Drs. Dabiri, Goreshi, Fischer, and Iwamoto are from the Department of Dermatology, Roger Williams Medical Center, Providence, Rhode Island. Dr. Tiger is the Department of Dermatology, Lahey Hospital & Medical Center, Burlington, Massachusetts.
The authors report no conflict of interest.
This case was part of a presentation at the 8th Cosmetic Surgery Forum under the direction of Joel Schlessinger, MD; November 30-December 3, 2006; Las Vegas, Nevada. Dr. Dabiri was a Top 10 Fellow and Resident Grant winner.
Correspondence: Ganary Dabiri, MD, PhD, 50 Maude St, 1st Floor, Department of Dermatology, Providence, RI 02908 (ganary.dabiri@chartercare.org).
Acute wounds created by dermatologists following the removal of nonmelanoma skin cancers are closed either by primary or secondary intention, and the best cosmetic outcome is preferentially desired. One parameter that determines the overall cosmesis of the healed wound is its vascularity. Vascular tone results from a complex interplay of a variety of chemokines in the body and their interaction with receptors located on endothelial cell surfaces. In this study, our aim was to determine if topical timolol could improve the overall cosmesis of acute surgical wounds. We determined that patients who treated their acute surgical wounds with topical timolol had improved cosmesis compared to control.
Dermatologists create acute surgical wounds on a daily basis. We should strive for excellent patient outcomes as well as the most desirable cosmetic result. This research article points to a possible new application of a longstanding medication to improve the cosmetic outcome in acute surgical wounds.
References
Timolol is a nonselective β-adrenergic receptor antagonist indicated for treating glaucoma, heart attacks, hypertension, and migraine headaches. It is made in both an oral and ophthalmic form. In dermatology, the beta-blocker propranolol is approved for the treatment of infantile hemangiomas (IHs). The exact mechanism of action of beta-blockers for the treatment of IHs is not yet completely understood, but it is postulated that they inhibit growth by at least 4 distinct mechanisms: (1) vasoconstriction, (2) inhibition of angiogenesis or vasculogenesis, (3) induction of apoptosis, and (4) recruitment of endothelial progenitor cells to the site of the hemangioma.1
Scar cosmesis can be calculated using the visual analog scale (VAS), which is a subjective scar assessment scored from poor to excellent. The multidimensional VAS is a photograph-based scale derived from evaluating standardized digital photographs in 4 dimensions—pigmentation, vascularity, acceptability, and observer comfort—plus contour. It uses the sum of the individual scores to obtain a single overall score ranging from excellent to poor.2 In this study, we sought to determine if the use of topical timolol after excision or Mohs micrographic surgery (MMS) treatment of nonmelanoma skin cancers improved the overall cosmesis of the scar.
Methods
The study protocol was approved by the institutional review board at Roger Williams Medical Center (Providence, Rhode Island). Eligibility criteria included patients who required excision or MMS for their nonmelanoma skin cancer located below the patella and those who agreed to allow their wounds to heal by secondary intention when given options for closure of their wounds. Patients were randomized to either the timolol (study medication) group or the saline (placebo) group. The initial defects were measured and photographed. Patients were educated on how to apply the study medication. All patients were prescribed 40 mm Hg compression stockings to wear following application of the study medication. Patients were asked to return at 1 and 5 weeks postsurgery and then every 1 to 2 weeks for wound assessment and measurement until their wounds had healed or at 13 weeks, depending on which came first. A healed wound was defined as having no exudate, exhibiting complete reepithelialization, and being stable for 1 week.
Healed wounds were assessed by a blinded outside dermatologist who examined photographs of the wounds and then completed the VAS for each participant’s scar.
Results
A total of 9 participants were enrolled in the study. Three participants were lost to follow-up; 6 completed the study (4 females, 2 males). The mean age was 70 years (age range, 46–89 years). The average wound size was 2×2 cm with a depth of 1 mm. Three participants were in the active medication group and 3 were in the control group.
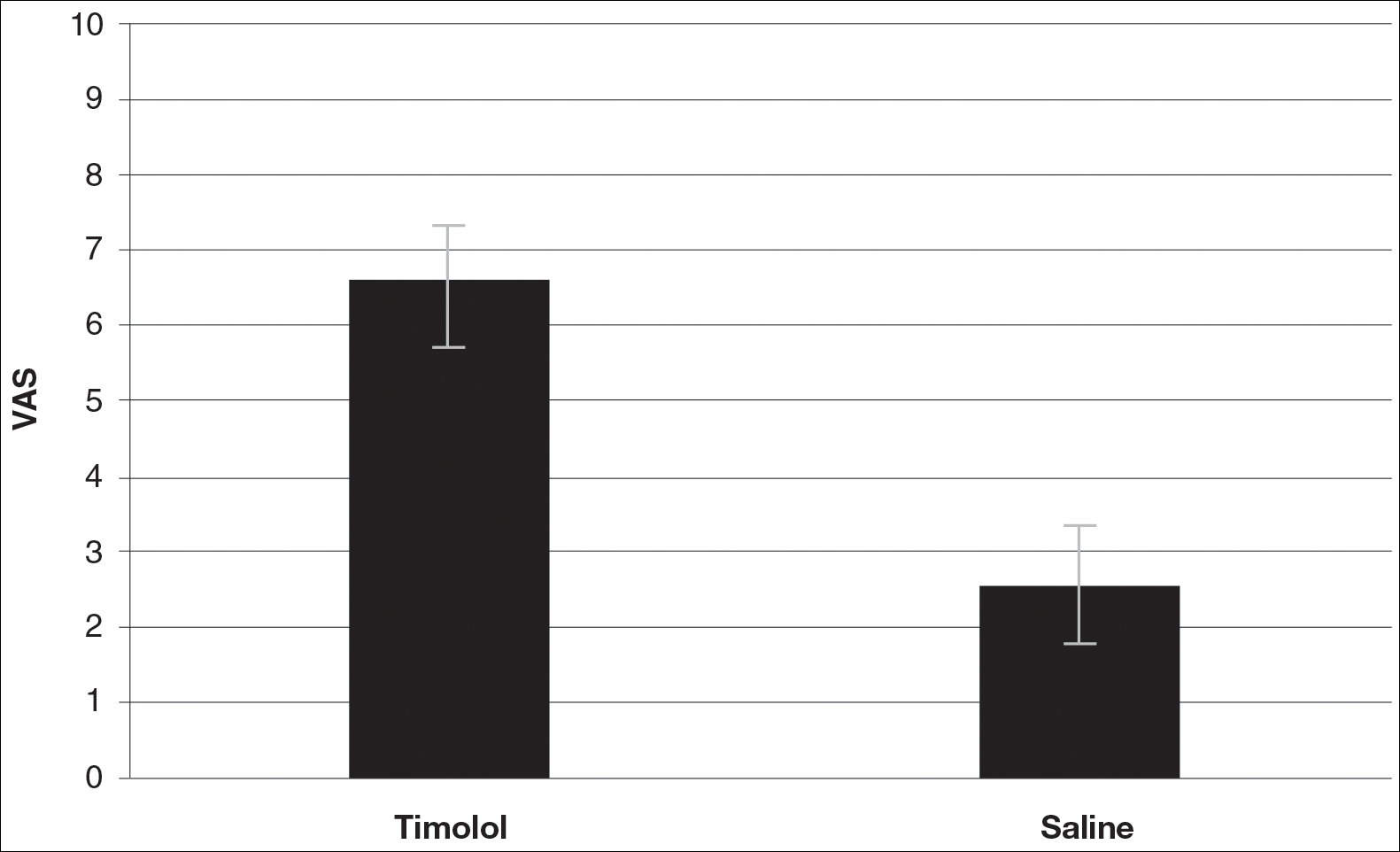
A VAS was completed for each participant’s scar by an outside blinded dermatologist. Based on the VAS, wounds treated with timolol resulted in more cosmetically favorable scars (scored higher on the VAS) compared to control (mean [SD]: 6.5±0.9 vs 2.5±0.7; P<0.05). See Figures 1 and 2 for representative results.
Figure 1. Topical timolol had a higher visual analog scale score compared to control (saline)(measure from poor to excellent).
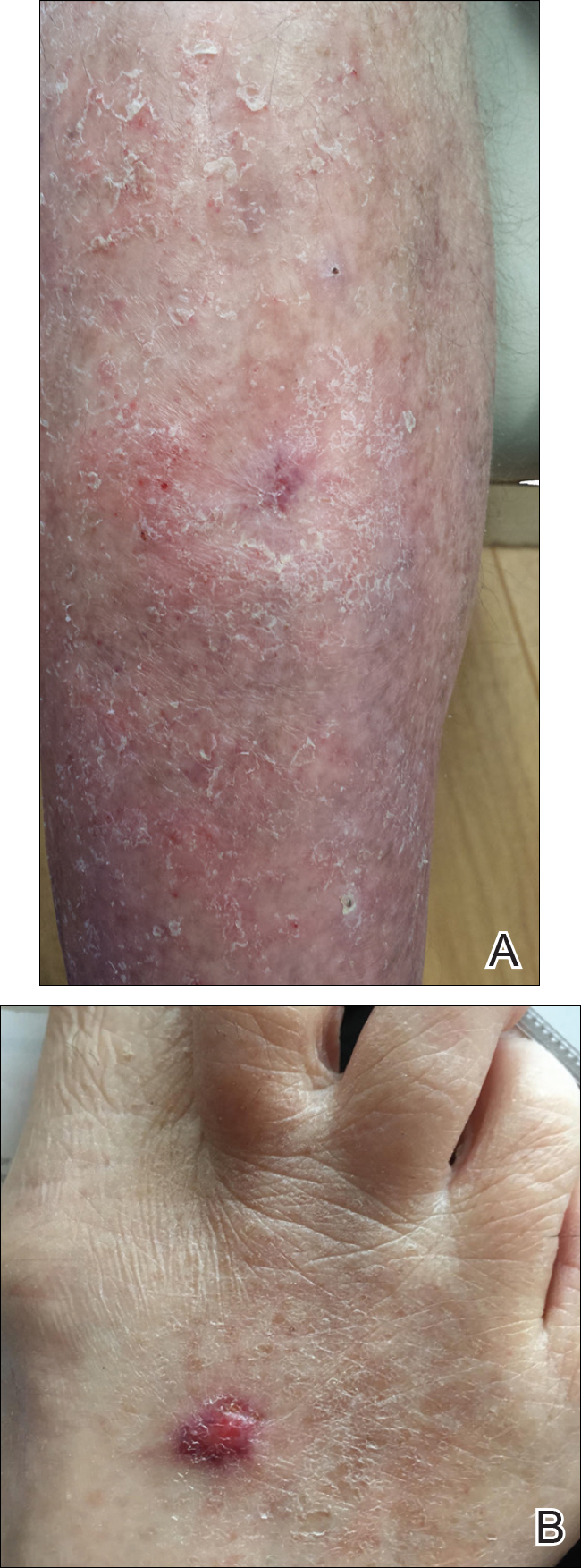
Figure 2. Wounds treated with topical timolol (A) had a more cosmetically favorable result compared to control (B).