User login
Despite a general understanding among hospitalists that malnutrition has severe negative effects on hospitalized patients, preventive or corrective measures often aren’t taken.
The ill effects of nutritional deficiency are particularly profound in elderly inpatients. Estimates of protein-energy malnutrition vary between 20%-78% of elderly medical patients, who are uniquely disposed to the cognitive, metabolic, and immune-mediating consequences of malnutrition.1
Most hospitalists know when to request a nutritionist consultation or order extra mealtime cans of Ensure. But many do not realize these efforts often do little to alter patients’ descent into nutritional deficiency.
Define the Problem
Four patterns of problematic eating have been described in elderly inpatients.
The first and most common is the patient who is permitted nothing by mouth and is not provided an alternate route of nutrition. Data show 44% of elderly malnourished inpatients fall into this category.2
Other abnormal feeding subgroups include patients who need to be fed but have no other eating problem, patients who refuse food but can swallow with difficulty, and those who aspirate liquid or solid food. In a study of 73 institutionalized patients with Alzheimer’s dementia, the latter subgroup accounted for 34% of the patients assessed.
Poor diet is the main source of protein-energy deficiency in elderly inpatients. Occult malabsorption secondary to bacterial overgrowth in the small intestine may also be an important factor, as is the increased catabolic state associated with acute illness.
Though the most at-risk patients have severe mental and physical incapacities, other problems including respiratory disease, gastrointestinal disease, and stroke are associated with a malnourished state.3
Though hospitalists generally acknowledge the potential seriousness of a patient developing nutritional deficits, the attending healthcare team may be slow to diagnose or manage this problem because:
- Elderly patients can be malnourished on admission, but classic signs of protein-energy deficiency are mistaken for normal signs of aging;
- Nutritional problems are observed by the medical staff, but aggressive treatment is deferred in light of seemingly more pressing medical issues;
- Many physicians take action to prevent nutritional deficiencies, but these interventions are often insufficient or ineffective in preventing the spiral into malnutrition; and
- Physicians may assume a nutritionist is working to prevent and treat nutritional deficiencies, while the nutritionist is waiting for the medical staff to address the problem with a feeding tube.
Clinical Outcomes
Most physicians have observed the declining physical and cognitive capabilities of a nutritionally deprived elderly inpatient.
Although a causal relationship between malnutrition and adverse events has not been established, this is most likely because an older person’s clinical course affects and is affected by his nutritional status. Further, frequently compromised homeostatic mechanisms make the risk of complications related to malnutrition potentially more severe.
Though researchers are studying how inadequate nutritional intake contributes to the risk of adverse outcomes in elderly inpatients, numerous studies have identified strong correlations between the severity of the nutritional deficit and the risk of subsequent morbid events.
Sullivan, et al., found in their 1999 study of protein-energy undernutrition among elderly hospitalized patients that those maintained on nutrient intakes far less than their estimated energy requirements were at more risk of in-hospital mortality.
Other studies have shown that the risk of in-hospital starvation correlates strongly with polypharmacy and long stay. The severity of the nutritional deficiency correlates not only with weight loss and secretory protein loss, but also the risk of in-hospital and long-term complications.
Who Needs Help
Basic nutritional requirements vary much less than might be expected among younger and older patients. However, while a malnourished 20-year-old can be easily identified, the classic signs of malnutrition (wasting, brittle hair, dry skin, fissured mucus membranes) are less easily detected in elderly patients. They are often mistaken for signs of normal aging. Questions that can elicit evidence of a protein-energy deficiency include:
- Has food intake decreased recently?
- Are there physical difficulties with eating?
- Is the patient confused or depressed?
- Has there been diarrhea or vomiting?
- Has the patient been able to shop and manage food preparation?
- Has the patient or family noticed weight loss?
- What does the patient regard as a normal weight?
However, because the clinical signs of malnutrition-weight loss, muscle wasting, and fatigue can be difficult to detect from history alone, use of an assessment tool is often necessary.
There is no simple diagnostic test for undernutrition. Measurements of albumin, prealbumin, body-mass index (BMI), and weight loss have been used, albeit problematically, for this purpose. More useful for the quantification of nutritional status in elderly outpatients, these measurements are difficult to use in the hospital because albumin levels are frequently affected by disease processes involving the liver, kidney, and immune system, and correct baseline weights and heights are notoriously difficult to obtain from elderly patients.4
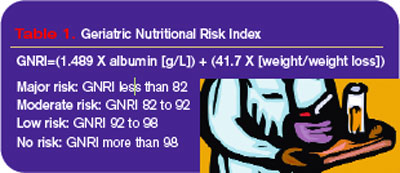
The Nutritional Risk Index was developed in response to these difficulties, but it was originally calibrated for young, post-surgical patients. Because of the problematic nature of obtaining the accurate heights and weights needed for the NRI in elderly patients, Bouillanne, et al,. developed the Geriatric Nutritional Risk Index (GNRI) in 2005 based on albumin levels, hospital recorded weights, and weight loss (see Table 1, above).
The GNRI’s creators classified patients according to their level of malnutrition and calculated their risk of related comorbidities. They found that 44% of their study population had major or moderate nutrition-related risk and recommended nutritional supplementation.
Path to Recovery
Refeeding regimens for elderly patients diagnosed as undernourished are best started with meals of personally chosen foods, timed for when patients are hungry.
Many elderly patients do not eat on a strict schedule at home and have difficulty complying with such a schedule. If oral intake remains inadequate, offer nutritional supplements. Because low-energy diets are usually low in vitamins and minerals, supplementation with a multivitamin, thiamine, folic acid, and zinc can be beneficial.
A common approach to problems with nutritional intake in elderly patients, particularly those with altered cognition or fluctuating consciousness, is insertion of a feeding tube.5 According to Medicare data from the 1990s, in individuals older than 85, one in 131 whites, and one in 58 African-Americans had a gastrostomy.
Despite the large numbers of feeding-tube placements in elderly patients, proof of their effectiveness is scant. No randomized trials have been performed to determine whether this practice improves survival, and observational data reveal that the one-year survival for these patients is less than 40%.
Feeding tubes are often placed to reverse the clinical sequelae of malnutrition—to heal pressure ulcers, prevent infection, and improve the patient’s functional status. But prospective observational studies do not support this methodology, and some contradictory evidence in the form of worsening pressure ulcers has been observed.
Aspiration pneumonia is the most serious infection for which tube feeding is considered a preventive measure. The condition results from the misdirection of pharyngeal contents and is believed to develop when nonpathologic oral secretions are deposited in dependent areas of the lung. The bacterial inoculum is high enough to overcome local defenses, which results in an infectious, febrile illness, usually involving mixed gram-negative rods and anaerobes.
Summaries of current data show that tube feeding may increase the risk of aspiration pneumonia. Further support for this hypothesis comes from the observation that jejunostomy feeding also does not appear to reduce the risk of aspiration pneumonia. If a patient is unable to protect his airway during mealtimes, he will also be at risk of aspiration and pneumonia between meals, regardless of how nutrition is delivered. TH
Dr. Landis is a rheumatologist and freelance writer.
References
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients. JAMA. 1999;281(21):2013-2019.
- Incalzi RA, Gemma A, Capparella O, et al. Energy intake and in-hospital starvation: a clinically relevant relationship. Arch Intern Med. 1996;156(4):425-429.
- Tierney A. Undernutrition and elderly patients. J Adv Nurs. 1995;23(2):228-236.
- Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777-783.
- Finucane T, Williams M. Tube feeding the demented patient: a review of the evidence. American Geriatrics Society Annual Scientific Meeting 2001.
Despite a general understanding among hospitalists that malnutrition has severe negative effects on hospitalized patients, preventive or corrective measures often aren’t taken.
The ill effects of nutritional deficiency are particularly profound in elderly inpatients. Estimates of protein-energy malnutrition vary between 20%-78% of elderly medical patients, who are uniquely disposed to the cognitive, metabolic, and immune-mediating consequences of malnutrition.1
Most hospitalists know when to request a nutritionist consultation or order extra mealtime cans of Ensure. But many do not realize these efforts often do little to alter patients’ descent into nutritional deficiency.
Define the Problem
Four patterns of problematic eating have been described in elderly inpatients.
The first and most common is the patient who is permitted nothing by mouth and is not provided an alternate route of nutrition. Data show 44% of elderly malnourished inpatients fall into this category.2
Other abnormal feeding subgroups include patients who need to be fed but have no other eating problem, patients who refuse food but can swallow with difficulty, and those who aspirate liquid or solid food. In a study of 73 institutionalized patients with Alzheimer’s dementia, the latter subgroup accounted for 34% of the patients assessed.
Poor diet is the main source of protein-energy deficiency in elderly inpatients. Occult malabsorption secondary to bacterial overgrowth in the small intestine may also be an important factor, as is the increased catabolic state associated with acute illness.
Though the most at-risk patients have severe mental and physical incapacities, other problems including respiratory disease, gastrointestinal disease, and stroke are associated with a malnourished state.3
Though hospitalists generally acknowledge the potential seriousness of a patient developing nutritional deficits, the attending healthcare team may be slow to diagnose or manage this problem because:
- Elderly patients can be malnourished on admission, but classic signs of protein-energy deficiency are mistaken for normal signs of aging;
- Nutritional problems are observed by the medical staff, but aggressive treatment is deferred in light of seemingly more pressing medical issues;
- Many physicians take action to prevent nutritional deficiencies, but these interventions are often insufficient or ineffective in preventing the spiral into malnutrition; and
- Physicians may assume a nutritionist is working to prevent and treat nutritional deficiencies, while the nutritionist is waiting for the medical staff to address the problem with a feeding tube.
Clinical Outcomes
Most physicians have observed the declining physical and cognitive capabilities of a nutritionally deprived elderly inpatient.
Although a causal relationship between malnutrition and adverse events has not been established, this is most likely because an older person’s clinical course affects and is affected by his nutritional status. Further, frequently compromised homeostatic mechanisms make the risk of complications related to malnutrition potentially more severe.
Though researchers are studying how inadequate nutritional intake contributes to the risk of adverse outcomes in elderly inpatients, numerous studies have identified strong correlations between the severity of the nutritional deficit and the risk of subsequent morbid events.
Sullivan, et al., found in their 1999 study of protein-energy undernutrition among elderly hospitalized patients that those maintained on nutrient intakes far less than their estimated energy requirements were at more risk of in-hospital mortality.
Other studies have shown that the risk of in-hospital starvation correlates strongly with polypharmacy and long stay. The severity of the nutritional deficiency correlates not only with weight loss and secretory protein loss, but also the risk of in-hospital and long-term complications.
Who Needs Help
Basic nutritional requirements vary much less than might be expected among younger and older patients. However, while a malnourished 20-year-old can be easily identified, the classic signs of malnutrition (wasting, brittle hair, dry skin, fissured mucus membranes) are less easily detected in elderly patients. They are often mistaken for signs of normal aging. Questions that can elicit evidence of a protein-energy deficiency include:
- Has food intake decreased recently?
- Are there physical difficulties with eating?
- Is the patient confused or depressed?
- Has there been diarrhea or vomiting?
- Has the patient been able to shop and manage food preparation?
- Has the patient or family noticed weight loss?
- What does the patient regard as a normal weight?
However, because the clinical signs of malnutrition-weight loss, muscle wasting, and fatigue can be difficult to detect from history alone, use of an assessment tool is often necessary.
There is no simple diagnostic test for undernutrition. Measurements of albumin, prealbumin, body-mass index (BMI), and weight loss have been used, albeit problematically, for this purpose. More useful for the quantification of nutritional status in elderly outpatients, these measurements are difficult to use in the hospital because albumin levels are frequently affected by disease processes involving the liver, kidney, and immune system, and correct baseline weights and heights are notoriously difficult to obtain from elderly patients.4
The Nutritional Risk Index was developed in response to these difficulties, but it was originally calibrated for young, post-surgical patients. Because of the problematic nature of obtaining the accurate heights and weights needed for the NRI in elderly patients, Bouillanne, et al,. developed the Geriatric Nutritional Risk Index (GNRI) in 2005 based on albumin levels, hospital recorded weights, and weight loss (see Table 1, above).
The GNRI’s creators classified patients according to their level of malnutrition and calculated their risk of related comorbidities. They found that 44% of their study population had major or moderate nutrition-related risk and recommended nutritional supplementation.
Path to Recovery
Refeeding regimens for elderly patients diagnosed as undernourished are best started with meals of personally chosen foods, timed for when patients are hungry.
Many elderly patients do not eat on a strict schedule at home and have difficulty complying with such a schedule. If oral intake remains inadequate, offer nutritional supplements. Because low-energy diets are usually low in vitamins and minerals, supplementation with a multivitamin, thiamine, folic acid, and zinc can be beneficial.
A common approach to problems with nutritional intake in elderly patients, particularly those with altered cognition or fluctuating consciousness, is insertion of a feeding tube.5 According to Medicare data from the 1990s, in individuals older than 85, one in 131 whites, and one in 58 African-Americans had a gastrostomy.
Despite the large numbers of feeding-tube placements in elderly patients, proof of their effectiveness is scant. No randomized trials have been performed to determine whether this practice improves survival, and observational data reveal that the one-year survival for these patients is less than 40%.
Feeding tubes are often placed to reverse the clinical sequelae of malnutrition—to heal pressure ulcers, prevent infection, and improve the patient’s functional status. But prospective observational studies do not support this methodology, and some contradictory evidence in the form of worsening pressure ulcers has been observed.
Aspiration pneumonia is the most serious infection for which tube feeding is considered a preventive measure. The condition results from the misdirection of pharyngeal contents and is believed to develop when nonpathologic oral secretions are deposited in dependent areas of the lung. The bacterial inoculum is high enough to overcome local defenses, which results in an infectious, febrile illness, usually involving mixed gram-negative rods and anaerobes.
Summaries of current data show that tube feeding may increase the risk of aspiration pneumonia. Further support for this hypothesis comes from the observation that jejunostomy feeding also does not appear to reduce the risk of aspiration pneumonia. If a patient is unable to protect his airway during mealtimes, he will also be at risk of aspiration and pneumonia between meals, regardless of how nutrition is delivered. TH
Dr. Landis is a rheumatologist and freelance writer.
References
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients. JAMA. 1999;281(21):2013-2019.
- Incalzi RA, Gemma A, Capparella O, et al. Energy intake and in-hospital starvation: a clinically relevant relationship. Arch Intern Med. 1996;156(4):425-429.
- Tierney A. Undernutrition and elderly patients. J Adv Nurs. 1995;23(2):228-236.
- Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777-783.
- Finucane T, Williams M. Tube feeding the demented patient: a review of the evidence. American Geriatrics Society Annual Scientific Meeting 2001.
Despite a general understanding among hospitalists that malnutrition has severe negative effects on hospitalized patients, preventive or corrective measures often aren’t taken.
The ill effects of nutritional deficiency are particularly profound in elderly inpatients. Estimates of protein-energy malnutrition vary between 20%-78% of elderly medical patients, who are uniquely disposed to the cognitive, metabolic, and immune-mediating consequences of malnutrition.1
Most hospitalists know when to request a nutritionist consultation or order extra mealtime cans of Ensure. But many do not realize these efforts often do little to alter patients’ descent into nutritional deficiency.
Define the Problem
Four patterns of problematic eating have been described in elderly inpatients.
The first and most common is the patient who is permitted nothing by mouth and is not provided an alternate route of nutrition. Data show 44% of elderly malnourished inpatients fall into this category.2
Other abnormal feeding subgroups include patients who need to be fed but have no other eating problem, patients who refuse food but can swallow with difficulty, and those who aspirate liquid or solid food. In a study of 73 institutionalized patients with Alzheimer’s dementia, the latter subgroup accounted for 34% of the patients assessed.
Poor diet is the main source of protein-energy deficiency in elderly inpatients. Occult malabsorption secondary to bacterial overgrowth in the small intestine may also be an important factor, as is the increased catabolic state associated with acute illness.
Though the most at-risk patients have severe mental and physical incapacities, other problems including respiratory disease, gastrointestinal disease, and stroke are associated with a malnourished state.3
Though hospitalists generally acknowledge the potential seriousness of a patient developing nutritional deficits, the attending healthcare team may be slow to diagnose or manage this problem because:
- Elderly patients can be malnourished on admission, but classic signs of protein-energy deficiency are mistaken for normal signs of aging;
- Nutritional problems are observed by the medical staff, but aggressive treatment is deferred in light of seemingly more pressing medical issues;
- Many physicians take action to prevent nutritional deficiencies, but these interventions are often insufficient or ineffective in preventing the spiral into malnutrition; and
- Physicians may assume a nutritionist is working to prevent and treat nutritional deficiencies, while the nutritionist is waiting for the medical staff to address the problem with a feeding tube.
Clinical Outcomes
Most physicians have observed the declining physical and cognitive capabilities of a nutritionally deprived elderly inpatient.
Although a causal relationship between malnutrition and adverse events has not been established, this is most likely because an older person’s clinical course affects and is affected by his nutritional status. Further, frequently compromised homeostatic mechanisms make the risk of complications related to malnutrition potentially more severe.
Though researchers are studying how inadequate nutritional intake contributes to the risk of adverse outcomes in elderly inpatients, numerous studies have identified strong correlations between the severity of the nutritional deficit and the risk of subsequent morbid events.
Sullivan, et al., found in their 1999 study of protein-energy undernutrition among elderly hospitalized patients that those maintained on nutrient intakes far less than their estimated energy requirements were at more risk of in-hospital mortality.
Other studies have shown that the risk of in-hospital starvation correlates strongly with polypharmacy and long stay. The severity of the nutritional deficiency correlates not only with weight loss and secretory protein loss, but also the risk of in-hospital and long-term complications.
Who Needs Help
Basic nutritional requirements vary much less than might be expected among younger and older patients. However, while a malnourished 20-year-old can be easily identified, the classic signs of malnutrition (wasting, brittle hair, dry skin, fissured mucus membranes) are less easily detected in elderly patients. They are often mistaken for signs of normal aging. Questions that can elicit evidence of a protein-energy deficiency include:
- Has food intake decreased recently?
- Are there physical difficulties with eating?
- Is the patient confused or depressed?
- Has there been diarrhea or vomiting?
- Has the patient been able to shop and manage food preparation?
- Has the patient or family noticed weight loss?
- What does the patient regard as a normal weight?
However, because the clinical signs of malnutrition-weight loss, muscle wasting, and fatigue can be difficult to detect from history alone, use of an assessment tool is often necessary.
There is no simple diagnostic test for undernutrition. Measurements of albumin, prealbumin, body-mass index (BMI), and weight loss have been used, albeit problematically, for this purpose. More useful for the quantification of nutritional status in elderly outpatients, these measurements are difficult to use in the hospital because albumin levels are frequently affected by disease processes involving the liver, kidney, and immune system, and correct baseline weights and heights are notoriously difficult to obtain from elderly patients.4
The Nutritional Risk Index was developed in response to these difficulties, but it was originally calibrated for young, post-surgical patients. Because of the problematic nature of obtaining the accurate heights and weights needed for the NRI in elderly patients, Bouillanne, et al,. developed the Geriatric Nutritional Risk Index (GNRI) in 2005 based on albumin levels, hospital recorded weights, and weight loss (see Table 1, above).
The GNRI’s creators classified patients according to their level of malnutrition and calculated their risk of related comorbidities. They found that 44% of their study population had major or moderate nutrition-related risk and recommended nutritional supplementation.
Path to Recovery
Refeeding regimens for elderly patients diagnosed as undernourished are best started with meals of personally chosen foods, timed for when patients are hungry.
Many elderly patients do not eat on a strict schedule at home and have difficulty complying with such a schedule. If oral intake remains inadequate, offer nutritional supplements. Because low-energy diets are usually low in vitamins and minerals, supplementation with a multivitamin, thiamine, folic acid, and zinc can be beneficial.
A common approach to problems with nutritional intake in elderly patients, particularly those with altered cognition or fluctuating consciousness, is insertion of a feeding tube.5 According to Medicare data from the 1990s, in individuals older than 85, one in 131 whites, and one in 58 African-Americans had a gastrostomy.
Despite the large numbers of feeding-tube placements in elderly patients, proof of their effectiveness is scant. No randomized trials have been performed to determine whether this practice improves survival, and observational data reveal that the one-year survival for these patients is less than 40%.
Feeding tubes are often placed to reverse the clinical sequelae of malnutrition—to heal pressure ulcers, prevent infection, and improve the patient’s functional status. But prospective observational studies do not support this methodology, and some contradictory evidence in the form of worsening pressure ulcers has been observed.
Aspiration pneumonia is the most serious infection for which tube feeding is considered a preventive measure. The condition results from the misdirection of pharyngeal contents and is believed to develop when nonpathologic oral secretions are deposited in dependent areas of the lung. The bacterial inoculum is high enough to overcome local defenses, which results in an infectious, febrile illness, usually involving mixed gram-negative rods and anaerobes.
Summaries of current data show that tube feeding may increase the risk of aspiration pneumonia. Further support for this hypothesis comes from the observation that jejunostomy feeding also does not appear to reduce the risk of aspiration pneumonia. If a patient is unable to protect his airway during mealtimes, he will also be at risk of aspiration and pneumonia between meals, regardless of how nutrition is delivered. TH
Dr. Landis is a rheumatologist and freelance writer.
References
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients. JAMA. 1999;281(21):2013-2019.
- Incalzi RA, Gemma A, Capparella O, et al. Energy intake and in-hospital starvation: a clinically relevant relationship. Arch Intern Med. 1996;156(4):425-429.
- Tierney A. Undernutrition and elderly patients. J Adv Nurs. 1995;23(2):228-236.
- Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777-783.
- Finucane T, Williams M. Tube feeding the demented patient: a review of the evidence. American Geriatrics Society Annual Scientific Meeting 2001.