The results of patch testing with routine screening series of allergens in North America have been the basis for a number of published reports.1 Similar information on supplemental series of allergens is not as readily available. This report reviews the experience of one dermatologist with supplemental allergens from 1990 to mid-1998. Just as the configuration of the screening series of allergens used by the North American Contact Dermatitis Group (NACDG) changes to reflect the latest information on specific allergens, the composition of these commercially available series of allergens has also evolved over the past 10 years. This report examines the merits of such supplemental series over this period of time, while attempting to identify the allergens most likely to enhance the information gathered by the TRUE test screening system.
Methods
Supplemental allergens were added to the patch tests applied to patients seen at Ochsner Clinic from January 1990 to July 1998, based on clinical history. All patients received the screening series of the NACDG, but only about one-third of patients were tested with supplemental allergens.2 A total of 657 supplemental series were used during this period (about six per month). Twelve series of supplemental allergens were purchased from a single source, Chemotechnique (Dormer Laboratories, Pointe-Claire, Quebec, Canada), and a plant-vegetation series was assembled from allergens obtained from Bjorn Hausen, MD, and Hermal (Omniderm/Pharmascience, Montreal, Canada). The series thus available for testing were: Cosmetic; Textile and Dyes; Methacrylate; Plastic and Glues; Plants; Dental; Hair-dressing; Sunscreen; Oil and Coolant; Photographic; Isocyanates; and Bakers.
A patch test that was scored +1, +2, or +3 according to the criteria of the NACDG1 was considered positive for purposes of data in this paper. Doubtful reactions were considered negative.
Results
The frequency of use of each series and the number of positive reactions are found in Table I. The raw data can be misleading as to the utility of the information obtained by use of a series, since allergens are included that are also present in the commonly employed screening series. This redundant information is also identified in Table I. A special circumstance occurs within the cosmetic series that contains octyl gallate, dodecyl gallate, and propyl gallate. Although these substances frequently induce delayed positive reactions and account for a total of 37 reactions, the data have been treated as “redundant,” since not one of these reactions was relevant. This specific point is needed to place the value of the cosmetic series in proper perspective.

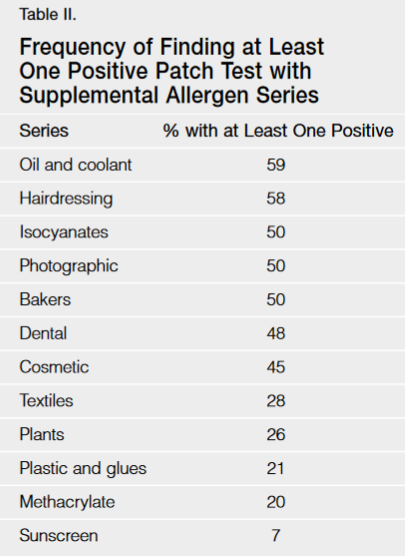
Table II shows the percentage of patients who had a positive test to at least one substance for each of the supplemental series. Table II was constructed using uncorrected data and is more a reflection of how easily or how well the history and the supplemental allergens can be correctly linked. For example, the history that an individual was a hairdresser readily linked to positive reactions on the hairdressing series 58% of the time. This may also partially reflect on how well the supplemental series is constituted. It also reflects on the ability of the physician to take a proper history and intelligently select appropriate allergens for testing.
Discussion
The unique features of each series of supplemental allergens represent its strengths and weaknesses.
Cosmetic Series — On the surface, this appears to be an important series. It was the one most frequently used and reflects the concerns of both patient and physician that a cosmetic may be the underlying cause of contact dermatitis. This heightened concern is supported by the study of the NACDG. These experts were surprised to find that in about half the cases in which a cosmetic was the source of dermatitis, it was unsuspected.3 However, slightly more than half of the patch test results produced by this series were either worthless or redundant to information obtained by the allergens on the screening series. If the gallates, redundant information, and thimerosal are eliminated, 86 of the reactions would not be recorded, leaving only 43 reactions in 177 people tested. The most frequent response becomes Amerchol L101 with 14 reactions. This links to lanolin sensitivity, and it is unclear whether this substance overstates the likelihood of clinical lanolin allergy as compared with the screening substance: wool wax alcohol. Next most frequent was cocamidopropyl betaine, with six reactions.
The overall utility of this series is disappointing. The NACDG study on cosmetics referred to above found fragrances and preservatives to be the most important cosmetic allergens. The TRUE test system lacks several of the more important preservatives identified in the most recent NACDG report.1 These are imidazolidinyl urea, diazolidinyl urea, and DMDM hydantoin. These three formaldehyde-releasing preservatives are a good supplement to the TRUE test series. The compound 2-bromo-2-nitropropane-1,3-diol (Bronopol), which is also a formaldehyde-releasing preservative, was not included as a recommendation because it is not widely used in marketed products.4
Textiles and Dyes — In this second most utilized series, none of the allergens is redundant with commonly used screening series. Textile finishes produced the bulk of the reactions recorded, and there are six of them in the series. They are (in order of frequency of reaction) dimethylol propylene urea (16 reactions), dimethylol dihydroxyethylene urea (14 reactions), urea formaldehyde (13 reactions), melamine formaldehyde (13 reactions), tetramethylol acetylenediurea (13 reactions), and ethylene urea melamine formaldehyde mix (9 reactions). These substances usually react in concert, which supports the recommendation that the first two allergens mentioned should be a sufficient screen for textile finish. The dyes reacted less often than the finishes. The dye that most frequently produced a reaction was disperse orange 3 (6 reactions). All of the individuals with positive reactions were also sensitive to paraphenylenediamine, and this likely represents a cross-reaction of uncertain relevance. The next most common allergenic dye was disperse blue 124 (4 reactions). The dye reactions do not lend themselves well to screening with one single or a few substances; if this is a serious consideration, the full series is recommended.
Methacrylate — The allergens of this series and those of the screening series do not overlap. While only 20% of those tested proved positive to at least one allergen, the 119 reactions indicate the multiple positive tests usually found in individuals sensitive to acrylates. A smaller series for screening purposes would be desirable and has been proposed to consist of ethyl acrylate (EA), hydroxyethyl acrylate (HEA), ethylene glycol dimethacrylate (EGDMA), triethylene glycol diacrylate (TEGDA), and alpha ethyl cyanoacrylate.5 Others have suggested hydroxypropyl methacrylate (HPMA), HEA, and hydroxyethyl methacrylate (HEMA).6 The top three allergens on the methacrylate series as used in New Orleans proved to be HEMA (13 reactions), HPMA (11 reactions), and EGDMA (9 reactions). Both HEMA and EGDMA also proved useful on the dental series, and are recommended for screening purposes. Results in New Orleans of the screening series recommended by the Oregon group5 were: EA (3 reactions), TEGDA (7 reactions), alpha ethyl cyanoacry-late (not tested), and a point of agreement, EGDMA (9 reactions). The acrylates recommended by the group in Finland scored as follows in New Orleans: HEA (6 reactions), HPMA (7 reactions), and a point of agreement, HEMA (13 reactions).
Plastic and Glue — This series, the fourth most commonly used supplemental series, was seldom helpful. This was probably because of my high index of suspicion and a low incidence of allergy to these materials. The most frequent reaction was to abitol (3 reactions). This series or any of the individual allergens are not recommended for most dermatologists. The cases of plastic or glue allergy documented by this series were all somewhat idiosyncratic, and those cases require the full series.
Plants — The group of plant allergens proved to be very idiosyncratic. Trends did not emerge. The top three allergens—carnation, sunflower, and yarrow—each produced five reactions. An ideal panel of allergens to screen for vegetation-induced contact dermatitis has not yet been developed.
Dental — The dental series covers two important areas: acrylates and dental metals. Negative reactions with this series are just as helpful to our dental colleagues as the positive reactions. For that reason, the full series is recommended to those seriously interested in working with patients with suspected reactions to dental materials. If a condensed version is required, the highest yield of positive reactions (excluding redundant results) came from HEMA, EGDMA, mercury, palladium, and gold sodium thiosulfate.
Hairdressing — In the seventh most frequently used supplemental series, 58% of patients tested had at least one positive reaction. This suggests that the series had considerable value, but more than half of the reactions were redundant information. Nickel, cobalt, balsam of Peru, and paraphenylenediamine are all on the screening series. Three allergens added to the screening series make a good hairdressing assessment: ammonium persulfate, glyceryl thioglycolate, and cocamidopropyl betaine.
Sunscreen — This series has not been helpful. Only 2 of 29 people tested had a reaction. It may be that a history of sunscreen intolerance is most commonly due to irritant contact dermatitis and the results are an accurate reflection of the rarity of true sunscreen allergy. Alternatively, a failure to do parallel photopatch testing with this series may result in false-negative information. This latter possibility is unlikely, since most of these patients were also photopatch tested with a more expansive photopatch test series used by the NACDG, but not reported on in this paper.
Oil and Coolant — The limited value reported for this series may reflect the lack of machinists in the patients referred to Ochsner Clinic. This criticism would be true for any highly “aimed” series of allergens. If the industry is not in the area, the allergens are of little value. Two substances not found on the screening series were Bioban P-1487 (3 reactions) and Grotan BK (2 reactions), which produced occasionally helpful information. The redundant information came from thimerosal, mercaptobenzothiazole, and formaldehyde.
Photography — Only two items on this series were helpful: CD 2 and metol. The series was used only eight times in 8.5 years.
Isocyanates — While isocyanates are manufactured in large quantities in the metropolitan New Orleans area, this series was needed only four times. The only positive reaction has been to diaminodiphenyl-(4,4) methane, rather than to an isocyanate.
Bakers — This series was used only four times in 8.5 years. The two reactions were both to octyl gallate. These were not relevant, and this is not considered an important series, despite all of the fresh-baked French bread for which New Orleans is well known.
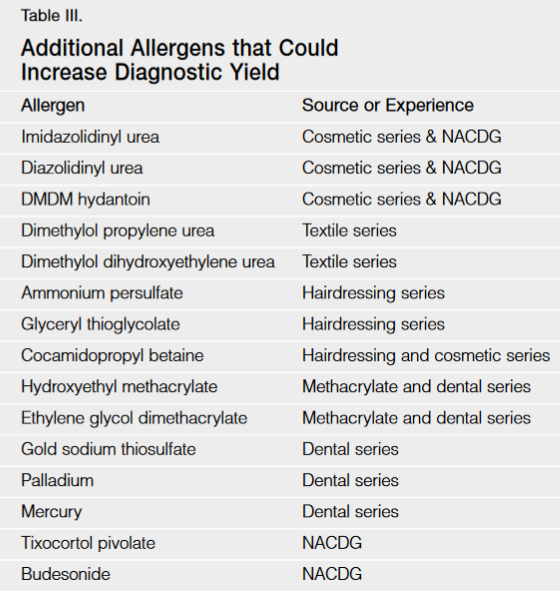
Comments
I have attempted to review my experience with supplemental allergens while considering a practical question posed to me by a colleague. He asked what additional 10 or 12 allergens would increase his yield over the use of a screening series such as TRUE test. The question is understandable, since the cost of all of the supplemental series reported here exceeds $5000. My recommendations are based on a review of the data presented here and the recent publication by the NACDG (Table III).1 Adjustments to this list would be appropriate based on industries and referral patterns that create unique circumstances. The recommendation for imidazolidinyl urea comes from experience with the former Hermal series of 20 allergens that was sold in the United States. This allergen is not among the components of the TRUE test, but in the NACDG series, 2.6% of 3101 patients tested positive. The recommendations for diazolidinyl urea and DMDM hydantoin also come from NACDG data, indicating that 3.7% of 3085 patients were positive to the former and 2.3% of 3082 patients were positive to the latter. Allergic contact dermatitis to corticosteroids is important in patient management, and screening with tixocortol pivolate 1% and budesonide 0.1% was positive in 2.3% and 1.1%, respectively, of patients tested by the NACDG.1 These substances are recommended for screening of all patients patch tested.