When they are allowed to reach this size, BCCs can become a real problem. In extreme instances, they can erode into the face and even into bone. Patients can lose ears, noses, or even their entire face to this relentless but “safe” cancer. Given enough time and bad luck, BCC can metastasize to local lymph nodes and even to the brain or lung; it is even occasionally a cause of death.
Patients often ask why we have to remove BCCs if they’re usually “safe.” Without trying to scare them, we describe cases such as this one as the inevitable outcome of prolonged neglect and/or an aggressive tumor. BCCs almost never heal without treatment and almost always grow wider and deeper over time. Some are extremely indolent, taking 20 years to become noticeable, while others are more aggressive. In addition to the clinical behavior of any given BCC, there are also histologic clues to how aggressive a particular BCC might be.
This patient was referred to a Mohs surgeon, who will be able to do two things that require specialized training:
1. He’ll remove the biopsy-proven cancer with scalpel surgery, and while the patient is still present, check the margins for residual cancer. If the margins are positive, he’ll go back to the area and remove more, repeating this step until clear wide and deep microscopic margins are visualized by frozen section technique. (It’s important to note that the exact way the frozen specimen is processed and examined permits evaluation of the entire margin—top, bottom, sides—making it considerably different from ordinary frozen sections.)
2. Then, the Mohs surgeon will have the skill to close the defect in an acceptable way: usually by primary closure, sometimes with flaps or with grafts. All of this is typically done on an outpatient basis, on the same visit, although it may take most of a morning or afternoon.
Mohs surgery was pioneered in the 1930s by Frederic Mohs, MD, a general surgeon, as a way to address large and/or aggressive cancers located in difficult areas (eg, face or genitals). It is not indicated for ordinary, relatively small skin cancers on the arms, legs, or trunk.
Some BCCs and squamous cell carcinomas develop in especially difficult areas, such as the eyelids, or involve large areas of the ear. These lesions may require the attention of relevant surgical specialists, such as oculoplastic or head and neck surgeons.
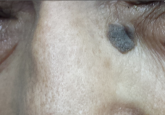
This patient will undergo Mohs surgery in the near future, and her defect will probably be closed primarily. The depth and histologic markers indicating exceptional aggression may dictate a further step: Radiation therapy may be required to minimize the likelihood of recurrence. Her chances of a complete cure are 95% to 97% with Mohs surgery alone.
• Basal cell carcinomas (BCCs) are often mistaken for infection.
• BCCs almost never heal on their own, grow slowly but steadily, and can reach prodigious size and depth.
• BCCs can metastasize to local nodes or even to the brain and lung.
• Ordinary excision is adequate for most BCCs, but Mohs surgery is indicated for larger lesions located in difficult areas (eg, face, scalp or groin).
• Simple shave biopsy is adequate to diagnose most BCCs.