A 26-year-old Hispanic woman presented to the emergency department (ED) with myalgia and weakness. The work-up revealed profound hyperthyroidism, with a TSH < 0.01 mIU/mL (normal, 0.4-4.2 mIU/L), potassium 2.4 mEq/L (normal, 3.7-5.2 mEq/L), hypophosphatemia, and low urinary potassium. There were no prior symptoms, and family history was negative for endocrinopathies. She was admitted and started on methimazole (10 mg bid) for thyroid suppression and given propranolol (10 mg bid) for anticipated hyperadrenergic adverse effects. The remainder of her hospital stay was uneventful, and she was discharged six days after admission. Soon after, an outpatient thyroid scan ordered by her primary care provider confirmed that the patient had Graves disease.
Eight months later, the patient returned to the ED with myalgia and rapidly progressing paralysis from the neck down; she was immediately intubated. Her potassium level was 1.2 mEq/L. An ECG revealed conduction abnormalities consistent with hypokalemia.
THE DIAGNOSIS
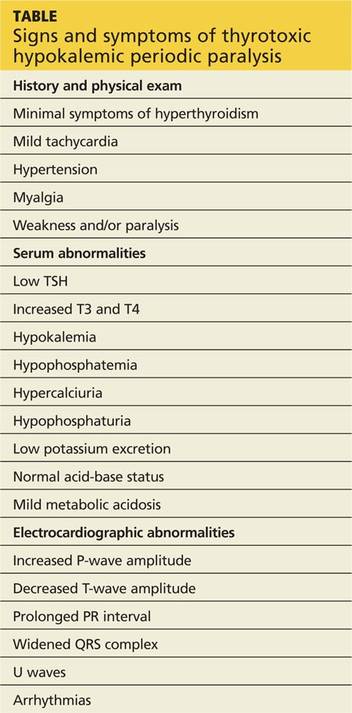
Based on the patient’s paralysis, hyperthyroidism, and hypokalemia, she was diagnosed with thyrotoxic hypokalemic periodic paralysis (THPP). This rare endocrinopathy causes electrolyte disturbances that can result in paralysis and lethal tachyarrhythmias.1-6
Patients with THPP typically have a history of myalgia, cramping, and stiffness followed by weakness or paralysis that tends to develop rapidly, most commonly in the late evening or early morning (see Table, below).1-9 Proximal muscles are predominantly affected symmetrically, and the attacks usually resolve over a period of hours to several days. Ocular, bulbar, and respiratory muscles are usually spared, but these can be affected by the hypokalemia.1
Continue for discussion of THPP >>