Selecting Among Recommended Antibiotic Choices
As antibiotic preparations for treating bacterial AOM are oral suspensions, taste is a major factor for pediatric patients. TABLE 4 summarizes comparative taste ratings for antibiotic suspensions based on several studies and shows the range, from those that can enhance compliance to those that discourage compliance.23
Adverse events, especially diarrhea, nausea/vomiting, and gastritis, are also of concern. These are shortcomings of amoxicillin/clavulanate, which has a higher incidence of diarrhea and nausea than cephalosporins.24
Dosing frequency is also a factor among recommended agents. Amoxicillin, amoxicillin/clavulanate, cefprozil, and cefpodoxime require twice-daily dosing. Cefdinir can be effective at once-daily dosing.24
Duration of approved therapy is perhaps the most critical selection factor given the reality of patient behaviors. Cefpodoxime and cefdinir are the only 2 FDA-approved agents for 5-day treatment of bacterial AOM that are also guideline-recommended.
TABLE 4
Compliance-Enhancing Ranking of Antibiotic Suspensions
| STRONGLY COMPLIANCE-ENHANCING | |
|
|
| MODERATELY COMPLIANCE-ENHANCING | |
|
|
| EQUIVOCAL COMPLIANCE-ENHANCING | |
| |
| NOT COMPLIANCE-ENHANCING | |
| |
| DISCOURAGES COMPLIANCE | |
|
|
| TMP-SMX, trimethoprim sulfamethoxazole | |
| Sources: Adapted from Steele RW, et al. Pediatr Infect Dis J. 2001;20:1-5. | |
| Demers DM, et al. Pediatr Infect Dis J. 1994;13:87-89. | |
| Ruff ME, et al. Pediatr Infect Dis J. 1991;10:30-33. | |
Choices for Effective Initial Therapy
Considering the changing microbial population in bacterial AOM and the increasing concern of effectiveness of amoxicillin and other antibiotics against β-lactamase–producing H influenzae, the choice of therapy may need modification. Specifically, that may mean changing the choice of effective antibiotic, taking into consideration the compliance-enhancing advantages of available options.
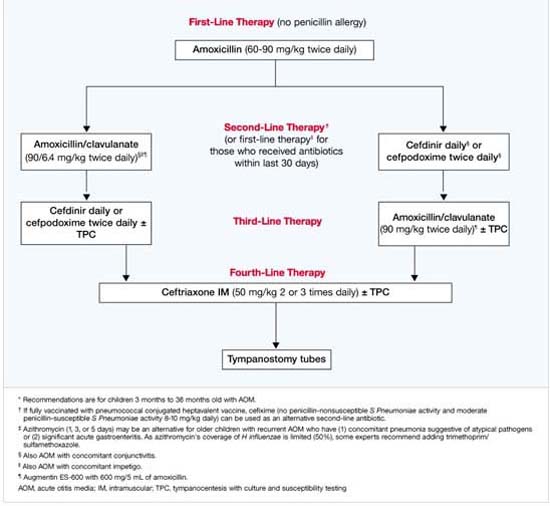
Based on efficacy, the overall prevalence of antibiotic-resistant AOM pathogens for PCV-7-vaccinated children, the potential for adverse effects, and patient compliance issues, Block and Harrison developed an algorithm (FIGURE) for the management of AOM diagnosed by strict criteria in an otherwise healthy child between 4 months and 36 months old.24 As the environment of AOM evolves, the choices for treatment must be not only effective but also the best and most appropriate.
FIGURE Antibiotic Choices for Acute Otitis Media in the 2000s