The chaos of a busy ED can test the cognitive reserve of even the most focused practitioner. To streamline the challenge of serial diagnosis and treatment, clinicians employ heuristics while honing the skills of pattern recognition. However, by definition, heuristics employs shortcuts, leaving out information for the sake of efficiency—sometimes at the expense of accuracy. Whether a patient presents with chest pain, abdominal pain, headache, or (the dreaded) dizziness, emergency physicians (EPs) employ algorithms based on a combination of education and prior experience.
Most of the time, these models lead the EP along the correct path, but not always. For example, when a clinician evaluating a patient presenting with psychotic behavior assumes the patient has schizophrenia, he or she will be correct eight or nine times out of 10. However, in some cases, a patient’s bizarre behavior may not be due to a true psychiatric disorder but, for example, from ingestion of an illicit substance.
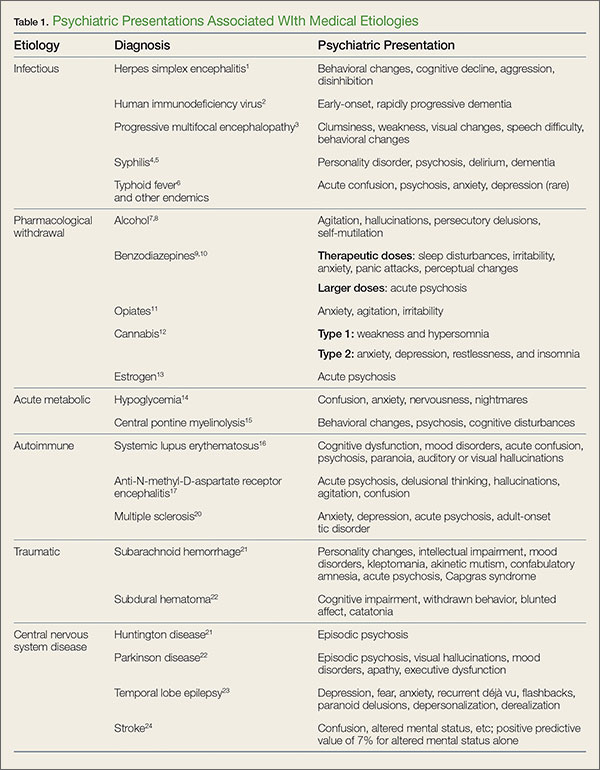
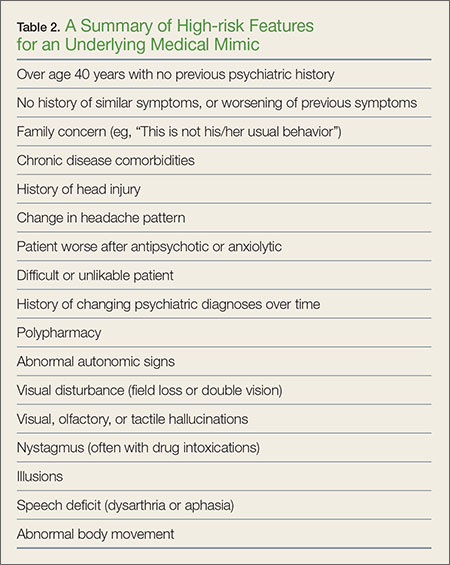
In addition, in such patients, psychiatric symptoms may be masking a serious acute, organic condition—one requiring prompt intervention and therapy to avoid morbidity or death. To help prevent diagnostic errors, this 2-part series reviews several of the most common medical mimics of psychiatric conditions. Part 1 of this series reviews the psychiatric presentations associated with medical conditions of an infectious, pharmacological withdrawal, metabolic, autoimmune, traumatic, or central nervous system etiology (Table 1). This article also discusses clinical signs and symptoms that suggest an increased likelihood that a patient’s psychiatric symptoms are from an underlying medical condition (Table 2).
Case Scenarios
Case 1
A 58-year-old woman with a history of smoking 40 packs of cigarettes per year presented to the ED 1 hour after onset of intermittent chest pain. Upon arrival at the ED, the patient stated that she had trouble catching her breath on and off throughout the day. The patient’s vital signs, electrocardiogram (ECG), and chest X-ray were all normal. The physical examination was unremarkable except for mild diaphoresis. The patient denied experiencing palpitations, recent travel, or previous episodes; she further stated that she was currently not on any medications. There was no previous history of visits to this hospital. The patient’s husband, who accompanied her to the ED, noted that his wife’s behavior had been atypical for approximately 1 week.
After receiving aspirin, the patient appeared symptom-free. Pending the results of another chest radiograph and laboratory evaluation, the EP anticipated moving her to the chest-pain observation unit.
Case 2
A 36-year-old woman presented with altered mental status to the ED via emergency medical services (EMS). Her vital signs, including temperature, were normal. Despite intermittently appearing to be asleep, the patient was alternatingly cooperative and combative. She repetitively whispered, “Who am I?” and randomly shouted at staff members as they walked by her room.
Her neurological examination was nonfocal. The hospital’s electronic medical record (EMR) for this patient showed nearly monthly ED visits for behavioral symptoms. Precipitating events noted in the EMR included job loss and separation from her husband. While waiting for the results of the basic laboratory work-up and toxicology screening to medically clear the patient for psychiatric evaluation, the EP contemplated a computed tomography (CT) study. Realizing the patient would not be able to remain still for the scan, the EP ordered 10 mg of intramuscular ziprasidone for sedation. When the patient’s husband arrived, the EP placed the CT scan on hold until she could obtain additional history from him.
Infections
Herpes Simplex Encephalitis
Herpes simplex encephalitis (HSE) is a serious but treatable disease—one that requires early detection and treatment to avoid severe morbidity. While the classic symptoms are fever and altered mental status, recent literature has noted that afebrile patients with HSE may present with behavioral changes, cognitive decline, aggression, and disinhibition. Therefore, diagnosis of a functional psychiatric complaint, if made initially, could delay appropriate treatment with acyclovir.1
Human Immunodeficiency Virus
Progression of human immunodeficiency virus (HIV) is a well-known cause of various neurocognitive disorders, including early-onset dementia. Since the availability of highly active antiretroviral therapy, the incidence of HIV dementia has decreased, but HIV remains the most common preventable cause of dementia in persons younger than age 50 years. Recent literature has described HIV dementia presenting as an early-onset, rapidly progressing dementia in a young person. Thus, the EP should consider early HIV testing in any young patient who presents with dementia, especially one with a history of fever of unknown origin.2
Progressive Multifocal Encephalopathy
Caused by reactivation of the John Cunningham virus, progressive multifocal encephalopathy has been classically described as a potentially lethal complication of a severely immunocompromised state, often presenting with clumsiness, weakness, visual changes, speech difficulty, and behavioral changes. Though typically described as occurring in the context of acquired immunodeficiency disease syndrome, hematological malignancy, or organ transplant, the condition can occur in the setting of minimal or occult immunosuppression—especially in patients with a history of cirrhosis. If the condition is detected early, immunotherapy can result in significant clinical improvement.3