Adolescent
It is during adolescence (ages 10 to 18) that idiopathic scoliosis is most common. Approximately 2% to 3% of children ages 10 to 15 have scoliosis with a curve of at least 10°. Among these patients, however, just 5% have scoliosis of clinical significance to warrant treatment (ie, curve progression > 30°).5,22
Each child should be examined initially for nonstructural scoliosis. This includes postural scoliosis, which resolves when a child is recumbent; compensatory scoliosis, which can be the result of a leg-length discrepancy (with no fixed vertebral rotation); sciatic scoliosis, an abnormality that results from avoiding the pain of an irritated sciatic nerve; inflammatory scoliosis, which could result from an infectious process, such as acute appendicitis; and hysterical scoliosis, a very rare form with an underlying psychological factor.4
Structural scoliosis comprises the remaining types of scoliosis, including the idiopathic variety. Patients with adolescent idiopathic scoliosis (AIS) are older than 10 and usually undergoing a rapid growth phase. Thus, some adolescent patients' curves can progress rapidly.4
Adolescents with idiopathic scoliosis rarely complain of pain or neurologic symptoms. Generally, their spinal curves do not cause organ pressure or shortness of breath. Many patients with AIS are involved in extracurricular activities that can trigger low back pain, yet activity-related low back pain is not an uncommon complaint among teens in general. Therefore, it is felt that when a patient with AIS has intermittent low back pain, it is most likely not related to their curve(s). Nevertheless, if a patient with AIS develops continued or unexplained low back pain and/or new neurologic symptoms, MRI is warranted.3
HISTORY, PHYSICAL EXAMINATION, AND DIAGNOSIS
During the exam, elicit any family history of scoliosis, especially in the setting of known diseases, such as Marfan syndrome, neurofibromatosis, muscular dystrophy, or other related diseases. Approximately 30% of AIS patients have a family history of scoliosis, so although the cause may not be clear, some genetic component is possible.3 The examination should stem from the patient's current stage of growth and development (see Table 31,3,4,7,23). The diagnosis of scoliosis is typically made during the examination and confirmed by radiography.
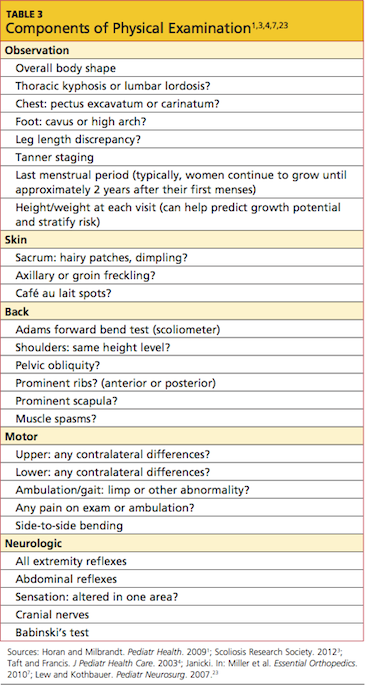
The newborn patient should be kept warm but be wearing only a diaper during the exam. A child or adolescent should be undressed and wearing a patient gown (unless at a school screening).
A general observation should be done initially, including the child's overall shape. The examiner should look for marfanoid features, such as excessive height, long arms, long trunk, and joint laxity.7 In the examination of the feet, an extremely high arch or cavus foot may be indicative of tethered spinal cord, spinal syrinx, or Charcot-Marie-Tooth disease, especially if the cavus is unilateral.1,7,23 MRI would be warranted in these instances.1
The examining clinician should note the child's Tanner stage. Height and weight measurements should be taken, and for a girl, age at menarche should be recorded.4
Next, the skin should be carefully inspected. In the infant, the examiner should look for hairy patches at the base of the spine, cutaneous sinuses, sacral dimpling, or other skin lesions that may suggest spinal dysraphism (ie, failure of the posterior elements to fuse around the spinal cord).4 Examination for café au lait spots and/or freckling in the axilla or groin area should be included, as this could signify neurofibromatosis.1,4,7
Examine the back in a standing child. Note whether the head appears to be centered over the sacrum. Evaluate for shoulder height or truncal asymmetry, scapular or posterior rib prominence, and excessive thoracic kyphosis and/or lumbar lordosis. Examine the pelvic bones, looking for obliquity (ie, one side higher than the other). Look for leg length discrepancy, both while the patient is standing still and during a gait review.1
During an anterior exam, look for shoulder or truncal asymmetry, leg length discrepancy, and anterior rib prominence. If shoulder height asymmetry is apparent, measure from each acromioclavicular joint to the floor and note the difference in centimeters. In the case of pelvic obliquity, measure from each anterior (or posterior) superior iliac spine to the floor and note the difference in centimeters. If the head does not appear to align over the sacrum, lower a plum line from the spinous process of C7 down to the gluteal cleft level. Measure by centimeters the distance from the cleft to the line, noting the side to which the line sways.
View the patient from the side. The sagittal curve can be assessed from the occiput to the sacrum; observe for an increased lordotic or kyphotic curve or abnormal positioning related to abnormal curves.4
