Enhanced brief lifestyle counseling by a primary care team helped about one-third of obese patients lose and keep off 5% or more of their baseline weight after 2 years, according to a study published online Nov. 14 in the New England Journal of Medicine and simultaneously presented at the annual meeting of the American Heart Association.
However, many of the patients during the study’s second year regained at least some of the lost weight, confirming "the problem of weight regain despite ongoing counseling for weight-loss maintenance," the study’s authors noted.
The intervention involved quarterly visits with a primary care physician, brief lifestyle coaching delivered monthly by a medical assistant, and the use of meal replacements or weight-loss medication.
The average weight loss of 4.7%, most of which was maintained for 2 years and was accompanied by improvements in some cardiovascular risk factors, was greater than that observed in other primary care trials, said Thomas A. Wadden, Ph.D., of the department of psychiatry at the University of Pennsylvania, Philadelphia, and his associates (N. Engl. J. Med. 2011 Nov. 14 [doi:10.1056/NEJMoa1109220]).
The results of the 2-year study of 390 obese patients demonstrate that "primary care physicians could help a considerable minority of obese persons achieve clinically meaningful weight loss, which they may not achieve if they were simply told to reduce their weight on their own," the investigators noted.
Dr. Wadden and his colleagues conducted the POWER-UP (Practice-based Opportunities for Weight Reduction trial at the University of Pennsylvania) study at three primary care practices in urban settings and three in suburban settings. A total of 30 primary care physicians took part.
The study enrolled 311 women and 79 men, with a mean age of 52 years, a mean body weight of 108 kg, and a mean body mass index of 39 kg/m2 at baseline. By patient self-report, approximately 59% were white, 38.5% were black, and 4.6% were Hispanic.
The study participants all had the same dietary and activity goals but were given different levels of support to achieve them.
All were instructed to gradually increase their physical activity to 180 min/wk. Those who weighed less than 113 kg were prescribed a diet of 1,200-1,500 kcal/day, while those who were heavier were prescribed 1,500-1,800 kcal/day.
A total of 130 patients were randomly assigned to receive usual care, which consisted of quarterly visits in which their primary care physician spent 5-7 minutes discussing the weight-loss information and reviewing any weight change.
Another 131 were randomly assigned to that same care plus brief lifestyle counseling, in which they spent 10-15 min/mo with a medical assistant, called a "lifestyle coach," who conducted a weigh-in, reviewed a diary of food intake, reviewed a physical activity diary, and delivered abbreviated lessons from the Diabetes Prevention Program.
Another 129 patients were randomly assigned to receive enhanced lifestyle counseling, which included that same intervention plus their choice of taking sibutramine, orlistat, or meal replacements under the guidance of the primary care physician. Sibutramine was withdrawn from the market during the trial, and patients in that group were switched to orlistat or meal replacements.
Patients taking meal replacements were instructed to substitute two meals and one snack every day with Slim-Fast shakes or meal bars for the first 4 months, and to replace one meal and one snack each day for the remainder of the study.
The primary outcome was weight loss at 2 years. Enhanced lifestyle counseling produced significantly greater weight loss (mean, 4.6 kg) than either lifestyle counseling (2.9 kg) or usual care (1.7 kg). Within the group receiving enhanced lifestyle counseling, there were no significant differences in weight loss among those taking meal replacements (67 patients), sibutramine (38 patients), or orlistat (24 patients).
The differences among the groups were first evident at 6 months, and maximal weight loss was achieved at 12 months. Between year 1 and year 2, however, most patients regained at least some of the weight they had lost.
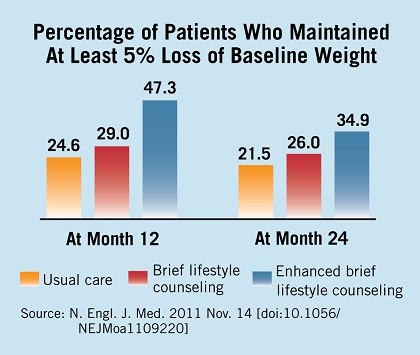
Secondary outcomes also were significantly better in the group that received enhanced lifestyle counseling than in the usual-care group, including the percentage of patients whose weight was at or below their baseline weight at 1 year (72.1% vs. 59.2%) and 2 years (67.4% vs. 53.1%); the percentages who lost 5% or more of their baseline weight at 1 year (47.3% vs. 24.6%) and 2 years (34.9% vs. 21.5%); and the percentages who lost 10% or more of their baseline weight at 1 year (25.6% vs. 3.9%) and 2 years (17.8% vs. 6.2%).
Patients who received enhanced lifestyle counseling showed significantly greater improvements in waist circumference, HDL cholesterol levels, and triglyceride levels, but not in LDL cholesterol levels or blood pressure.