User login
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.


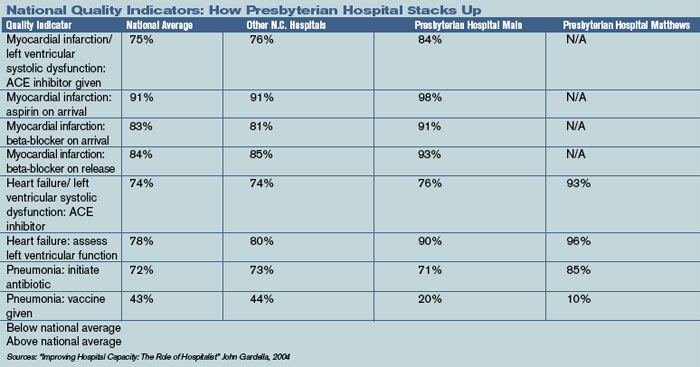
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.
Busy community physicians planted the seeds of Charlotte, N.C., Presbyterian Hospital’s hospitalist program in the late 1990s. The hospital, which anchors Novant Health’s presence in North Carolina’s Southern Piedmont region, is a 460-bed tertiary care hospital offering emergency, medical, surgical, and behavioral services.
Novant, the parent company, is a nonprofit healthcare system headquartered in Winston-Salem. Adjacent to Presbyterian Hospital and joined by skywalks is the Presbyterian Orthopedic Hospital. Two community hospitals, Presbyterian Hospital Matthews (10 miles south in suburban Charlotte) and Presbyterian Hospital Huntersville (16 miles north and close to an interstate) complete the Charlotte Presbyterian Hospital system.
By 1997 Charlotte’s population was growing so quickly its office-based physicians struggled to cover night calls or leave their office practices during the day to admit patients to the hospital. Presbyterian Hospital answered by forming an Inpatient Management Team (IMT) of five hospitalist internists to handle admissions for community internists from 5 p.m. to 7 a.m. Monday through Friday and on weekends.
While the internists delegated admissions to the IMT, they subsequently managed their own patients. Family practitioners, on the other hand, usually delegated the care of their inpatients to the IMT from admission to discharge. Steven Wallenhaupt, MD, and Presbyterian’s executive vice president of medical affairs says that the evening hours overwhelmed local physicians—particularly those who had moved to the Charlotte area for a decent lifestyle.
“It’s really not all about the money—either for the hospitalists or community doctors,” he explains. “It’s about wanting to have a good life and to practice good medicine.”
Mary Le-Bliss, MD, a Presbyterian Hospital clinical director, was one of the original IMT hospitalists. She explains what happened next, in 1999. “Three of the IMT physicians weren’t happy. They felt we were just running an admitting service,” she says. “They wanted something bigger—to manage patients throughout their stay—so they resigned.”
That was a wake-up call. While some community physicians still resisted turning over their patients completely to the hospitalists, a large majority decided to work with the hospitalists. The two groups of physicians (community-based and inpatient) found ways to coexist, hammering out a written agreement that community doctors sign to empower Presbyterian’s hospitalists to follow their hospitalized patients.
“It was nothing out of their pockets, they had an affiliation and the hospitalists got what they wanted,” notes Dr. Wallenhaupt.
So in1999 a new hospitalist program was born—the Presbyterian Inpatient Care Services (PICS) team, replacing its predecessor, IMT. PICS started with eight internists providing 24/7 coverage at Presbyterian Hospital and the adjacent Presbyterian Orthopedic Hospital. In April 1999 PICS expanded to the Matthews campus, where, for the first six months, the Matthews hospitalists worked 6 a.m. to 6 p.m. shifts, with the community physicians covering after hours.
By fall 1999 the PICS team at Matthews had grown to four physicians, enabling its own 24/7 coverage. In November 2004 when Presbyterian opened a community hospital in Huntersville, its PICS team provided 24/7 coverage of from the beginning.
Since early 1999 PICS has grown to 43 staff providers plus moonlighters, offering 24/7 coverage at the four hospitals. PICS maintains coverage agreements with approximately 330 primary care physicians, and provides consulting services for specialists throughout the South Piedmont region
To enhance communication, PICS providers leave voice messages summarizing the patients’ hospital stay with the primary at the time of patient admission and discharge. Additionally, most of the primary care practices have access to the hospital information system, including all notes dictated at the hospital as soon as they are transcribed.
Room to Roam
One of the hospitalist movement’s greatest contributions to the practice of medicine is its ability to spur innovation. Because hospitalists spend their work lives in hospitals, they can diagnose what has to be done to make things work better and implement new programs and processes to do that.
John Gardella, MD, MBA, of the Presbyterian Hospital Matthews PICS team, a transplant from New York to Charlotte in 1979, and the self-described “old man of the hospitalist team,” has done just that at Presbyterian. Dr. Gardella and other leaders stimulated development of orthopedic hospitalists, stroke center hospitalists, the nocturnist program (the 11 p.m. to 7 a.m. shift), and many best practices and order sets.
Dr. Gardella cites the work of hospitalist Jeanne Huddleston, MD, at the Mayo Clinic as the inspiration for Presbyterian’s orthopedic hospitalist program.
“The way she was managing comorbidities encouraged us to try to clone the program here and address the many needs of our elderly orthopedic patients,” says Dr. Gardella.
In August 2003, Presbyterian Orthopedic Hospital opened a preoperative service directed by Sarah Reynolds, MD. Now, with support from the referring orthopedic surgeons, the PICS team handles perioperative situations such as diabetes, hypertension, sleep medication, urinary incontinence and antibiotic prescriptions.
Also in 2003 the hospital added a PICS neurology team. (See “Hospitalist Specialist—the PICS Neurology Team,” left.)
A Balanced Life
Presbyterian Hospital’s administrators realized that providing a decent lifestyle for hospitalists, one that allowed doctors to have adequate free time and to provide quality care, was essential to avoiding stress and burnout. Dr. Wallenhaupt says that compensation is based on Medical Group Management Association salary recommendations plus incentives for productivity (relative value units). Shortened hours such as the nocturnist shift, which is an eight-hour rather than the usual 12-hour shift for the same pay, compensates for the inconveniences of night duty.
Vital to the PICS team’s success is a manageable caseload for each physician. While it may seem obvious that a reasonable average daily census would result in better patient care and reduced length of stay, Dr. Gardella has documented the correlation between the two (see chart below):
In pursuit of a balanced life, all hospitalist-internists work one week on followed by one week off (generally in 12-hour shifts) and can voluntarily moonlight during their week off. To help ease the workload during the emergency department’s busiest time, another physician works from 2 p.m. to midnight, handling admissions and consultations from the emergency department and the medical-surgical units, as well as phone consultations with community physicians. During the day nurses, nurse practitioners, and physicians assistants help with admissions, rounds, discharge planning, patient education, and follow-up with primary care physicians.
Solving one of medicine’s biggest headaches—night coverage—Presbyterian recruited Floyd Hale, MD, and Peter Le, MD, as nocturnists. In addition, moonlighters are recruited to work a short night shift from 6 p.m. to midnight, assisting with emergency department admissions when things get hectic.
At the community hospitals in Matthews and Huntersville, the PICS teams admit and manage the majority of the medical cases and provide consultation for the emergency department and the specialists on staff. The Matthews and Huntersville PICS teams also provide code blue and ICU coverage. Because the PICS MDs in the community hospitals are responsible for patient management and consultation in the ICU, all the physicians are expected to receive certification in the fundamentals of critical care and life support.
Financial Performance, Quality
Financially, the PICS team has been a boon to the hospital system. Gross patient revenue generated by the team grew from $2.2 million in 1999 to nearly $8 million in 2004, representing 28% compound annual growth. Over the same time period, operating expenses grew from $1.8 million to $4.5 million, representing 20% compound annual growth. Administrative support of the PICS team has actually dropped from $1.8 million or 32% of gross revenue in 1999 to $971,000 in 2004.
The PICS team has boosted revenues by reducing average length of stay, from .83 days for all patients and 1.36 days for Medicare diagnosis-related groups. Dr. Gardella calculated that reducing length of stay allows the hospitals to handle 1,300 more cases a year, which brought in an additional $10.4 million last year.
Although the PICS cadre is more than 40 strong, team members are well connected to improve efficiency and reduce wasted time. E-mails, an intranet, team leaders disseminating order sets and guidelines, and lunch-and-learn educational programs sponsored by vendors keep everyone informed. Small teams meet over lunch once a week, while the entire PICS team meets monthly to discuss business over pizza.
Presbyterian Hospital has long tracked clinical as well as financial metrics, and it compares favorably with other national and regional hospitals.
Publicly available data from CMS show that comparison. (See “National Quality Indicators: How Presbyterian Hospital Stacks Up,” p. 24.)
With care quality now reported so openly, Presbyterian Hospital’s administration, in conjunction with PICS leaders, is revising the PICS compensation package, which is now a combination of fixed salary plus productivity relative value units. The leaders are attempting to create financial incentives for order set usage and compliance with core measures.
At present, the PICS team manages about 70% of the internal medicine admissions at Presbyterian Hospital, and nearly all the medical cases at the Matthews and Huntersville sites. It is anticipated that the trend toward using hospitalists for inpatient management will continue. Further, it is likely that all orthopedic patients, or at least those with comorbidities, will be comanaged by the PICS team and their referring physicians.
Checklist for Change
The PICS team is instrumental in leading patient safety and quality improvement initiatives throughout the Charlotte, N.C., Presbyterian system. Among the operational improvement initiatives:
- Developing order sets in anticipation of computerized physician order entry;
- Working with the Institute of Healthcare Improvement’s 100,000 Lives Campaign. In particular assisting with the development of a medical response team and with medication reconciliation (www.ihi.org, click on “100,000 lives campaign”);
- Improving the care of hospitalized diabetics via participation in VHA’s Project Diabetes (VHA is a national alliance of nonprofit healthcare providers based in Irving, Texas);
- Helping develop a direct admission unit to reduce emergency department workload while providing better service for patients;
- Working with nursing to create a more team-oriented approach to inpatient management; and
- Working with the Operation Improvement group on initiatives to improve throughput.
Conclusion
Charlotte’s Presbyterian Hospital hospitalist program has grown rapidly. From its inception as an admitting service for busy community physicians, through an inpatient management team at the main hospital, to a group that now covers three hospitals and has specialists in orthopedics and neurology, the PICS team has learned to manage change and to grow successfully. More than 40 strong, they’re well equipped to keep pursuing the quest for quality, both at the hospital and as part of a national effort. TH
Writer Marlene Piturro is based in New York.