User login
Firearms are the most common means of suicide in the United States, accounting for approximately 20,000 adult deaths annually,1 which is approximately two-thirds of the more than 32,000 gun-related fatalities each year in the United States. Of approximately 3,000 American children who are shot to death annually, one-third are suicides.1-4
Firearms are dangerous; it has been documented that even guns obtained for recreation or protection increase the risk of suicide, homicide, or injury.2,3 This problem has become a public health concern.3-8 Because most suicide attempts with firearms are fatal, psychiatrists have an interest in reducing such outcomes.1-8
Risk factors for suicide by firearm
Easy availability of a gun in the home, with ammunition present—especially a gun that is kept loaded and not locked up—is the one of the biggest risk factors for suicide by firearms.4 Unrestricted, quick access allows people who are impulsive little time to reconsider suicide. The risk presented by easy availability is magnified by dangerous concomitant intoxication (see below), distress, and lack of supervision (of children).
Alcohol consumption is associated with suicide. Approximately one-fourth of the people who commit suicide are intoxicated at the time of death.9 Alcohol use, especially binge drinking, is observed in an even larger percentage of suicide attempts than individuals using guns while sober.
Female sex. In recent years, gun use by women has increased, along with firearm-related suicide. Simply having a gun at home greatly increases the suicide rate for women.2-4
People with a history of high impulsivity, impaired judgment, violence, or psychiatric and neurologic disorders places people at greater risk of shooting themselves, especially those with depression, suicidal ideation, substance abuse, psychosis, or dementia.4
Older age, particularly men who live alone, increases the risk of suicide by firearms, especially in the context of chronic pain or other health problems. Gunfire is the most common means of suicide among geriatric patients of both sexes.8
Lethality. In general, suicide attempts with guns are more likely to be fatal than overdosing, poisoning, or self-mutilation.1,2 Most self-inflicted gunshot wounds result in death, usually on the day of the shooting.1,2
Evidence about these risk factors has led the American Medical Association and other health care groups to encourage physicians—in particular, psychiatric clinicians who focus on suicide prevention—to counsel patients about gun safety.
What can you do to minimize risk?
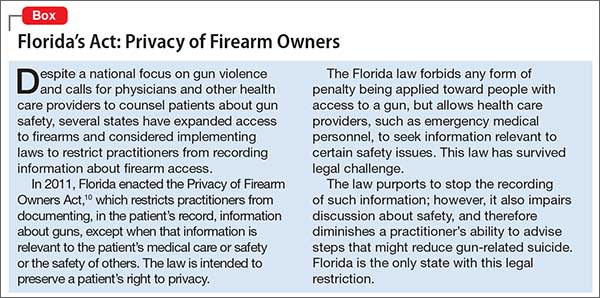
Gun-related inquiry and counsel by psychiatrists can benefit patients and their family.4 Be aware, however, of restrictions on such discussions by health care providers in some states (Box).10
Ask about the presence of firearms in the home. Our advice and our “doctor’s orders” are a means to promote health; suggestions in the context of a supportive physician-patient relationship could result in compliance.3,4 Firearm-focused discussions might be uncomfortable or unpopular but are critical for preventing suicide. Openly discussing such issues with our patients could avoid tragedies.4 Involving family or significant others in these interventions also might be helpful.
Ask about access to and storage of firearms. Simply talking about gun safety is helpful.4 Seeking information about gun usage is especially called for in psychiatric practices that treat patients with suicidal ideation, depression, substance abuse, and cognitive impairment.8 Discuss firearm availability with patients who have a history of substance use, impulsivity, anger, or violence, or who have a brain disorder or neurologic condition. Talking about firearms with patients and educating them about safety is indicated whenever you observe a risk factor for suicide.
Advise safe storage. Aim to have the entire family agree to a safety policy. Guns should be kept unloaded and not stored with ammunition (eg, keep guns in the attic and ammunition in the basement), which might diminish the risk of (1) an impulsive shooting and (2) a planned attempt by giving people time to consider options other than suicide. Firearm safety includes locking ammunition and weapons in a safe and applying trigger locks. Try to get patients and their family to plan for compliance with such recommendations whenever possible.
Guide dialogue and educate patients about handling guns safely. Be sure that patients know that most firearm deaths that happen inside a home are suicide.2-4 Advise patients, and their family, that firearms should not be handled while intoxicated.4 Encourage families to remove gun access from members who are suicidal, depressed, abusing pharmaceuticals or using illicit drugs, and those in distress or with a significant mental or neurologic illness.
In such circumstances, institute a protective plan to prevent shootings. This can be time-limited, or might include removing guns or ammunition from the home or deactivating firing mechanisms, etc. For safety reasons, some families do not keep ammunition in their home.
Additionally, firearms in the hands of children ought to include close monitoring by a responsible, sober adult. Keeping guns in locked storage is especially important for preventing suicide in children. Despite suicide being less frequent among younger people than in adults, taking steps to avoid 1,000 child suicides each year in the United States is a valuable intervention.
Conclusion
Specific inquiry, overt discussion, and face-to-face counseling about gun safety can be a life-saving aspect of psychiatric intervention. With such recommendations and education, psychiatrists can play a productive role in reducing firearm-related suicide.
1. Center for Disease Control and Prevention. Injury prevention and control: data and statistics. http://www.cdc.gov/injury/wisqars. Updated December 8, 2015. Accessed April 1, 2016.
2. Narang P, Paladugu A, Manda SR, et al. Do guns provide safety? At what cost? South Med J. 2010;103(2):151-153.
3. Cherlopalle S, Kolikonda MK, Enja M, et al. Guns in America: defense or danger? J Trauma Treat. 2014;3(4):207.
4. Lippmann S. Doctors teaching gun safety. Journal of the Kentucky Medical Association. 2015;113(4):112.
5. Cooke BK, Goddard ER, Ginory A, et al. Firearms inquiries in Florida: “medical privacy” or medical neglect? J Am Acad Psychiatry Law. 2012;40(3):399-408.
6. Valeras AB. Patient with gun. Fam Med. 2013;45(8):584-585.
7. Butkus R, Weissman A. Internists’ attitude toward prevention of firearm injury. Ann Intern Med. 2015;160(12):821-827.
8. Kapp MB. Geriatric patients, firearms, and physicians. Ann Intern Med. 2013;159(6):421-422.
9. Kaplan MS, McFarland BH, Huguet N, et al. Acute alcohol intoxication and suicide: a gender-stratified analysis of the National Violent Death Reporting System. Inj Prev. 2013;19(1):38-43.
10. Fla Stat §790.338.
Firearms are the most common means of suicide in the United States, accounting for approximately 20,000 adult deaths annually,1 which is approximately two-thirds of the more than 32,000 gun-related fatalities each year in the United States. Of approximately 3,000 American children who are shot to death annually, one-third are suicides.1-4
Firearms are dangerous; it has been documented that even guns obtained for recreation or protection increase the risk of suicide, homicide, or injury.2,3 This problem has become a public health concern.3-8 Because most suicide attempts with firearms are fatal, psychiatrists have an interest in reducing such outcomes.1-8
Risk factors for suicide by firearm
Easy availability of a gun in the home, with ammunition present—especially a gun that is kept loaded and not locked up—is the one of the biggest risk factors for suicide by firearms.4 Unrestricted, quick access allows people who are impulsive little time to reconsider suicide. The risk presented by easy availability is magnified by dangerous concomitant intoxication (see below), distress, and lack of supervision (of children).
Alcohol consumption is associated with suicide. Approximately one-fourth of the people who commit suicide are intoxicated at the time of death.9 Alcohol use, especially binge drinking, is observed in an even larger percentage of suicide attempts than individuals using guns while sober.
Female sex. In recent years, gun use by women has increased, along with firearm-related suicide. Simply having a gun at home greatly increases the suicide rate for women.2-4
People with a history of high impulsivity, impaired judgment, violence, or psychiatric and neurologic disorders places people at greater risk of shooting themselves, especially those with depression, suicidal ideation, substance abuse, psychosis, or dementia.4
Older age, particularly men who live alone, increases the risk of suicide by firearms, especially in the context of chronic pain or other health problems. Gunfire is the most common means of suicide among geriatric patients of both sexes.8
Lethality. In general, suicide attempts with guns are more likely to be fatal than overdosing, poisoning, or self-mutilation.1,2 Most self-inflicted gunshot wounds result in death, usually on the day of the shooting.1,2
Evidence about these risk factors has led the American Medical Association and other health care groups to encourage physicians—in particular, psychiatric clinicians who focus on suicide prevention—to counsel patients about gun safety.
What can you do to minimize risk?
Gun-related inquiry and counsel by psychiatrists can benefit patients and their family.4 Be aware, however, of restrictions on such discussions by health care providers in some states (Box).10
Ask about the presence of firearms in the home. Our advice and our “doctor’s orders” are a means to promote health; suggestions in the context of a supportive physician-patient relationship could result in compliance.3,4 Firearm-focused discussions might be uncomfortable or unpopular but are critical for preventing suicide. Openly discussing such issues with our patients could avoid tragedies.4 Involving family or significant others in these interventions also might be helpful.
Ask about access to and storage of firearms. Simply talking about gun safety is helpful.4 Seeking information about gun usage is especially called for in psychiatric practices that treat patients with suicidal ideation, depression, substance abuse, and cognitive impairment.8 Discuss firearm availability with patients who have a history of substance use, impulsivity, anger, or violence, or who have a brain disorder or neurologic condition. Talking about firearms with patients and educating them about safety is indicated whenever you observe a risk factor for suicide.
Advise safe storage. Aim to have the entire family agree to a safety policy. Guns should be kept unloaded and not stored with ammunition (eg, keep guns in the attic and ammunition in the basement), which might diminish the risk of (1) an impulsive shooting and (2) a planned attempt by giving people time to consider options other than suicide. Firearm safety includes locking ammunition and weapons in a safe and applying trigger locks. Try to get patients and their family to plan for compliance with such recommendations whenever possible.
Guide dialogue and educate patients about handling guns safely. Be sure that patients know that most firearm deaths that happen inside a home are suicide.2-4 Advise patients, and their family, that firearms should not be handled while intoxicated.4 Encourage families to remove gun access from members who are suicidal, depressed, abusing pharmaceuticals or using illicit drugs, and those in distress or with a significant mental or neurologic illness.
In such circumstances, institute a protective plan to prevent shootings. This can be time-limited, or might include removing guns or ammunition from the home or deactivating firing mechanisms, etc. For safety reasons, some families do not keep ammunition in their home.
Additionally, firearms in the hands of children ought to include close monitoring by a responsible, sober adult. Keeping guns in locked storage is especially important for preventing suicide in children. Despite suicide being less frequent among younger people than in adults, taking steps to avoid 1,000 child suicides each year in the United States is a valuable intervention.
Conclusion
Specific inquiry, overt discussion, and face-to-face counseling about gun safety can be a life-saving aspect of psychiatric intervention. With such recommendations and education, psychiatrists can play a productive role in reducing firearm-related suicide.
Firearms are the most common means of suicide in the United States, accounting for approximately 20,000 adult deaths annually,1 which is approximately two-thirds of the more than 32,000 gun-related fatalities each year in the United States. Of approximately 3,000 American children who are shot to death annually, one-third are suicides.1-4
Firearms are dangerous; it has been documented that even guns obtained for recreation or protection increase the risk of suicide, homicide, or injury.2,3 This problem has become a public health concern.3-8 Because most suicide attempts with firearms are fatal, psychiatrists have an interest in reducing such outcomes.1-8
Risk factors for suicide by firearm
Easy availability of a gun in the home, with ammunition present—especially a gun that is kept loaded and not locked up—is the one of the biggest risk factors for suicide by firearms.4 Unrestricted, quick access allows people who are impulsive little time to reconsider suicide. The risk presented by easy availability is magnified by dangerous concomitant intoxication (see below), distress, and lack of supervision (of children).
Alcohol consumption is associated with suicide. Approximately one-fourth of the people who commit suicide are intoxicated at the time of death.9 Alcohol use, especially binge drinking, is observed in an even larger percentage of suicide attempts than individuals using guns while sober.
Female sex. In recent years, gun use by women has increased, along with firearm-related suicide. Simply having a gun at home greatly increases the suicide rate for women.2-4
People with a history of high impulsivity, impaired judgment, violence, or psychiatric and neurologic disorders places people at greater risk of shooting themselves, especially those with depression, suicidal ideation, substance abuse, psychosis, or dementia.4
Older age, particularly men who live alone, increases the risk of suicide by firearms, especially in the context of chronic pain or other health problems. Gunfire is the most common means of suicide among geriatric patients of both sexes.8
Lethality. In general, suicide attempts with guns are more likely to be fatal than overdosing, poisoning, or self-mutilation.1,2 Most self-inflicted gunshot wounds result in death, usually on the day of the shooting.1,2
Evidence about these risk factors has led the American Medical Association and other health care groups to encourage physicians—in particular, psychiatric clinicians who focus on suicide prevention—to counsel patients about gun safety.
What can you do to minimize risk?
Gun-related inquiry and counsel by psychiatrists can benefit patients and their family.4 Be aware, however, of restrictions on such discussions by health care providers in some states (Box).10
Ask about the presence of firearms in the home. Our advice and our “doctor’s orders” are a means to promote health; suggestions in the context of a supportive physician-patient relationship could result in compliance.3,4 Firearm-focused discussions might be uncomfortable or unpopular but are critical for preventing suicide. Openly discussing such issues with our patients could avoid tragedies.4 Involving family or significant others in these interventions also might be helpful.
Ask about access to and storage of firearms. Simply talking about gun safety is helpful.4 Seeking information about gun usage is especially called for in psychiatric practices that treat patients with suicidal ideation, depression, substance abuse, and cognitive impairment.8 Discuss firearm availability with patients who have a history of substance use, impulsivity, anger, or violence, or who have a brain disorder or neurologic condition. Talking about firearms with patients and educating them about safety is indicated whenever you observe a risk factor for suicide.
Advise safe storage. Aim to have the entire family agree to a safety policy. Guns should be kept unloaded and not stored with ammunition (eg, keep guns in the attic and ammunition in the basement), which might diminish the risk of (1) an impulsive shooting and (2) a planned attempt by giving people time to consider options other than suicide. Firearm safety includes locking ammunition and weapons in a safe and applying trigger locks. Try to get patients and their family to plan for compliance with such recommendations whenever possible.
Guide dialogue and educate patients about handling guns safely. Be sure that patients know that most firearm deaths that happen inside a home are suicide.2-4 Advise patients, and their family, that firearms should not be handled while intoxicated.4 Encourage families to remove gun access from members who are suicidal, depressed, abusing pharmaceuticals or using illicit drugs, and those in distress or with a significant mental or neurologic illness.
In such circumstances, institute a protective plan to prevent shootings. This can be time-limited, or might include removing guns or ammunition from the home or deactivating firing mechanisms, etc. For safety reasons, some families do not keep ammunition in their home.
Additionally, firearms in the hands of children ought to include close monitoring by a responsible, sober adult. Keeping guns in locked storage is especially important for preventing suicide in children. Despite suicide being less frequent among younger people than in adults, taking steps to avoid 1,000 child suicides each year in the United States is a valuable intervention.
Conclusion
Specific inquiry, overt discussion, and face-to-face counseling about gun safety can be a life-saving aspect of psychiatric intervention. With such recommendations and education, psychiatrists can play a productive role in reducing firearm-related suicide.
1. Center for Disease Control and Prevention. Injury prevention and control: data and statistics. http://www.cdc.gov/injury/wisqars. Updated December 8, 2015. Accessed April 1, 2016.
2. Narang P, Paladugu A, Manda SR, et al. Do guns provide safety? At what cost? South Med J. 2010;103(2):151-153.
3. Cherlopalle S, Kolikonda MK, Enja M, et al. Guns in America: defense or danger? J Trauma Treat. 2014;3(4):207.
4. Lippmann S. Doctors teaching gun safety. Journal of the Kentucky Medical Association. 2015;113(4):112.
5. Cooke BK, Goddard ER, Ginory A, et al. Firearms inquiries in Florida: “medical privacy” or medical neglect? J Am Acad Psychiatry Law. 2012;40(3):399-408.
6. Valeras AB. Patient with gun. Fam Med. 2013;45(8):584-585.
7. Butkus R, Weissman A. Internists’ attitude toward prevention of firearm injury. Ann Intern Med. 2015;160(12):821-827.
8. Kapp MB. Geriatric patients, firearms, and physicians. Ann Intern Med. 2013;159(6):421-422.
9. Kaplan MS, McFarland BH, Huguet N, et al. Acute alcohol intoxication and suicide: a gender-stratified analysis of the National Violent Death Reporting System. Inj Prev. 2013;19(1):38-43.
10. Fla Stat §790.338.
1. Center for Disease Control and Prevention. Injury prevention and control: data and statistics. http://www.cdc.gov/injury/wisqars. Updated December 8, 2015. Accessed April 1, 2016.
2. Narang P, Paladugu A, Manda SR, et al. Do guns provide safety? At what cost? South Med J. 2010;103(2):151-153.
3. Cherlopalle S, Kolikonda MK, Enja M, et al. Guns in America: defense or danger? J Trauma Treat. 2014;3(4):207.
4. Lippmann S. Doctors teaching gun safety. Journal of the Kentucky Medical Association. 2015;113(4):112.
5. Cooke BK, Goddard ER, Ginory A, et al. Firearms inquiries in Florida: “medical privacy” or medical neglect? J Am Acad Psychiatry Law. 2012;40(3):399-408.
6. Valeras AB. Patient with gun. Fam Med. 2013;45(8):584-585.
7. Butkus R, Weissman A. Internists’ attitude toward prevention of firearm injury. Ann Intern Med. 2015;160(12):821-827.
8. Kapp MB. Geriatric patients, firearms, and physicians. Ann Intern Med. 2013;159(6):421-422.
9. Kaplan MS, McFarland BH, Huguet N, et al. Acute alcohol intoxication and suicide: a gender-stratified analysis of the National Violent Death Reporting System. Inj Prev. 2013;19(1):38-43.
10. Fla Stat §790.338.