Infantile hemangiomas treated with propranolol recurred in 25% of children after discontinuation of propranolol in a retrospective study of nearly 1,000 patients, according to findings published online March 7 in Pediatrics.
“Identifying risk factors for rebound growth could affect treatment strategies, particularly duration of therapy,” wrote Dr. Sonal D. Shah of the University of California, San Francisco, and colleagues.
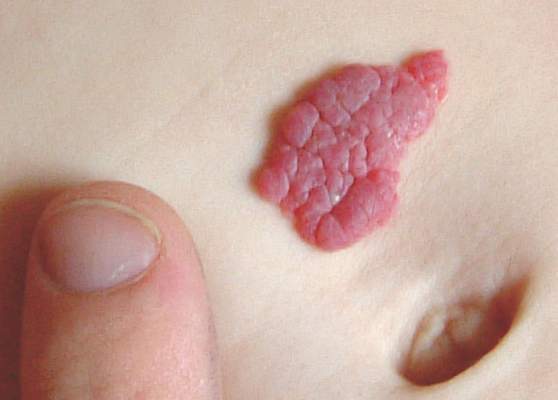 Wikimedia Commons/Zeimusu/Public Domain
Wikimedia Commons/Zeimusu/Public Domain
The study population was the largest to date, the researchers noted, and included 980 children seen at 10 academic centers between 2008 and 2013. Most were term (82%) and female (77%). The average age at the start of treatment was 6 months, and a visual analog scale was used to determine the children’s response to treatment (Pediatrics. 2016. doi: 10.1542/peds.2015-1754). Overall, hemangiomas rebounded in 231 patients (25%). Of these, 191 (83%) required treatment modification. The mean age before initial hemangioma rebound was 17 months, after a mean treatment duration of 11 months.
“The most potent risk factor for rebound was the presence of a deep infantile hemangioma component (i.e., deep or mixed morphology), which was also noted in other studies,” the researchers wrote.
In a multivariate analysis, deep hemangiomas and mixed hemangiomas were significantly more likely (odds ratio, 3.3 and 2.4, respectively) to rebound than superficial hemangiomas, and rebounds were significantly more likely among girls than boys (OR, 1.7).
“The exact reasons for this are uncertain, but it appears that girls are intrinsically more predisposed not only to hemangioma development but also to growth,” Dr. Shah and associates said.
Children least likely to rebound were those who discontinued or tapered propranolol between ages 12 and 18 months, and this group was used as a reference group. By comparison, the odds of rebound were notably high among children who discontinued when they were younger than 9 months (OR, 2.4). The odds ratios for rebound when propranolol was discontinued at ages 18-21 months, 21-24 months, and older than 24 months were 2.0, 1.7, and 2.5, respectively.
The results were limited by the fact that most patients represented more severe cases that were referred for additional treatment, Dr. Shah and associates said. However, the findings suggest that recognizing the risk factors for rebound could aid clinicians when planning therapy.
Lead author Dr. Shah had no relevant financial conflicts to disclose. Several coauthors reported serving as investigators or consultants for Pfizer and for Pierre Fabre Dermatology, which manufactures the propranolol product used in the study. The study was supported by the University of California, San Francisco, Pediatric Dermatology research fund.