
A new endoluminal device that reduces the coronary sinus significantly improved refractory angina in patients with advanced coronary artery disease who weren’t candidates for revascularization in a small phase II clinical trial. The results were published online Feb. 5 in the New England Journal of Medicine.
The international, randomized, double-blind study, sponsored by Neovasc, maker of the Reducer device, involved 104 patients enrolled who had Canadian Cardiovascular Society (CCS) class III or IV angina despite maximal medical therapy, evidence of reversible myocardial ischemia, and a left ventricular ejection fraction over 25%. These participants (mean age 68 years; range, 35-87 years) underwent right heart catheterization with angiography of the coronary sinus to determine whether the anatomy was suitable for implantation. Then 52 underwent implantation (the treatment group) and 52 underwent a sham procedure (the control group), and all were followed for up to 3 years, said Dr. Stefan Verheye of Antwerp (Belgium) Cardiovascular Center and his associates.
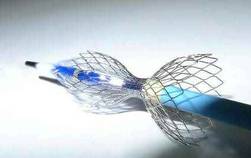 Courtesy Neovasc Inc.
Courtesy Neovasc Inc.
Neovasc's Reducer device creates a focal narrowing that increases pressure in the coronary sinus.
The stainless steel device is balloon expandable and shaped like an hourglass. It creates a focal narrowing that increases pressure in the coronary sinus, which is thought to recruit coronary collateral blood flow, redistributing blood from the less-ischemic epicardium to the ischemic endocardium. The primary efficacy end point of the trial – the number of patients whose angina improved by two or more CCS classes within 6 months – was achieved by more than twice as many patients in the treatment group (18, or 35%) as in the control group (8, or 15%).
A total of 37 patients (71%) who received active treatment showed an improvement of at least one CCS class, compared with 22 (42%) of those who received the sham treatment. Quality of life, as measured by Seattle Angina Questionnaire score, improved by 17.6 out of a possible 100 points for active treatment, compared with 7.6 points for sham treatment. And exercise duration improved by 1 minute (13%) for active treatment, compared with 4 seconds (1%) for sham treatment, Dr. Verheye and his associates said (N. Engl. J. Med. 2015 Feb. 5 [doi:10.1056/NEJMoa1402556]). “Our study was not statistically powered to detect an improvement in ischemia by means of objective measures such as stress testing or wall-motion index. A larger trial would be necessary to show such a benefit,” they noted.
There were 76 adverse events in patients who received the implant and 93 in the control group; the numbers of serious adverse events in this high-risk cohort were 10 and 24, respectively. This included one periprocedural MI that occurred in a patient receiving active treatment. Among 36 of the patients who received the implant and later underwent CT angiography, none showed any evidence of device migration or occlusion, the investigators added.
This study was supported by Neovasc, manufacturer of the Reducer device. Dr. Verheye reported having no financial disclosures. His associates reported ties to Neovasc, Abbott, Boston Scientific, Novo Nordisk, Eli Lilly, and Zealand Pharma.