HOUSTON – Nearly 30% of trauma patients who were identified upon admission as being high risk for venous thromboembolism using a validated risk assessment tool went on to develop the thrombotic condition during their ICU stay, a study has shown.
Importantly, the deep vein thromboses in most of these patients were asymptomatic and might have gone undetected with potentially life-threatening consequences but for periodic ultrasound screening, Dr. Chad Thorson reported at the annual congress of the Society of Critical Care Medicine.
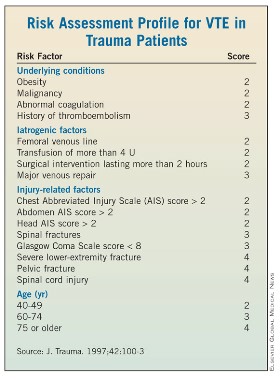
"Routine venous thromboembolism screening in the trauma population has been widely debated, and there currently is no protocol for it," according to Dr. Thorson of the Ryder Trauma Center at the University of Miami. Although the principal diagnostic screening tool – venous duplex ultrasound (VDU) – is not considered cost effective for screening all trauma patients, the investigators sought to determine whether prescreening trauma patients using the risk assessment profile (RAP) would yield a cohort of high- risk patients in whom increased vigilance and VDU screening are warranted (J. Trauma 1997;42:100-3).
Toward this end, all patients admitted to the Ryder Center’s level 1 trauma intensive care unit from November 2009 through January 2012 were prospectively screened with RAP, which stratifies an individual’s venous thromboembolism (VTE) risk based on underlying conditions, iatrogenic factors, injury-related factors, and age, within 24 hours of admission.
"Patients with [RAP] scores of 10 or higher received bilateral lower-extremity venous duplex ultrasounds at the time of admission and then weekly throughout their ICU stay," Dr. Thorson said, noting that logistic regression was performed on risk factors to identify independent predictors of VTE development. Among the risk factors considered were RAP score, RAP score higher than 20, femoral central venous catheterization for more than 24 hours, operative intervention duration longer than 2 hours, lower-extremity fracture, pelvic fracture, and spinal cord injury with paraplegia.
Of 534 trauma ICU admissions during the study period, 106 patients (mean age, 47 years) were identified as high risk based on their RAP score. Blunt trauma was the primary mechanism of injury in 79% of the population, and the mean injury severity score of the predominantly male (74%) high-risk population was 30, said Dr. Thorson.
Routine VDU screening identified 30 VTEs, including 20 that were asymptomatic and 10 that were symptomatic, despite the patients having received thromboprophylaxis (heparin 5,000 U every 8 hours or dalteparin 5,000 U daily), Dr. Thorson reported. Four of the symptomatic events were pulmonary emboli, and of the asymptomatic VTEs, six were identified on admission, seven were identified within the first week of admission, and four were identified within 2 weeks of admission, he said.
A comparison of those who did and did not develop VTEs showed significant differences in the number of risk factors, overall RAP score, and RAP score greater than 20, Dr. Thorson reported. Specifically, those in the non-VTE group averaged five risk factors compared with seven in the VTE group, and the respective median RAP scores were 14 and 19, he said. In addition, 6 patients in the non-VTE and 11 in the VTE group had RAP scores higher than 20. In the stepwise logistic regression analysis, RAP score and a combination of pelvic fracture and prolonged operative intervention were independent predictors of VTE development, he said.
Prescreening trauma patients with RAP is useful for identifying patients at increased risk of VTE who may be candidates for increased surveillance, according to Dr. Thorson. "There is plenty of debate with regard to the utility and cost effectiveness of routine screening, as well as the benefit of identifying asymptomatic deep vein thromboses," Dr. Thorson said in an interview.
Dr. Chad Thorson
"Ideally, we hope to find a decrease in the rate of pulmonary embolism as a result of screening, as this consequence can be devastating."
An important implication of the screening protocol, however, is identifying that DVT/VTE should not be included on the Centers for Medicare and Medicaid Services’ list of preventable complications (defined as errors in medical care that are clearly identifiable and preventable, and thus may no longer be eligible for reimbursement).
"A decision to no longer pay for [VTE] treatment could have devastating effects on many urban trauma centers," Dr. Thorson stressed.
The prescreening study was supported by grants from the Office of Naval Research and the U.S. Army Medical Research and Materiel Command. Dr. Thorson reported that he had no relevant financial disclosures.