Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
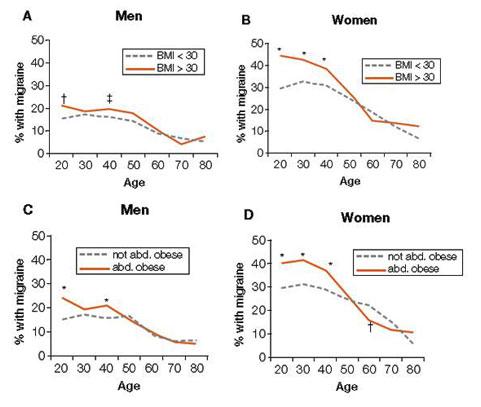
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]