Casey E. Watkins, MD; John Litchfield, DO; George Youngberg, MD; Stuart S. Leicht, MD; Guha Krishnaswamy, MD
All from the Quillen College of Medicine, East Tennessee State University, Johnson City. Dr. Litchfield is from the Department of Internal Medicine, Dr. Youngberg is from the Department of Pathology, Dr. Leicht is from the Department of Dermatology, and Dr. Krishnaswamy is from the Department of Allergy and Immunology. Dr. Krishnaswamy also is from Mountain Home VA Medical Center, Tennessee.
The authors report no conflict of interest.
Correspondence: Casey E. Watkins, MD, Quillen College of Medicine, East Tennessee State University, PO Box 70580, Johnson City, TN 37614 (watkince@goldmail.etsu.edu).
Glatiramer acetate (GA) is a drug that commonly is used for the treatment of relapsing-remitting multiple sclerosis (RRMS). Although it typically is known as a safe and effective therapy, a number of adverse effects associated with GA have been reported in the literature. Local injection-site reactions (LISRs) and mild systemic symptoms are among the most commonly described adverse effects. A review of the literature revealed limited reports of panniculitis as an adverse effect of GA injection and even fewer describing associated skin necrosis. We report a case of GA-induced panniculitis and skin necrosis and discuss the occurrence of panniculitis, necrosis, and lipoatrophy following GA injections.
Glatiramer acetate is a common and highly effective therapy administered subcutaneously for the treatment of relapsing-remitting multiple sclerosis.
Common adverse effects include local injection-site reactions and transient acute systemic reactions.
Rarely, localized lipoatrophy and mostly lobular panniculitis with occasional necrosis can be observed at the site of glatiramer acetate injections. This reaction is specific to the medication and can recur with subsequent injections.
References
Glatiramer acetate (GA), a synthetic polypeptide that is injected subcutaneously, has proven effective in the treatment of relapsing-remitting multiple sclerosis (RRMS) and is now considered a first-line agent in the treatment of this condition. Adverse effects associated with GA primarily include local injection-site reactions (LISRs)(eg, erythema, pruritus, burning, pain, inflammation). Transient acute systemic reactions such as flushing and dyspnea also are commonly reported. Lipoatrophy at the injection site frequently has been reported in the literature as a cutaneous adverse effect of GA, but lobular panniculitis and necrosis at the site of injection rarely have been noted.
We report the case of a 36-year-old woman who experienced a severe adverse reaction to a single injection of GA after nearly 1 year of daily use to control symptoms of RRMS. Review of the current literature revealed few reports of the severe reaction of panniculitis and necrosis occurring at the injection site of GA.
Case Report
A 36-year-old woman was referred by her neurologist to the emergency department of our institution’s allergy and immunology clinic for treatment of an allergic reaction to a 20-mg GA injection, which she had been receiving daily for nearly 1 year as therapy for RRMS. A nodule immediately formed at the injection site and eventually became ulcerated. The patient also reported intense chest tightness, shortness of breath, and flushing following the injection. Physical examination revealed a large 8- to 9-cm erythematous area at the injection site on the left buttock. Necrosis and eschar formation also were evident (Figure 1).
Figure 1. Panniculitis with central ulceration and necrosis at the site of a glatiramer acetate injection on the left buttock (A). Closer view of an irregularly shaped necrotic lesion with surrounding erythema (B).
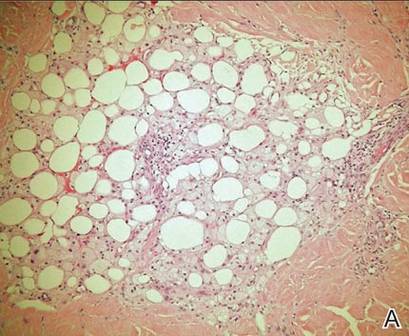
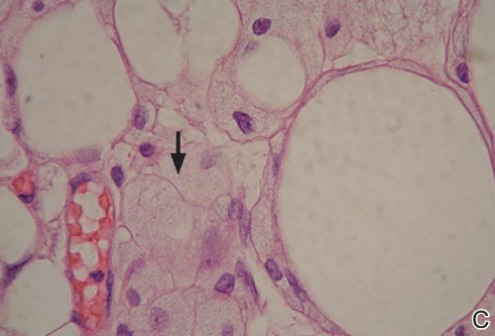
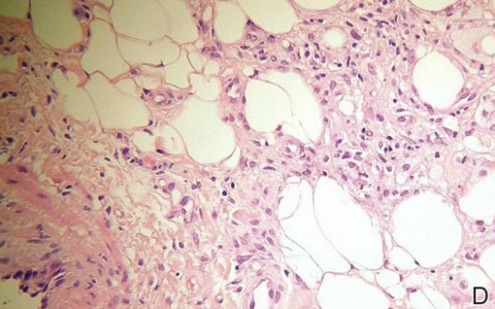
A punch biopsy from the edge of the lesion revealed predominantly lobular panniculitis (Figure 2A) with fat necrosis and numerous foamy macrophages (Figures 2B and 2C). Scattered lymphocytes also were present but no neutrophils or eosinophils were noted (Figure 2B). Interlobular septa were widened secondary to fibrosis (Figure 2A). No lymphoid follicles were identified. A subcutaneous artery was sampled but was negative for vasculitis (Figure 2D).
Figure 2. Lobular panniculitis with fat necrosis, foamy macrophages, and scattered lymphocytes. Septa were widened (A)(H&E, original magnification ×4). Fat necrosis and foamy macrophages were seen (B)(H&E, original magnification ×10). High-power field revealed foamy macrophages (black arrow)(C)(H&E, original magnification ×100). A subcutaneous artery (lower left) was negative for vasculitis (D)(H&E, original magnification ×20).
The necrotic lesion on the left buttock was present for more than 2 months before complete healing occurred. The patient had a history of intolerance or unresponsiveness to all prior medications for RRMS. Several years prior she responded well to treatment with GA for a few months and had been responding well to the injections over the last year. Incremental challenge testing with GA for desensitization was offered to the patient, but she declined treatment out of fear of a recurrent episode, particularly the severe systemic symptoms she had experienced. Unfortunately, she was lost to follow-up.
Comment
Glatiramer acetate, formerly known as copolymer-1, is a first-line treatment of patients with RRMS.1 Daily administration of subcutaneous injections of GA (20 mg/mL) has proven effective in relapse rate reduction and reduced morbidity in patients with RRMS.2 Long-term studies support a relapse rate reduction of more than 50% in patients using GA.3 The most common adverse effects are LISRs.2 Systemic reactions following GA injection also are common. A much less common reaction is panniculitis followed by lipoatrophy and/or skin necrosis. Only a few instances of panniculitis-associated necrosis have been reported.
The occurrence of LISRs was reported in 20% to 90% of patients using GA to control RRMS.2,4 Local injection-site reactions typically resolve within hours to days and have been reported to decrease in frequency over time.5 Acute systemic reactions (eg, anxiety, flushing, palpitations, dyspnea) to GA injection are described in approximately 15% of patients.6 Systemic reactions usually resolve in 5 to 15 minutes but can last for more than 1 hour.5 These reactions are mostly benign and generally are not considered to be allergic or anaphylactic in nature. True systemic anaphylaxis associated with administration of GA is extremely rare.7
Lipoatrophy, or localized loss of subcutaneous adipose tissue without evidence of inflammation, has been reported fairly frequently in association with GA (up to 45% of patients receiving GA injections).2,6,8,9 Lipoatrophy also has been seen following subcutaneous injection of many other drugs, including steroids and insulin. Unlike LISRs, the likelihood of developing lipoatrophy at the injection site increases with longer durations of GA injections.5 Lipoatrophy also develops following panniculitis at the site of GA injection.