CHICAGO – Adding a small rubber tip with flexible, circular rings to the end of a colonoscope dramatically improves polyp and adenoma detection during colonoscopy, according to interim results from a randomized, tandem study.
In a per lesion analysis, the adenoma miss rate was 13% when patients underwent an EndoRing colonoscopy followed by a standard colonoscopy and 53% when standard colonoscopy was done before the EndoRing colonoscopy (P less than .001).
 ©EndoAid Ltd.
©EndoAid Ltd.
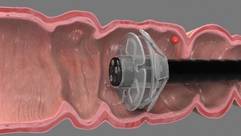
The flexible, circular rings of the EndoRings improve visualization by engaging and stretching colonic folds during withdrawal.
The miss rates for polyps were 11% and 58% (P less than .001), *Dr. Peter D. Siersema said in a late-breaking abstract session at the annual Digestive Disease Week.
Adenomas are missed in about 25% of tandem studies with standard colonoscopies, and the miss rate may be as high as 40% with new techniques. This is mainly due to inadequate visualization of proximal aspects of folds and inner curves of flexures. The flexible, circular rings of the EndoRings improve visualization by engaging and stretching colonic folds during withdrawal, explained Dr. Siersema of the University Medical Center Utrecht, the Netherlands. The EndoRings device is Food and Drug Administration and CE approved and available in the U.S. and Europe.
 ©EndoAid Ltd.
©EndoAid Ltd.
A close-up view of the EndoRings device.
From July 2013 to April 2014, investigators in the Netherlands and Israel enrolled 106 patients, aged 40-75 years, with an indication for screening, surveillance, or diagnostic colonoscopy, to undergo same-day, back-to-back colonoscopies by the same endoscopist. Bowel preparation followed standard protocol at the centers (polyethylene glycol or sodium picosulfate). Conscious sedation (midazolam, fentanyl, propofol, or combination) was used in most patients. Polyps found during the first procedure were immediately removed.
The average time to the cecum and withdrawal times were similar in the two groups, although total procedure time was significantly longer with the EndoRings (mean 22 minutes vs. 18 minutes; P less than .001) due to the removal of more polyps, Dr. Siersema said.
Among 49 evaluable patients in the study group, 79 polyps were detected with EndoRings during the first procedure and 10 additional polyps during the subsequent standard colonoscopy.
Among 47 evaluable controls, 25 polyps were detected during the first pass with standard colonoscopy and 34 additional adenomas in the second pass with EndoRings.
There was no difference in the location, size, morphology, and histology of the missed polyps between groups, he said.
In the study group, 46 adenomas were found during the initial procedure with EndoRings and 7 more during the second pass using standard colonoscopy.
Among controls, 17 adenomas were detected during the first pass with standard colonoscopy and 19 more in the second pass with EndoRings.
 Patrice Wendling/Frontline Medical News
Patrice Wendling/Frontline Medical News
*Dr. Peter D. Siersema
Surveillance intervals were shortened for eight patients who underwent standard colonoscopy first and two patients who underwent EndoRings colonoscopy first, Dr. Siersema said. There were no adverse events in the study.
During a discussion of the results, Dr. Siersema said the single-use device "was very cheap" to purchase and has an additional advantage of stabilizing the scope in the center of the colon.
Session cochair Dr. Pankaj Pasricha, director of the Johns Hopkins Center for Neurogastroenterology, said some colonoscopes are incorporating expandable tips, and that there are four or five other add-on devices, one with streamers and another with a balloon.
"They are relatively inexpensive, simple approaches to solving a complex problem," he said in an interview. "It is a real problem looking behind folds, missed polyps, and if large-scale studies show that [this is improved], then this could be really something very easily incorporated into your practice, as opposed to buying a new scope for hundreds of thousands of dollars."
Dr. Siersema reported a travel grant to attend the meeting. Three coauthors reported consultancy for and one reported employment with the study sponsor, EndoAid. Dr. Pasricha reported relationships with Pentax, GI Supply, and Apollo Endosurgery.
Correction 5/20/14: A previous version of this story incorrectly identified Dr. Peter D. Siersema in both the photograph and in references throughout the text. This version has been corrected and updated.