This article describes the challenges of diagnosis and treatment of pediatric concussive injuries, with particular attention to the effects of concussion on the developing brain. It highlights the need for individualized, age-dependent care; standardized return-to-play and return-to-school protocols; and better-informed clinicians, parents, teachers, and coaches.
Pediatric concussions—those occurring in children younger than 18—account for almost half a million emergency department visits each year.1 Of these, more than 25% occur during sports-related activities.2 Yet it is believed that pediatric concussive injuries are significantly underreported because parents do not always seek medical attention for their concussed children and because little has been published on the management of sports-related concussions in pre–high-school-age athletes.2
The 4th International Consensus Conference on Concussion in Sport, the American Academy of Neurology, and the American Medical Society for Sports Medicine all recently updated their guidelines for concussion evaluation and management.3-5 However, the lack of data on concussions in younger pediatric athletes presents challenges for the optimal management of these patients.6 In fact, in a February 2014 report, the Institute of Medicine said that more research is needed to develop evidence-based sports-related concussion management guidelines for children and adolescents.7
In this article, the factors that distinguish concussions in children from those in adults will be described, as will the management techniques that primary care clinicians can use to effectively address them.
WHAT IS A CONCUSSION?
Although the term concussion has been used interchangeably with head trauma and brain injury, concussion is most often described as mild traumatic brain injury (mTBI). Variations in terminology reflect both the lack of agreement on a standard definition for concussion, especially as it applies to the pediatric population, and the complexities of concussion diagnosis and management.8 This inherent ambiguity can lead to suboptimal recognition and awareness of concussion among clinicians, patients, families, school personnel, and sports staff, especially of its serious aftereffects in the pediatric patient.
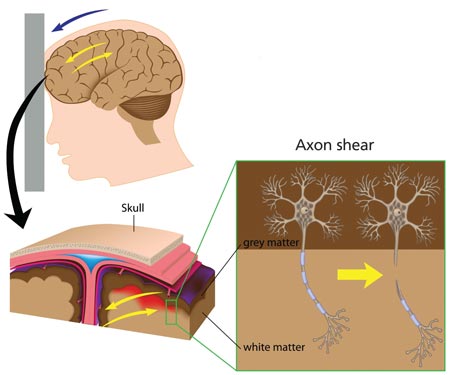
A blow to the head can propel the brain to strike one side of the skull and then bounce off the opposite side. This can damage or tear the axons—the signal transmitters of the neurons—from their cell bodies, disrupting brain cell communications and causing neurocognitive deficits.
While a concussion is a direct injury to the brain, it is also an evolving process comprised of several pathophysiologic components that are a consequence of biomechanical forces. The brain does not directly contact the skull but is surrounded by cerebrospinal fluid and fluid-filled vessels with a greater density than the brain itself. This intracranial space provides room for the brain to move upon impact by shifting and compressing from one side of the skull to the other.9 The concussive injury occurs as a result of either a direct strike to the head or from an indirect force traumatic enough to be transmitted to the brain. The strike or force produces a complex disturbance to the brain that, in most cases, does not result in loss of consciousness.3
THE GREATER VULNERABILITY OF THE PEDIATRIC BRAIN
Pathophysiology
For a concussion to occur, the biomechanical threshold at which nerve cells' adaptability is impeded must be crossed.10 This sets in motion a cascade of events, developing over minutes, hours, and even days, in which homeostasis is disrupted due to an imbalance of ionic, neuronal, metabolic, and pathophysiologic processes.5
While many studies have sought to explain the pathophysiology of pediatric sports-related concussions, much is still unknown. One hypothesis suggests that, after the injury, neuronal depolarization occurs, releasing excitatory neurotransmitters and altering metabolism by the immediate release of potassium. Restoration of homeostasis demands response by the sodium-potassium pump, requiring energy in the form of glucose. Coupled with axonal injury and alterations in cerebral blood flow, an imbalance between energy supply and demand occurs.5
Maugans et al found that a single pediatric concussion does not cause a structural or metabolic injury but instead a physiologic interruption—different from what occurs in adult concussions.10 They observed a statistically significant reduction in cerebral blood flow of more than 10% in a small group of postconcussion children, ages 11 to 15, compared with a control group. This alteration persisted for two weeks in two-thirds of the children and for up to a month in the remaining third.10 The delayed return of normal cerebral blood flow is believed to be a major contributing factor to pediatric concussion-related symptoms. However, little is known about the long-term effects of concussion on the developing brain.9
Crucial developmental years
Because the pediatric brain is still developing, children between the ages of 5 and 12 are at greater risk for sustaining a disruption in brain function from a concussion. In addition, this group is more susceptible in general to sports injuries compared to adults, because of their stage of growth and development.11
With a pediatric concussion, the individual child’s stage of brain development and the possible effects on his or her evolving neurocognitive functioning must be taken into account. Critical skills, such as language, emotion, memory, problem solving, and motor dexterity, emerge during childhood, and a disturbance during this time could have substantial consequences.12 Motor skills and primary senses usually mature by age 5, with language maturity occurring by age 10.9 However, many other vital skills and processes, such as emotion, judgment, and abstract reasoning, are not fully developed until adulthood. As a result, damage to cortical areas of the brain, such as the parietal lobe and frontal areas—involved in fine motor skills and complex thinking—can hinder or delay the development of these necessary processes.9
Many researchers suggest that, while a concussion to the developing brain may not significantly affect previously learned functions, it may notably delay development of new cognitive functions. As a result, recovery from a concussion during these years may be poorer.2,9,12
On the next page: Clinical presentation and post injury evaluation >>