User login

The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
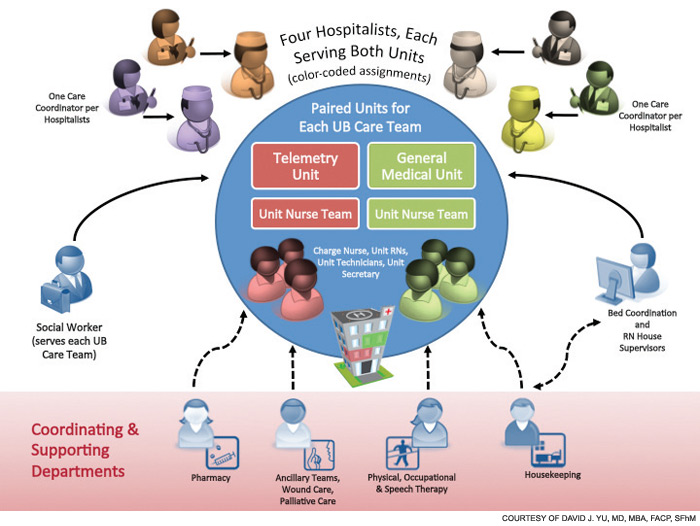
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.

Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.
The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.
Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.
The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.
Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.