Point-of-care (POC) ultrasound is a great adjunct to the evaluation and treatment of shoulder dislocations. This modality can assist with identification of the dislocation—especially posterior dislocations, which can be notoriously difficult to diagnose on plain radiography.1,2 Moreover, it can aid with reduction by guiding intra-articular anesthetic injection, regional anesthesia with an interscalene brachial plexus nerve block, or suprascapular nerve block. Following treatment, POC ultrasound also can immediately confirm successful reduction.
Imaging Technique
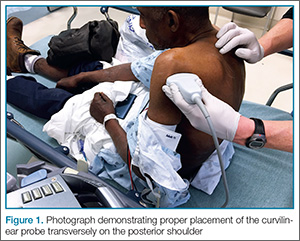
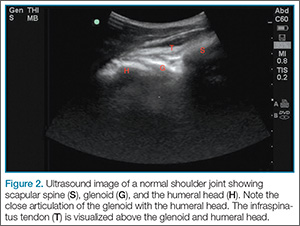
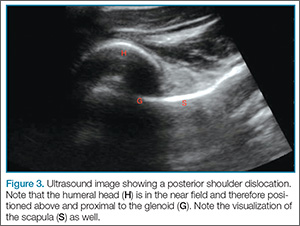
Since the shoulder joint is a deep structure, ultrasound should be performed using the lower frequency curvilinear probe. The probe should be positioned in the transverse orientation, behind the shoulder and over the scapular spine (Figure 1). The probe is then moved laterally to identify the glenoid; after the glenoid is visualized, the probe is moved further to locate the humeral head and determine its relationship to the glenoid. If the shoulder joint is immediately adjacent to glenoid, then it is in the appropriate anatomical position (Figure 2). If the humeral head is located in the near field of the image above the glenoid on the ultrasound screen, then a posterior dislocation is present—ie, since the probe is touching the posterior shoulder, the top of the screen represents posterior structures and the bottom of the screen represents anterior structures (Figure 3). If the humeral head is below the glenoid in the far field of the image, then the shoulder is anteriorly dislocated (Figure 4). A hyperechoic hemarthrosis is often seen in the joint when shoulder is anteriorly dislocated.
Facilitation of Reduction
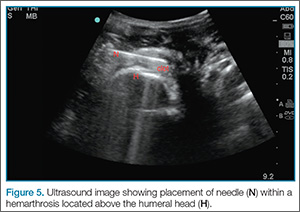
Ultrasound-guided intra-articular joint injection is a simple and effective technique to deliver anesthesia to the shoulder.3 Imaging is performed with the same curvilinear probe using sterile precautions—ie, sterile probe and cord cover, sterile gloves, and skin prepped with chlorhexidine. To access the shoulder joint, a long needle, such as a spinal needle, is utilized to deliver a short-acting local anesthetic (eg, 1% lidocaine). It is essential to line up the probe marker with the screen marker to facilitate needle placement and adjustment. The spinal needle is inserted into the lateral deltoid, beneath the acromion and a few centimeters from the edge of the probe. It is then directed by ultrasound in real-time toward the hemarthrosis. Once the needle is within the joint, fluid should be aspirated to confirm return of blood and inject 20 cc of lidocaine (Figure 5). A video demonstrating this technique may be accessed online at https://vimeo.com/156762428. Before performing the reduction technique of choice, the clinician should wait 10 to 15 minutes for the joint injection to take effect.
Summary
Bedside ultrasound is an excellent adjunct to traditional radiographs in the evaluation of patients presenting with shoulder injuries. In addition to its high sensitivity in detecting dislocation, this modality can be used to guide intra-articular treatment and to confirm successful reduction.
Dr Meer is an assistant professor and director of emergency ultrasound, department of emergency medicine, Emory University School of Medicine, Atlanta. Dr Beck is an assistant professor, department of emergency medicine, Emory University School of Medicine, Atlanta. Dr Taylor is an assistant professor and director of postgraduate medical education, department of emergency medicine, Emory University School of Medicine, Atlanta.