Camilo Andrés Morales-Cardona, MD; Álvaro Andrés Luque-Acevedo, MD; Luis Fernando Bermúdez-Bula, MD
Drs. Morales-Cardona and Luque-Acevedo are from Centro Dermatológico Federico Lleras Acosta, Bogotá, Colombia. Dr. Bermúdez-Bula is from the School of Medicine, Universidad CES, Medellín, Colombia.
The authors report no conflict of interest.
Correspondence: Camilo Andrés Morales-Cardona, MD, Teaching and Research Office, Centro Dermatológico Federico Lleras Acosta, Ave 1, No 13A-61, Bogotá, Colombia (camiderm@yahoo.com).
Onychomatricoma is a subungual tumor that is clinically characterized by banded or diffuse thickening, yellowish discoloration, splinter hemorrhages, and transverse overcurvature of the nail plate. It is often and easily misdiagnosed because the condition is not well known and rarely has been described. We report the case of a 45-year-old man with a subungual tumor on the right index finger that fulfills the criteria of onychomatricoma.
Onychomatricoma has been described mostly in white individuals, but it can occur in all races and ethnic groups.
Onychomatricoma should be kept in mind in the differential diagnosis of subungual or periungual tumors.
Treatment of onychomatricoma is complete surgical excision.
References
Changes in the appearance of the nail apparatus can be produced by a variety of conditions. Onychomatricoma is an unusual benign tumor with specific clinical characteristics that was first described more than 2 decades ago.1 It is often and easily misdiagnosed because the condition rarely has been described. We report a case of onychomatricoma in a 54-year-old Colombian man who presented with a deformity of the nail plate on the right index finger that corresponded with the classic description of onychomatricoma. We emphasize the importance of reporting such lesions to prevent misdiagnosis and delay of proper treatment.
Case Report
A 54-year-old Colombian man presented with nail dystrophy involving the right index finger of 2 years’ duration. He did not recall any trauma prior to the onset of the nail abnormalities. Several topical treatments had previously been ineffective. Physical examination revealed a longitudinally banded thickening of the lateral half of the nail plate on the right index finger with yellowish brown discoloration, transverse overcurvature of the nail, longitudinal white lines, and splinter hemorrhages (Figure 1). Direct microscopy and fungal culture were performed to diagnose or rule out onychomycosis.
Figure 1. Clinically dystrophic nail with transverse overcurvature, thickening, yellow discoloration of the nail plate, longitudinal bands, and splinter hemorrhages on the right index finger.
A clinical diagnosis of onychomatricoma was made, and the lesion was surgically removed and sent for histopathologic study (Figure 2). The radial half of the nail plate was avulsed, and the proximal part of the removed nail plate contained a large, firmly attached, filamentous tumor arising from the nail matrix (Figure 3) with multiple fine filiform projections (Figure 4). The nail bed was cleaned with a curette to remove any debris, the ulnar half of the nail plate and nail bed was left in place, and the radial border was reconstructed. Histology confirmed the clinical diagnosis (Figure 5). No recurrences of the tumor were seen 36 months following surgery.
Figure 2. Macroscopic appearance of the removed nail plate and tumor.
Figure 3. Reflection of the proximal nail fold revealed projections arising from the nail matrix.
Figure 4. When bisected, the nail plate exhibited multiple channels formed by fine filiform projections.
Comment
Since the original report of this tumor,1 fewer than 10 cases of onychomatricoma have been reported in Latin America,2-5 with no more than 80 cases reported worldwide.6 Clinicians and academicians are becoming interested in the topic, which will result in better recognition and more reports in the literature.
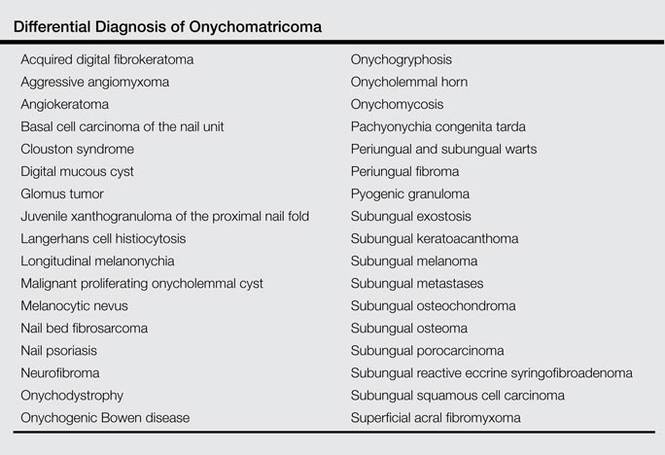
The clinical differential diagnosis of onycho-matricoma is extensive,7,8 but onychomatricoma has characteristic clinical and histopathologic features that allow its separation from other nail disorders and subungual tumors (Table).9 There are 4 cardinal clinical signs that suggest a diagnosis of onychomatricoma: (1) banded or diffuse thickening of the nail plate of variable widths; (2) yellowish discoloration of the involved nail plate, often showing fine splinter hemorrhages in the proximal nail portion; (3) transverse overcurvature of the nail; and (4) exposure of a filamentous tufted tumor emerging from the matrix in a funnel-shaped nail by avulsion.1
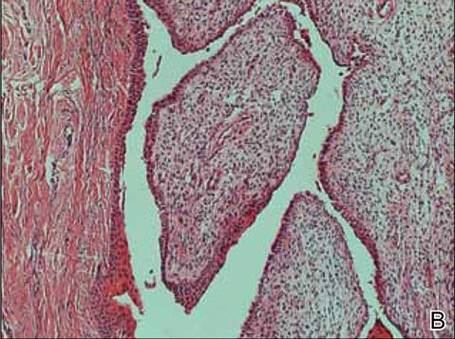
Figure 5. Histology revealed multiple filiform projections of dense connective tissue alternating with vertically oriented invaginations covered by nail matrix epithelium (A)(H&E, original magnification ×2.5). Papillomatous cellular fibrous tissue underlying nail matrix epithelium was noted (B)(H&E, original magnification ×10).
Histologic findings of onychomatricoma typically demonstrate a fibroepithelial tumor with a biphasic growth pattern mimicking normal nail matrix histology, including a proximal zone, which corresponds to the base of the fibroepithelial tumor, and a distal zone, which is composed of multiple epithelial digitations that extend into the small cavities present in the attached nail.10-12 Nevertheless, the anatomic tumor location, the often fragmented aspect of the tissue specimen, and the choice of the section planes may change the typical histologic features seen in onychomatricoma.13 Stromal prominence, cellularity, and atypia may vary in individual cases.10-12
The etiology of onychomatricoma is not yet known. Although it has been suggested that onychomatricoma could be an epithelial and connective tissue hamartoma simulating the nail matrix structure,1,10 the more recent concept of an epithelial onychogenic tumor with onychogenic mesenchyme will help to clarify its etiology because new histopathologic and immunohistochemical features suggest a neoplastic nature.14 On the other hand, predisposing factors such as trauma to the nail plate and onychomycosis may play a role,7 as the thumbs, index fingers, and great toes are more susceptible to onychomycosis and accidental trauma.
Conclusion
Our patient fulfilled the criteria of onychomatricoma.1 Onychomatricoma should be kept in mind in the differential diagnosis of subungual or periungual tumors to avoid misdiagnosis and erroneous treatments.