
After adjusting for the effects of multiple other factors, the risk of dying in the hospital decreased 11%, the risk of symptomatic intracerebral hemorrhage or TPA complications each decreased 17%, and the odds of being discharged to home increased 14%, all highly statistically significant and clinically significant outcomes, he said.
These gains were seen in secondary analyses in all subgroups, including men and women, patients older or younger than the median age of 72 years, patients with lesser or greater stroke severity, and patients of different races and ethnicities, he said at the meeting, which was sponsored by the American Heart Association (AHA).
Target: Stroke is a nationwide quality-improvement initiative launched by the AHA and the American Stroke Association (ASA) in 2010 that identified 10 evidence-based strategies that are associated with timely stroke reperfusion and are feasible for hospitals to implement rapidly and cost effectively, Dr. Fonarow said.
The project also supplied clinical decision support tools, performance feedback, and other tools to help hospitals reduce door-to-needle times to less than an hour for most ischemic stroke patients. He and his colleagues described the design and rationale of the initiative in an earlier article (Stroke 2011;42:2983-9).
Only 16% of U.S. hospitals had door-to-needle times of 60 minutes or less in 2009, right before Target: Stroke launched. By 2013, that proportion "increased markedly" to 47% of participating hospitals meeting this benchmark, he said. In 4 years, the project achieved its goal of having at least half of ischemic stroke patients get TPA within an hour of arrival, which would have taken 15 or more years if rates of progress before Target: Stroke had persisted.
The AHA/ASA set a new target for phase II of Target: Stroke, which was launched at the meeting: Reducing door-to-needle times to less than an hour for at least 75% of ischemic stroke patients at participating hospitals.
The current study controlled for the effects of age, sex, race, history of atrial fibrillation, prosthetic heart valve, previous stroke or transient ischemic attack, coronary heart disease or prior MI, carotid stenosis, peripheral vascular disease, hypertension, dyslipidemia, current smoking, stroke severity, arrival time and mode, onset-to-arrival time, hospital size, region, annual volume of TPA, annual stroke discharge, and whether the facility was a teaching hospital or a certified stroke center.
Dr. Fonarow said that it was not feasible to include a true control group of hospitals that did not join the program because the lack of participation in nationwide quality improvement programs makes it difficult to gather data from those facilities.
He and his associates previously reported that, before Target: Stroke, most U.S. stroke patients were not receiving TPA within an hour of arrival at a hospital (Circulation 2011;123:750-8).
Dr. Fonarow and one of his associates in the study are employees of the University of California, which holds a patent on retriever devices for treating acute stroke. Five of his coauthors reported financial associations with multiple companies, some of which make treatments and devices for stroke.
On Twitter @sherryboschert
This is enormously exciting. It shows that all these efforts to improve treatment time, the door-to-needle time, have a payoff. The patients did better. It shows that these interventions matter.
What strikes me is that there’s no single magic intervention. There’s no high technology or amazing breakthroughs. It’s just by making every step in the process a little bit better.
 |
| Dr. Steven Greenberg |
Another message is that you can always get better. You’re never done.
This will be an ongoing effort. I don’t think you’ll see any single breakthrough but hope you’ll see small improvements and small improvements, but ones that really impact people’s lives.
Dr. Steven Greenberg, professor of neurology at Harvard Medical School in Boston, was chairman of the International Stroke Conference Program Committee. He was not involved in creating or studying Target: Stroke and reported no relevant disclosures.
This is enormously exciting. It shows that all these efforts to improve treatment time, the door-to-needle time, have a payoff. The patients did better. It shows that these interventions matter.
What strikes me is that there’s no single magic intervention. There’s no high technology or amazing breakthroughs. It’s just by making every step in the process a little bit better.
|
| Dr. Steven Greenberg |
Another message is that you can always get better. You’re never done.
This will be an ongoing effort. I don’t think you’ll see any single breakthrough but hope you’ll see small improvements and small improvements, but ones that really impact people’s lives.
Dr. Steven Greenberg, professor of neurology at Harvard Medical School in Boston, was chairman of the International Stroke Conference Program Committee. He was not involved in creating or studying Target: Stroke and reported no relevant disclosures.
This is enormously exciting. It shows that all these efforts to improve treatment time, the door-to-needle time, have a payoff. The patients did better. It shows that these interventions matter.
What strikes me is that there’s no single magic intervention. There’s no high technology or amazing breakthroughs. It’s just by making every step in the process a little bit better.
|
| Dr. Steven Greenberg |
Another message is that you can always get better. You’re never done.
This will be an ongoing effort. I don’t think you’ll see any single breakthrough but hope you’ll see small improvements and small improvements, but ones that really impact people’s lives.
Dr. Steven Greenberg, professor of neurology at Harvard Medical School in Boston, was chairman of the International Stroke Conference Program Committee. He was not involved in creating or studying Target: Stroke and reported no relevant disclosures.
SAN DIEGO – The percentage of patients arriving at hospitals with ischemic stroke who were treated with tissue plasminogen activator within the recommended 60 minutes increased from 30% to 53% on average at 1,030 hospitals engaged in the Target: Stroke program in the past 4 years.
Average time from arrival to treatment showed a significant decrease of 15 minutes, from 74 to 59 minutes. Clinical outcomes confirmed Target: Stroke’s motto that "time lost is brain lost," showing significant improvements in rates of death, symptomatic intracerebral hemorrhage, and the likelihood of being discharged home, Dr. Gregg C. Fonarow and his associates reported at the International Stroke Conference.
The study analyzed data on 71,169 patients seen for ischemic stroke at U.S. hospitals that implemented the Target: Stroke program, comparing practices and outcomes before the program launched (2003-2009) with data from after program implementation (2010-2013) and adjusting the results for patient and hospital characteristics.
Average in-hospital mortality decreased from 10% in 27,319 patients seen before Target: Stroke to 8% in the 43,850 seen after the start of the program. The proportion of patients discharged home increased from 38% to 43%, rates of symptomatic intracranial hemorrhage decreased from 6% to 5%, and complications from tissue plasminogen activator (TPA) treatment decreased from 7% to 6%, said Dr. Fonarow, chair of cardiovascular medicine and science at the University of California, Los Angeles.
After adjusting for the effects of multiple other factors, the risk of dying in the hospital decreased 11%, the risk of symptomatic intracerebral hemorrhage or TPA complications each decreased 17%, and the odds of being discharged to home increased 14%, all highly statistically significant and clinically significant outcomes, he said.
These gains were seen in secondary analyses in all subgroups, including men and women, patients older or younger than the median age of 72 years, patients with lesser or greater stroke severity, and patients of different races and ethnicities, he said at the meeting, which was sponsored by the American Heart Association (AHA).
Target: Stroke is a nationwide quality-improvement initiative launched by the AHA and the American Stroke Association (ASA) in 2010 that identified 10 evidence-based strategies that are associated with timely stroke reperfusion and are feasible for hospitals to implement rapidly and cost effectively, Dr. Fonarow said.
The project also supplied clinical decision support tools, performance feedback, and other tools to help hospitals reduce door-to-needle times to less than an hour for most ischemic stroke patients. He and his colleagues described the design and rationale of the initiative in an earlier article (Stroke 2011;42:2983-9).
Only 16% of U.S. hospitals had door-to-needle times of 60 minutes or less in 2009, right before Target: Stroke launched. By 2013, that proportion "increased markedly" to 47% of participating hospitals meeting this benchmark, he said. In 4 years, the project achieved its goal of having at least half of ischemic stroke patients get TPA within an hour of arrival, which would have taken 15 or more years if rates of progress before Target: Stroke had persisted.
The AHA/ASA set a new target for phase II of Target: Stroke, which was launched at the meeting: Reducing door-to-needle times to less than an hour for at least 75% of ischemic stroke patients at participating hospitals.
The current study controlled for the effects of age, sex, race, history of atrial fibrillation, prosthetic heart valve, previous stroke or transient ischemic attack, coronary heart disease or prior MI, carotid stenosis, peripheral vascular disease, hypertension, dyslipidemia, current smoking, stroke severity, arrival time and mode, onset-to-arrival time, hospital size, region, annual volume of TPA, annual stroke discharge, and whether the facility was a teaching hospital or a certified stroke center.
Dr. Fonarow said that it was not feasible to include a true control group of hospitals that did not join the program because the lack of participation in nationwide quality improvement programs makes it difficult to gather data from those facilities.
He and his associates previously reported that, before Target: Stroke, most U.S. stroke patients were not receiving TPA within an hour of arrival at a hospital (Circulation 2011;123:750-8).
Dr. Fonarow and one of his associates in the study are employees of the University of California, which holds a patent on retriever devices for treating acute stroke. Five of his coauthors reported financial associations with multiple companies, some of which make treatments and devices for stroke.
On Twitter @sherryboschert
SAN DIEGO – The percentage of patients arriving at hospitals with ischemic stroke who were treated with tissue plasminogen activator within the recommended 60 minutes increased from 30% to 53% on average at 1,030 hospitals engaged in the Target: Stroke program in the past 4 years.
Average time from arrival to treatment showed a significant decrease of 15 minutes, from 74 to 59 minutes. Clinical outcomes confirmed Target: Stroke’s motto that "time lost is brain lost," showing significant improvements in rates of death, symptomatic intracerebral hemorrhage, and the likelihood of being discharged home, Dr. Gregg C. Fonarow and his associates reported at the International Stroke Conference.
The study analyzed data on 71,169 patients seen for ischemic stroke at U.S. hospitals that implemented the Target: Stroke program, comparing practices and outcomes before the program launched (2003-2009) with data from after program implementation (2010-2013) and adjusting the results for patient and hospital characteristics.
Average in-hospital mortality decreased from 10% in 27,319 patients seen before Target: Stroke to 8% in the 43,850 seen after the start of the program. The proportion of patients discharged home increased from 38% to 43%, rates of symptomatic intracranial hemorrhage decreased from 6% to 5%, and complications from tissue plasminogen activator (TPA) treatment decreased from 7% to 6%, said Dr. Fonarow, chair of cardiovascular medicine and science at the University of California, Los Angeles.
After adjusting for the effects of multiple other factors, the risk of dying in the hospital decreased 11%, the risk of symptomatic intracerebral hemorrhage or TPA complications each decreased 17%, and the odds of being discharged to home increased 14%, all highly statistically significant and clinically significant outcomes, he said.
These gains were seen in secondary analyses in all subgroups, including men and women, patients older or younger than the median age of 72 years, patients with lesser or greater stroke severity, and patients of different races and ethnicities, he said at the meeting, which was sponsored by the American Heart Association (AHA).
Target: Stroke is a nationwide quality-improvement initiative launched by the AHA and the American Stroke Association (ASA) in 2010 that identified 10 evidence-based strategies that are associated with timely stroke reperfusion and are feasible for hospitals to implement rapidly and cost effectively, Dr. Fonarow said.
The project also supplied clinical decision support tools, performance feedback, and other tools to help hospitals reduce door-to-needle times to less than an hour for most ischemic stroke patients. He and his colleagues described the design and rationale of the initiative in an earlier article (Stroke 2011;42:2983-9).
Only 16% of U.S. hospitals had door-to-needle times of 60 minutes or less in 2009, right before Target: Stroke launched. By 2013, that proportion "increased markedly" to 47% of participating hospitals meeting this benchmark, he said. In 4 years, the project achieved its goal of having at least half of ischemic stroke patients get TPA within an hour of arrival, which would have taken 15 or more years if rates of progress before Target: Stroke had persisted.
The AHA/ASA set a new target for phase II of Target: Stroke, which was launched at the meeting: Reducing door-to-needle times to less than an hour for at least 75% of ischemic stroke patients at participating hospitals.
The current study controlled for the effects of age, sex, race, history of atrial fibrillation, prosthetic heart valve, previous stroke or transient ischemic attack, coronary heart disease or prior MI, carotid stenosis, peripheral vascular disease, hypertension, dyslipidemia, current smoking, stroke severity, arrival time and mode, onset-to-arrival time, hospital size, region, annual volume of TPA, annual stroke discharge, and whether the facility was a teaching hospital or a certified stroke center.
Dr. Fonarow said that it was not feasible to include a true control group of hospitals that did not join the program because the lack of participation in nationwide quality improvement programs makes it difficult to gather data from those facilities.
He and his associates previously reported that, before Target: Stroke, most U.S. stroke patients were not receiving TPA within an hour of arrival at a hospital (Circulation 2011;123:750-8).
Dr. Fonarow and one of his associates in the study are employees of the University of California, which holds a patent on retriever devices for treating acute stroke. Five of his coauthors reported financial associations with multiple companies, some of which make treatments and devices for stroke.
On Twitter @sherryboschert
AT THE INTERNATIONAL STROKE CONFERENCE
Major finding: The percentage of patients with ischemic stroke who got TPA within 1 hour of hospital arrival increased from 30% before Target: Stroke to 53% after implementation.
Data source: An analysis of data on 71,169 stroke patients at 1,030 U.S. hospitals.
Disclosures: Dr. Fonarow and one of his associates in the study are employees of the University of California, which holds a patent on retriever devices for treating acute stroke. Five of his coauthors reported financial associations with multiple companies, some of which make treatments and devices for stroke.

Hypothermia associated with persistent lymphopenia in sepsis
SAN FRANCISCO – Patients with sepsis had significantly higher rates of persistent lymphopenia, 28-day mortality, and 1-year mortality if they were hypothermic, compared with normothermic patients in a small retrospective study.
In the study, 32 of 58 septic patients who were hypothermic within 24 hours of their blood cultures developed persistent lymphopenia (55%), compared with 43% of 183 normothermic patients and 48% of 204 febrile patients.
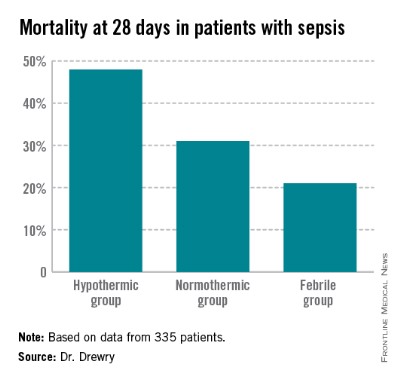
Dr. Anne Drewry reported that hypothermia was associated with a nearly tripled risk for persistent lymphopenia (odds ratio, 2.7) compared with normothermic patients in a multivariate logistic regression analysis to account for confounding variables. The likelihood of persistent lymphopenia in febrile patients was not significantly different from that of normothermic patients.
The significantly higher risk of persistent lymphopenia in patients with hypothermia compared with normothermia was accompanied by significantly higher risk for some secondary adverse outcomes in the observational cohort study, she reported at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Thirty-nine hypothermic patients developed septic shock (67%), compared with 55% of normothermic patients and 47% of febrile patients.
Mortality rates at 28 days were 48% in the hypothermic group (28 patients), 31% in the normothermic group, and 21% in the febrile group (which was significantly lower compared with the normothermic patients). At 1 year, 35 hypothermic patients had died (60%) compared with 45% of normothermic patients and 39% of febrile patients, she said.
"Hypothermic patients may be candidates for early treatment with agents that reverse sepsis-induced lymphopenia in future clinical trials," said Dr. Drewry of Washington University, St. Louis.

She and her associates studied data on 455 patients hospitalized between January 2010 and July 2012 and diagnosed with sepsis, and whose blood cultures were positive for bacterial or fungal organisms within 5 days of admission. They considered patients to be hypothermic if their most extreme temperature values within the first 24 hours of blood cultures were less than 36° C and to be febrile if the temperature values were 38.3° C or higher.
Data on 335 patients were analyzed for the primary outcome of persistent lymphopenia, not counting 110 patients who died or were discharged prior to day 4 after sepsis diagnosis or who had no blood counts drawn on day 4.
Mean APACHE II (Acute Physiology and Chronic Health Evaluation II) scores at baseline were 22 in the hypothermic group, significantly higher than the mean score of 16 in normothermic patients and 17 in febrile patients. Higher APACHE II scores were the only variable besides hypothermia to be significantly associated with increased risk of persistent lymphopenia; higher scores conferred a 7% increase in risk.
Hypothermic patients were significantly more likely to be infected with gram-negative organisms (50%) than were normothermic patients (36%) or febrile patients (34%).
The three groups did not differ significantly in rates of acute kidney injury, secondary infection, or need for mechanical ventilation, among secondary outcomes in a univariate analysis. Factors that were not significantly associated with persistent lymphopenia risk in the multivariable analysis included the presence of comorbidity and the type of organism (gram-positive, gram-negative, fungal, or polymicrobial).
Hypothermia occurs in 10%-25% of critically ill patients with sepsis, Dr. Drewry said. A prior study by other investigators suggested that severely septic patients with hypothermia are older, have more severe disease, and are at higher risk of death than normothermic or febrile patients (Crit. Care 2013;17:R271).
"Previous data from our group suggests that persistent lymphopenia predicts mortality and secondary infection in septic patients and may be a marker for sepsis-induced immunosuppression" even after accounting for possible confounders, Dr. Drewry said.
It’s unclear why some patients don’t mount a fever in response to infection and why these patients have worse outcomes, she added. "Our overarching hypothesis is that hypothermia in response to infection is a sign of an underlying predisposition to sepsis-induced immunosuppression."
The study excluded patients diagnosed with hematological or immunological disease and patients treated with chemotherapy or corticosteroids while hospitalized or within 6 months before admission.
Dr. Drewry reported having no financial disclosures.
sboschert@frontlinemedcom.com On Twitter @sherryboschert
SAN FRANCISCO – Patients with sepsis had significantly higher rates of persistent lymphopenia, 28-day mortality, and 1-year mortality if they were hypothermic, compared with normothermic patients in a small retrospective study.
In the study, 32 of 58 septic patients who were hypothermic within 24 hours of their blood cultures developed persistent lymphopenia (55%), compared with 43% of 183 normothermic patients and 48% of 204 febrile patients.
Dr. Anne Drewry reported that hypothermia was associated with a nearly tripled risk for persistent lymphopenia (odds ratio, 2.7) compared with normothermic patients in a multivariate logistic regression analysis to account for confounding variables. The likelihood of persistent lymphopenia in febrile patients was not significantly different from that of normothermic patients.
The significantly higher risk of persistent lymphopenia in patients with hypothermia compared with normothermia was accompanied by significantly higher risk for some secondary adverse outcomes in the observational cohort study, she reported at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Thirty-nine hypothermic patients developed septic shock (67%), compared with 55% of normothermic patients and 47% of febrile patients.
Mortality rates at 28 days were 48% in the hypothermic group (28 patients), 31% in the normothermic group, and 21% in the febrile group (which was significantly lower compared with the normothermic patients). At 1 year, 35 hypothermic patients had died (60%) compared with 45% of normothermic patients and 39% of febrile patients, she said.
"Hypothermic patients may be candidates for early treatment with agents that reverse sepsis-induced lymphopenia in future clinical trials," said Dr. Drewry of Washington University, St. Louis.
She and her associates studied data on 455 patients hospitalized between January 2010 and July 2012 and diagnosed with sepsis, and whose blood cultures were positive for bacterial or fungal organisms within 5 days of admission. They considered patients to be hypothermic if their most extreme temperature values within the first 24 hours of blood cultures were less than 36° C and to be febrile if the temperature values were 38.3° C or higher.
Data on 335 patients were analyzed for the primary outcome of persistent lymphopenia, not counting 110 patients who died or were discharged prior to day 4 after sepsis diagnosis or who had no blood counts drawn on day 4.
Mean APACHE II (Acute Physiology and Chronic Health Evaluation II) scores at baseline were 22 in the hypothermic group, significantly higher than the mean score of 16 in normothermic patients and 17 in febrile patients. Higher APACHE II scores were the only variable besides hypothermia to be significantly associated with increased risk of persistent lymphopenia; higher scores conferred a 7% increase in risk.
Hypothermic patients were significantly more likely to be infected with gram-negative organisms (50%) than were normothermic patients (36%) or febrile patients (34%).
The three groups did not differ significantly in rates of acute kidney injury, secondary infection, or need for mechanical ventilation, among secondary outcomes in a univariate analysis. Factors that were not significantly associated with persistent lymphopenia risk in the multivariable analysis included the presence of comorbidity and the type of organism (gram-positive, gram-negative, fungal, or polymicrobial).
Hypothermia occurs in 10%-25% of critically ill patients with sepsis, Dr. Drewry said. A prior study by other investigators suggested that severely septic patients with hypothermia are older, have more severe disease, and are at higher risk of death than normothermic or febrile patients (Crit. Care 2013;17:R271).
"Previous data from our group suggests that persistent lymphopenia predicts mortality and secondary infection in septic patients and may be a marker for sepsis-induced immunosuppression" even after accounting for possible confounders, Dr. Drewry said.
It’s unclear why some patients don’t mount a fever in response to infection and why these patients have worse outcomes, she added. "Our overarching hypothesis is that hypothermia in response to infection is a sign of an underlying predisposition to sepsis-induced immunosuppression."
The study excluded patients diagnosed with hematological or immunological disease and patients treated with chemotherapy or corticosteroids while hospitalized or within 6 months before admission.
Dr. Drewry reported having no financial disclosures.
sboschert@frontlinemedcom.com On Twitter @sherryboschert
SAN FRANCISCO – Patients with sepsis had significantly higher rates of persistent lymphopenia, 28-day mortality, and 1-year mortality if they were hypothermic, compared with normothermic patients in a small retrospective study.
In the study, 32 of 58 septic patients who were hypothermic within 24 hours of their blood cultures developed persistent lymphopenia (55%), compared with 43% of 183 normothermic patients and 48% of 204 febrile patients.
Dr. Anne Drewry reported that hypothermia was associated with a nearly tripled risk for persistent lymphopenia (odds ratio, 2.7) compared with normothermic patients in a multivariate logistic regression analysis to account for confounding variables. The likelihood of persistent lymphopenia in febrile patients was not significantly different from that of normothermic patients.
The significantly higher risk of persistent lymphopenia in patients with hypothermia compared with normothermia was accompanied by significantly higher risk for some secondary adverse outcomes in the observational cohort study, she reported at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
Thirty-nine hypothermic patients developed septic shock (67%), compared with 55% of normothermic patients and 47% of febrile patients.
Mortality rates at 28 days were 48% in the hypothermic group (28 patients), 31% in the normothermic group, and 21% in the febrile group (which was significantly lower compared with the normothermic patients). At 1 year, 35 hypothermic patients had died (60%) compared with 45% of normothermic patients and 39% of febrile patients, she said.
"Hypothermic patients may be candidates for early treatment with agents that reverse sepsis-induced lymphopenia in future clinical trials," said Dr. Drewry of Washington University, St. Louis.
She and her associates studied data on 455 patients hospitalized between January 2010 and July 2012 and diagnosed with sepsis, and whose blood cultures were positive for bacterial or fungal organisms within 5 days of admission. They considered patients to be hypothermic if their most extreme temperature values within the first 24 hours of blood cultures were less than 36° C and to be febrile if the temperature values were 38.3° C or higher.
Data on 335 patients were analyzed for the primary outcome of persistent lymphopenia, not counting 110 patients who died or were discharged prior to day 4 after sepsis diagnosis or who had no blood counts drawn on day 4.
Mean APACHE II (Acute Physiology and Chronic Health Evaluation II) scores at baseline were 22 in the hypothermic group, significantly higher than the mean score of 16 in normothermic patients and 17 in febrile patients. Higher APACHE II scores were the only variable besides hypothermia to be significantly associated with increased risk of persistent lymphopenia; higher scores conferred a 7% increase in risk.
Hypothermic patients were significantly more likely to be infected with gram-negative organisms (50%) than were normothermic patients (36%) or febrile patients (34%).
The three groups did not differ significantly in rates of acute kidney injury, secondary infection, or need for mechanical ventilation, among secondary outcomes in a univariate analysis. Factors that were not significantly associated with persistent lymphopenia risk in the multivariable analysis included the presence of comorbidity and the type of organism (gram-positive, gram-negative, fungal, or polymicrobial).
Hypothermia occurs in 10%-25% of critically ill patients with sepsis, Dr. Drewry said. A prior study by other investigators suggested that severely septic patients with hypothermia are older, have more severe disease, and are at higher risk of death than normothermic or febrile patients (Crit. Care 2013;17:R271).
"Previous data from our group suggests that persistent lymphopenia predicts mortality and secondary infection in septic patients and may be a marker for sepsis-induced immunosuppression" even after accounting for possible confounders, Dr. Drewry said.
It’s unclear why some patients don’t mount a fever in response to infection and why these patients have worse outcomes, she added. "Our overarching hypothesis is that hypothermia in response to infection is a sign of an underlying predisposition to sepsis-induced immunosuppression."
The study excluded patients diagnosed with hematological or immunological disease and patients treated with chemotherapy or corticosteroids while hospitalized or within 6 months before admission.
Dr. Drewry reported having no financial disclosures.
sboschert@frontlinemedcom.com On Twitter @sherryboschert
AT THE CRITICAL CARE CONGRESS
Major finding: Persistent lymphopenia occurred in 55% of hypothermic patients, 43% of normothermic, and 48% of febrile patients with sepsis.
Data source: A retrospective, observational cohort study of 455 hospitalized patients diagnosed with sepsis.
Disclosures: Dr. Drewry reported having no financial disclosures.
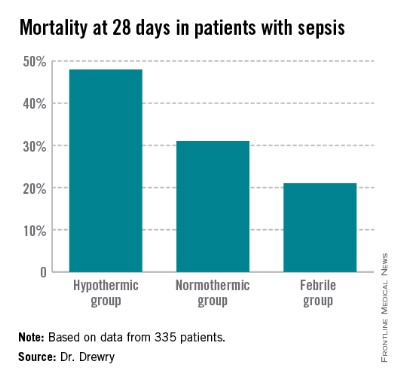
Sepsis resuscitation reduces mortality, even after 6 hours
SAN FRANCISCO – Meeting the goals of the Surviving Sepsis Campaign’s resuscitation care bundle significantly decreased the risk for in-hospital mortality, even when the goals were met beyond the recommended 6-hour window after diagnosis of severe sepsis, a study of 395 patients found.
In-hospital mortality rates were 88% lower in the 85 patients who met the resuscitation bundle goals 6-18 hours after diagnosis and 55% lower in the 95 patients who met the goals within the desired 6 hours after diagnosis compared with 216 patients who did not reach the goals within 18 hours of diagnosis, Dr. Zerihun A. Bunaye reported at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.

For resuscitation care in severe sepsis, it’s better late than never, he said. "Definitely this is showing that there’s a benefit if we continue to aggressively resuscitate the patients beyond 6 hours and try to achieve the goals," said Dr. Bunaye of Mercy Hospital, St. Louis. The lead investigator in the study was Dr. Farid Sadaka, also of the hospital.
Better survival in the group that complied with resuscitation bundle goals in 6-18 hours compared with the 6-hour compliance group surprised the investigators and may be due to several confounding factors that were not analyzed in the study, he said.
The Surviving Sepsis Campaign recommends two sets of "bundles" of care (sets of elements of care selected from evidence-based practice guidelines that have an effect on outcomes when implemented as a group that’s beyond the effect of individual implementation), some to be completed within 3 hours and other goals to be met within 6 hours.
The resuscitation bundle of care aims to prescribe appropriate antibiotics within 3 hours and within 6 hours to get the patient’s mean arterial pressure above 65 mm Hg, get central venous pressure above 8 mm Hg, achieve central venous oxygen saturation greater than 70%, and measure lactic acid, Dr. Bunaye said.
The investigators prospectively collected data as part of a performance improvement project with feedback mechanisms for alerting physicians when bundle goals were not being met so they could continue efforts to meet the goals beyond the recommended deadlines.
The study included patients with septic shock treated between July 2011 and January 2013 in a 54-bed ICU at the large university-affiliated hospital. It compared compliance with the resuscitation bundles within 18 hours of diagnosis and survival rates during approximately 31 days in the hospital.
Compared with the 54% of cases that did not comply with the resuscitation bundles within 18 hours, the hazard ratio for mortality was 0.45 in the 24% of cases that complied within 6 hours and 0.12 in the 22% that complied within 18 hours, Dr. Bunaye reported. Patients in the three groups did not differ significantly at baseline by age, weight, or Sequential Organ Failure Assessment score.
Previous studies have suggested that only 30%-40% of hospitals adhere to the Surviving Sepsis Campaign guidelines. The current study suggests that continuing efforts to meet the goals beyond 6 hours are beneficial, he said.
The findings are limited by the small sample size and the focus on a single institution. The study also did not account for potential confounding variables.
Severe sepsis in the United States is more common than AIDS, colon cancer, and breast cancer combined and is the leading cause of death in noncoronary ICUs, the literature suggests. The United States sees more than 500,000 cases of severe sepsis and septic shock each year, leading to death in 20% of patients with severe sepsis and 45% of those with septic shock, Dr. Bunaye said.
The investigators reported that they have no relevant financial disclosures.
Data suggest better late than never
Dr. Steven Q. Simpson, FCCP, comments: It is very encouraging to see that benefit accrues to patients who meet SSC (and National Quality Forum) bundle goals for physiological parameters, even if they are not met until later in the course of severe sepsis treatment. It seems a bit paradoxical that those who meet physiological goals between 6 and 16 hours after presentation have a higher mortality reduction than those who meet goals within 6 hours. Unfortunately, the study was not set up to determine how or why that may have happened, and whether the phenomenon is real.
The key point, though, is that these are valid goals to work toward in patients with severe sepsis and septic shock, and that we should follow through even when we miss the 6-hour time frame.
On Twitter @sherryboschert
SAN FRANCISCO – Meeting the goals of the Surviving Sepsis Campaign’s resuscitation care bundle significantly decreased the risk for in-hospital mortality, even when the goals were met beyond the recommended 6-hour window after diagnosis of severe sepsis, a study of 395 patients found.
In-hospital mortality rates were 88% lower in the 85 patients who met the resuscitation bundle goals 6-18 hours after diagnosis and 55% lower in the 95 patients who met the goals within the desired 6 hours after diagnosis compared with 216 patients who did not reach the goals within 18 hours of diagnosis, Dr. Zerihun A. Bunaye reported at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
For resuscitation care in severe sepsis, it’s better late than never, he said. "Definitely this is showing that there’s a benefit if we continue to aggressively resuscitate the patients beyond 6 hours and try to achieve the goals," said Dr. Bunaye of Mercy Hospital, St. Louis. The lead investigator in the study was Dr. Farid Sadaka, also of the hospital.
Better survival in the group that complied with resuscitation bundle goals in 6-18 hours compared with the 6-hour compliance group surprised the investigators and may be due to several confounding factors that were not analyzed in the study, he said.
The Surviving Sepsis Campaign recommends two sets of "bundles" of care (sets of elements of care selected from evidence-based practice guidelines that have an effect on outcomes when implemented as a group that’s beyond the effect of individual implementation), some to be completed within 3 hours and other goals to be met within 6 hours.
The resuscitation bundle of care aims to prescribe appropriate antibiotics within 3 hours and within 6 hours to get the patient’s mean arterial pressure above 65 mm Hg, get central venous pressure above 8 mm Hg, achieve central venous oxygen saturation greater than 70%, and measure lactic acid, Dr. Bunaye said.
The investigators prospectively collected data as part of a performance improvement project with feedback mechanisms for alerting physicians when bundle goals were not being met so they could continue efforts to meet the goals beyond the recommended deadlines.
The study included patients with septic shock treated between July 2011 and January 2013 in a 54-bed ICU at the large university-affiliated hospital. It compared compliance with the resuscitation bundles within 18 hours of diagnosis and survival rates during approximately 31 days in the hospital.
Compared with the 54% of cases that did not comply with the resuscitation bundles within 18 hours, the hazard ratio for mortality was 0.45 in the 24% of cases that complied within 6 hours and 0.12 in the 22% that complied within 18 hours, Dr. Bunaye reported. Patients in the three groups did not differ significantly at baseline by age, weight, or Sequential Organ Failure Assessment score.
Previous studies have suggested that only 30%-40% of hospitals adhere to the Surviving Sepsis Campaign guidelines. The current study suggests that continuing efforts to meet the goals beyond 6 hours are beneficial, he said.
The findings are limited by the small sample size and the focus on a single institution. The study also did not account for potential confounding variables.
Severe sepsis in the United States is more common than AIDS, colon cancer, and breast cancer combined and is the leading cause of death in noncoronary ICUs, the literature suggests. The United States sees more than 500,000 cases of severe sepsis and septic shock each year, leading to death in 20% of patients with severe sepsis and 45% of those with septic shock, Dr. Bunaye said.
The investigators reported that they have no relevant financial disclosures.
Data suggest better late than never
Dr. Steven Q. Simpson, FCCP, comments: It is very encouraging to see that benefit accrues to patients who meet SSC (and National Quality Forum) bundle goals for physiological parameters, even if they are not met until later in the course of severe sepsis treatment. It seems a bit paradoxical that those who meet physiological goals between 6 and 16 hours after presentation have a higher mortality reduction than those who meet goals within 6 hours. Unfortunately, the study was not set up to determine how or why that may have happened, and whether the phenomenon is real.
The key point, though, is that these are valid goals to work toward in patients with severe sepsis and septic shock, and that we should follow through even when we miss the 6-hour time frame.
On Twitter @sherryboschert
SAN FRANCISCO – Meeting the goals of the Surviving Sepsis Campaign’s resuscitation care bundle significantly decreased the risk for in-hospital mortality, even when the goals were met beyond the recommended 6-hour window after diagnosis of severe sepsis, a study of 395 patients found.
In-hospital mortality rates were 88% lower in the 85 patients who met the resuscitation bundle goals 6-18 hours after diagnosis and 55% lower in the 95 patients who met the goals within the desired 6 hours after diagnosis compared with 216 patients who did not reach the goals within 18 hours of diagnosis, Dr. Zerihun A. Bunaye reported at the Critical Care Congress, sponsored by the Society for Critical Care Medicine.
For resuscitation care in severe sepsis, it’s better late than never, he said. "Definitely this is showing that there’s a benefit if we continue to aggressively resuscitate the patients beyond 6 hours and try to achieve the goals," said Dr. Bunaye of Mercy Hospital, St. Louis. The lead investigator in the study was Dr. Farid Sadaka, also of the hospital.
Better survival in the group that complied with resuscitation bundle goals in 6-18 hours compared with the 6-hour compliance group surprised the investigators and may be due to several confounding factors that were not analyzed in the study, he said.
The Surviving Sepsis Campaign recommends two sets of "bundles" of care (sets of elements of care selected from evidence-based practice guidelines that have an effect on outcomes when implemented as a group that’s beyond the effect of individual implementation), some to be completed within 3 hours and other goals to be met within 6 hours.
The resuscitation bundle of care aims to prescribe appropriate antibiotics within 3 hours and within 6 hours to get the patient’s mean arterial pressure above 65 mm Hg, get central venous pressure above 8 mm Hg, achieve central venous oxygen saturation greater than 70%, and measure lactic acid, Dr. Bunaye said.
The investigators prospectively collected data as part of a performance improvement project with feedback mechanisms for alerting physicians when bundle goals were not being met so they could continue efforts to meet the goals beyond the recommended deadlines.
The study included patients with septic shock treated between July 2011 and January 2013 in a 54-bed ICU at the large university-affiliated hospital. It compared compliance with the resuscitation bundles within 18 hours of diagnosis and survival rates during approximately 31 days in the hospital.
Compared with the 54% of cases that did not comply with the resuscitation bundles within 18 hours, the hazard ratio for mortality was 0.45 in the 24% of cases that complied within 6 hours and 0.12 in the 22% that complied within 18 hours, Dr. Bunaye reported. Patients in the three groups did not differ significantly at baseline by age, weight, or Sequential Organ Failure Assessment score.
Previous studies have suggested that only 30%-40% of hospitals adhere to the Surviving Sepsis Campaign guidelines. The current study suggests that continuing efforts to meet the goals beyond 6 hours are beneficial, he said.
The findings are limited by the small sample size and the focus on a single institution. The study also did not account for potential confounding variables.
Severe sepsis in the United States is more common than AIDS, colon cancer, and breast cancer combined and is the leading cause of death in noncoronary ICUs, the literature suggests. The United States sees more than 500,000 cases of severe sepsis and septic shock each year, leading to death in 20% of patients with severe sepsis and 45% of those with septic shock, Dr. Bunaye said.
The investigators reported that they have no relevant financial disclosures.
Data suggest better late than never
Dr. Steven Q. Simpson, FCCP, comments: It is very encouraging to see that benefit accrues to patients who meet SSC (and National Quality Forum) bundle goals for physiological parameters, even if they are not met until later in the course of severe sepsis treatment. It seems a bit paradoxical that those who meet physiological goals between 6 and 16 hours after presentation have a higher mortality reduction than those who meet goals within 6 hours. Unfortunately, the study was not set up to determine how or why that may have happened, and whether the phenomenon is real.
The key point, though, is that these are valid goals to work toward in patients with severe sepsis and septic shock, and that we should follow through even when we miss the 6-hour time frame.
On Twitter @sherryboschert
Major finding: The risk for death during hospitalization was 55% lower in patients who met resuscitation bundle goals within 6 hours and 88% lower in patients who met the goals in 6-18 hours compared with those who did not reach the goals within 18 hours.
Data source: An observational study of 395 patients with severe sepsis at a single institution.
Disclosures: Financial disclosures for the investigators were not available at press time.

Ideas, but no easy way to ease intensivist shortage
The shortage of intensivists in the critical care game isn't shrinking. What's the best strategy to cope with the shortfall?
Alter the playing field and encourage more players, speakers suggested at a session at the recent Critical Care Congress in San Francisco.
A paper submitted for review by the journal Critical Care Medicine will propose that the Accreditation Council for Graduate Medical Education (ACGME) relax some "very restrictive mandates" on internal medicine-based critical care medicine training programs.
One hurdle requires the critical care medicine program's primary site to offer at least three out of five key fellowship programs. "That can be very difficult for many of the smaller programs that are not major academic centers, where they may not have things like fellowships in infectious diseases, nephrology, pulmonary, et cetera," said Dr. Stephen M. Pastores, FCCP, a lead author of the paper. Dr. Pastores is director of the critical care fellowship program at Memorial Sloan-Kettering Cancer Center, New York, and a board-certified internist, pulmonologist, and intensivist there.

He cochaired a 20-person committee to create proposals for the Critical Care Societies Collaborative's task force on critical care educational pathways in internal medicine.
Another barrier excludes physicians who are not certified in internal medicine from being counted as key faculty in internal medicine-based critical care training programs. "In my program, we have anesthesiologists and surgeons who are teaching our fellows, and there's no good reason they shouldn't be counted as key faculty," Dr. Pastores said at the congress, sponsored by the Society for Critical Care Medicine.
He and Dr. Brian Wessman, who also spoke at the meeting, cited another ACGME barrier, this one blocking the pipeline of emergency medicine physicians. Internal medicine-based critical care medicine training programs must limit the proportion of emergency medicine trainees to 25% of their programs.
However, because their training already includes exposure to undifferentiated critical care patients and development of a "robust procedural acumen applicable to critical care," emergency medicine physicians are the ideal candidates for critical care medicine, Dr. Wessman, an emergency medicine physician and codirector of the critical care fellowship program at Washington University, St. Louis, said at the meeting.
The hospitalist option
Hospitalists are another logical option, particularly because often they are already performing critical care duties. "Even if not hired primarily for that, they're doing it anyway," said Dr. Andrew D. Auerbach, a hospitalist and researcher at the University of California, San Francisco. A 2010 study found that 34 of 72 open intensive care units in Michigan had hospitalists as ICU attending physicians (J. Hosp. Med. 2010;5:4-9). These included smaller hospitals outside major population centers, not just small community hospitals, he said at the meeting.
Intensivists could benefit by forging clinical partnerships with hospitalists to tap hospitalists' expertise in sepsis care, patient monitoring, antimicrobial stewardship, comanaging surgical patients, and transitioning patient care, he suggested.
"Hospitalists want to go into critical care medicine but have been at times in limbo because there is no pathway for them except to do the 2 years of fellowship training," Dr. Pastores agreed in a separate presentation. "We need to help our hospitalists get to the promised land of the ICU," either by creating a shortened training pathway or by offering new incentives.
Community hospitals that want more intensivists could pay for hospitalists to pursue fellowship training and guarantee intensivist jobs when training is finished, said Dr. Pastores.
Hospitals that are determined to have intensivists run the ICU might consider that approach, which could offset the hassle of leaving one's job and taking a temporary pay cut in order to pursue a critical care fellowship, Dr. Franklin A. Michota agreed in an interview. Or, they simply could offer higher salaries to recruit intensivists. "It's a supply-and-demand phenomenon," said Dr. Michota, director of academic affairs in the department of hospitalist medicine at the Cleveland Clinic.
Two years ago, the Society of Hospital Medicine and Society of Critical Care Medicine (SCCM) proposed a 1-year expedited training pathway for "experienced" hospitalists to achieve CCM certification through the ABIM, Dr. Pastores and associates noted in a recent viewpoint article (Crit. Care Med. 2013;41:2754-61).
The proposal was met with deep skepticism by many in the chest physician community. Today, the concept is held by SCCM as a stepping stone toward a much-needed solution to a well-acknowledged problem.
In an interview, SCCM president Dr. Chris Farmer spoke to the issue broadly and with care: "There are not enough intensivists to fill the gap. Many hospitalists currently work in this capacity, and we need to work for longer-term solutions."
The American College of Chest Physicians and the American Association of Critical-Care Nurses have advocated for a "comprehensive approach to improving critical care delivery in the United States" (Chest 2012;142:5), pointing to telemedicine and interdisciplinary strategies to cope with the intensivist shortage rather than endorsing the expedited hospitalist training model.
Internal medicine as pipeline
Besides hospitalists, Dr. Pastores sees greater possibilities from expanding the pipeline of internists into critical care.
"The internal medicine-based trained intensivists really have no competing responsibilities" compared with pulmonologists, surgeons, or other specialists and thus are more likely to work full-time in an ICU, he said. "From that perspective, why are there only 34 stand-alone programs in internal medicine critical care compared to 134 programs in pulmonary critical care? Maybe that could be addressed in a more efficient way."
Pulmonary critical care medicine programs also could be doing more. Dr. Pastores said that although it's not well known, the ACGME allows pulmonary critical care programs every other year to train a fellow who does not want to be certified in pulmonary medicine but wants only to do critical care medicine. If the programs took advantage of that, the number of full-time critical care providers would increase, he said.
The speakers had no relevant disclosures.
Lori Buckner Farmer contributed to this article.
Dr. Eleanor Summerhill, FCCP, comments: How to address the growing shortfall in board-certified intensivists remains an area of continued debate. Currently, institutions are utilizing telemedicine, physician extenders, and in many instances, hospitalist physicians to fill this gap. At the Society of Critical Care Medicine (SCCM) Critical Care Congress in January 2014, speakers advocated for a number of possible solutions to this problem, largely involving expanding opportunities for further critical care training. These included relaxation of the ACGME mandate requiring that a critical care medicine fellowship's primary training site offer at least three of five key fellowship programs.
Given that there is a significant body of evidence that shows that patients cared for in high-intensity vs. low-intensity intensivist staffing models have reduced mortality and length of stay, going forward it will be important to consider some of these "thinking out of the box" models, while ensuring that alternative training strategies maintain appropriate levels of competency.
The shortage of intensivists in the critical care game isn't shrinking. What's the best strategy to cope with the shortfall?
Alter the playing field and encourage more players, speakers suggested at a session at the recent Critical Care Congress in San Francisco.
A paper submitted for review by the journal Critical Care Medicine will propose that the Accreditation Council for Graduate Medical Education (ACGME) relax some "very restrictive mandates" on internal medicine-based critical care medicine training programs.
One hurdle requires the critical care medicine program's primary site to offer at least three out of five key fellowship programs. "That can be very difficult for many of the smaller programs that are not major academic centers, where they may not have things like fellowships in infectious diseases, nephrology, pulmonary, et cetera," said Dr. Stephen M. Pastores, FCCP, a lead author of the paper. Dr. Pastores is director of the critical care fellowship program at Memorial Sloan-Kettering Cancer Center, New York, and a board-certified internist, pulmonologist, and intensivist there.
He cochaired a 20-person committee to create proposals for the Critical Care Societies Collaborative's task force on critical care educational pathways in internal medicine.
Another barrier excludes physicians who are not certified in internal medicine from being counted as key faculty in internal medicine-based critical care training programs. "In my program, we have anesthesiologists and surgeons who are teaching our fellows, and there's no good reason they shouldn't be counted as key faculty," Dr. Pastores said at the congress, sponsored by the Society for Critical Care Medicine.
He and Dr. Brian Wessman, who also spoke at the meeting, cited another ACGME barrier, this one blocking the pipeline of emergency medicine physicians. Internal medicine-based critical care medicine training programs must limit the proportion of emergency medicine trainees to 25% of their programs.
However, because their training already includes exposure to undifferentiated critical care patients and development of a "robust procedural acumen applicable to critical care," emergency medicine physicians are the ideal candidates for critical care medicine, Dr. Wessman, an emergency medicine physician and codirector of the critical care fellowship program at Washington University, St. Louis, said at the meeting.
The hospitalist option
Hospitalists are another logical option, particularly because often they are already performing critical care duties. "Even if not hired primarily for that, they're doing it anyway," said Dr. Andrew D. Auerbach, a hospitalist and researcher at the University of California, San Francisco. A 2010 study found that 34 of 72 open intensive care units in Michigan had hospitalists as ICU attending physicians (J. Hosp. Med. 2010;5:4-9). These included smaller hospitals outside major population centers, not just small community hospitals, he said at the meeting.
Intensivists could benefit by forging clinical partnerships with hospitalists to tap hospitalists' expertise in sepsis care, patient monitoring, antimicrobial stewardship, comanaging surgical patients, and transitioning patient care, he suggested.
"Hospitalists want to go into critical care medicine but have been at times in limbo because there is no pathway for them except to do the 2 years of fellowship training," Dr. Pastores agreed in a separate presentation. "We need to help our hospitalists get to the promised land of the ICU," either by creating a shortened training pathway or by offering new incentives.
Community hospitals that want more intensivists could pay for hospitalists to pursue fellowship training and guarantee intensivist jobs when training is finished, said Dr. Pastores.
Hospitals that are determined to have intensivists run the ICU might consider that approach, which could offset the hassle of leaving one's job and taking a temporary pay cut in order to pursue a critical care fellowship, Dr. Franklin A. Michota agreed in an interview. Or, they simply could offer higher salaries to recruit intensivists. "It's a supply-and-demand phenomenon," said Dr. Michota, director of academic affairs in the department of hospitalist medicine at the Cleveland Clinic.
Two years ago, the Society of Hospital Medicine and Society of Critical Care Medicine (SCCM) proposed a 1-year expedited training pathway for "experienced" hospitalists to achieve CCM certification through the ABIM, Dr. Pastores and associates noted in a recent viewpoint article (Crit. Care Med. 2013;41:2754-61).
The proposal was met with deep skepticism by many in the chest physician community. Today, the concept is held by SCCM as a stepping stone toward a much-needed solution to a well-acknowledged problem.
In an interview, SCCM president Dr. Chris Farmer spoke to the issue broadly and with care: "There are not enough intensivists to fill the gap. Many hospitalists currently work in this capacity, and we need to work for longer-term solutions."
The American College of Chest Physicians and the American Association of Critical-Care Nurses have advocated for a "comprehensive approach to improving critical care delivery in the United States" (Chest 2012;142:5), pointing to telemedicine and interdisciplinary strategies to cope with the intensivist shortage rather than endorsing the expedited hospitalist training model.
Internal medicine as pipeline
Besides hospitalists, Dr. Pastores sees greater possibilities from expanding the pipeline of internists into critical care.
"The internal medicine-based trained intensivists really have no competing responsibilities" compared with pulmonologists, surgeons, or other specialists and thus are more likely to work full-time in an ICU, he said. "From that perspective, why are there only 34 stand-alone programs in internal medicine critical care compared to 134 programs in pulmonary critical care? Maybe that could be addressed in a more efficient way."
Pulmonary critical care medicine programs also could be doing more. Dr. Pastores said that although it's not well known, the ACGME allows pulmonary critical care programs every other year to train a fellow who does not want to be certified in pulmonary medicine but wants only to do critical care medicine. If the programs took advantage of that, the number of full-time critical care providers would increase, he said.
The speakers had no relevant disclosures.
Lori Buckner Farmer contributed to this article.
Dr. Eleanor Summerhill, FCCP, comments: How to address the growing shortfall in board-certified intensivists remains an area of continued debate. Currently, institutions are utilizing telemedicine, physician extenders, and in many instances, hospitalist physicians to fill this gap. At the Society of Critical Care Medicine (SCCM) Critical Care Congress in January 2014, speakers advocated for a number of possible solutions to this problem, largely involving expanding opportunities for further critical care training. These included relaxation of the ACGME mandate requiring that a critical care medicine fellowship's primary training site offer at least three of five key fellowship programs.
Given that there is a significant body of evidence that shows that patients cared for in high-intensity vs. low-intensity intensivist staffing models have reduced mortality and length of stay, going forward it will be important to consider some of these "thinking out of the box" models, while ensuring that alternative training strategies maintain appropriate levels of competency.
The shortage of intensivists in the critical care game isn't shrinking. What's the best strategy to cope with the shortfall?
Alter the playing field and encourage more players, speakers suggested at a session at the recent Critical Care Congress in San Francisco.
A paper submitted for review by the journal Critical Care Medicine will propose that the Accreditation Council for Graduate Medical Education (ACGME) relax some "very restrictive mandates" on internal medicine-based critical care medicine training programs.
One hurdle requires the critical care medicine program's primary site to offer at least three out of five key fellowship programs. "That can be very difficult for many of the smaller programs that are not major academic centers, where they may not have things like fellowships in infectious diseases, nephrology, pulmonary, et cetera," said Dr. Stephen M. Pastores, FCCP, a lead author of the paper. Dr. Pastores is director of the critical care fellowship program at Memorial Sloan-Kettering Cancer Center, New York, and a board-certified internist, pulmonologist, and intensivist there.
He cochaired a 20-person committee to create proposals for the Critical Care Societies Collaborative's task force on critical care educational pathways in internal medicine.
Another barrier excludes physicians who are not certified in internal medicine from being counted as key faculty in internal medicine-based critical care training programs. "In my program, we have anesthesiologists and surgeons who are teaching our fellows, and there's no good reason they shouldn't be counted as key faculty," Dr. Pastores said at the congress, sponsored by the Society for Critical Care Medicine.
He and Dr. Brian Wessman, who also spoke at the meeting, cited another ACGME barrier, this one blocking the pipeline of emergency medicine physicians. Internal medicine-based critical care medicine training programs must limit the proportion of emergency medicine trainees to 25% of their programs.
However, because their training already includes exposure to undifferentiated critical care patients and development of a "robust procedural acumen applicable to critical care," emergency medicine physicians are the ideal candidates for critical care medicine, Dr. Wessman, an emergency medicine physician and codirector of the critical care fellowship program at Washington University, St. Louis, said at the meeting.
The hospitalist option
Hospitalists are another logical option, particularly because often they are already performing critical care duties. "Even if not hired primarily for that, they're doing it anyway," said Dr. Andrew D. Auerbach, a hospitalist and researcher at the University of California, San Francisco. A 2010 study found that 34 of 72 open intensive care units in Michigan had hospitalists as ICU attending physicians (J. Hosp. Med. 2010;5:4-9). These included smaller hospitals outside major population centers, not just small community hospitals, he said at the meeting.
Intensivists could benefit by forging clinical partnerships with hospitalists to tap hospitalists' expertise in sepsis care, patient monitoring, antimicrobial stewardship, comanaging surgical patients, and transitioning patient care, he suggested.
"Hospitalists want to go into critical care medicine but have been at times in limbo because there is no pathway for them except to do the 2 years of fellowship training," Dr. Pastores agreed in a separate presentation. "We need to help our hospitalists get to the promised land of the ICU," either by creating a shortened training pathway or by offering new incentives.
Community hospitals that want more intensivists could pay for hospitalists to pursue fellowship training and guarantee intensivist jobs when training is finished, said Dr. Pastores.
Hospitals that are determined to have intensivists run the ICU might consider that approach, which could offset the hassle of leaving one's job and taking a temporary pay cut in order to pursue a critical care fellowship, Dr. Franklin A. Michota agreed in an interview. Or, they simply could offer higher salaries to recruit intensivists. "It's a supply-and-demand phenomenon," said Dr. Michota, director of academic affairs in the department of hospitalist medicine at the Cleveland Clinic.
Two years ago, the Society of Hospital Medicine and Society of Critical Care Medicine (SCCM) proposed a 1-year expedited training pathway for "experienced" hospitalists to achieve CCM certification through the ABIM, Dr. Pastores and associates noted in a recent viewpoint article (Crit. Care Med. 2013;41:2754-61).
The proposal was met with deep skepticism by many in the chest physician community. Today, the concept is held by SCCM as a stepping stone toward a much-needed solution to a well-acknowledged problem.
In an interview, SCCM president Dr. Chris Farmer spoke to the issue broadly and with care: "There are not enough intensivists to fill the gap. Many hospitalists currently work in this capacity, and we need to work for longer-term solutions."
The American College of Chest Physicians and the American Association of Critical-Care Nurses have advocated for a "comprehensive approach to improving critical care delivery in the United States" (Chest 2012;142:5), pointing to telemedicine and interdisciplinary strategies to cope with the intensivist shortage rather than endorsing the expedited hospitalist training model.
Internal medicine as pipeline
Besides hospitalists, Dr. Pastores sees greater possibilities from expanding the pipeline of internists into critical care.
"The internal medicine-based trained intensivists really have no competing responsibilities" compared with pulmonologists, surgeons, or other specialists and thus are more likely to work full-time in an ICU, he said. "From that perspective, why are there only 34 stand-alone programs in internal medicine critical care compared to 134 programs in pulmonary critical care? Maybe that could be addressed in a more efficient way."
Pulmonary critical care medicine programs also could be doing more. Dr. Pastores said that although it's not well known, the ACGME allows pulmonary critical care programs every other year to train a fellow who does not want to be certified in pulmonary medicine but wants only to do critical care medicine. If the programs took advantage of that, the number of full-time critical care providers would increase, he said.
The speakers had no relevant disclosures.
Lori Buckner Farmer contributed to this article.
Dr. Eleanor Summerhill, FCCP, comments: How to address the growing shortfall in board-certified intensivists remains an area of continued debate. Currently, institutions are utilizing telemedicine, physician extenders, and in many instances, hospitalist physicians to fill this gap. At the Society of Critical Care Medicine (SCCM) Critical Care Congress in January 2014, speakers advocated for a number of possible solutions to this problem, largely involving expanding opportunities for further critical care training. These included relaxation of the ACGME mandate requiring that a critical care medicine fellowship's primary training site offer at least three of five key fellowship programs.
Given that there is a significant body of evidence that shows that patients cared for in high-intensity vs. low-intensity intensivist staffing models have reduced mortality and length of stay, going forward it will be important to consider some of these "thinking out of the box" models, while ensuring that alternative training strategies maintain appropriate levels of competency.

Moderate exercise reduces female stroke risk
SAN DIEGO – Moderate exercise significantly reduced the risk of stroke in women and seemed to offset much but not all of the increased stroke risk in postmenopausal women on hormone therapy, a large retrospective study found.
A self-reported history of moderate-to-strenuous physical activity in the prior 3 years was associated with a roughly 20%-30% lower risk for stroke in an analysis of data on 133,479 women in the California Teachers Study who had been followed every 4-5 years since 1995 by questionnaire, Sophia S. Wang, Ph.D., and her associates reported.

They linked the data set with hospitalization data during 1996-2010 to identify 2,416 ischemic strokes and 710 hemorrhagic strokes in the cohort that were validated by a review of medical records.
The strongest reduction in stroke risk was seen in women who reported moderate physical activity such as brisk walking, recreational tennis, golf, volleyball, or cycling on level streets. Women who reported in 1995-1996 questionnaires that they had engaged in moderate activity in the prior 3 years were 12%-22% less likely to develop a stroke, depending on the amount of activity each week, compared with inactive women who reported less than a half-hour per week of moderate activity.
"You don’t have to climb a mountain" to gain the stroke-reducing benefits of exercise, Dr. Wang said in an interview at the International Stroke Conference. And the fact that people tend to overreport how much they exercise when surveyed makes the findings "particularly robust," she said.
Indeed, reports of strenuous activity were not significantly associated with lower stroke risk. Strenuous activity included swimming laps, aerobics, running, calisthenics, jogging, basketball, racquetball, or cycling on hills. Risk levels ranged from an increase of 3% to a reduction of 18% with strenuous activity, compared with inactive women.
Because most women who exercised strenuously also reported moderate activity, the investigators combined those two activity categories and again found approximately a 20% reduction in stroke risk that clearly was being driven by the benefits of moderate activity, said Dr. Wang of Beckman Research Institute at the City of Hope, Duarte, Calif. Stroke risk reductions ranged from 15%-23% in the combined activity analysis for the 1995-1996 surveys.
Surveyed again in 2005-2006, women who reported moderate or strenuous activity in the prior 3 years were 12%-20% less likely to develop a stroke, compared with inactive women, she said at the meeting, sponsored by the American Heart Association.
More than 5 hours of activity wasn’t more beneficial than fewer hours, she added. Stroke reduction benefits seemed greatest with 3.5-5 hours of activity per week, which was associated with a 23% risk reduction in the earlier survey and a 29% reduction in the later survey. With more than 5 hours, the risk reduction was 17% and 27%, respectively.
In inactive postmenopausal women, current hormone use was associated with a 59% higher risk for stroke and former hormone use was associated with a 16% increased risk, compared with postmenopausal women who didn’t use hormones, Dr. Wang said. However, the elevated stroke risk with hormone use fell in women who exercised, compared with those who didn’t.
In current hormone users, stroke risk was 37% higher in women who reported 0.51-3.5 hours of moderate or strenuous activity per week and 29% higher in women who reported more than 3.5 hours of activity per week, compared with non-hormone users. In former hormone users, stroke risk was 15% higher in those who reported 0.51-3.5 hours of activity per week and 5% higher in those who exercised more than 3.5 hours per week, compared with non-hormone users.
Because of smaller numbers of women in the subset analyses of postmenopausal hormone use, these differences between groups did not reach statistical significance, Dr. Wang said.
She and her associates plan further studies related to these findings, including whether or not activity levels may help prevent stroke in women who’ve already had a stroke, she said.
Dr. Wang and her colleagues reported having no financial disclosures. The National Institute of Neurological Disorders and Stroke funded the study.
On Twitter @sherryboschert
SAN DIEGO – Moderate exercise significantly reduced the risk of stroke in women and seemed to offset much but not all of the increased stroke risk in postmenopausal women on hormone therapy, a large retrospective study found.
A self-reported history of moderate-to-strenuous physical activity in the prior 3 years was associated with a roughly 20%-30% lower risk for stroke in an analysis of data on 133,479 women in the California Teachers Study who had been followed every 4-5 years since 1995 by questionnaire, Sophia S. Wang, Ph.D., and her associates reported.
They linked the data set with hospitalization data during 1996-2010 to identify 2,416 ischemic strokes and 710 hemorrhagic strokes in the cohort that were validated by a review of medical records.
The strongest reduction in stroke risk was seen in women who reported moderate physical activity such as brisk walking, recreational tennis, golf, volleyball, or cycling on level streets. Women who reported in 1995-1996 questionnaires that they had engaged in moderate activity in the prior 3 years were 12%-22% less likely to develop a stroke, depending on the amount of activity each week, compared with inactive women who reported less than a half-hour per week of moderate activity.
"You don’t have to climb a mountain" to gain the stroke-reducing benefits of exercise, Dr. Wang said in an interview at the International Stroke Conference. And the fact that people tend to overreport how much they exercise when surveyed makes the findings "particularly robust," she said.
Indeed, reports of strenuous activity were not significantly associated with lower stroke risk. Strenuous activity included swimming laps, aerobics, running, calisthenics, jogging, basketball, racquetball, or cycling on hills. Risk levels ranged from an increase of 3% to a reduction of 18% with strenuous activity, compared with inactive women.
Because most women who exercised strenuously also reported moderate activity, the investigators combined those two activity categories and again found approximately a 20% reduction in stroke risk that clearly was being driven by the benefits of moderate activity, said Dr. Wang of Beckman Research Institute at the City of Hope, Duarte, Calif. Stroke risk reductions ranged from 15%-23% in the combined activity analysis for the 1995-1996 surveys.
Surveyed again in 2005-2006, women who reported moderate or strenuous activity in the prior 3 years were 12%-20% less likely to develop a stroke, compared with inactive women, she said at the meeting, sponsored by the American Heart Association.
More than 5 hours of activity wasn’t more beneficial than fewer hours, she added. Stroke reduction benefits seemed greatest with 3.5-5 hours of activity per week, which was associated with a 23% risk reduction in the earlier survey and a 29% reduction in the later survey. With more than 5 hours, the risk reduction was 17% and 27%, respectively.
In inactive postmenopausal women, current hormone use was associated with a 59% higher risk for stroke and former hormone use was associated with a 16% increased risk, compared with postmenopausal women who didn’t use hormones, Dr. Wang said. However, the elevated stroke risk with hormone use fell in women who exercised, compared with those who didn’t.
In current hormone users, stroke risk was 37% higher in women who reported 0.51-3.5 hours of moderate or strenuous activity per week and 29% higher in women who reported more than 3.5 hours of activity per week, compared with non-hormone users. In former hormone users, stroke risk was 15% higher in those who reported 0.51-3.5 hours of activity per week and 5% higher in those who exercised more than 3.5 hours per week, compared with non-hormone users.
Because of smaller numbers of women in the subset analyses of postmenopausal hormone use, these differences between groups did not reach statistical significance, Dr. Wang said.
She and her associates plan further studies related to these findings, including whether or not activity levels may help prevent stroke in women who’ve already had a stroke, she said.
Dr. Wang and her colleagues reported having no financial disclosures. The National Institute of Neurological Disorders and Stroke funded the study.
On Twitter @sherryboschert
SAN DIEGO – Moderate exercise significantly reduced the risk of stroke in women and seemed to offset much but not all of the increased stroke risk in postmenopausal women on hormone therapy, a large retrospective study found.
A self-reported history of moderate-to-strenuous physical activity in the prior 3 years was associated with a roughly 20%-30% lower risk for stroke in an analysis of data on 133,479 women in the California Teachers Study who had been followed every 4-5 years since 1995 by questionnaire, Sophia S. Wang, Ph.D., and her associates reported.
They linked the data set with hospitalization data during 1996-2010 to identify 2,416 ischemic strokes and 710 hemorrhagic strokes in the cohort that were validated by a review of medical records.
The strongest reduction in stroke risk was seen in women who reported moderate physical activity such as brisk walking, recreational tennis, golf, volleyball, or cycling on level streets. Women who reported in 1995-1996 questionnaires that they had engaged in moderate activity in the prior 3 years were 12%-22% less likely to develop a stroke, depending on the amount of activity each week, compared with inactive women who reported less than a half-hour per week of moderate activity.
"You don’t have to climb a mountain" to gain the stroke-reducing benefits of exercise, Dr. Wang said in an interview at the International Stroke Conference. And the fact that people tend to overreport how much they exercise when surveyed makes the findings "particularly robust," she said.
Indeed, reports of strenuous activity were not significantly associated with lower stroke risk. Strenuous activity included swimming laps, aerobics, running, calisthenics, jogging, basketball, racquetball, or cycling on hills. Risk levels ranged from an increase of 3% to a reduction of 18% with strenuous activity, compared with inactive women.
Because most women who exercised strenuously also reported moderate activity, the investigators combined those two activity categories and again found approximately a 20% reduction in stroke risk that clearly was being driven by the benefits of moderate activity, said Dr. Wang of Beckman Research Institute at the City of Hope, Duarte, Calif. Stroke risk reductions ranged from 15%-23% in the combined activity analysis for the 1995-1996 surveys.
Surveyed again in 2005-2006, women who reported moderate or strenuous activity in the prior 3 years were 12%-20% less likely to develop a stroke, compared with inactive women, she said at the meeting, sponsored by the American Heart Association.
More than 5 hours of activity wasn’t more beneficial than fewer hours, she added. Stroke reduction benefits seemed greatest with 3.5-5 hours of activity per week, which was associated with a 23% risk reduction in the earlier survey and a 29% reduction in the later survey. With more than 5 hours, the risk reduction was 17% and 27%, respectively.
In inactive postmenopausal women, current hormone use was associated with a 59% higher risk for stroke and former hormone use was associated with a 16% increased risk, compared with postmenopausal women who didn’t use hormones, Dr. Wang said. However, the elevated stroke risk with hormone use fell in women who exercised, compared with those who didn’t.
In current hormone users, stroke risk was 37% higher in women who reported 0.51-3.5 hours of moderate or strenuous activity per week and 29% higher in women who reported more than 3.5 hours of activity per week, compared with non-hormone users. In former hormone users, stroke risk was 15% higher in those who reported 0.51-3.5 hours of activity per week and 5% higher in those who exercised more than 3.5 hours per week, compared with non-hormone users.
Because of smaller numbers of women in the subset analyses of postmenopausal hormone use, these differences between groups did not reach statistical significance, Dr. Wang said.
She and her associates plan further studies related to these findings, including whether or not activity levels may help prevent stroke in women who’ve already had a stroke, she said.
Dr. Wang and her colleagues reported having no financial disclosures. The National Institute of Neurological Disorders and Stroke funded the study.
On Twitter @sherryboschert
AT THE INTERNATIONAL STROKE CONFERENCE
Major finding: Women who reported more than a half-hour of moderate activity per week in the prior 3 years were 12%-22% less likely to have a stroke, compared with less-active women.
Data source: A retrospective analysis of data on 133,479 women followed longitudinally in the California Teachers Study.
Disclosures: Dr. Wang and her colleagues reported having no financial disclosures. The National Institute of Neurological Disorders and Stroke funded the study.
