User login
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
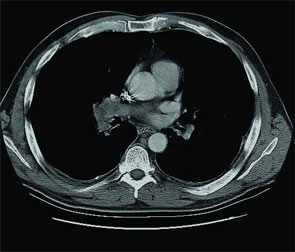
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5

Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5
Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5
Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.